
Abstract
Introduction. Chopart injuries are often misdiagnosed due to subtle presentations affecting a combination of the talar head, navicular, calcaneus, or cuboid bone. These injuries typically occur on both medial and lateral sides, but rarely both structures at a single side are injured. The aim of this study was to investigate functional outcome and complications in Chopart injuries with a transnavicular-transtalar fracture pattern. Methods. This retrospective cohort study examined patients with Chopart injury with concomitant navicular and talar head fractures. Patient characteristics, trauma mechanism, fracture classification, surgical management, follow-up, and complications were reported. Functional outcome was assessed using the American Orthopaedic Foot & Ankle Society (AOFAS) score and Foot Function Index (FFI). Quality of life was measured with the EuroQol-5D (EQ-5D). Patient satisfaction and general health were scored on a 0–10 visual analogue scale (VAS). Results. Twenty-two patients with Chopart injuries with concomitant navicular and talar head injuries were included. Four common injury pattern combinations were identified based on anatomical affected structures. Most cases underwent ORIF. Two underwent primary arthrodesis of the talonavicular joint. Mean follow-up was 57.6 months. Secondary talonavicular arthrodesis due to painful osteoarthritis (n = 3) was performed after a mean of 12.3 months. Implants were removed in 47% due to complaints after a mean of 10.5 months. There were no postoperative wound infections or cases of avascular necrosis. All fractures showed union. Functional outcome was good (median AOFAS 80.6; median FFI 20.5). Mean EQ-5D index was 0.46. Patient-reported outcomes were good (mean VAS treatment satisfaction 8.4; mean VAS perceived health 8.1). Conclusion. There is a significant amount of diversity among Chopart injuries. If treated correctly, outcomes are good, although a substantial number of patients require secondary surgery. Considering the rarity and complexity of these injuries with concomitant foot fractures, prompt referral to specialized foot surgeons and centralization of complex foot surgery are recommended.
“Significant amount of diversity among Chopart injuries . . . if treated correctly, outcomes are good . . . prompt referral to specialized foot surgeons and centralization of complex foot surgery are recommended”
Introduction
The Chopart joint consists of the talonavicular (TNJ) and calcaneocuboid (CCJ) joints, along with several supporting ligaments. 1 - 3 Chopart joint injuries are often misdiagnosed because of subtle clinical presentation (on occasion) and reliance on radiographic findings.4,5
Injuries involving this midfoot complex may present as either fractures, dislocations, or a combination of both. The fractures around the CCJ and TNJ are situated in either the talar-head, navicular bone, anterior process of the calcaneus or the cuboid. These fractures frequently appear in combination, with usually 1 injury on the medial and 1 on the lateral side.4,6 -10 The talus and navicular bones are crucial for foot biomechanics, with the talus aiding in force distribution and weight-bearing, and the navicular stabilizing the foot’s arch and facilitating midfoot motion.11 -13
