
Abstract
Hallux valgus deformity frequently presents with an increased distal metatarsal articular angle (DMAA) which may require additional correction. Minimally invasive hallux valgus surgery is often used in patients with increased DMAA. We hypothesized that the triplanar correction with the minimally invasive extra-articular metaphyseal distal transverse osteotomy (META) would improve the DMAA, in addition to the hallux valgus angle (HVA), intermetatarsal angle (IMA), and patient-reported outcomes. A retrospective chart review was performed on patients who underwent an META procedure for hallux valgus correction. The DMAA, HVA, IMA were measured on preoperative, 2-week postoperative, and final follow-up radiographs. Patient demographics, complications, and Patient-Reported Outcomes Measure Information System (PROMIS) pain, function, and mobility scores were recorded. Univariate analysis and t-test were used to describe measurements between DMAA, HVA, and IMA. Twenty-seven META osteotomies were performed on 25 patients. At the final follow-up, mean DMAA, HVA, IMA decreased from 9.73 ± 1.96 to 4.35 ± 0.85 degrees, 30.45 ± 7.91 to 6.59 ± 2.75 degrees, and 15.37 ± 3.67 to 3.72 ± 1.84 degrees, respectively (P < .001). The PROMIS pain scores significantly improved from 58.96 ± 6.00 to 49.69 ± 9.35 at the final follow-up (P < .001). These observations imply successful resolution of hallux valgus, with a single META procedure. This approach may be an alternative to open or multiple corrections of hallux valgus, while preserving improvement in functional outcomes.
Keywords
“Hallux valgus, a common deformity treated by orthopAedic foot and ankle surgeons, frequently presents with an increased distal metatarsal articular angle (DMAA), which may require surgical correction in addition to the hallux valgus deformity.”
Introduction
Hallux valgus, a common deformity treated by orthopaedic foot and ankle surgeons, frequently presents with an increased distal metatarsal articular angle (DMAA), which may require surgical correction in addition to the hallux valgus deformity. 1 The DMAA is the angle formed between a line perpendicular to the first metatarsal anatomic axis and a line delineating the distal articular surface of the metatarsal. This angle is used to assess for metatarsal phalangeal congruity, may be increased (>10°) in cases of hallux valgus,2-5 and plays a role in hallux valgus correction.2-5,6 An increased DMAA is most commonly associated with a subset of these patients who are adolescents or have an extensive history of hallux valgus pathology.6,7-12
The utilization of minimally invasive surgery (MIS) to attempt hallux valgus correction has become widely popular in orthopaedics.7,8,13 A randomized controlled trial by Kaufmann et al 9 reported no significant clinical or radiographic differences among MIS vs open surgery groups at 5 years postoperative. Similarly, a randomized controlled trial by Torrent et al 10 reported no difference in hallux valgus angle (HVA), intermetatarsal angle (IMA), or DMAA outcomes between their MIS vs open groups; however, Visual Analog Scale scores (quantifying patient pain experience) improved to a significantly larger degree in the MIS group.
There have been several open techniques described in the literature to offer correction of an increased DMAA. These techniques include the double and triple first ray osteotomies, biplanar chevron osteotomy, revolving scarf osteotomy, or the modified Lapidus procedure.6,11,12,14 Notably, although double and triple procedures are regarded as successful interventions for hallux valgus, they many times require repeat trips to the operating room to achieve DMAA correction due to initial surgery failure or hallux valgus recurrence.15,16 With any hallux valgus procedure, improper DMAA correction has been associated with the need for later revision. Multiple authors have described a direct correlation between improper correction of the DMAA and recurrence of hallux valgus deformity. 8 For example, Shah et al 8 performed 99 modified Lapidus procedure (MLP) for 85 patients with moderate-to-severe hallux valgus; they reported a recurrence rate (3.3%) which was correlated with improper correction of the DMAA.
A minimally invasive extra-articular metaphyseal distal transverse osteotomy (META) is an MIS procedure that utilizes the high-torque, low-speed, Shannon burr to create a transverse osteotomy at the metadiaphyseal junction of the distal first metatarsal neck. With this osteotomy, triplanar correction of hallux valgus deformity can be achieved. In theory, a triplanar approach allows for correction of all rotational pathology of the first metatarsal including an increased DMAA. Many reviews have exhibited improvement in the HVA, IMA, and DMAA with hallux valgus correction.7,8,13 Despite these positive results, data specifically regarding the DMAA following META intervention is limited. Accordingly, the purpose of this study was to assess the correction of the DMAA using the META technique for hallux valgus correction, at a minimum 6-month follow-up. This procedure allows for triplanar correction; therefore, we hypothesized that the META technique will correct DMAA in addition to HVA and IMA without the need for any additional osteotomies.
