
Abstract
Background
Weightbearing radiography is an essential diagnostic tool in orthopedics, especially in the setting of foot and ankle pathology. However, there is a lack of studies examining the percentage of weight placed on a limb during weightbearing x-rays, potentially affecting the quality of the radiograph.
Methods
Over a 3-month period, the percentage of weight placed through an injured extremity was recorded for 434 patients receiving weightbearing radiographs of the foot or ankle in a single clinic.
Results
For the overwhelming majority of radiographs, patients placed less than half their weight on their injured extremity. Lateral radiographs had a lesser percentage of weightbearing compared with anteroposterior (P = .0096) and oblique (P = .0042) radiographs. Patients with acute injuries placed less weight on their extremity in lateral foot radiographs compared with those with acute injuries (P = .0023). A high variability of weight was placed through the extremity regardless of pathology.
Conclusion
These results highlight the need for clinician awareness regarding the discrepancies in weightbearing radiography, the importance of technician and patient education on technique and importance of quality imaging, and the plethora of questions that still remain regarding what characteristics comprise a sufficient weightbearing radiograph.
Levels of Evidence:
Level III: Prognostic
“Weightbearing x-rays allow better standardization and reliability in assessment of lower limb pathologies in patients, especially in comparison with non-weightbearing x-rays.”
Introduction
Weightbearing radiography is standard in the diagnosis of several pathologies involving the foot, ankle, or hip. Standing on the limb puts stress on the injury during imaging, helping physicians evaluate the extent of instability caused by the injury. Evaluating stress radiographs is especially helpful in situations where instability is not clearly visible in initial radiographs, as soft tissue indicators such as swelling, tenderness, and ecchymosis are unreliable indicators of instability. 1
Studies have favorably compared the utility of weightbearing x-rays with non-weightbearing x-rays in diagnosis of Lisfranc injuries, 2 ankle fractures,3,4 fibular fractures,5,6 and hallux valgus deformities. 7 Weightbearing x-rays provide a more dynamic image of physiological stress in comparison with a static image provided by non-weightbearing x-rays 2 and are also considered to represent the clinical situation more closely than non-weightbearing x-rays. 1 In a study done by Boszczyk et al, 7 hallux valgus diagnoses for more than half of patients changed after assessment of weightbearing imaging when physicians were given no other clinical information. León-Muñoz et al 8 note that non-weightbearing x-rays underestimate the degree of deformity at knee joints, and weightbearing x-rays must be taken into consideration in the planning of total knee arthroplasty surgery. Overall, weightbearing x-rays allow better standardization and reliability in assessment of lower limb pathologies in patients, especially in comparison with non-weightbearing x-rays. 9 Several radiographic measurements differ significantly with increasing percentage of weight placed in weightbearing x-rays, including talonavicular coverage angle, talocalcaneal angle, and cuboid height to ground. 10
Typically, when weightbearing x-rays are taken, examiners do not quantify the percentage of weight placed on the foot. The percentage of weight placed on the limb may therefore vary with patient, x-ray view, or severity of injury. There is a lack of studies examining this variation in percentage of weight placed on limb during weightbearing x-rays. We hypothesize that patients with acute or subacute injuries will likely place a lesser percentage of weight on the injured extremity in comparison with patients with chronic injuries. The goal of this study is to investigate the percentage of weight placed on an injured extremity in weightbearing x-rays, stratified by anatomic location of injury and chronicity of injury to better understand pathologies that might be at risk of insufficient imaging.
Methods
Study Design
This study was reviewed and approved by the University of Texas Medical Branch institution’s institutional review board. We completed a prospective data collection of all new patients who presented to the senior faculty authors’ clinics over a 3-month period between May 1, 2021, and July 31, 2021, with complaints of ankle or foot pain. Radiographic views evaluated for patients included standard lateral foot, anteroposterior (AP) ankle, oblique (mortise) ankle, and/or lateral ankle films with selection of views based on original chief complaint during triage in clinic. During initial imaging, the patient’s injured extremity was placed on a scale, disguised to limit bias, and the patient was instructed to place weight on their injured extremity. The total weight placed on the scale was recorded per radiographic view. These values were then compared with the patient’s total weight.