Chopart injuries can be classified based on the mechanism of injury, including combined compression and distraction forces, leading to ligament injuries or fractures on both sides of the foot.7,14 -16 In their 1975 study, Main and Jowett analyzed 71 cases of midtarsal joint injuries. 17 Fracture patterns varied depending on foot position at the time of impact (dorsiflexion or plantarflexion). Inversion caused navicular or talar-head fractures, while eversion led to calcaneal or cuboid fractures. Rotational forces caused swivel dislocations and plantar impacts led to dislocations with avulsions. Crush injuries produced irregular fractures and soft tissue damage. An additional 40% of injuries resulted from longitudinal (axial) forces.3,7,18,19
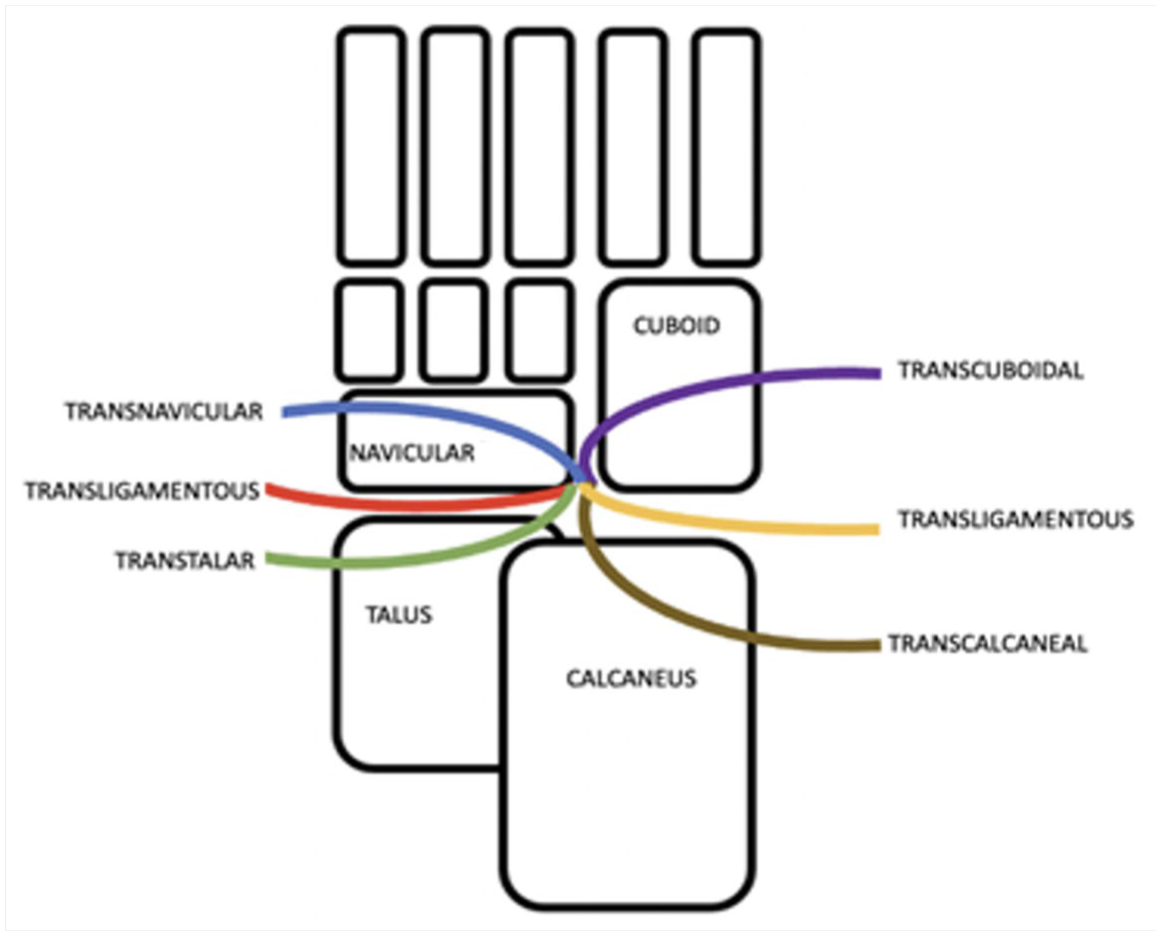
A more recent classification was proposed by Zwipp, where he divided Chopart injuries based on the affected anatomical structures (talus, navicular, calcaneus, cuboid, or ligamentous structures).3,20 Resulting in 6 groups: (1) Transligamentous, (2) Transtalar, (3) Transcalcaneal, (4) Transnavicular, (5) Transcuboidal, and (6) Combined injuries (Figure 1).
Most Chopart injuries involve a single injured structure per side, however a small amount may present with a combination of injuries on either the medial or lateral side. The concurrent occurrence of talar-head and navicular fractures rare and has been scarcely described in the literature.3,19,20
The primary aim of this study is to investigate the functional outcome and complications in transnavicular-transtalar Chopart injuries. The secondary aim of this study is to determine whether reducing the impaction of the talar head affects the outcome or complications.
Methods
Design and Patients
A retrospective cohort study was conducted on all trauma patients treated at our level 1 trauma center with an injury classified as transnavicular-transtalar according to Zwipp, between September 1, 2008, and January 1, 2025. Internal Review Board approval was obtained (number W19-247).
These bifocal single joint fractures were defined as a medial Chopart injury with intra-articular navicular bone fracture with concomitant talar head impaction or shear fracture involving the articular surface, not involving the talar neck. All injuries were diagnosed by conventional radiographs and subsequent computed tomography (CT) scan.
Inclusion criteria were age of at least 15 years at the time of injury and follow-up of at least 12 months. Patients with a bifocal single joint injury of the lateral Chopart (transcalcaneal-transcuboid; processus anterior of the calcaneus and concomitant intra-articular cuboid fracture) were excluded from this study.
Variables
Three categories of characteristics were extracted from the patient charts. Patient characteristics: age at injury, gender, body mass index (BMI), and smoking status. Fracture characteristics: the injury mechanism, open or closed fractures, Zwipp classification, type of navicular fractures, type of talar head fractures, data on dislocation of the TNJ and injury severity score (ISS). The last category was surgical characteristics, data extracted was whether the talar head injury was surgically addressed, the use of bridge plating, need for secondary arthrodesis due to osteoarthritis, complications like wound complications, the removal of implants and time to surgery.