Methods
The study was submitted for Institutional Review Board approval. After approval, a retrospective chart review was completed for patients who underwent an META osteotomy for hallux valgus correction between September 2021 and December 2022. Radiographs were obtained at preoperative, first postoperative (10-14 days, non-weightbearing), and at final follow-up (weightbearing). Function, pain, and mobility Patient-Reported Outcomes Measurement Information System (PROMIS) scores were collected preoperatively and at each postoperative follow-up. Inclusion criteria consisted of patients older than 18 years old undergoing the META procedure within the date range previously reported. Patients with risk factors such as obesity, diabetes, and rheumatologic diseases were not excluded from MIS hallux valgus correction. Similarly, there were no limitations regarding comorbidities or preoperative HVA measurement for patient inclusion in the current study. Procedures were completed by one of the 2 fellowship-trained orthopaedic foot and ankle surgeons. Patients who underwent hallux valgus correction utilizing an approach that was not META, patients with insufficient follow-up (<6 months), and patients with insufficient radiographs were excluded from analysis.
Surgical Procedure
Each patient was placed supine. Under fluoroscopic guidance, a stab incision was made in the area of the metadiaphyseal junction of the first metatarsal. An META was performed at the metadiaphyseal junction under fluoroscopic guidance with a (2 × 20 mm) Shannon burr (Figure 1A). Once complete, the surgeon could depronate the toe, reducing the sesamoids and DMAA (Figure 1B and C). The head was then translated