A standard bathroom scale with Bluetooth connectivity was used. The scale was shrouded in a sheet to avoid detection by the patient (Figure 1). The weight placed on the scale was communicated to the radiology technician’s smart phone via Bluetooth and the weight recorded by the scale at the time of imaging was used as the datapoint. The bathroom scale was calibrated with the manual clinic scale and was accurate to 2 decimals. However, as this study evaluates weight placed on the extremity as a percentage of the patient whole, this negates the need for calibration to achieve perfect matched values.
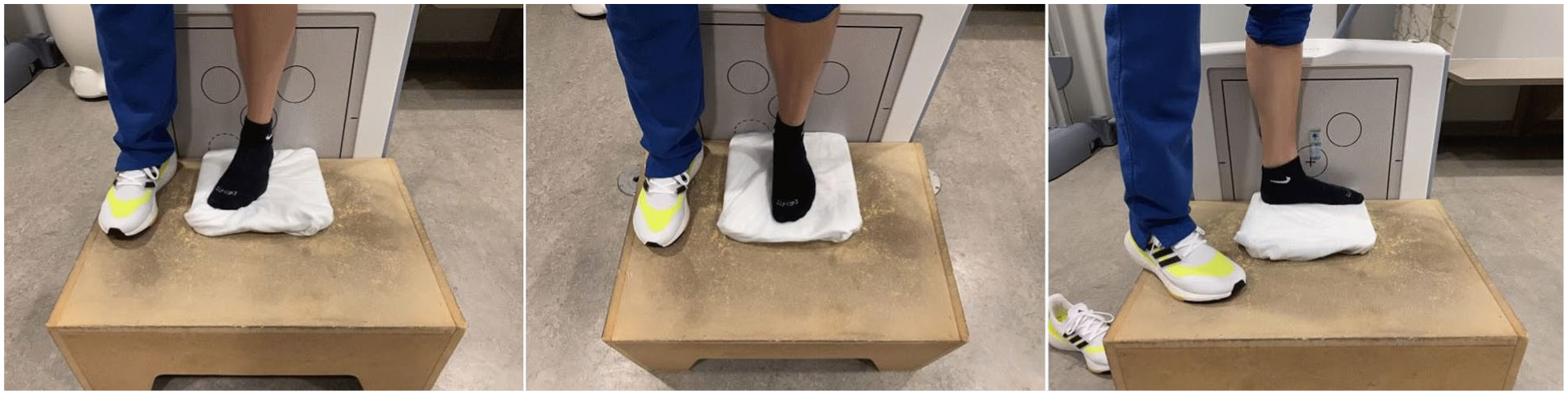
Clinical image of patient positioning on scale (shrouded) during data collection of Mortise ankle (left), anteroposterior ankle (middle), lateral foot, and ankle (right) x-ray views.
Demographics
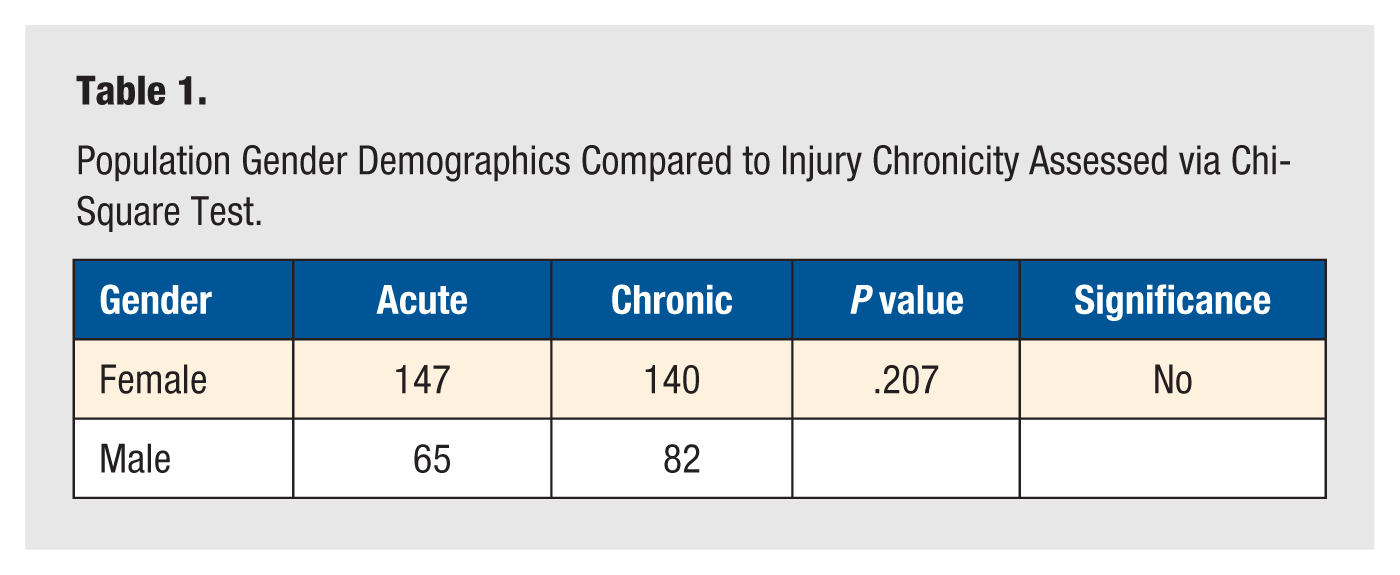
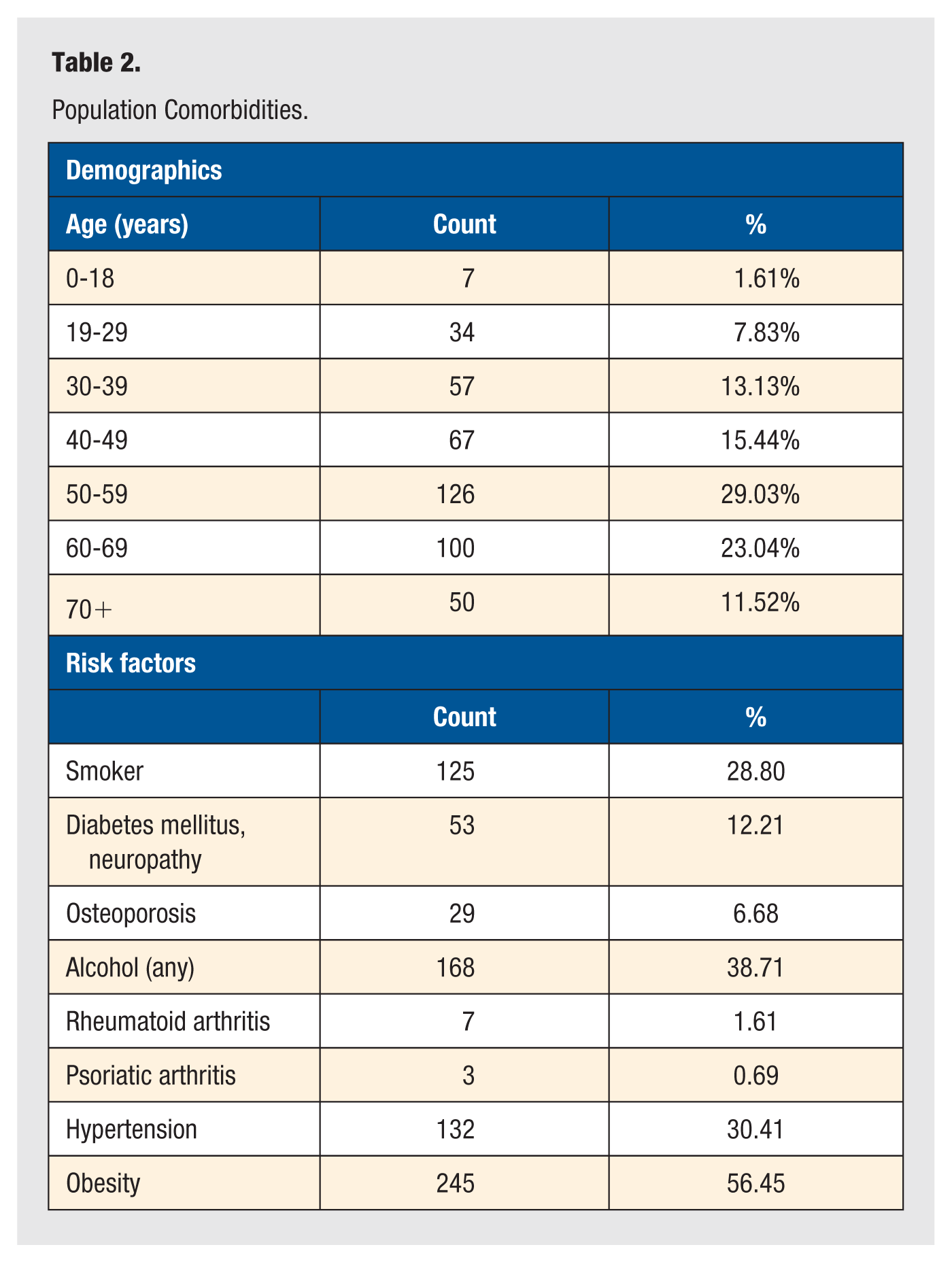
Inclusion criteria included patients 18 years old and above who were new patients to the foot and ankle clinic during the aforementioned date range. Exclusion criteria included patients in the prison system and pediatric patients. After data collection, we analyzed the results of 434 patients with ages ranging from 18 to 94 years. Although data were primarily collected from female patients (66%), the gender distribution was similar between acute and chronic groups (P = .207; Table 1). Other risk factors considered were age, a current history of smoking, diabetes, osteoporosis, alcohol use, rheumatoid arthritis, psoriatic arthritis, hypertension, and obesity (Table 2).
