
Abstract
Background:
Evidence concerning the complex foot trauma, especially its definitive management, is scarce. Soft tissue envelope sequalae are the primary parameters that delay or make internal fixation implausible. Stability conferred by external fixators makes them a reasonable initial treatment choice. Although AO or circular fixators can be applied around the foot, this can involve a learning curve and substantial costs, especially for the circular fixator. There is little evidence as to how well external fixators work as a definite method of fixation in patients where progression to internal fixation cannot be made.
Methods:
We prospectively evaluated 10 adult patients with severe and complex foot trauma who were consecutively treated at our clinic. Initial reduction and stabilization were performed with an external fixator that was initially conceived for distal radius fractures, applied during the initial procedure and mantained throughout the treatment.
Results:
Fracture healing was obtained in all 10 cases, and both internal and external column length was restored. One of the patients developed chronic osteomyelitis. At the 1-year follow-up visit, these patients averaged 45.6 points in the physical and 44.8 points on the mental status sections of the 12-Item Short Form Health Survey (SF-12). The Foot Function Index findings for pain, disability, and daily activities limitations were 33.3, 39, and 41.5, respectively, which suggest moderate residual impairment.
Conclusion:
In this relatively small case series of complex foot trauma, we found that the use of simple external fixation as definitive treatment worked reasonably well.
Level of Evidence:
Level III, prospective cohort study.
Introduction
There is currently no universally accepted best practice for the initial treatment of complex foot trauma, which is characterized by fractures, joint dislocations, and significant damage to soft tissues. 20 In this scenario, most of the time, the soft tissue condition is the element that delays definitive treatment and compromises the function of the region. Considering this fact, the leading treatment objective should be restoring the medial and lateral column length while achieving a correct relationship between the hindfoot and the forefoot while maintaining adequate stability. 17 This considers that the elected system must also allow the control of the soft tissue and wound progress and the successive need for surgical debridement without compromising the acquired stability.
To meet this purpose, multiple stabilization methods are habitually used: K-wires, casts, and external fixators. Kirchner wires entail the disadvantage of potential migration and pin track complications. Casts, on the other hand, may not offer optimal stability and make it difficult to evaluate the progression of wound healing. In this sense, the increased stability offered by external fixators makes them the most effective initial treatment choice. 5 Its use allows for better soft tissue management and wound healing progression, adding to the well-established effect of enhanced stability on this phenomenon. An additional advantage of the external fixators is that in the case of being unable to perform definitive reconstructive surgery, internal fixation, or arthrodesis, they allow for maintaining foot alignment and even fracture healing.2,5 The external fixator employed in our patient group offers an added benefit by enabling pins to be placed in multiple directions, enhancing the flexibility of the overall structure. The purpose of this study is to present the preliminary results of our first prospective cohort treated definitively with a novel external fixator in the context of complex foot trauma.
Material and Methods
With previous ethics committee approval, a prospective cohort study was carried out, including consecutive complex foot trauma patients who sought attention in our trauma center from January 2020 to July 2022. Adult patients with complex foot trauma as an isolated injury or in the polytrauma context that could not be converted to internal definitive fixation, and in whom the external fixator was the initial and definitive treatment, were included. Those patients with previous sequelae from foot trauma, diabetic patients, and those who received definitive internal fixation were excluded.
Severe or complex foot trauma (CFT) was defined as the one that implies the presence of fracture or fracture-dislocation of 1 or more foot joints associated with a severe compromise of the soft tissue, achieving more than 5 points in the proposed score by Zwipp et al, 20 which is a scaling system based on the level of skeletal injury and grading of tissue trauma. 10 Bony lesions were characterized by the AO classification. 19 The severity of soft tissue compromise was analyzed with the Tscherne scale 7 for closed lesions and Gustilo and Anderson 6 for the open ones.