laterally reducing the IMA and HVA. K-wires were placed and confirmed fluoroscopically. Two 4.0, fully threaded screws were placed. The medial spike of the proximal metatarsal was shaved down. An akin osteotomy was performed if hallux valgus interphalangeus was present (Figure 1D). All patients were instructed to maintain non-weightbearing status for 2 weeks postoperatively to minimize swelling. After this period, they transitioned to full weightbearing in a postoperative shoe or controlled ankle motion (CAM) walking boot for an additional 2 weeks. Patients were permitted to begin wearing a regular shoe at 6 weeks postoperative (Figure 1E and F).
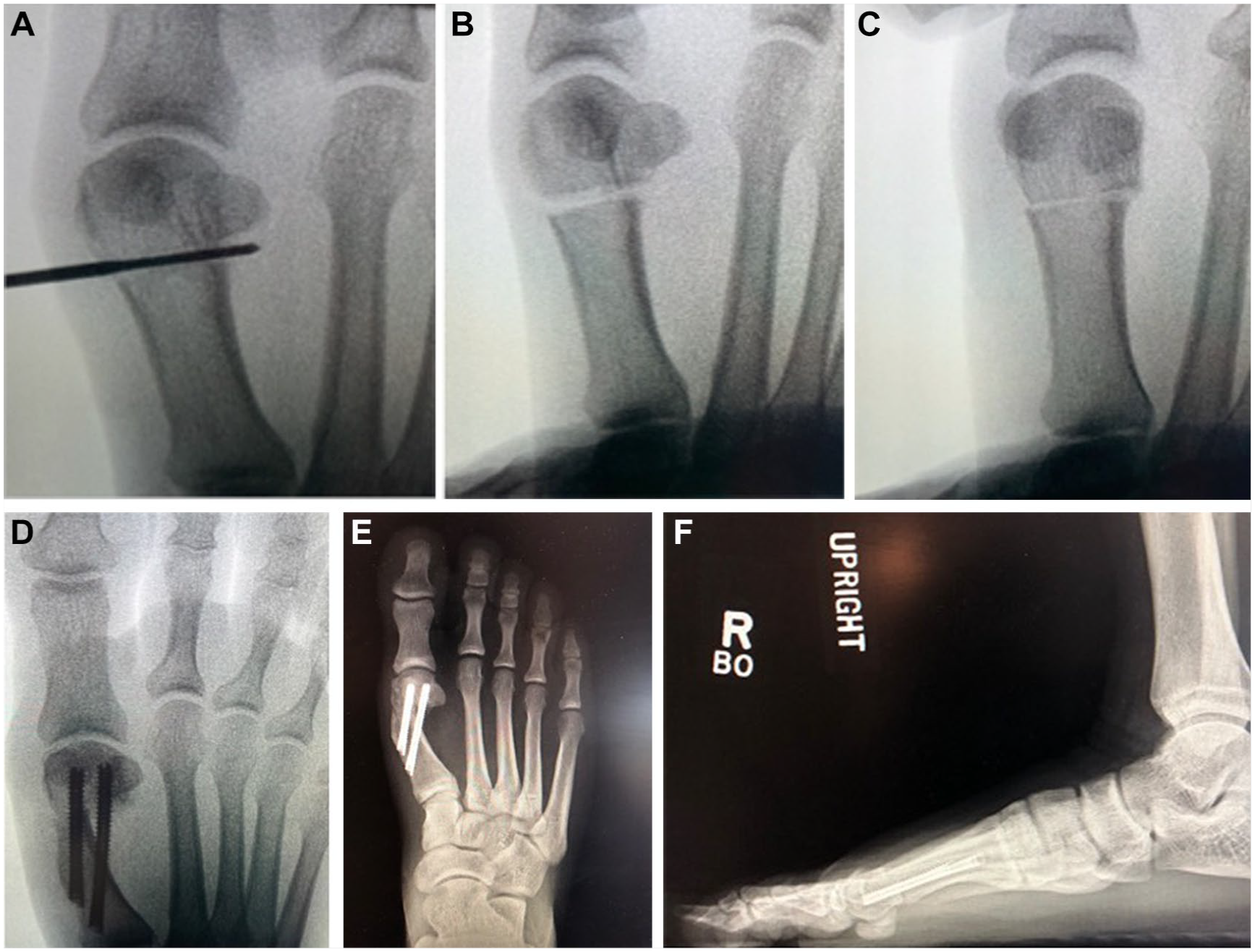
(A) Osteotomy location, (B) toe prior to derotation, demonstrating an increase in DMAA, (C) correction of DMAA after depronating the toe, and (D) final construct showing correction of DMAA, HVA, and IMA. (E) Final follow-up AP and (F) lateral radiographs.
Data Collection and Statistical Analysis
Patient demographics were recorded. Each DMAA measurement was taken as the angle between the long axis of the first metatarsal and a line through the base of the distal articular surface. The HVA and IMA were measured in standard fashion. All measurements were taken on anteroposterior foot radiographs to allow for consistent analysis at each timepoint. Univariate analysis (measure of location and variability) was used to describe preoperative and postoperative measurements for DMAA, HVA, and IMA. Differences in preoperative and postoperative measurements were evaluated using the paired t-test, assuming normality. Normality for preoperative and postoperative measures was evaluated using the