
Abstract
Background:
Intraoperative fracture of the lateral cortex is common during Akin osteotomy. In a recent study, lateral cortex fracture did not impede healing or result in loss of correction in a combined cohort of open and percutaneous osteotomies stabilized by K-wire fixation. We hypothesize that undesired lateral cortex fracture will not affect radiographic correction and patient-reported outcomes in a percutaneous cohort stabilized by permanent, rigid screw fixation.
Methods:
Consecutive patients with hallux valgus who underwent first metatarsal osteotomy and percutaneous Akin osteotomy stabilized by permanent, rigid screw fixation between May 2020 and January 2022 were retrospectively reviewed. Patients were stratified based on fractured lateral cortex (FC) or its absence (nonfractured cortex [NFC]). Visual analog scale (VAS) and Foot Function Index (FFI) were used to assess pain and patient-reported outcomes at 1-year follow-up. Patients were polled for satisfaction at 1-year follow-up by yes/no survey.
Results:
Ninety-eight patients (89% female) were reviewed (98 feet; 43 NFC, 55 FC). Mean age was 48.3 years (range, 18-83 years). Mean preoperative VAS score was 7.5 and 7.7 in NFC and FC groups, which significantly decreased to 0.6 (P < .01) and 0.6 (P < .01), respectively. Mean total FFI was 53.9 and 54.2 and decreased to 17.9 (P < .01) and 17.2 (P < .01) in the NFC group and FC group, respectively. Overall, 97.8% of the NFC group and 96.4% of the FC group reported satisfaction.
Mean HVA improved from 27.2 (16-42) degrees to 10.7 degrees (4-12) postoperatively in the NFC group. And in the FC group, HVA improved from 29.3 (19-39) degrees to 7.1 (4-12) degrees postoperatively. Postoperative HVA was significantly lower in the FC group (P < .05).
Conclusion:
In an exclusively percutaneous surgical cohort with correction maintained by rigid screw fixation, fracture of the lateral cortex is associated with improved postoperative radiologic alignment without detriment to patient-reported outcomes.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
The Akin osteotomy is a medial-based closing wedge osteotomy of the proximal phalanx coupled with medial eminence resection and lateral release first described in 1925. 6 It is used to address angulation of the proximal phalanx compared to the first metatarsal most commonly in the setting of hallux valgus. Multiple iterations of the open Akin osteotomy have been described, but the overall steps are to create a closing medial wedge through a horizontal osteotomy at the proximal phalanx. The correction may then be supported by external bandaging, temporary, or permanent fixation.2,10,19,20 A common occurrence in the procedure is an undesired intraoperative fracture of the lateral cortex of the proximal phalanx at the osteotomy site. This often occurs because of excessive weakening of the lateral cortex secondary to saw oscillation or resection of a large bone wedge. Fracture of the lateral cortex has been reported around 13% for open techniques and 25.9%-51.6% for minimally invasive techniques. Fracture has been debated in the literature as the cause of a secondary loss of correction and delayed bone healing.5,8,21
Although the minimally invasive Akin osteotomy has increased in utilization, the lack of open visibility makes preservation of the lateral cortex more challenging. A recent study compared intraoperative breach of the lateral cortex in open and minimally invasive cases and found that fracture occurred approximately 4 times more frequently in the minimally invasive group. 21 Additionally, fractures mainly occurred during the correction in the open group, whereas it occurred during burring in the minimally invasive technique. Despite the theory that lateral hinge fractures result in instability of the osteotomy and increase the risk of displacement, the study found that breach of the lateral cortex did not impair correction of the interphalangeal angle (IPA) or impair bone healing in the minimally invasive or open technique. Notably, the minimally invasive technique used temporary percutaneous K-wire fixation to maintain correction, which was removed postoperatively at 4 weeks whereas the current study will utilize permanent screw fixation. 21
The goal of the present study was to evaluate the clinical and radiographic outcomes of lateral cortex fracture in a cohort of exclusively percutaneous Akin osteotomies for the treatment of hallux valgus requiring only varization using permanent screw fixation for maintenance of correction. We hypothesize that undesired fracture of the lateral cortex will not affect postoperative HVA, IMA, and patient-reported outcomes compared to patients with an intact lateral cortex. The authors believe using rigid screw fixation promotes stability in cases where the lateral cortex hinge is fractured.