Population Gender Demographics Compared to Injury Chronicity Assessed via Chi-Square Test.
Population Comorbidities.
Collected data per patient were then stratified based on injury chronicity and the anatomic injury location per the final diagnosis made: forefoot, midfoot, hindfoot, ankle, and “other.” Patients included in “other” were those with diagnoses such as soft tissue masses or foreign bodies that could occur in various locations and those with diffuse pathology such as Charcot arthropathy or neuropathy. Acute injuries included those with symptoms less than 6 weeks and chronic with symptoms more than 6 weeks. Data were also further stratified per imaging view by lateral foot, AP ankle, oblique (mortise) ankle, and lateral ankle.
Statistical Analysis
We used a 1-way analysis of variance test to compare the average weightbearing percentage in the AP ankle, lateral ankle, and oblique ankle x-rays groups, which we followed with a Tukey test between the individual pairs. Comparisons between average weightbearing percentage for location of injury was made by 2-tailed t tests.
Results
Total Weight Placed Between Pathology and Radiographic View
When evaluating the amount of weight placed on each extremity during a weightbearing radiograph, it would be anticipated that each limb would support 50% of the patient’s weight. However, upon gross evaluation of the data, in only 2 combinations of imaging view and anatomic location was this seen. In patients with ankle pathology, an average of 50.43% of weight was placed on the injured extremity during an oblique radiograph and 49.97% was placed during an AP ankle radiograph. Slightly less but still near equal weight distribution was seen in patients with forefoot (45.72%) and midfoot (45.45%) injuries during lateral foot radiographs, and in patients with ankle pathology during lateral ankle radiographs (45.72%). Inversely, notably low weights were placed during the predominance of imaging, with lowest weightbearing percentages placed by patients with ankle pathology during lateral foot radiographs (7.22%); those with forefoot pathology during AP (17.99%), oblique (18.99%), and lateral ankle radiographs (14.96%); and those with midfoot pathology during lateral ankle radiographs (16.74%).
Weight Comparisons Between Radiographic Views of All Pathologies
When comparing percent of weight placed per radiographic view, patients placed significantly more weight on their injured extremity when obtaining an AP of the ankle (P = .0096) or an oblique view of the ankle (P = .0042) when compared with weight placed during a lateral ankle view. No significant difference existed between weight placed during an AP and an oblique ankle view (Figure 2).