Shapiro–Wilk test and histogram plots with a normal curve overlay (no major violations in normality were apparent). All radiographical measurements were independently evaluated by 2 different authors who were not involved in any of the surgical procedures or patient care. Intraclass correlation coefficient (ICC) analysis was performed to quantify reliability.
The PROMIS scores were collected preoperatively and at the final follow-up appointment. Preoperative and postoperative function, pain, and mobility scores were compared by paired t-test. An alpha level of 0.05 was used to determine the statistical significance. At the final follow-up, complications were recorded including infections, nerve injury, revision, and reported pain. All analyses were conducted using IBM SPSS Statistics 28 (IBM, Armonk, New York).
Results
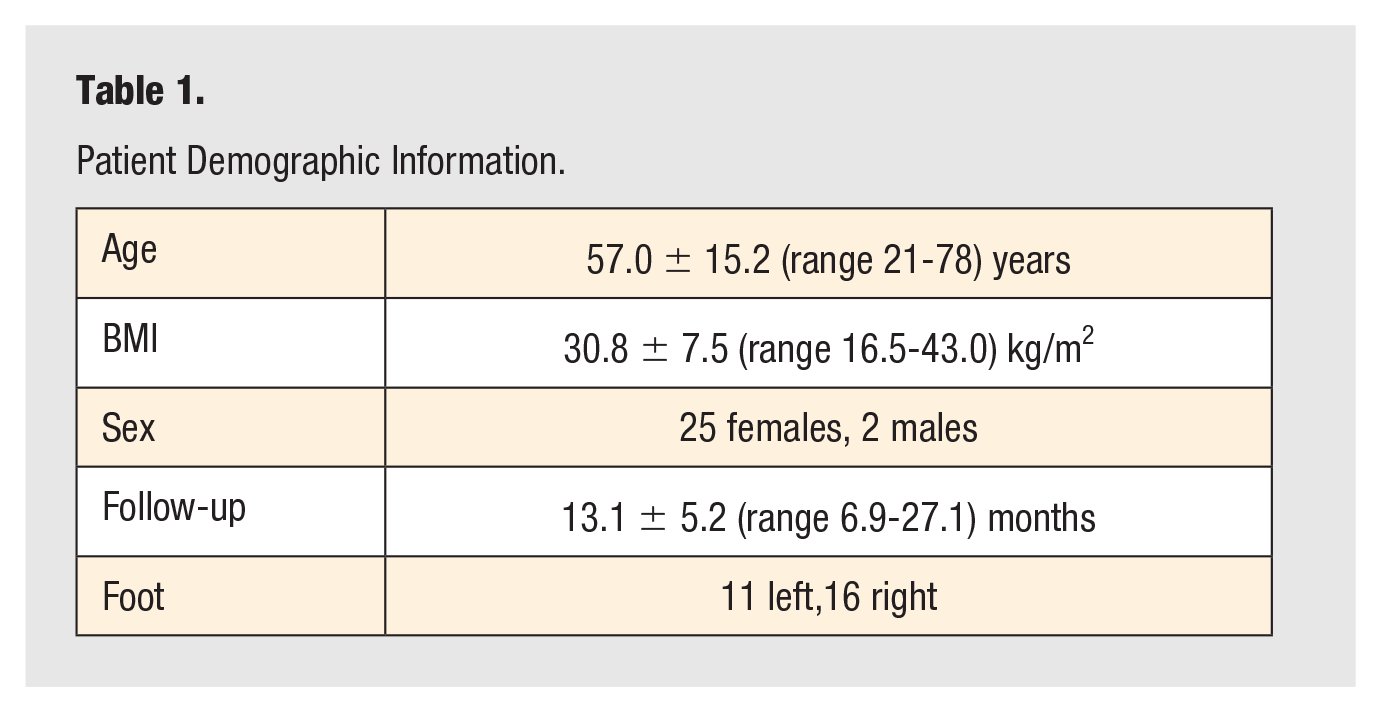
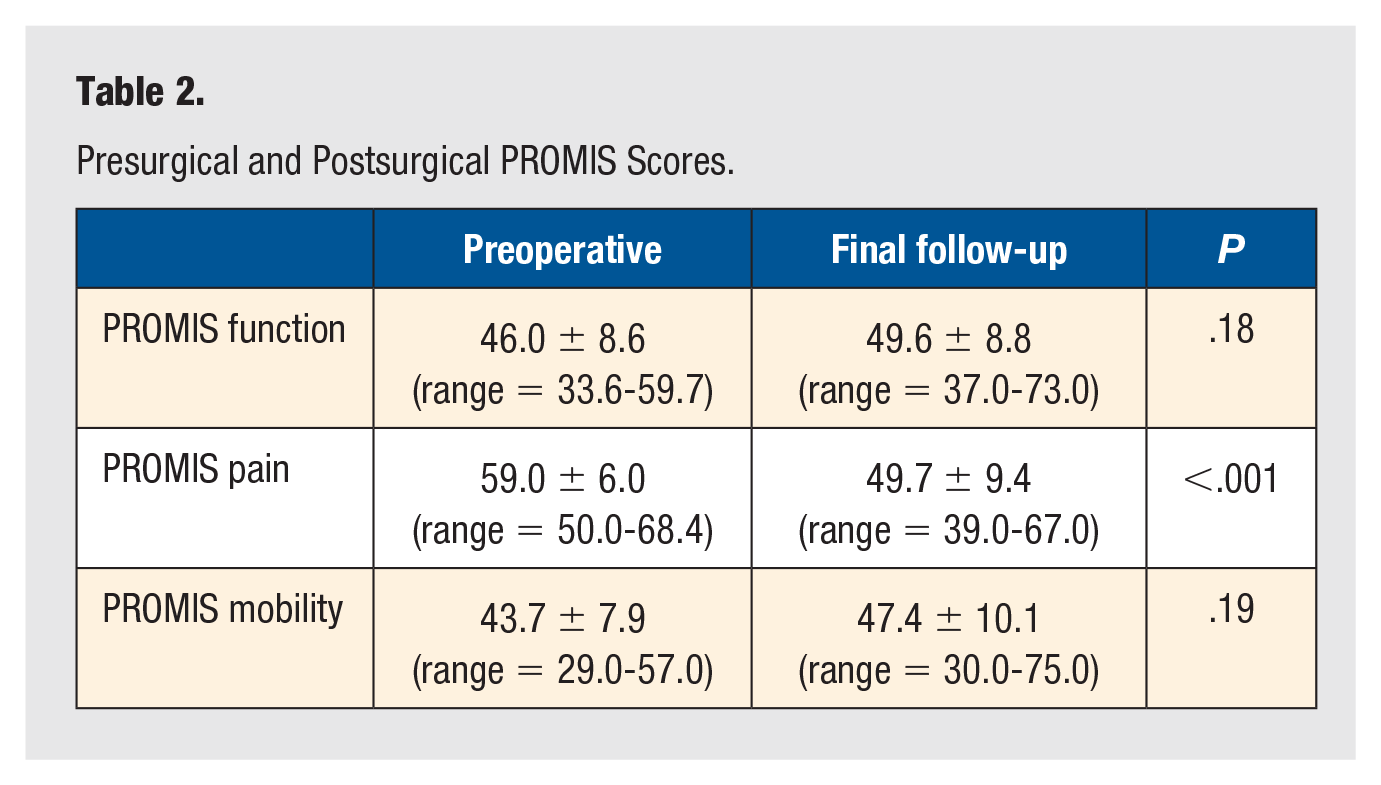
In total, 27 META hallux valgus corrections (11 left feet, 16 right feet) on 27 patients were included. There were 25 females and 2 males with a mean age of 57.00 ± 15.22 (range = 21-78) years and body mass index (BMI) of 30.77 ± 7.47 (range = 16.50-43.00) kg/m2. The mean final follow-up was 13.05 ± 5.19 (range = 6.89-27.14) months (Table 1). At the final follow-up, a total of 20 (74.07%) patients reported no pain, and 7 (25.93%) patients reported minimal pain around the surgical site. There were 2 (7.41%) cases of superficial wound infections that were successfully treated with oral antibiotics and resolved without further intervention. There were 3 (11.11%) cases with minor numbness around the surgical incision that did not resolve by final follow-up but did not require