Patient-Related Outcome Scores
The functional outcome was assessed using a validated questionnaire where the Foot Function Index (FFI) and the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score were described. The best score of the FFI is 0 points. The best score of the AOFAS is 100 points. The AOFAS was divided into groups based on literature: 90–100 points were graded as excellent, 75–89 points were graded as good, 50–74 points were graded as fair and less than 49 points were graded as poor outcome or a failure. Quality of Life (QoL) was scored on the EuroQol-5D questionnaire. Patient satisfaction was measured using a visual analogue scale (VAS) of 0-10, whereas 0 represents zero satisfaction and 10 represents the best possible satisfaction. VAS was also used to assess general health (10 represented excellent general health).
Statistical Analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 29 (SPSS, Chicago, IL). Numeric data are expressed with means with standard deviation (SD) in case of symmetrical distribution, or median with range for skewed data. Categorical data are shown as numbers with percentages. Independent sample t-tests and analysis of variance (ANOVA) with a significance level of .05 were used to compare means for variables including functional outcome, QoL, treatment satisfaction, and perceived health.
Results
Demographics
From a database of 129 operatively treated Chopart injuries, a total of 84 were identified to have had surgical treatment of the navicular bone. Out of these, 25 patients with 26 feet (1 bilateral injury) had a combined talar head and navicular injury. Of these 25 patients, 2 were excluded because of missed injury and subsequent delayed referral. One of the patients died during follow-up due to an unrelated cause. Excluding these 3 patients resulted in a study cohort of 22 patients with 23 injured feet.
Half of the patients were male (n = 11 out of 22, 50%). The mean age at the time of injury was 28.5 years (SD 10.3). Most of the patients were referrals (n = 17 out of 22, 77%). The mean BMI of the patients was 23.9 (SD = 4.2) and 22% of patients reported tobacco use (n = 5 out of 22).
Out of 22 patients, 20 patients (with 21 injured feet) had a minimal follow-up time of 12 months and were thus eligible for inclusion for functional outcome assessment. Eighteen patients (with 19 injured feet) completed the questionnaire, yielding a follow-up rate of 83%. The mean follow-up time from the day of trauma was 57.6 months (SD 46.5). Injury characteristics are described in Table 1.
Overview of Included Patients Who Have Concomitant Talonavicular Injuries, With or Without Additional Injuries.
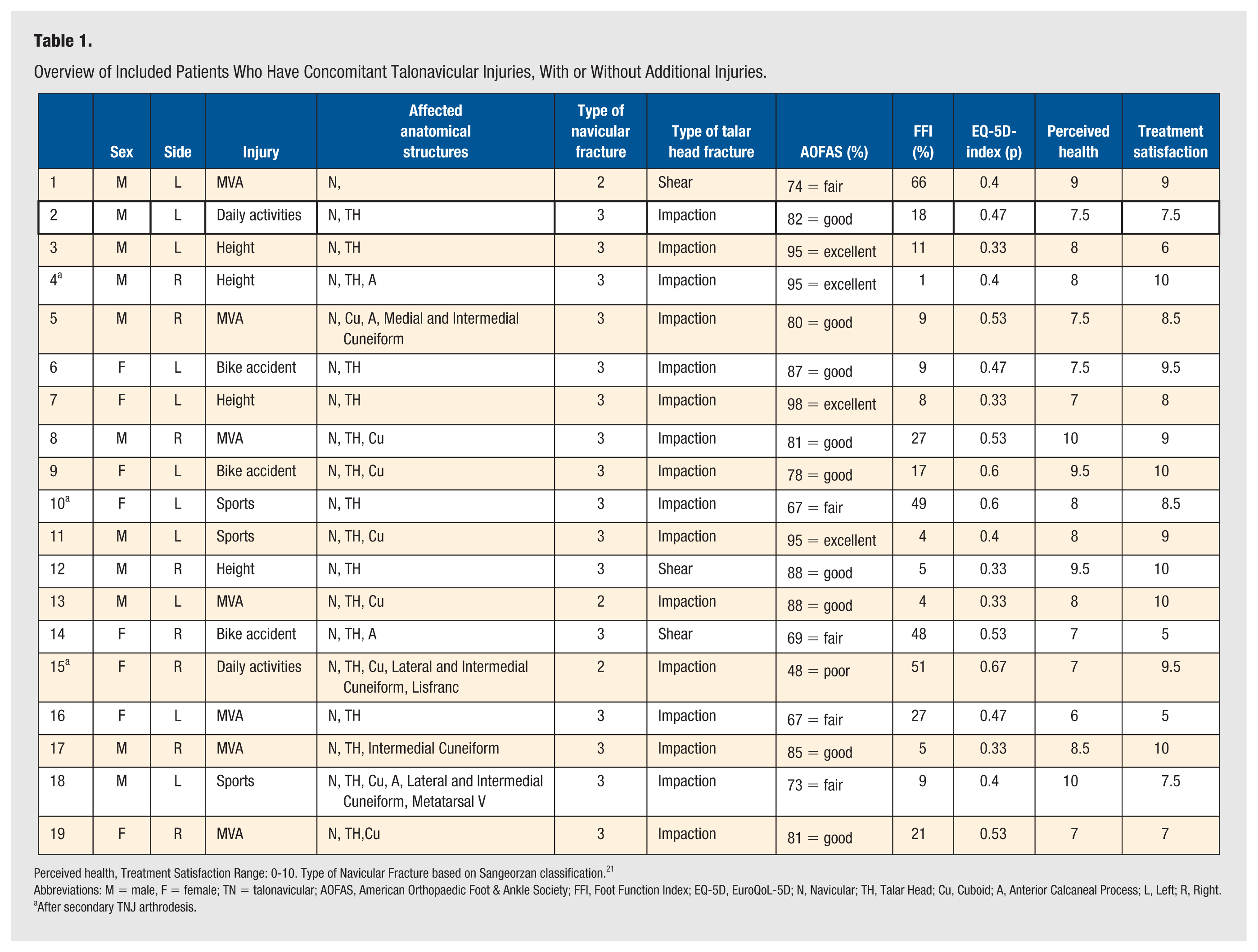
Perceived health, Treatment Satisfaction Range: 0-10. Type of Navicular Fracture based on Sangeorzan classification. 21