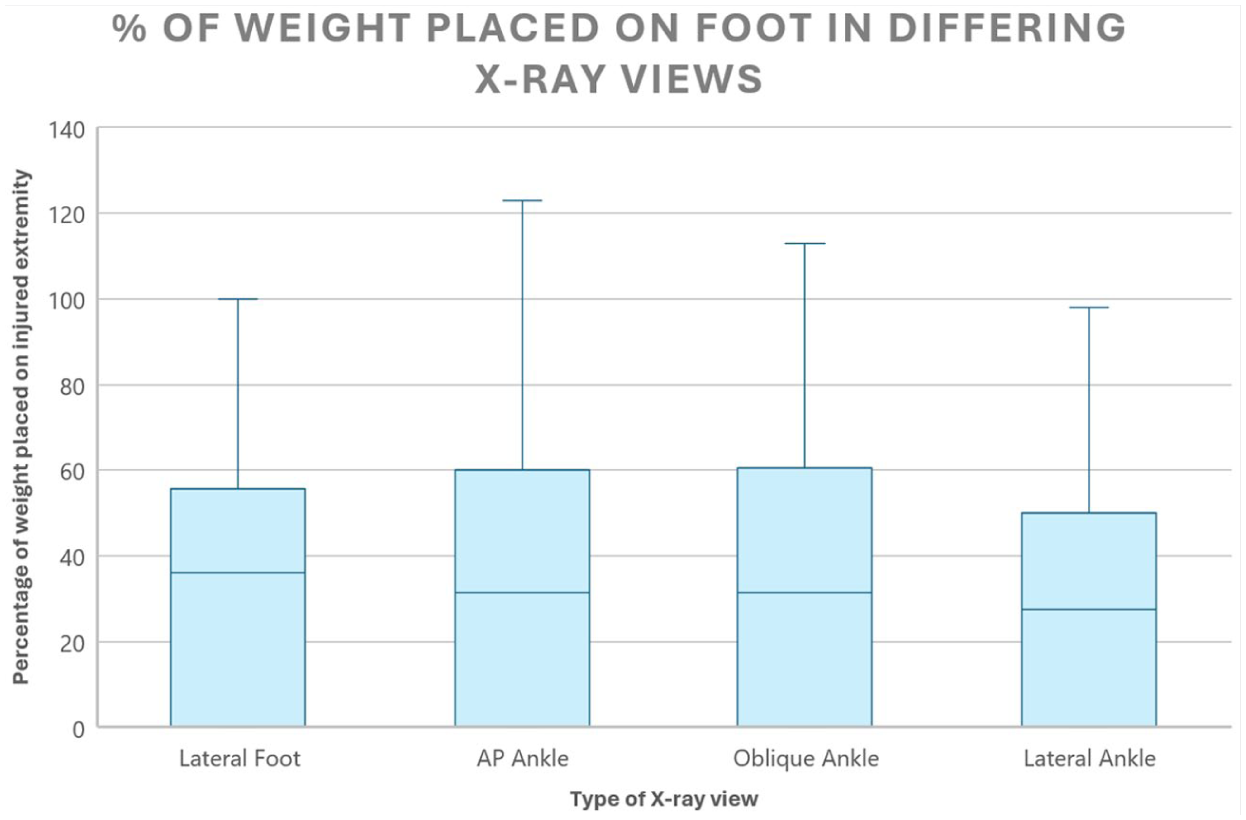
Percent of weight placed on foot in differing x-ray views. Abbreviation: AP, anteroposterior.
Weight Comparisons Based on Anatomic Location per Radiographic View
Notable differences in percent weightbearing on the injured extremity were noted when comparing the diagnosis anatomic location and imaging view. When comparing those with ankle pathology versus those with forefoot, midfoot, hindfoot, and “other” pathology, significant differences were found between those with ankle pathology and all those with “other” foot pathology in all radiographic views with the exception of the percentage of weight placed on the injured extremity during an oblique radiograph of the ankle in patients with either ankle or hindfoot pathology. When obtaining a lateral weightbearing foot radiograph, those with ankle pathology were noted to place on average only 7% of their weight on their injured extremity, significantly less than those with forefoot, midfoot, hindfoot, or “other” pathology (P < .0001 for all).