any additional treatment. There were no revisions or other complications among patients. The PROMIS function, pain, and mobility scores improved by the final follow-up. The PROMIS function scores increased from 45.99 ± 8.57 (range = 33.60-59.70) to 49.58 ± 8.80 (range = 37.00-73.00) (P = .18). The PROMIS pain scores improved significantly, from 58.96 ± 6.00 (range = 50.00-68.40) to 49.69 ± 9.35 (range = 39.00-67.00) (P < .001). The PROMIS mobility scores increased from 43.67 ± 7.90 (range = 29.00-57.00) to 47.44 ± 10.06 (range = 30.00-75.00) (P = .19) (Table 2).
Patient Demographic Information.
Presurgical and Postsurgical PROMIS Scores.
At 2 weeks postoperative, non-weightbearing AP radiologic evaluation demonstrated a decrease in mean DMAA from 9.73 ± 1.96 (range = 5.60-14.10) to 4.97 ± 1.45 (range = 1.90-7.80) degrees (P < .001, Table 3). The mean HVA decreased from 30.45 ± 7.91 (range = 15.50-51.20) to 4.21 ± 3.05 (range = 0.30-11.20) degrees at 2 weeks postoperative (P < .001, Table 3). Finally, the mean IMA decreased from 15.37 ± 3.67 (range = 7.70-24.70) to 3.01 ± 1.52 (range = 1.00-5.80) degrees at 2 weeks postoperative (P < .001, Table 3). On weightbearing AP radiologic evaluation at final follow-up, the mean DMAA was 4.35 ± 0.85 (range = 2.60-6.20) degrees ( P < .001), HVA was 6.59 ± 2.75 (range = 1.70-11.30) degrees (P < .001), IMA was 3.72 ± 1.84 (range = 0.60-7.50) degrees (P < .001). The ICC for the measurements that both authors took independently was statistically significant at 0.69 (P < .05) (Figure 2A-D).
Presurgical and Postsurgical Measurements of Distal Metatarsal Articular Angle (DMAA), Hallux Valgus Angle (HVA), and Intermetatarsal Angle (IMA).