The same surgical team performed all procedures. Evaluation on arrival consisted of anteroposterior (AP), lateral (L), and oblique projections nonweightbearing radiographs of the foot. Subsequently, computed tomographic (CT) images were obtained (Toshiba Activion 16-track multislice) to observe the fracture or fracture-dislocation personality. Once in the operating room, the decision not to perform a primary amputation was taken based on the Mangled Extremity Severity Score 4 and the Hannover Fracture Scale 3 plus the surgeon's perspective on the ability to achieve a stable construct and to cover the soft tissue defects.
All patients with open fractures or fracture-dislocation received a first dose of intravenous antibiotic on arrival, according to our existing protocol. In grade I and II patients, the antibiotic was cefazolin for 48 hours, and in grade III patients, gentamicin for 72 hours.1,19 In patients with closed lesions, the prophylactic antibiotic was formulated with 1 g of cefazolin during anesthetic induction.
In those cases, fracture-dislocation of the foot, closed reduction, and posterior stabilization with a monolateral external fixator (in a mono- or biplanar fashion) were carried out. This external fixator was originally conceived for extraarticular wrist fractures. 11 In more severe cases, with extensive comminution and alteration of the foot morphology, lateral and medial column length was prioritized, and so was the relationship between the hindfoot and forefoot. In those cases, with more simple patterns, anatomic reduction was preferred. In cases with open lesions, a thorough washout was carried out. Criteria of a compartmental syndrome (tensioned hematoma of the dorsum of the foot, slowing down of the capillary filling, and or intense pain when passively dorsiflexing the toes) 13 were carefully evaluated in closed lesions when those findings were positive, and a medial or dorsal fasciotomy was performed according to the affected compartment.
When primary wound closure was impossible, a vacuum-assisted closure system (Renasys Touch; Smith & Nephew, Sant Joan Despi, Barcelona) was used to achieve provisional closure, and in turn, a local flap was performed within the first week.
Patients who showed poor wound healing progression or signs suggestive of deep infection were taken back to the operating room for the appropriate debridement and sample collection. 10 Bone infection related to foot fractures was defined as the presence of 2 positive cultures for the same pathogen. 10
External Fixator Characteristics
This fixator can be used as a mono- or biplanar device measuring 70 mm in length by 10 mm in width. It has a head articulated to a body through a screw, on which it pivots (Figure 1). When adjusted, it is securely fixed in the desired position. The tutor has 6 holes. The articulated head has a triangular shape and features 3 holes inclined at 45 degrees to the tutor’s axis. The body has 3 holes, 2 of which are proximal and perpendicular to its axis and the third one is larger and intended for inserting an accessory pin, which can be oriented in a polyaxial manner (angular adjustment of up to 15 degrees). All the holes are regulated by a headless screw with a hexagonal adjustment slot, Allen type.
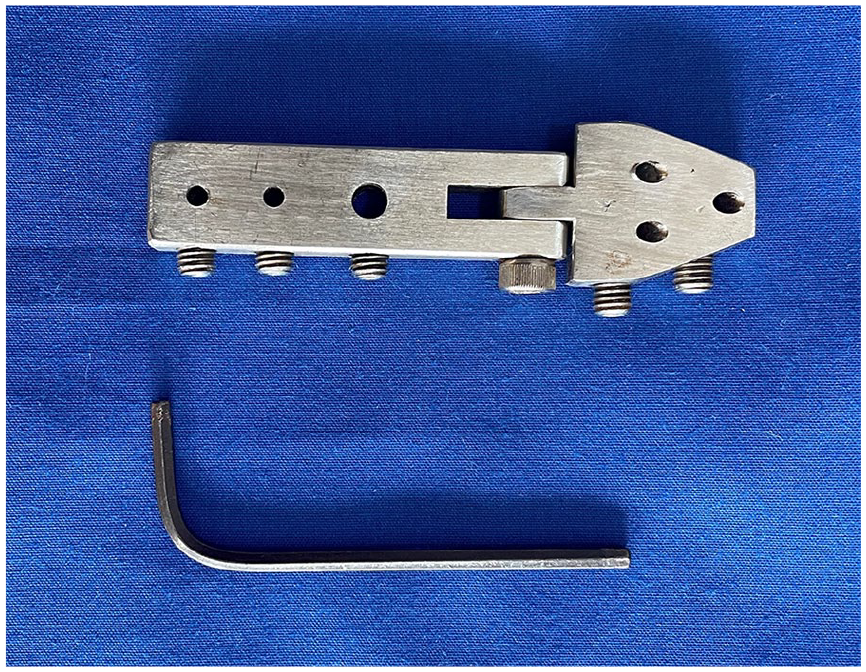
External fixator consisting of a mono or biplanar device measuring 70 mm in length by 10 mm in width. It has a head articulated to a body through a screw, on which it pivots.