Abbreviations: M = male, F = female; TN = talonavicular; AOFAS, American Orthopaedic Foot & Ankle Society; FFI, Foot Function Index; EQ-5D, EuroQoL-5D; N, Navicular; TH, Talar Head; Cu, Cuboid; A, Anterior Calcaneal Process; L, Left; R, Right.
After secondary TNJ arthrodesis.
Fracture Classification and Injury Pattern
The mechanism of injury were motor vehicle accident (n = 7 feet), (electric) bike accident (n = 5 feet), fall or inversion during daily activities (n = 3 feet), fall from height (n = 5 feet), and sports-related incidents (n = 3 feet). There were no open fractures. Mean ISS was 4.6 (SD 2.8). All injuries were classified using both conventional radiography and CT imaging.
Most patients had a talonavicular joint dislocation (n = 14, 61%). Twelve cases required open reduction. One case was reduced under sedation in the emergency department. In 1 case, closed reduction was attempted intraoperatively using K-wires; however, due to persistent subluxation, open reduction was subsequently performed.
All patients suffered talonavicular fractures with concomitant ipsilateral foot injuries. Chopart injuries were classified using the Zwipp classification, see Figure 1. Four combinations of Chopart injury-patterns were identified: transtalar and transnavicular only (n = 11 out of 23), transtalar, transnavicular and transcuboidal (n = 8 out of 23), transtalar, transcalcaneal, transnavicular and transcuboidal (n = 3 out of 23) and transnavicular, transtalar and transcalcaneal (n = 1 out of 23). The types of navicular and talar head fractures are listed in Table 1.
Management
Prior to definitive surgery, 4 injured feet were temporarily treated with external fixation. Definitive surgery was aimed at restoring the joint in 21 feet. Two feet underwent primary arthrodesis of the TNJ, because of extensive, unsalvagable cartilage damage diagnosed peroperatively. Mean time between trauma and surgery was 9.8 days (SD 5.3).
Depending on the type of talar head injury, the following method for fracture reduction and disimpaction of the talar head was used. Shear fractures were reduced using osteotomes and small K-wires as joysticks and subsequent temporary fixation. Headless screws of 2.0 to 2.4 mm were used subsequently. Impactions were reduced using drill holes proximally from the impaction in the neck. The tip of a 2.0 mm K-wire was bent and used to disimpact the impaction fracture. The hole was grafted and just proximal of the fracture two 2.0 or 2.4 mm screws were placed to stabilize the fracture. Patients with persistent TNJ dislocation also had some degree of rotational dislocation at the subtalar joint, which was reduced after reducing the TNJ. No additional stabilization of the subtalar joint was required.