Compared with other anatomic injury locations, those with forefoot pathology placed significantly less weight on their injured extremity than those with hindfoot injuries in all views (P < .01), and significantly less than those with ankle pathology in all ankle radiographs (P < .0001). However, the only patients who placed a greater percentage of weight than those with forefoot pathology were those with ankle pathology during the lateral foot radiographs (P < .0001). When comparing forefoot and midfoot pathology, weightbearing percentages on the injured extremity were not significantly different. No differences were found between the forefoot group and the “other” group in AP and oblique ankle radiographs. However, compared with patients with “other” pathology, patients with forefoot pathology placed more weight during lateral foot radiographs (P = .0485) and less during lateral ankle radiographs (P = .0324).
Looking at those with midfoot pathology, these patients placed similar weight to patients with foot and “other” pathology in all views. However, compared with patients with ankle pathology, those with midfoot pathology placed more weight comparatively during the lateral foot radiographs (P < .0001) and significantly less weight during AP (P = .001), oblique (P < .0001), and lateral (P < .0001) ankle views.
For patients with hindfoot pathology, again, no differences were noted during any view when compared with those with midfoot or “other” pathology. Those with hindfoot pathology, when compared with those with ankle pathology, placed notably more weight during the lateral foot radiographs (P < .00005) but notably less during AP ankle (P = .023) and lateral ankle (P = .004) radiographs. Patients with hindfoot pathology when compared with those with forefoot pathology placed notably less weight during lateral foot radiographs (P = .005), but notably more during AP ankle (P = .001), oblique ankle (P = .002), and lateral ankle (P = .001) views.
In patients with diagnoses without specific anatomic location, designated as “other,” significantly more weight was placed through the injured extremity than those with ankle pathology during lateral foot radiographs (P < .0001) and those with forefoot pathology during lateral ankle (P = .0324) radiographs. Patients with “other” pathology placed significantly less weight during AP radiographs than those with forefoot injuries (P = .0485) and those with ankle injuries during AP ankle (P = .0005), oblique ankle (P = .0010), and lateral ankle (P = .0039) radiographs.
Weight Comparisons Between Acute and Chronic Injuries
When evaluating the weight placed on the injured extremity per radiographic view, statistical differences were noted for patients with acute (<6 weeks) versus chronic (>6 weeks) pathology when evaluating lateral foot radiographs (P = .0023) but not for any ankle radiographs (Table 3). Of patients who received lateral foot radiographs, 109 had acute pathology and 117 had chronic pathology, with each group placing approximately 28.72% and 37.66% of their weight on their injured extremity, respectively (mean difference = –8.94335, 95% confidence interval [CI] = –14.676774 to –3.209931, P = .0023). This result is consistent with our hypothesis that those with acute injuries are likely to place less weight on their injured extremity than those with chronic injuries.
Percent of Patient Weight Placed on Injured Extremity per Radiographic View and Chronicity of Injury.