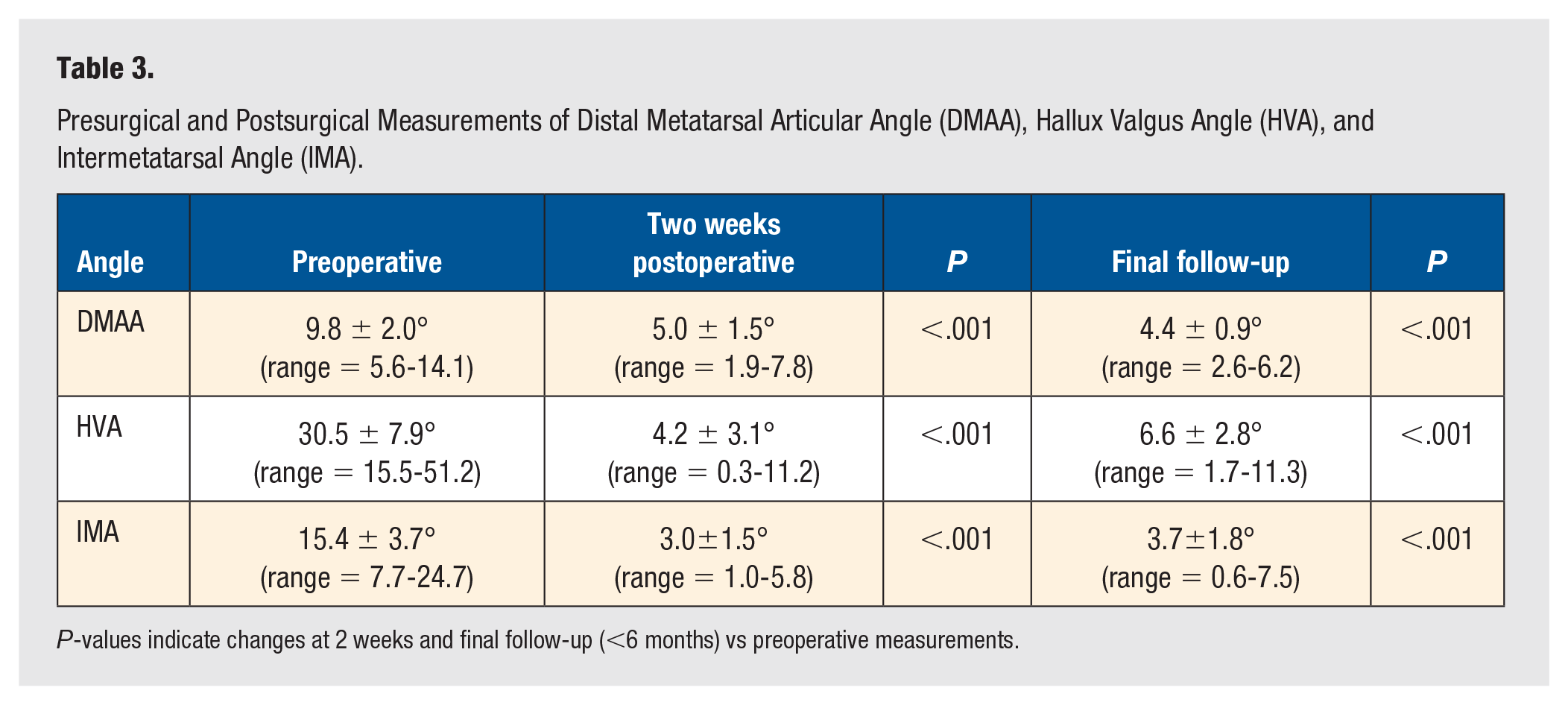
P-values indicate changes at 2 weeks and final follow-up (<6 months) vs preoperative measurements.
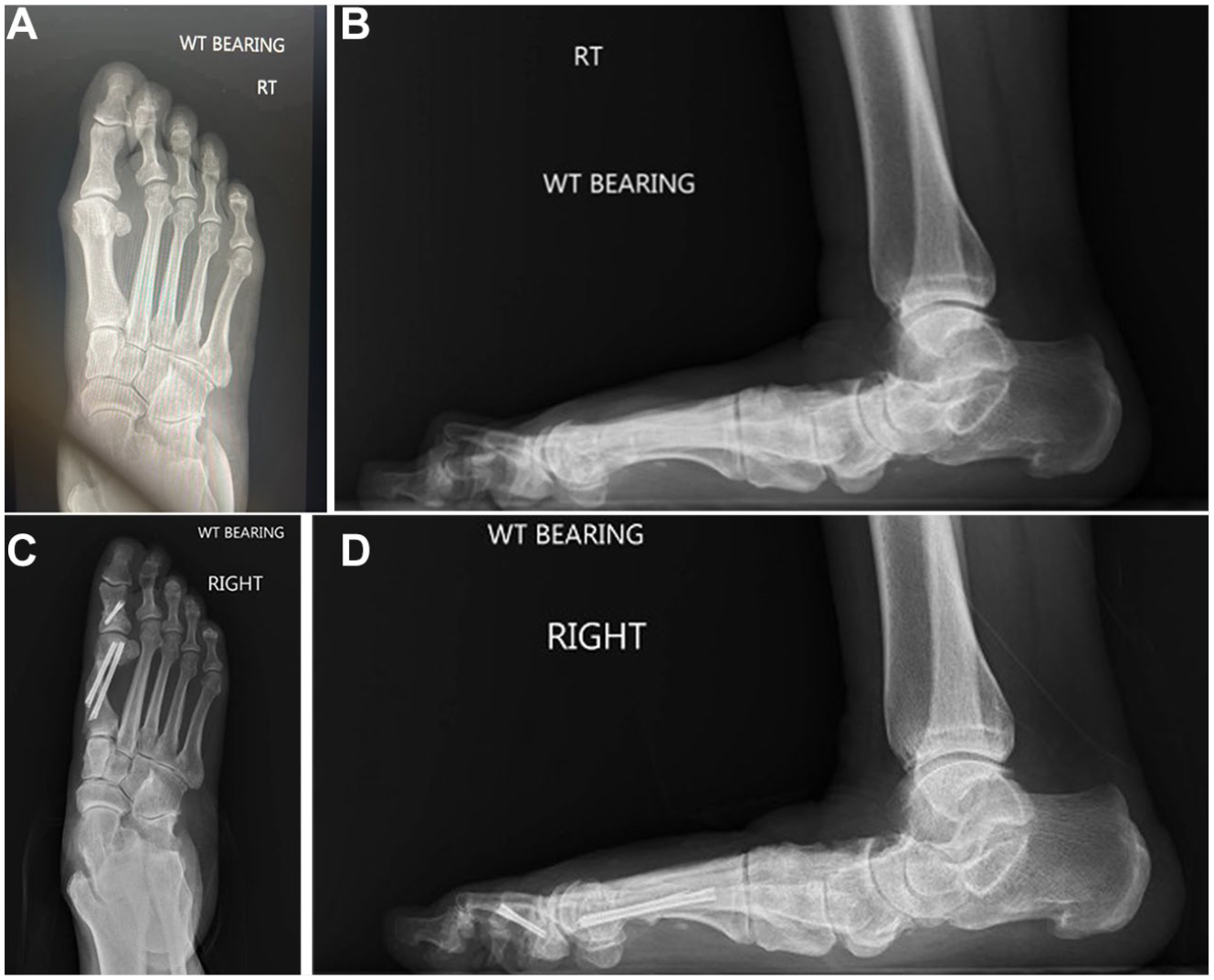
(A) Preoperative A/P radiograph and (B) preoperative lateral radiograph of patient with hallux valgus deformity. (C) Paired postoperative A/P and (D) lateral radiographs after surgical correction of hallux valgus deformity with META approach.
Discussion
This study demonstrated the META approach for hallux valgus correction is an effective method for not only IMA and HVA correction, but also for correction of the DMAA without the need for additional intervention. Radiographic analysis found that there was statistically significant correction of the DMAA in the immediate postoperative period (2 weeks postoperative) which was also observed at final follow-up (Table 3). Moreover, PROMIS pain scores were significantly improved at final follow-up in patients receiving META hallux valgus correction (P < .001). We did observe a marginal improvement in mobility and function PROMIS scores at final follow-up. Although paired t-test did not reveal these changes to be significant, statistical significance may have been limited by our modest sample size (Table 2).
It has been established that hallux valgus deformity is a multiplanar pathology that presents with pathologic rotation of the first metatarsal.17,18 Conti et al 19 reported significantly better PROMIS scores and a lower revision rate for patients who had a decrease in the first metatarsal pronation following hallux valgus correction. Conti et al utilized the triplanar angle measurement to determine pronation. However, more broadly in the literature, there has been inconsistent evidence regarding which radiographic measurements are indicative of rotational pathology of the first