Methods
Study Design, Setting, Participants
A retrospective cohort study was conducted on 98 consecutive patients (98 feet) with symptomatic hallux valgus refractory to at least 6 months of nonoperative therapy who underwent percutaneous distal first metatarsal and Akin osteotomies between May 2020 and January 2022 at a single hospital institution with at least 1 year of follow-up. All procedures were performed by a single fellowship-trained foot and ankle orthopaedic surgeon with fellowship training in minimally invasive surgery (MIS) using the same technique and postoperative protocol as detailed below. The operating surgeon has had multiple years of experience performing MIS procedures. Patients were stratified based on presence or absence of intraoperative lateral cortex fracture observed on perioperative fluoroscopy (Figures 1 and 2).

(A) Preoperative radiographs of a 47-year-old woman who underwent percutaneous Akin osteotomy. (B) Intraoperative radiograph of a 47-year-old woman who underwent percutaneous Akin osteotomy. The intraoperative radiograph demonstrates integrity of the lateral cortex of the first proximal phalanx. (C) 12-week postoperative radiographs of a 47-year-old woman who underwent percutaneous Akin osteotomy.

(A) Preoperative radiographs of a 43-year-old woman who underwent percutaneous Akin osteotomy. (B) Intraoperative radiograph of a 43-year-old woman who underwent percutaneous Akin osteotomy. The intraoperative radiograph demonstrates fracture of the lateral cortex of the first proximal phalanx. (C) 12-week postoperative radiographs of a 43-year-old woman who underwent percutaneous Akin osteotomy.
Variables and Data Sources
Hallux valgus was defined as hallux valgus angle (HVA) greater than 15 degrees and intermetatarsal angle (IMA) between the first and second metatarsals greater than 11 degrees. Inclusion criteria were symptomatic hallux valgus refractory to at least 6 months of nonoperative therapy who underwent percutaneous distal first metatarsal and Akin osteotomies with radiographic definition of hallux valgus. Patients were excluded if they simultaneously underwent any other significant first ray or midfoot fusion procedures. Patients that underwent lesser toe procedures including metatarsal osteotomies and hammertoe corrections were included. All patients eligible for inclusion, 98 patients, were included in the study.
Patients underwent physical examination and radiographic assessment of the operative foot 2, 6, and 12 weeks, 6 months, and 1 year postoperation (Figures 1 and 2). Physical examination included assessment for hammertoes, plantar or lateral callosities, cock-up lesions, and presence of neuropathy.
Anteroposterior (AP), lateral, and oblique weightbearing radiographs of the foot were taken to assess healing at every clinic visit (Figures 1C and 2C). Bone union was defined as bridging 2 or more cortices in the AP and oblique radiographs. Failure to achieve radiologic evidence of union at 3 months was considered delayed union, and failure by 6 months was considered a nonunion.
Lateral cortex fracture was recorded intraoperatively during the percutaneous Akin osteotomy.
Patient-reported outcomes including Foot Function Index (FFI) and visual analog scale (VAS) were collected preoperatively and at 1 year postoperatively. Additionally, patients were surveyed for overall satisfaction with a single-question binary response survey. Complications and reoperation rates were reported by patients or the primary surgeon.
Bias and Study Size
To address possible bias, an independent and trained observer oversaw data entry and postoperative radiologic evaluation. The study size was a convenience sample of consecutive patients.
Primary outcome
The primary outcome was radiographic deformity correction measured by the difference in HVA, IPA, and IMA between the first and second metatarsals preoperatively and postoperatively at 1-year follow-up. Using a weightbearing AP radiograph of the foot, the IMA was measured by calculating the angle between the longitudinal axes of the first and second metatarsals. Using a weightbearing AP radiograph of the foot, the HVA was measured by calculating the angle between the longitudinal axes of the first metatarsal and the proximal phalanx. Using a weightbearing AP radiograph of the foot, the IPA was measured by calculating the angle between the longitudinal axis of the shaft of the first toe proximal phalanx and the longitudinal axis of the shaft of the distal phalanx.
Secondary outcomes
The VAS and FFI questionnaire were used to assess pain and functional disability and activity restriction as secondary outcomes along with the Patient Satisfaction Survey. Complications and reoperation rates were collected as secondary outcomes.