Surgical Technique
The patients were positioned in a dorsal decubitus position. In all cases, dislocations were reduced and the affected foot columns were realigned through careful manipulation. Initially, this was done in a closed manner, and if it could not be achieved, open reduction was performed. External fixator stabilization was carried out based on the location of the injury and the affected columns:
In cases involving the forefoot and midfoot with the involvement of the medial column, the fixator was placed parallel to the first ray (Figure 2A). For those affecting both columns, the fixator was positioned dorsomedially oblique to the first ray, with the fixator head tilted at an angle of about 20 to 25 degrees to achieve biplanar stabilization (Figure 2B). In both cases, 2 to 3 distal and proximal Kirchner wires (1.5-mm) were used through the fixator, passing through both columns (Figure 2C). Finally, when the dislocations were reduced or the length of any of the columns of the foot was restored, the configuration of the construct was completed through 2 more pins to the body and 2 to the head of the external fixator (Figure 3).
For injuries in the hindfoot, the fixator was placed vertically, with the proximal head in the coronal plane of the posterior region of the calcaneal tuberosity. In all cases, 2 pins (2-mm each) were inserted through the holes in the fixator head into the talus, and 2 to 3 pins (2-mm) were placed in the calcaneus through the holes in the fixator body. In cases of comminution, the fixator head was tilted at an angle of about 20 degrees so that the calcaneal pins would stabilize the coronal plane (Figure 4A and B). In combined cases of injuries to the talus and calcaneus, only 1 fixator was utilized. When a fracture dislocation of the ankle was present, an additional AO delta frame was placed, in a usual fashion, before placing the foot fixator, although this was only necessary in one of the patients.
All patients remained hospitalized for at least 7 days, depending on accompanying injuries and intravenous treatment as per the microbiological findings. Discharge was granted after completing the intravenous antibiotic therapy period prescribed by the infectious disease department and achieving good pain control with adequate soft tissue coverage. Patients were evaluated weekly, and during the fourth week, front and lateral nonweightbearing radiographs were requested. Between the eighth and ninth weeks, if 3 of 4 cortices were consolidated, the external fixator was removed, and anteroposterior and lateral radiographs were taken with weightbearing as tolerated. Patients were assessed monthly for up to 12 months following the procedure. The time to wound healing was determined as the point at which the patient no longer required wound care, coinciding with the appearance of skin wrinkles.

(A) Foot model depicting the configuration intended in function of the lesion location. When the involvement is located onto the forefoot and midfoot and/or the medial column, the fixator was placed parallel to the first ray. (B) For those affecting both columns, the fixator was positioned dorsomedial oblique to the first ray. (C) In both cases, 2 to 3 distal and proximal Kirchner wires were used, passing through both columns. (D) Illustrates the biplanar configuration of the fixator by flexing the head approximately 45 degrees to allow for the placement of one kirchner wire in the coronal plane and another one in the sagittal plane.

Once finally, the length of the columns of the foot was restored, the configuration of the construct was completed through 2 more pins to the body and 2 to the head of the external fixator.