metatarsal. The systematic literature review by Najefi et al evaluated 14 studies which analyzed the rotation of the first metatarsal on computerized tomography (CT). They found the metatarsal pronation angle and the alpha angle to yield the highest reliability and reproducibility when assessing pronation correction following hallux valgus surgery. 20 However, contradictory to this evidence, Mahmoud et al 21 reported the alpha angle to be abnormal in patients without hallux valgus pathology, therefore suggesting this measurement has limited diagnostic utility. Separately, the systematic review by Steadman et al included 26 studies that reported on the significance of first metatarsal rotation and the HVA, IMA, and DMAA. Their conclusion suggests that the HVA and IMA are independent from first metatarsal rotational deformity. 17 Meanwhile, there is evidence to suggest that an increased DMAA is a product of pathological first metatarsal rotation.4,17,22,23
There has been controversy on the accuracy and reproducibility of DMAA measurements, particularly on standard radiographs. Lalevée et al 24 described a significant increase in DMAA in patients with hallux valgus in comparison to a control group, utilizing conventional radiographs, weightbearing computer tomography (WBCT), and WBCT with plane correction. Lalevée et al 24 observed standard radiographs and WBCT without correction to overestimate the severity of the DMAA angle. Similarly, Mansur et al 2 found a strong correlation between the HVA and DMAA; however, there was a significant difference in the DMAA angle when comparing WBCT to conventional radiograph. 8 Aravena et al 25 tout the benefits of weightbearing CT to properly measure preoperative and postoperative DMAA. However, this may be an unrealistic to accomplish in every patient, at every medical center.