Operative technique
The Akin procedure was completed after the distal metatarsal osteotomy in all cases. The distal first metatarsal osteotomy is an extracapsular procedure performed percutaneously at the metadiaphyseal flare using a 2 × 12-mm cutting burr. A flat cut was completed followed by lateral translation of the metatarsal head and fixation with two 4-mm beveled-head fully threaded screws. A minimally invasive Akin procedure was performed as described by Vernois and Redfern 23 and Mikhail et al. 17
The percutaneous Akin osteotomy is completed with a 2 × 12-mm cutting burr through a medial portal created just proximal to the hallux interphalangeal joint that is started midaxial in the proximal phalanx. The burr is introduced from distal to proximal aiming for the lateral corner of the base of the proximal phalanx attempting to preserve the lateral cortex. Burring is completed under fluoroscopy with the dorsal and then plantar sides of the osteotomy completed. The osteotomy is then manually closed with a varus force on distal phalanx. Integrity of the lateral cortex is assessed under fluoroscopy at this point to determine if it has been fractured. Once satisfied with correction, fixation is performed with a K-wire. The K-wire is then overdrilled and a fully threaded 3-mm cannulated screw is inserted over the K-wire and the K-wire is subsequently removed. All lateral wall fractures are unintentional with this technique.
Postoperative protocol
Patients were permitted full weightbearing in a flat rigid sandal for the first 6 weeks postoperatively. Patients were transitioned to a semirigid shoe (ie, sneaker) thereafter. High-impact activities and return to any shoe wear was allowed at 12 weeks from surgery. There were no differences in postoperative protocol for patients with lateral cortex fracture.
Statistical analysis
Data analysis was performed using Stata/MP 16.1 (StataCorp, College Station, TX). Descriptive statistical analysis was performed on all variables, yielding frequency and percentages for categorical variables, and mean, SD, and ranges for continuous variables. Fisher exact test was used to determine association between categorical variables. P values ≤.05 were considered to be statistically significant.
Results
Ninety-eight patients (87 females [89%] and 11 males [11%]) were included in the analysis. There were no patients lost to follow-up. At the time of surgery, the mean age was 48.3 years with a minimum of 18 and a maximum of 83 years (Table 1). Seven were known diabetic patients (4 in the fractured group and 3 in the nonfractured group) and 3 had rheumatoid arthritis (all in the fractured group). There were 48 associated procedures performed that were all completed outside of the first ray that were composed of 6 lesser metatarsal osteotomies and 42 hammertoe corrections. Mean follow-up was 12 months (range, 12-25 months) in the fractured cohort and 12 months (range, 12-25 months) in the group without fracture.
Patient Demographics and Stratification.
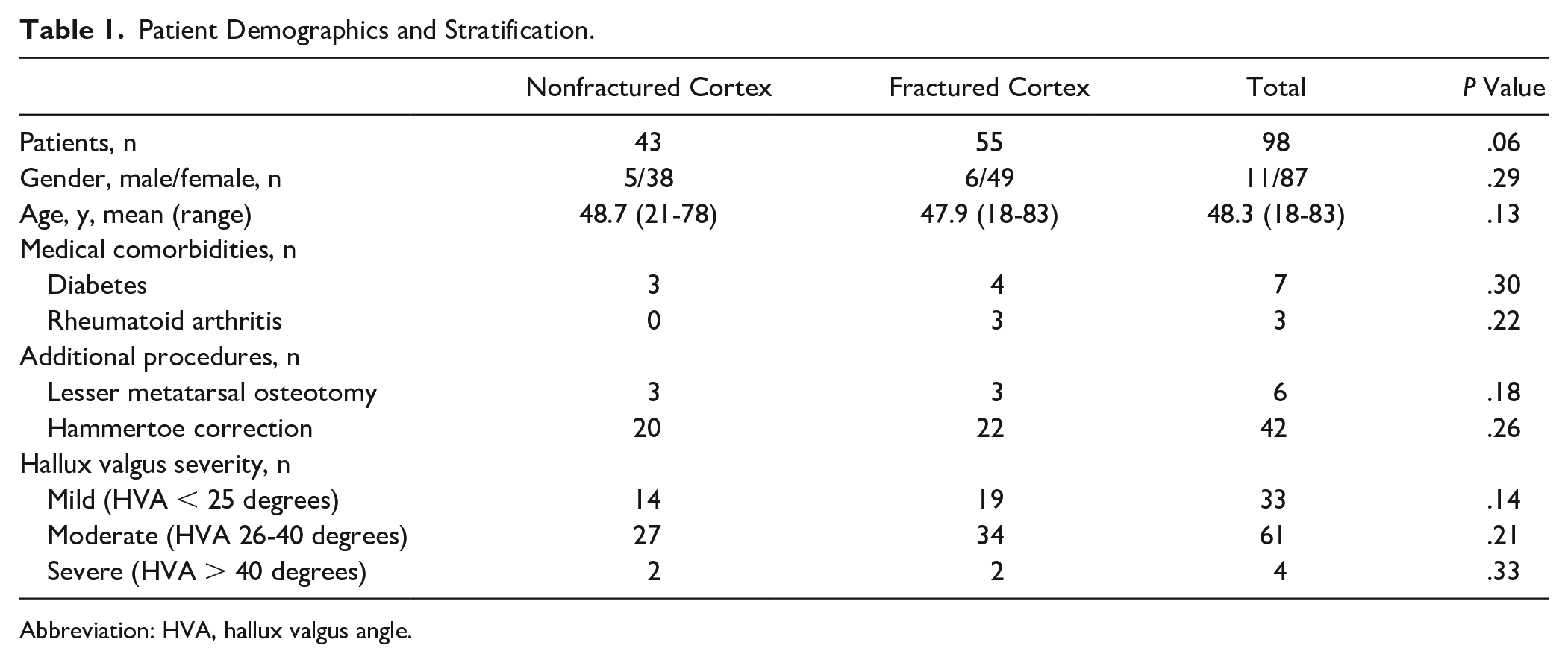
Abbreviation: HVA, hallux valgus angle.