(A, B) For injuries in the hindfoot, the fixator was placed vertically, with the proximal head in the coronal plane of the posterior region of the calcaneal tuberosity.
The Foot Function Index (FFI) 12 and quality of life were assessed using the SF-12 questionnaire for the clinical evaluation at the 1-year follow-up visit. 9
Results
The initial series consisted of 15 patients. In 5 among those cases, the transition to definitive osteosynthesis was performed because of good soft tissue healing. In the remaining 10 patients, the external fixator was used as the definitive treatment, and these patients were included and analyzed in the study. Among them, 4 patients were female and 6 were male, with 7 right feet and 3 left feet. The average age was 38.1 years (range 25-54 years) (Table 1).
Demographic Characteristics of the Patients Presented in the Study.

The locations of the injuries were as follows: 3 cases in the hindfoot, and 3 forefoot lesions, one of them additionally compromising the navicular and Lisfranc joint; 4 patients sustained injuries to the midfoot, one of which was an isolated Gustilo III A navicular fracture due to a gunshot wound. The rest were combinations of Lisfranc and navicular, Lisfranc and chopart (Figure 5), or navicular and ankle involvement (Table 2).

Young adult male patient who sustained a motorcycle accident. (A, B and C): radiographs and photographs taken at arrival depicting severe open dislocation compromising the tarsometatarsal, chopart, and ankle joint. (D, E, and F): radiographs and photographs at initial reduction and stabilization with the external fixator.
The General Evolution of the 10 Patients.

Abbreviations: D, disability; FFI, Foot Function Index; L, daily activities; MTPJ, metatarsophalangeal Joint; NPWT, negative-pressure wound therapy; OA, Osteosynsthesefragen Arbeitsgemeinshaft für; OM, osteomyelitis; P, pain.
Three cases were closed injuries, all type III according to the Tscherne classification. Seven cases were open injuries, including 4 Gustilo IIIB, 2 Gustilo IIIA, and 1 Gustilo II. Six patients healed primarily through primary closure in the initial procedure. On the other hand, in the 4 cases where soft tissue defects were observed, 1 patient was treated with advanced wound care (initially calcium alginate and later hydrogel), achieving complete epithelialization secondarily. In the remaining 3 cases, negative pressure wound therapy systems, along with multiple wound dressings, were used for 15-30 days, followed by advanced wound care until final epithelialization in 2 cases. An extensor digitorum brevis pedicle muscle flap was required in the remaining case.
The microbiological findings for the 7 open lesions at the second look were as follows: 4 cases of methicillin-sensitive Staphylococcus aureus (MSSA), 2 of them associated with Staphylococcus epidermidis. Three cases of methicillin-resistant S aureus (MRSA), 1 of them associated with Klebsiella pneumoniae, and 1 case of coinfection between Escherichia coli and Pseudomonas aeruginosa.
In all patients, fracture healing was achieved, and medial and lateral column lengths were restored. One of the patients developed chronic osteomyelitis (case 3). The average raw scores for the physical and mental aspects of the SF-12 questionnaire were 45.66 points and 44.80 points, respectively. Regarding the functional impact on the foot, the average scores for pain, disability, and limitations in daily activities in the FFI were 33.3, 39, and 41.5, respectively.
Two of the 3 patients with injuries in the forefoot (involving the metatarsophalangeal joint of the hallux) showed signs of osteoarthritis in radiologic studies (hallux rigidus grade II). Among the 3 cases with hindfoot involvement, 2 had symptoms of posttraumatic arthritis with a Ramelt type III sequela. 16 One of them developed chronic osteomyelitis, which was treated with suppressive antibiotic therapy. The remaining case had a mild depression of the posterolateral facet, which, from a clinical perspective, did not cause functional limitations in basic daily activities. Among the patients with midfoot involvement, only 1 patient presented with posttraumatic arthritis of the central and lateral columns of the Lisfranc with slight metatarsal adduction (Figures 5A-F and 6). In no case did we observe intolerance to the fixator pins.