Surgical correction of hallux valgus occurs at a rate of over 200 000 per year in the United States alone.26,27 Most institutions do not have a weightbearing CT scanner; therefore, measuring the DMAA in this way is not an option for most surgeons. Most surgeons must rely on preoperative and postoperative AP radiographs to assess their correction and maintained alignment. Ray et al 4 have described an AP radiograph to be an appropriate, common measure of DMAA when evaluating patients. The purpose of this study was to utilize the most common tool in measuring the DMAA to broaden the generalizability of our results. Therefore, we retrospectively analyzed radiographs corresponding to the surgical technique as described above. The authors do acknowledge the inherent flaws in radiographic analysis of DMAA. However, as stated, this remains the technique utilized by most surgeons to judge postoperative correction. The questioned reproducibility of DMAA measurement highlights the importance of having multiple authors independently measure each angle for analysis, which we accomplished.
The MIS hallux valgus correction is becoming widely popular among foot and ankle surgeons. 6 In the past few years, several systematic reviews and meta-analyses have noted excellent outcomes for patients undergoing MIS hallux valgus correction.6-9,12-16 However, only 2 of many systematic reviews included DMAA data in their analysis. The systematic review by Gonzalez et al 13 evaluated 17 hallux valgus correction studies and 4 studies reported improvements in DMAA, 2 of which were statistically significant. The systematic review by Ji et al evaluated 22 MIS vs open surgery studies for hallux valgus correction. Ten studies reported DMAA improved outcomes in the MIS group; the other 12 studies did not report DMAA measurements. 7 This is a widely understudied, yet clinically important aspect of hallux valgus correction.
The current study has certain limitations, including a relatively small patient sample size and short follow-up. The size of our study may have limited the significance of any changes in mobility and function PROMIS scores; our limited number of cases may have inflated the report of certain complications. For example, we observed a 7.41% rate of cellulitis among 27 cases included in the current study. This equates to only 2 incidences of cellulitis which resolved with a course of oral antibiotics. However, the purpose of this study was to demonstrate correction of the DMAA with the META osteotomy, which we were able to accomplish at 2 weeks postoperative and at the final follow-up. In addition, the current study relied solely on standard radiographs for DMAA measurements. Although prior studies have declared weightbearing CT as the preferred modality for DMAA measurement,2,8,24,25 not all institutions have this capability. In addition, measuring DMAA in the operating room requires fluoroscopy; therefore, we wanted to standardize these measurements to recreate real operating room scenarios. As such, we assumed this limitation in our study to allow for more generalizable findings.
Our study was a retrospective review which brings forth its own inherent limitations. This study also only included patients who were operated on by one of 2 surgeons with substantial experience in an META approach for hallux valgus correction. It would be prudent to conduct a multisurgeon, multicenter analysis to further explore outcomes and recurrence rates after correction. A larger study would allow for increased power and generalizability of our results, and investigations into which patients experience the most success with the META. Long-term research is also warranted to continue to evaluate the capacity of an META approach to maintain hallux valgus correction over time, although this was outside the scope of the current study. An additional extension of this study includes a prospective review of META utilizing WBCT analysis for DMAA measurement to further explore this imaging modality and its accuracy. At our institution, we do have a WBCT; however, most foot and ankle surgeons in the United States do not. As previously mentioned, to increase the generalizability of our results, we did not use WBCT to assess DMAA in the current study.
Conclusion
The META approach for correction of hallux valgus deformity significantly reduced the DMAA, along with the IMA and HVA, without the need for additional metatarsal osteotomies. This observation implies successful resolution of pathological hallux valgus deformity with a single META operation. This study provides evidence to suggest that META is effective for patients who require DMAA correction associated with hallux valgus deformity, being an alternative to open or multiple osteotomies for hallux valgus deformity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: There are no relevant conflicts of interest pertinent to the topic of this manuscript. Oliver N. Schipper, MD, reports royalties or licenses and consulting fees from Treace Medical Concepts, Vilex, Exactech, and Enovis. Jonathan Kaplan, MD, reports royalties or licenses and consulting fees from Surgical Fusion Technologies, Enovis, Treace Medical Concepts, and Vilex; consulting fees from Artelon, Edge Surgical, Exactech, and Surgebright. J. Benjamin Jackson III, MD, MBA, reports consulting fees from Synthes. Tyler A. Gonzalez, MD, MBA, reports royalties or licenses and consulting fees from Treace Medical Concepts, Surgical Fusion Technologies, and Vilex; consulting fees from Stryker, Surgebright, and Enovis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB application was completed, project title [1960747-1].
Informed Consent
Retrospective study.
Trial Registration
n/a.