Primary Outcomes
The radiographic outcomes are detailed in Table 2. In the group without fracture the mean first-to-second IMA improved from 13.2 (12-21) degrees preoperatively to 3.4 (2-6) degrees postoperatively. In the same group the mean HVA improved from 27.2 (16-42) degrees preoperatively to 10.7 degrees (4-12) postoperatively. The mean IPA in the unfractured group improved from 13.9 (11-17) degrees to 3.9 (3-8) degrees postoperatively. In the group with lateral cortex fracture, the mean first-to-second IMA angle preoperatively was 13.3 (11-22) degrees and improved postoperatively to 3.8 (1-6) degrees. The preoperative HVA was 29.3 (19-39) degrees and improved to 7.1 (4-12) degrees postoperatively. The mean IPA improved from 13.5 (9-16) degrees to 4.7 (3-8) degrees postoperatively. The preoperative IMA, HVA, and IPA differences between the fracture and nonfracture group were not significant (P > .05). Postoperatively, there was not a significant difference in IMA (P = .22) or IPA (P = .06) between groups. Notably the postoperative HVA was significantly lower in the fractured group compared to the nonfractured group (P < .05).
Radiographic Outcomes.
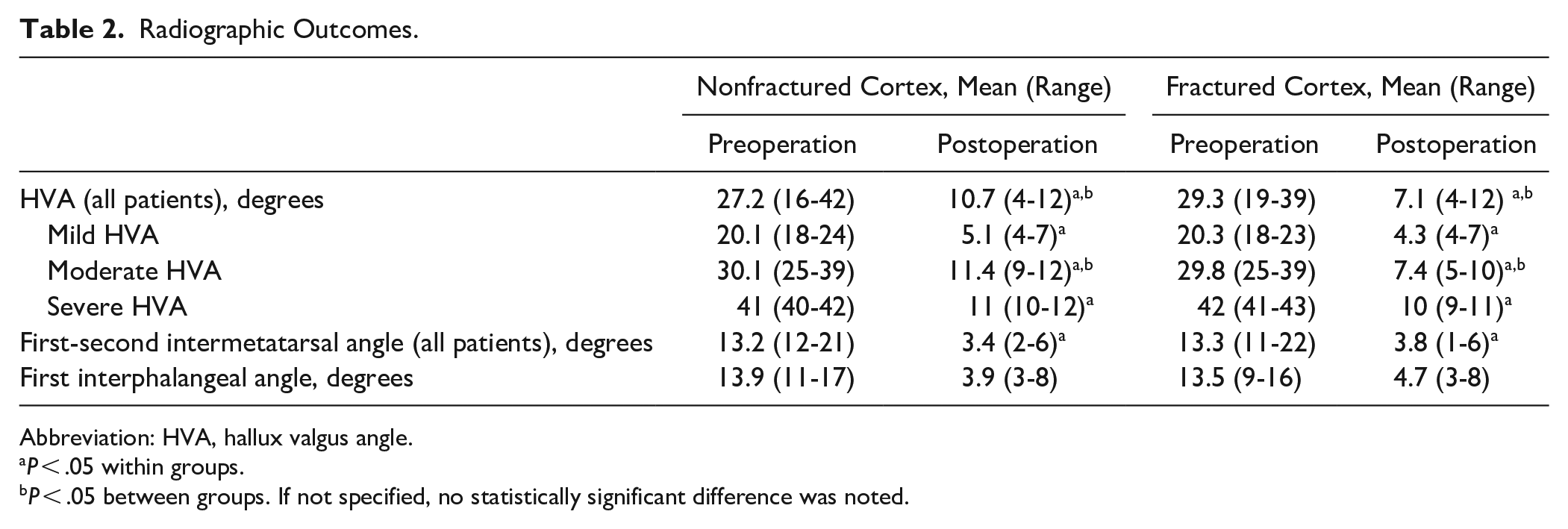
Abbreviation: HVA, hallux valgus angle.
