
Abstract
Background
It remains unclear whether repairing the deltoid ligament (DL) is beneficial in acute ankle fractures. The aim of this review is to critically review the developments in deltoid ligament repair (DLR) in ankle fractures over the course of 44 years.
Method
An electronic search was conducted on the PubMed and Embase database including comparative studies evaluating the effect of performing DLR in adults suffering from a closed acute ankle fracture with suspected rupture of the DL.
Results
A total of 27 studies were retrieved, of which only one was a randomized study. A total of 1327 patients were reviewed (663 undergoing DLR and 664 receiving non-DLR treatment for an acute ankle fracture). Although earlier studies concluded that DLR holds little necessity in ankle fracture treatment if the anatomy of the ankle is restored, more recent studies support DLR due to more favorable clinical and radiographic outcomes.
Discussion
All studies agree that restoration of the ankle anatomy to its pre-fracture state is necessary to achieve the best clinical outcome. However, there is still controversy in whether to standardize DLR in ankle fracture treatment. The literature shows a clear shift toward more frequent restoration of the DL, and in light of improved surgical techniques and implants, there is a need for more rigorous studies to provide a clear indication for DLR in acute ankle fracture treatment.
Level of Evidence:
III
“The aim of this review is to critically review the developments in deltoid ligament repair in ankle fractures over the course of 44 years.
Introduction
The deltoid ligament (DL) constitutes a complex structure and is the most important medial stabilizer of the ankle joint. It originates at the medial malleolus and inserts into the calcaneus, navicular, and talus. 1 The DL is composed of a superficial (SDL) and a deeper portion (DDL), which restrain eversion of the hindfoot and external rotation of the talus, respectively. 2 Owing to pronation external rotation (PER) and supination-external rotation (SER) during rotational ankle fractures, the DL can be partially damaged or completely ruptured.3 -5 Injury of the DL is diagnosed in 40% of rotational ankle fractures. 3 This could result in instability, leading to abnormal anatomical position of the talus, opening of the medial clear space (MCS) and instability of the ankle joint.6 -10 Incorrect treatment of DL rupture potentially leads to chronic instability in the ankle joint and traumatic arthritis. 11 For decades, surgeons have grappled with the question of whether repairing the DL is beneficial in acute ankle fractures.12 -14 Since 1987, a considerable amount of techniques have been recommended as a treatment for DL rupture, ranging from suture anchors, graft reconstruction, simple primary repair, to non-operative management, even with usage of an external fixator.4,15 -17,18,19 In recent years, casting has mostly been used as treatment for DL rupture, whereas suture-anchor techniques have gained prominence in ankle fractures where surgical deltoid ligament repair (DLR) was deemed necessary.20 -22 Recommendations have changed in the past decades: earlier research suggests no significant difference between performing DLR or not, whereas more recent literature indicates promising outcome in the utility of DLR.16,23 Nevertheless, the decision of whether to repair a ruptured deltoid ligament in the context of ankle fractures remains unclear. The aim of this review is to critically review the developments in DLR in ankle fractures over the course of 44 years.
Materials and Methods
We aim to conduct a descriptive review of the current literature evaluating the outcome following DLR in ankle fractures.
Literature Search
In order to identify all relevant studies, we conducted an extensive literature search in PubMed and Embase using the Medical Subject Headings (MeSH) terms “deltoid ligament,” “Fractures, Bone,” “ankle,” “ligament rupture,” and “treatment.” In addition, reference lists of relevant studies and previous systematic reviews were searched manually for qualified studies. Primary screening was done on the title and abstract, and secondary screening was done on the full text article. The whole screening procedure was conducted by 2 reviewers independently (JVB and TS). Disagreement was resolved by discussion and a third observer (DP). Eligible were studies in adult patients evaluating the effect of DLR in acute ankle fracture cases. The identification, screening, and inclusion of studies are demonstrated in Figure 1.