In patients treated with Open Reduction and Internal Fixation (ORIF), most fractures were fixed using a 2.7 mm navicular plate or a 2.0 mm generic T-plate and screws (n = 9), navicular plate and bridge plate of the talonavicular joint (n = 3), single bridge plate of the TN-joint (n = 2) or a navicular plate and/or bridge plate with additional temporary K-wires (n = 4). Two case are presented in Figures 2 and 3. The mean interval between bridge plate insertion and removal was 244 days (SD = 180.5). Reconstruction of the talar head with a graft was performed in 5 patients.
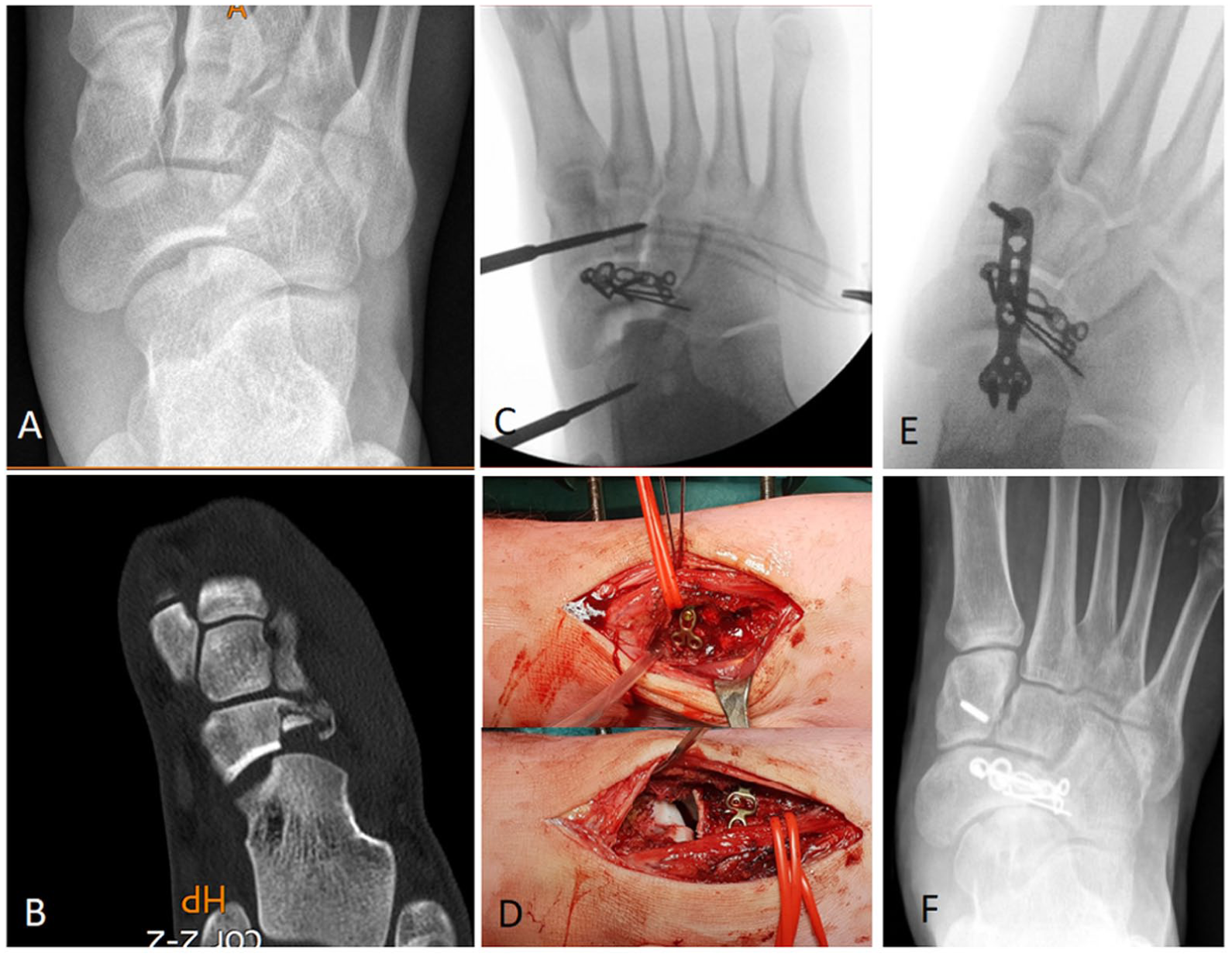
16-year old male patient with transnavicular-transtalar Chopart injury. (A) Preoperative AP radiograph showing talar head impaction and lateral navicular fracture. (B) Preoperative CT-scan. (C) Reconstruction and fixation of lateral navicular fracture. (D) Peroperative images showing talar head impaction. (E) Bridge plate after reduction of talar head fracture and absorbable pin fixation. (F) Follow-up radiograph after 2 years.