P < .05 within groups.
P < .05 between groups. If not specified, no statistically significant difference was noted.
Secondary Outcome Measures
In the nonfractured cohort, the average preoperative VAS score was 7.5, which significantly decreased postoperatively to 0.6 (P < .001). In the fracture cohort, average preoperative VAS was 7.7, which significantly decreased to 0.6 (P < .001). Patients also reported significant improvement in total FFI from 53.9 preoperatively to 17.9 postoperatively in the nonfractured group, and 54.2 to 17.2 in the fractured group (P < .001) (Table 3). All categories (pain, disability, and activity) significantly decreased postoperatively in both the nonfractured and fractured groups.
Foot Function Index (FFI) Outcomes.
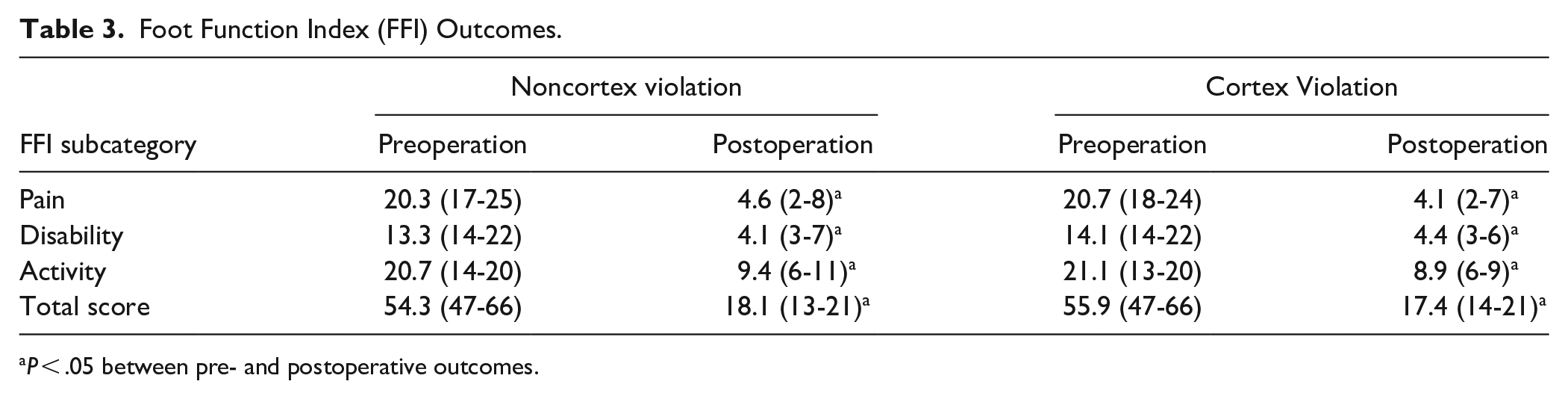
P < .05 between pre- and postoperative outcomes.
In the fractured cohort, average time to bone union of the Akin osteotomy was achieved at 12.1 weeks postoperatively (range 12-24 weeks). In the nonfractured cohort, average time to bone union of the Akin osteotomy was also 12.1 weeks postoperatively (range 12-26 weeks). Additionally, 96 out of 98 patients reported being satisfied with the outcome of the procedure.
Two complications secondary to the procedure were identified in 2 feet (2.0%). One complication was a superficial wound dehiscence at the first metatarsal osteotomy incision, and the second complication was a delayed union of a first metatarsal osteotomy that consolidated at 7 months without further intervention. Both complications occurred in the nonfractured cohort. There were no instances of hardware removal, malunion, loss of correction, infection, neuroma, or unplanned return to the operating room associated with the Akin procedure.