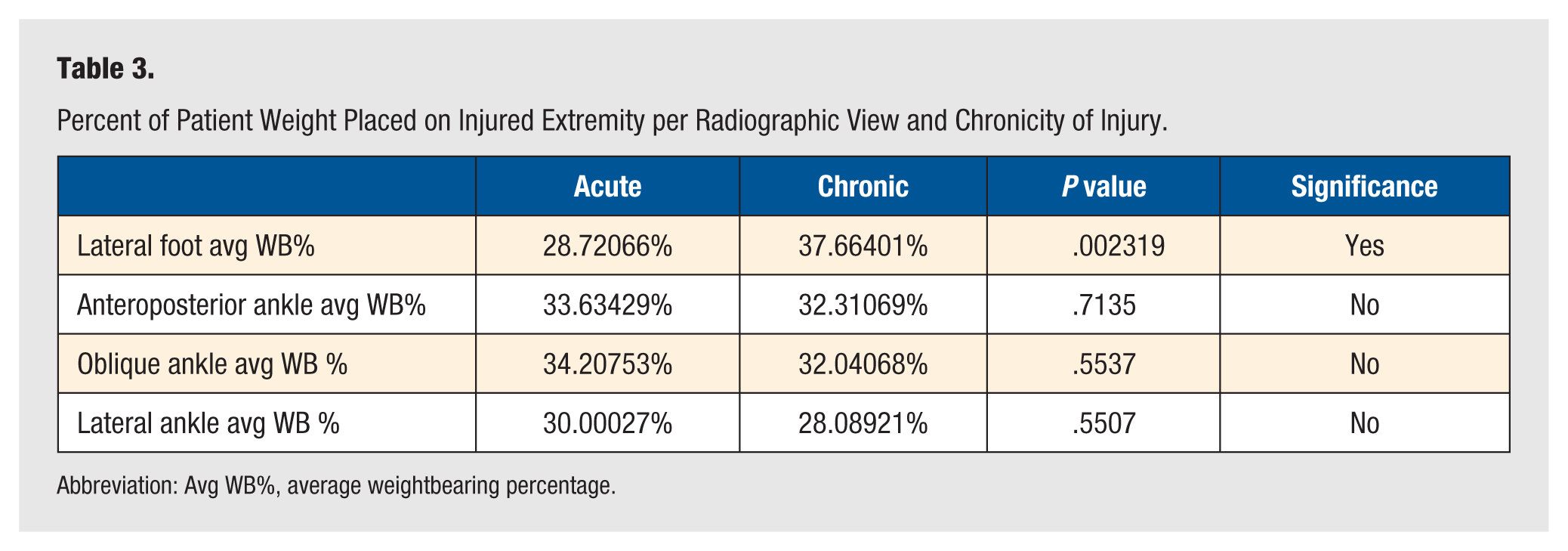
Abbreviation: Avg WB%, average weightbearing percentage.
In evaluation of ankle radiography, no significant differences were found between those with acute and chronic pathology. For those receiving AP ankle radiographs, 102 patients had acute pathology and 67 had chronic pathology and placed approximately 33.63% and 32.31% of their weight on their injured extremity, respectively (mean difference = 1.3236, 95% CI = –5.761394 to 8.408602, P = .7135). Oblique radiographs of the ankle were obtained for 189 patients (102 with acute and 67 with chronic pathology). In this view, patients with acute pathology placed an average of 34.21% of their weight on the injured extremity, while patients with chronic pathology placed an average of 32.04% of their weight on the injured extremity (mean difference = 2.16685, 95% CI = –5.023381 to 9.357094, P = .5537). Finally, lateral ankle radiographs were taken of 102 acutely injured patients who placed an average of 30.00% of their weight on their injured extremity and 67 chronically injured patients who placed an average of 28.09% of their weight on their injured extremity (mean difference = 1.91106, 95% CI = –4.383643 to 8.205768, P = .5507).
Discussion
Weightbearing radiography is an essential diagnostic tool in orthopedics, especially in the setting of foot and ankle pathology. However, no study has yet investigated the amount of weightbearing that occurs during a weightbearing radiograph. With decreased weight application to the affected extremity, a decreased quality of radiograph can be expected. Our results highlight that in nearly every described combination of radiographic view and pathology, less than the anticipated weight—half the weight of the patient—was borne through the injured limb, which can ultimately lead to diminished appearance of pathology on radiographs and potentially increased risk of misdiagnosis.
Existing literature underscores the importance of adequate loading on image quality. Shelton et al found that increasing applied load altered several radiographic alignment parameters in healthy individuals, most notably increased hindfoot valgus and medial arch flattening between 10% and 25% loading, but demonstrated little change once >25% body weight was applied. Their work suggests that achieving a certain minimum weightbearing threshold is essential for accurate radiographic interpretation. Our findings complement this conclusion by demonstrating that, in clinical practice, patients frequently fail to reach even half their body weight on the affected limb—suggesting that many “weightbearing” radiographs may not exceed Shelton functional threshold. Importantly, our study expands upon theirs by evaluating patients with pathology, and by demonstrating how patient behavior, injury location, and radiographic view influence weightbearing levels, which Shelton et al did not investigate.