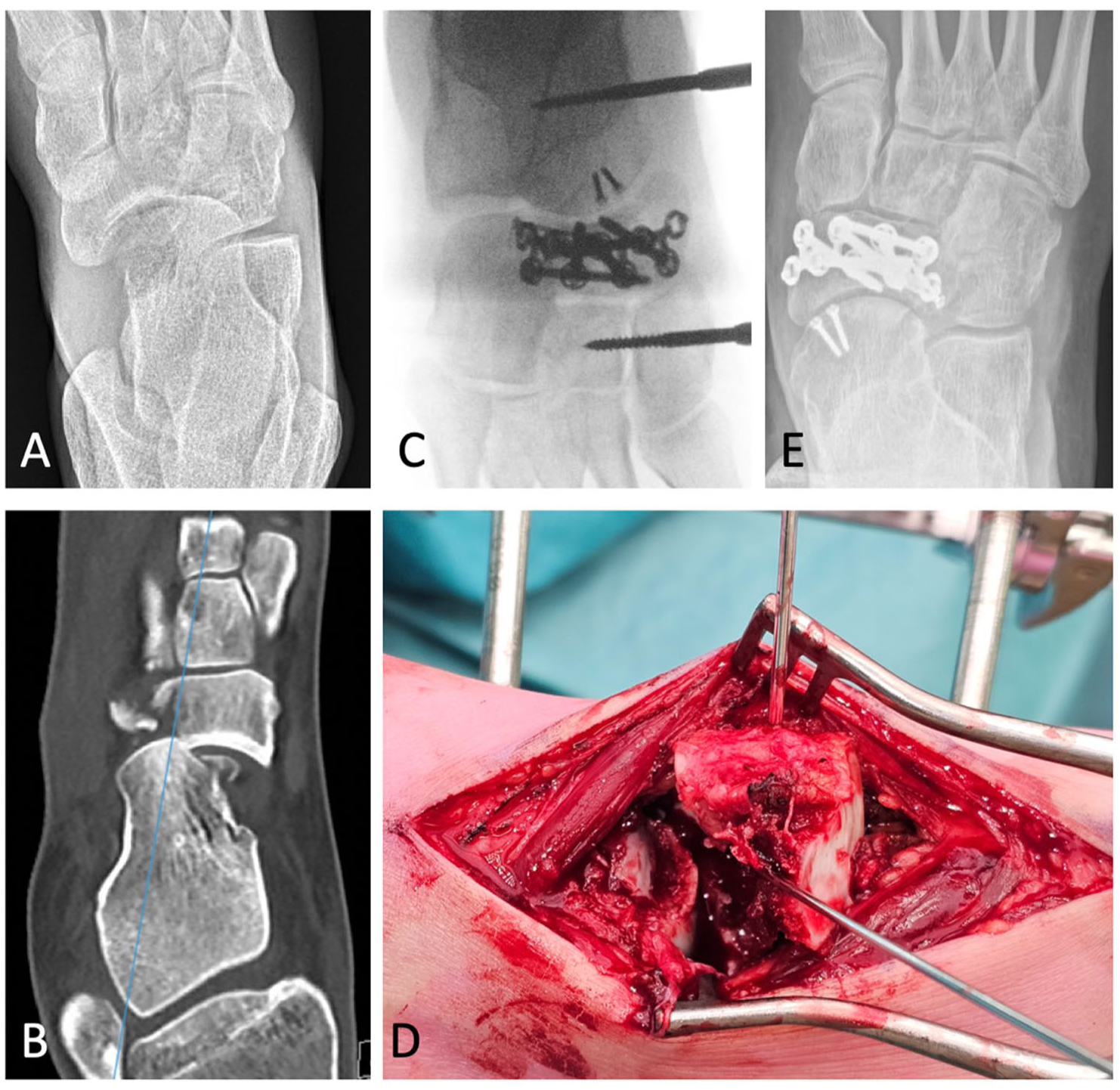
21-year old female patient with transtalar-transcalcaneal-transnavicular Chopart injury. (A) Preoperative AP radiograph showing talar head shear with central and lateral navicular fracture. (B) Preoperative CT-scan. (C) Disimpaction, reconstruction, fixation of talar head (2× 1.5 mm screw) and navicular fracture (VA foot plate). (D) Peroperative images showing talar head shear and navicular impaction. (E) Follow-up radiograph after 1.5 years.