Discussion
The minimally invasive Akin osteotomy, coupled with a distal metatarsal osteotomy, for correction of hallux valgus is a third-generation percutaneous hallux valgus surgery characterized by rigid, permanent fixation at the Akin osteotomy site as opposed to previous generations using temporary percutaneous K-wires or no intraosseous fixation. 4 The MIS Akin procedure has been reported as effective in the literature. Overall, studies have reported similar outcomes with effective deformity correction, short learning curve, low complication rate, low symptomatic recurrence, low postoperative opioid use, and high patient satisfaction.3,9,11-15,17,18,22
Although this study focused on a third-generation technique with rigid, permanent fixation, there are multiple techniques for the percutaneous Akin throughout the literature. Biz et al 1 reported on 80 patients with 2-year follow-up who underwent percutaneous Akin osteotomy as part of hallux valgus correction; however, the technique only created the percutaneous osteotomy and then bandaged the foot in appropriate position to maintain correction. The authors reported significant improvement in mean AOFAS scores, with improvement continuing up to 2 years and significant radiographic improvement in IMA, HVA, and distal metatarsal articular angle (DMAA) in mild to severe hallux valgus. 1 Similarly, Kaufmann et al 8 reported effective deformity correction and also reported no correlation between healing and integrity of the lateral hinge using a percutaneous Akin technique without fixation device. Schilde et al 21 performed fixation of the Akin osteotomy with transcutaneous K-wires removed at 4 weeks postoperatively with good result as well.
Reports of undesired lateral cortex fracture are ubiquitous throughout the literature.1,7-9 Lateral hinge fractures have been thought to contribute to osteotomy instability and secondary displacement. 16 However, Schilde et al 21 recently reported on minimally invasive and open Akin osteotomy techniques and found that disruption of the lateral cortex occurred more frequently in the minimally invasive group (51.6% vs 13.9%), but there was no significant delay in bone healing using their transcutaneous temporary K-wire technique. Also, additional subgroup analysis found that mean IPA was unaffected by fracture, and that loss of correction was not correlated with cortex fracture. 21 In the current study of the 98 patients who exclusively underwent a minimally invasive Akin osteotomy supported by permanent screw fixation, 43 had an intact, nonfractured proximal phalanx and 55 had an iatrogenic fracture of the proximal phalanx cortex. The most notable result obtained was that the mean postoperative HVA was significantly improved in the fractured group when compared to the nonfractured group (7.1 vs 10.7 degrees), indicating that routine fracture of the lateral cortex during the osteotomy may improve radiographic alignment of the first phalanx.
Our results support the findings of Schilde et al, 21 who suggest fracture does not affect stability or cause a loss of correction in their technique using transient K-wire fixation. However, our findings further suggest that regular fracture may improve radiographic correction. The radiographic improvement in the fracture cohort may be explained by enabling more aggressive correction that is then rigidly fixed with a permanent implant. Stability of the osteotomy is likely not decreased even in the setting of lateral cortex fracture as rigid screw fixation is used to hold the osteotomy. It may be that fixation with a permanent rigid screw with an intact lateral wall and a fractured lateral wall is biomechanically equivalent, but further testing is required.
The main limitation to the current study is the lack of randomization and retrospective design. Additionally, there was only a single independent reviewer to evaluate postoperative radiographs and data entry. An additional independent observer for postoperative radiographs with assessment of interrater reliability may have been beneficial. The strengths of the study include its moderate-sized cohort and strict evaluation of a single surgical technique without additional procedures in the first ray.
In conclusion, this study demonstrates that undesired lateral cortex fracture of the proximal phalanx during fully percutaneous, minimally invasive Akin osteotomy when only varization is required, supported with rigid, permanent fixation may provide improved radiographic alignment of the HVA with no difference in patient-reported outcomes. As such, although it may be undesired intraoperatively, lateral wall fracture can be considered safe from a radiographic and patient outcome perspective.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231209765 – Supplemental material for Fracturing the Lateral Hinge Improves Radiographic Alignment and Does Not Affect Clinical Outcomes of the Minimally Invasive Akin Osteotomy
Supplemental material, sj-pdf-1-fai-10.1177_10711007231209765 for Fracturing the Lateral Hinge Improves Radiographic Alignment and Does Not Affect Clinical Outcomes of the Minimally Invasive Akin Osteotomy by Gerard Marciano, Beth G. Ashinsky, Nishad Mysore and Ettore Vulcano, MD in Foot & Ankle International
Footnotes
Ethical Approval
This study was completed with IRB approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.