Radiographic and photographs of clinical alignment taken at 1-year follow-up.
Discussion
Treatment of patients with complex foot trauma involves extended periods of interventions, and if a deep infection occurs, the number of procedures needed for definitive reconstruction can multiply, leading to a significant economic impact. 12
Although multiple treatment strategies have been proposed, ranging from immobilization with casts to open reconstructions, 15 the fact remains that there is currently no universally accepted standard for treating this condition. In this regard, one possibility is to perform a staged procedure, with the premises of initially realigning the foot and achieving adequate stability. Doing so with a method that also allows for monitoring the progression of soft tissues is of utmost importance. For this purpose, the initial and temporary use of external fixators has, at least in theory, several advantages concerning the care and healing of traumatic wounds. 21
Although comparisons between K wires and external fixators in the acute and temporary setting of an ankle fracture dislocation were published with similar results in terms of skin necrosis, redislocation of the ankle, surgical wound infection, and posttraumatic ankle osteoarthritis frequency were not significantly different between the groups, except for pin-site infection (P = .036). 18
In a similar sense, the mini Ilizarov external fixator may appear as an alternative since in addition to stability, it can distract, compress, 8 and neutralize, which allows it to expand indications and even to use it as a definitive method, although it does not seem to have multidirectional pin options, which we believe is an advantage in our fixator. 8
In certain possible developmental scenarios in these injuries, such as the presence of severe soft tissue defects, deep infectious processes (even osteomyelitis), uncooperative patients with multiple comorbidities, or polytrauma patients requiring life support due to central injuries, the external fixator can indeed be considered as the definitive treatment, as was the case in our group of patients.
Although in the context of severe trauma and other locations, these systems are widely described and even standardized to some extent, there are still limited records of the use of external fixators in foot trauma. 11 Furthermore, currently, the data registry regarding functional outcomes in the treatment of complex foot trauma is limited.11,16
In a series similar to ours, Marchesini et al 14 evaluated a group of 27 patients who sustained complex foot trauma and reported an average SF-12 score at 12 months of follow-up of 37.9 (physical component) and 45.2 (mental component). In this patient group, the FFI revealed that the average pain score was 49%, the average disability score was 53%, and the average activity limitation score was 37%, indicating persistent pain with significant residual disability.
Evidence regarding the treatment of acute severe foot trauma is still far from robust. However, despite this, our initial experience with the definitive management of this condition shows promising results. Although our series is small and has a short follow-up period, which does not allow for inferential statistics and thus conclusion, 2 characteristics related to the technique are particularly noteworthy:
The relative simplicity of placement, which allows for a small learning curve.
The versatility provided by the multidirectionality of the pins makes it possible to adapt to multiple areas of the hindfoot, midfoot, or forefoot in 1 or 2 planes, as well as the ability to create different assemblies as needed for greater stability.
Concerns may arise about pin-track infections. Fortunately, this was not a complication we found in our small group of patients; in any case, this potential risk may also be present with the use of K-wires alone. In the case of need, pin replacement in a different location may be able to be carried on without altering stability.
Conclusion
It is our perspective that the spectrum of midfoot lesions that we present could constitute a strength of this study, appealing to the versatility of the fixation device in different settings. Our initial observations suggest potential benefits in managing complex foot trauma with this approach.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241265113 – Supplemental material for A Novel Uni- and Biplanar External Fixator for Initial and Definitive Complex Foot Trauma
Supplemental material, sj-pdf-1-fao-10.1177_24730114241265113 for A Novel Uni- and Biplanar External Fixator for Initial and Definitive Complex Foot Trauma by Juan Pablo Randolino, Laura Gaitán, Gastón Slullitel, Emanuel Gonzalez and Valeria Lopez in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from “Sanatorio de La Mujer” Ethical Committee (approval number 126).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.