All patients underwent postoperative immobilization in a cast for a period between 6 and 8 weeks. Temporary K-wire fixation was used in 4 cases; the wires were removed after 6 weeks in 3 patients and after 8 weeks in 1 patient. In the majority of cases (n = 15), weight-bearing was initiated immediately following cast removal. In the remaining patients, a gradual weight-bearing protocol was applied, either commencing during the period of immobilization (n = 3) or postponed until complete cast removal, depending on fracture stability and soft tissue condition.
Complications
After primary surgical treatment, union was achieved in all 19 feet. There were no postoperative wound infections and no avascular necrosis was observed. One patient had dislocation of the TNJ after surgery, and therefore the patient underwent closed reposition without surgical re-fixation. Implants were removed in 47% of treated feet due to complaints. Mean time to implant removal was 10.5 months (SD 13.2). None of the patients suffered from loss of alignment of the TNJ, nor loss of arcus. Secondary arthrodesis (SA) of the TNJ due to painful osteoarthritis with functional impairment was performed in 3 feet after a mean time of 12.3 months after primary surgery (SD 2.5). Another patient with painful TN osteoarthritis, following reconstruction of both the navicular and talar head with temporary bridge plating, a fascia lata interposition TNJ arthroplasty was performed at 78 months after primary surgery to maintain function and reduce pain. However, this was only done last month and the patient’s functional outcome scores were obtained prior. Outcome scores are described separately for patients with and without SA.
Functional Outcome, QoL, and Other Patient-Reported Outcomes
In patients without SA, overall AOFAS was good (mean: 82.6, SD 9.2, n = 16), scores were categorized as excellent (n = 3), good (n = 10), and fair (n = 3). The mean FFI was 18.0 (SD 17.3). The mean EuroQoL-5D-index was 0.66 (SD 0.1). The mean treatment satisfaction scored on VAS-scale per feet was 8.2 (SD 1.7). The mean score of perceived health, scored with a VAS-scale, was 8.1 (SD 1.2). With the numbers available, using independent samples t-tests, no significant differences were detected in outcome scores (functional, QoL, health, and satisfaction) between male and female, with or without tobacco use, BMI, or the presence of joint dislocation.
In terms of daily activities, one patient was unable able to walk barefoot. The majority of patients reported stiffness of the injured foot (n = 14, 74%), limited to morning only (n = 9, 47%) or permanent (n = 5, 26%). All patients returned to work (n = 18, patients who worked prior to trauma), of which one patient had to change the type or intensity of work. In total, 73% of the patients was able to return to the same level of sports (n = 11 of 15 who performed sports prior to trauma).
In 3 patients who underwent SA, overall AOFAS was fair (mean: 70.0, SD 23.6, n = 3), scores were categorized as excellent (n = 1), fair (n = 1), and poor (n = 1). The mean FFI was 33.7 (SD 28.3). The mean EuroQoL-5D-index was 0.56 (SD 0.1). The mean treatment satisfaction scored on VAS-scale per feet was 9.3 (SD 0.8). The mean score of perceived health, scored with a VAS-scale, was 7.7 (SD 0.6). In terms of daily activities, two patients struggled to walk barefoot. Two out of 3 patients had stiffness of the injured foot. All patients returned to work and to the same level of sports.
Discussion
Chopart injuries are amongst the most severe foot injuries.7,22 In this series, we described a subset of Chopart injury with a transnavicular-transtalar fracture pattern as defined by Zwipp.10,11 Subdivision of Chopart injuries may facilitate future comparisons of outcome, though smaller subgroups complicate statistical analysis due to limited numbers.
As shown in Table 1, about half of the patients with this subtype sustained concomitant ipsilateral foot injuries. According to the Main-Jowett classification, these were mostly medial swivel dislocations, though some resulted from axial load mechanisms. 17 With respect to the incidence of navicular fractures in patients with a talar head fracture, this was previously reported between 18.8% (Hammarberg et al, 18 n = 6/32) and 47.6% (Engelmann et al, 2 n = 10/21).
Given the broad range of possible associated injuries in our series, it is impossible to present a general surgical plan or provide detailed recommendations on how to reduce and fix talonavicular injuries. In general, patients were primarily managed with ORIF. In case of talonavicular joint instability, ORIF is recommended to restore articular congruency. 23 The navicular fracture was usually treated with a 2.7 mm anatomical plate or with a 2.0 mm plate in case of a comminuted fracture of the lateral portion of the navicular bone.