As this study has highlighted, a significant variability exists when obtaining a weightbearing radiograph regardless of pathology anatomic location or radiographic view. The authors observed a notably low percentage of weight placed through the affected extremity in patients with forefoot pathology during ankle radiographs and, inversely, patients with ankle pathology during foot radiographs, despite logical anticipation of the opposite results. This could be the result of radiology technician’s appropriate verbal queuing as well as patients attempting to provide a good performance during imaging of their injury and resting during imaging of other locations.
In addition, significant differences were seen between radiographic views. During AP and oblique ankle radiographs, weight was more effectively placed on the injured extremity than during a lateral radiograph. Perhaps this can be attributed to patient positioning, as stance during an AP or oblique radiograph is more similar to the natural standing position while positioning during a lateral weightbearing radiograph requires mildly prolonged abnormal positioning by the patient, resulting in compensation by the unaffected limb.
Although the authors anticipated chronicity of pathology to play a role in the quality of weightbearing during weightbearing radiographs, this was found to be less impactful during ankle imaging. It was hypothesized that in the acute setting, patients would be less willing to apply weight to their injured extremity. This was observed during lateral imaging of the foot. However, inversely, in each view of the ankle, those with acute injuries were observed to place a slightly higher percentage of their weight on their affected extremity, yet this was noted to be not statistically significant in any single view.
Overall, a large number of statistically significant findings were discovered over the course of this study, some of which aligned with the authors’ expected results and some were unexpected. It is known that high-quality weightbearing radiographs are necessary in the diagnosis of various foot and ankle pathologies. The results of this study, which highlight the irregularities among weightbearing radiographs, raise the question of how much weight is required for a sufficient weightbearing radiograph: Is it a percentage of patient weight, a total amount of weight, or even, does it vary by pathology? The senior author (VKP) coined the term ‘Weighted Weight-Bearing’ or ‘WWB’ x-rays when the amount of weight is quantified on these weight bearing x-rays. 11
This study does have limitations, the first of which is the overwhelming percentage of women in the studied population. Although unlikely to have affected the outcome, this discrepancy cannot be dismissed. In addition, this study took place in a single clinic with a small number of radiographic technicians, and while the results of these data can be extrapolated, the inclusion of more locations and technicians would assist in the accuracy of generalizing these results. Finally, the height of the bathroom scale may have created a less stable stance during lateral views, which could contribute to decreased weightbearing. However, this likely reflects real-world patient behavior, as individuals experiencing discomfort or imbalance during weightbearing radiographs commonly compensate by unloading the injured limb.
Conclusion
The wide variability of results in this study highlights the vast discrepancies in weightbearing radiography. As a modality that is imperative to make many appropriate diagnoses, awareness of the variability between patients and even radiographic views for any pathology is important to keep at the forefront of the clinician’s mind. Currently, the clinical impact of this specific data is unknown, as no conclusive literature exists to highlight the minimum weight required for a sufficient weightbearing radiograph. However, this study paves the way for more specific questions to be answered. In the interim, we advocate for technician and subsequently patient education to be prioritized when standardizing methods for obtaining weightbearing radiographs to best obtain the highest quality imaging and most accurate diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: V.K.P. is an editor for Lippincott Williams and Wilkins publisher and has received consulting fees, honoraria, and financial support for food and beverage, lodging, and education from Stryker Corporation, Trilliant Surgical, MedShape Inc., Paragon 28, Crossroads Extremity Systems LLC, 3D Systems, Medinc of Texas, DePuy Synthes Sales, and Integra LifeSciences Corporation unrelated to this study. The other authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was waived by The University of Texas Medical Branch Institutional Review Board (IRB 21-0104) because it falls into exemption category 2 in accordance with our institution’s policies:
Informed Consent
The study was determined to be exempt by the Institutional Review Board of the University of Texas Medical Branch (IRB # 21-0104), therefore informed consent was waived.
Trial Registration
Trial registration was not required for this study.
Consent to Participate
Not applicable.
Data Availability
Not applicable.