Reconstruction of the talar head in these medial swivel dislocations has been described as early as 1990. 24
In 5 of our cases, the talar head was amendable to disimpaction and fixation either with a small plate, screws only, or in case of comminution a bridge plate for 4 months. From this group, 2 patients eventually required secondary talonavicular fusion. None of the patients in whom the talar head injury was too small or too comminuted to reconstruct required a secondary arthrodesis. It might be surprising that those amenable to reconstruction of the talar head needed secondary fusion. This might be due to the fact that these patients had larger impaction injuries of the talar head, which may have caused more severe cartilage damage. Regardless of the management type, about 80% of our patients returned to their normal daily activities during long-term follow-up.
In management of the fractures with ORIF, some patients were treated with temporary K-wires while others were treated with a bridge plate across the talonavicular joint. Although K-wires can be easily removed in the outpatient clinic, their transarticular placement may cause articular damage. Alberta et al 25 reported that both transarticular screws and dorsal plates effectively realign the first and second tarsometatarsal joints, but screws may cause measurable damage to the articular surfaces, thereby increasing the risk of post-traumatic arthritis. Dorsal plating is suggested as a viable alternative that could reduce complications associated with screw fixation, such as hardware removal difficulties. K-wires, being one-third the diameter of a screw, may cause less articular damage, though this has not been studied in foot surgery.
Similar to the TNJ bridge plating technique we used, Xi Hua et al 26 evaluated 2 surgical strategies for treating fractures of the anterior process of the calcaneus with calcaneocuboid (CC) joint injury, specifically comparing “not-across” and “across” CC joint plate fixation techniques. The “not-across” (no bridge plate) CC joint plate fixation (group NA) demonstrated significantly better early functional recovery compared with the “across” CC joint fixation (group A). This was assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) score and visual analogue scale (VAS) pain score, with group NA showing superior results at 1 month postsurgery. In our study, sample size was too small for subgroup analysis.
With respect to functional outcome, the AOFAS score in this cohort (mean 80.6, SD 12.1) corresponds to previous literature (Schmid 79 points, Richter 75 points, Rammelt 72 points).7,22,27 This indicates that even though transnavicular-transtalar fractures are severe injuries, acceptable results may be obtained after adequate treatment. Schmid et al 27 demonstrated that patients with navicular fractures without talar head injury (AOFAS 86) scored better than patients with talar head involvement (9 out of 24 patients, AOFAS 79). Rammelt and Missbach 7 reported long-term outcomes for patients with Chopart injuries, assessing functional outcome using the FFI. At an average follow-up of 10.1 years, the FFI was 26.9, indicating significant functional impairment. Factors such as high injury severity, multiple fractures, and delayed treatment negatively impacted the outcomes, with open reduction and internal fixation yielding better results than other methods. Similar to the literature, mean FFI was 20.5, indicating some functional impairment.
Limitations
Strengths of the current study are related to use of validated patient-reported outcome instruments and long-term follow-up. The patients in this study outnumber the sample size of previous studies published in the English and German language. Results may be skewed by the fact that the worst injuries were referred to our academic, foot and ankle trauma expertise center. In addition, twelve of the patients suffered additional foot injuries that are likely to influence outcome. There is potential bias due to the very low incidence of talonavicular fractures, which led to a retrospective design, small sample size and the lack of a comparable control group. The present study included a heterogeneous cohort comprising a wide range of fracture and dislocation patterns of the talonavicular joint. While this reflects the variability encountered in clinical practice, it introduces heterogeneity that may impact the interpretation of outcomes. As such, caution is warranted when extrapolating these results to specific injury subtypes. Future investigations focusing on more homogeneous injury patterns are required to provide generalizable evidence. Future international registration of these rare injuries may improve research opportunities aimed at evaluating operative treatment and outcome.
Conclusion
Chopart injuries involving fractures of the navicular and talar head are rare and often occur in combination with other fractures. Adequate treatment including early reduction and stabilization may result in acceptable functional outcome. Addressing the talar head impaction did not improve functional outcome, nor did it prevent secondary arthrodesis in this small series. Due to the low incidence and high complexity of the talonavicular fractures, early referral and diagnosis by experienced foot surgeons and centralization of the complex treatment is recommended.
Footnotes
Author Contributions
Study conception and design (Schepers, Halm, Engelmann). Acqusition of data (Engelmann, Meelen). Analysis and interpretation of data (Meelen, Engelmann). Drafting of manuscript (Meelen). Critical revision of manuscript (Schepers, Halm, Engelmann).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Internal Review Board approval was obtained (number W19-247).
Consent to Participate/Publication
Verbal and/or written consent was obtained from all patients, included in this study.