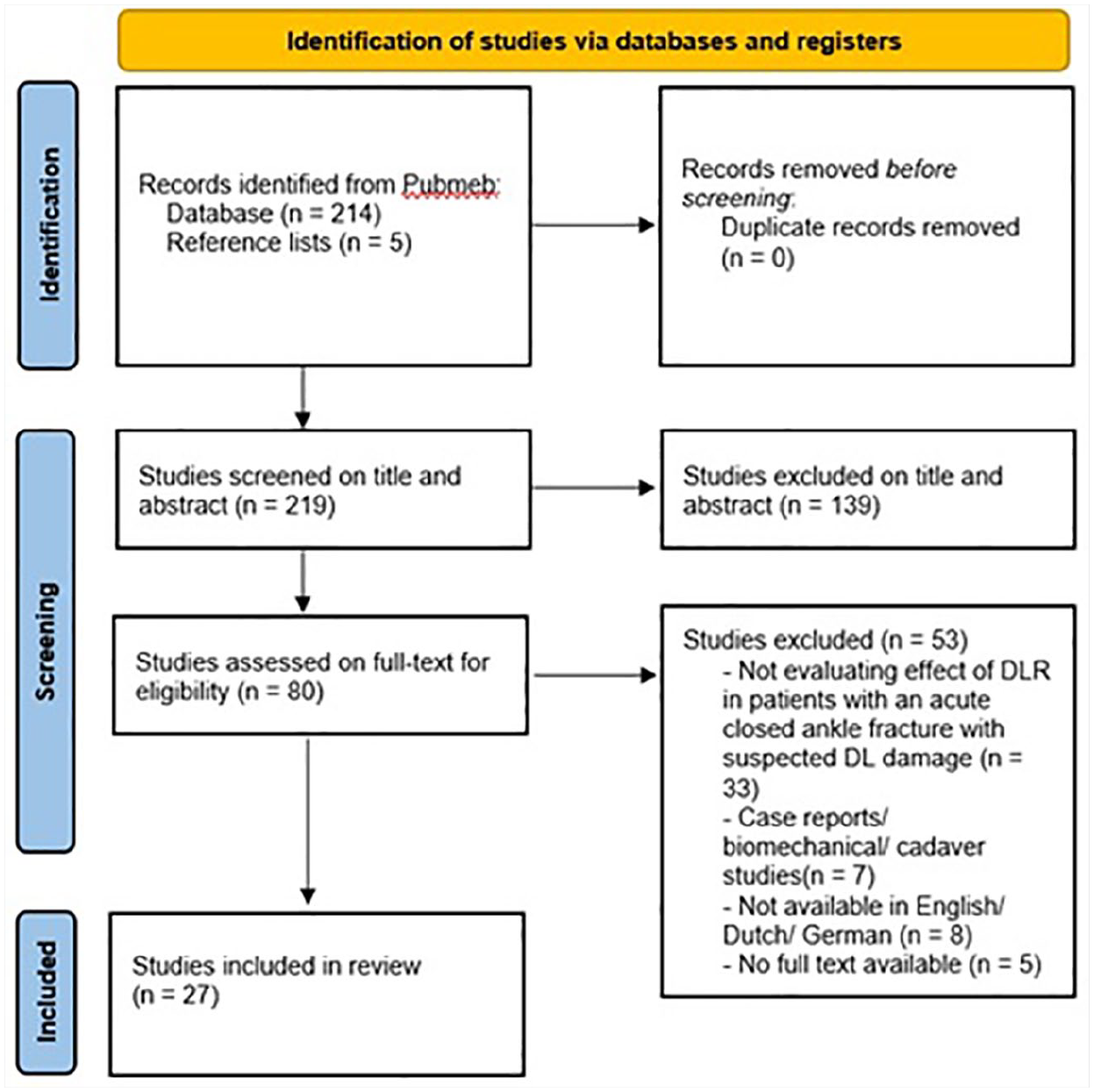
Study selection procedure.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows:
Comparative and non-comparative studies evaluating the effect of DLR in patients >18 years, with a closed acute ankle fracture with suspected deltoid ligament damage.
Studies with self-acquired data.
Full length available and published in a peer-reviewed journal.
Available in English, Dutch, or German.
Exclusion criteria were as follows:
Case reports, biomechanical studies, or cadaver studies.
Not available in English, Dutch, or German.
No full text available.
Data Extraction and Quality Assessment
We documented the type of study, study characteristics (name, year, level of evidence based on the methodological quality of their design, follow-up period), subjects’ characteristics (sample size and age), analyzed outcome parameters, complication rates, and key findings. The Newcastle-Ottawa Quality Assessment scale was used for quality and bias assessment of the studies. 24 The Newcastle-Ottawa scale examined quality for selection, comparability, and outcome.
Outcome Parameters
Based on the critical review, the following topics will be addressed to present the paradigm change over time and a missing conformity throughout the studies available:
Historical treatment trends.
How is deltoid instability diagnosed?
Do papers differentiate between DDL and SDL repair?
Do papers compare isolated syndesmotic treatment to deltoid ligament treatment and a combination of the two?
Does repairing the deltoid ligament in acute ankle fractures have beneficial outcomes?
Results
Study Selection
The outcome of the study selection procedure is illustrated in Figure 1. Our electronic search resulted in a total of 219 potentially relevant articles: 214 from PubMed and Embase and 5 found manually in potentially relevant reference lists. A total of 219 articles were screened on title and abstract. We assessed 80 articles in full text for eligibility after 118 studies did not meet the inclusion criteria and 21 studies met the exclusion criteria. Of the 80 articles, 53 did not meet inclusion criteria or met exclusion criteria: 33 studies were not evaluating the effect of DLR in patients with a closed acute ankle fracture with suspected deltoid ligament damage. Seven studies were case reports, biomechanical studies, or cadaver studies. Eight studies were not available in English, Dutch, or German. Five studies were not available in full text. Between 1987 and 2023, a total of 27 studies were eventually defined as eligible and included in the quality assessment.
Study Findings
A total of 27 studies were examined, including 1 level I evidence study by Stromsoe et al. 25 Seven studies were classified as level II evidence studies, whereas 10 studies held level III evidence status, and the remaining 9 studies were categorized as level IV evidence studies. Key findings from each study have been summarized in Table 1.
Summary of Included Studies Divided in Comparative and Non-Comparative Studies.
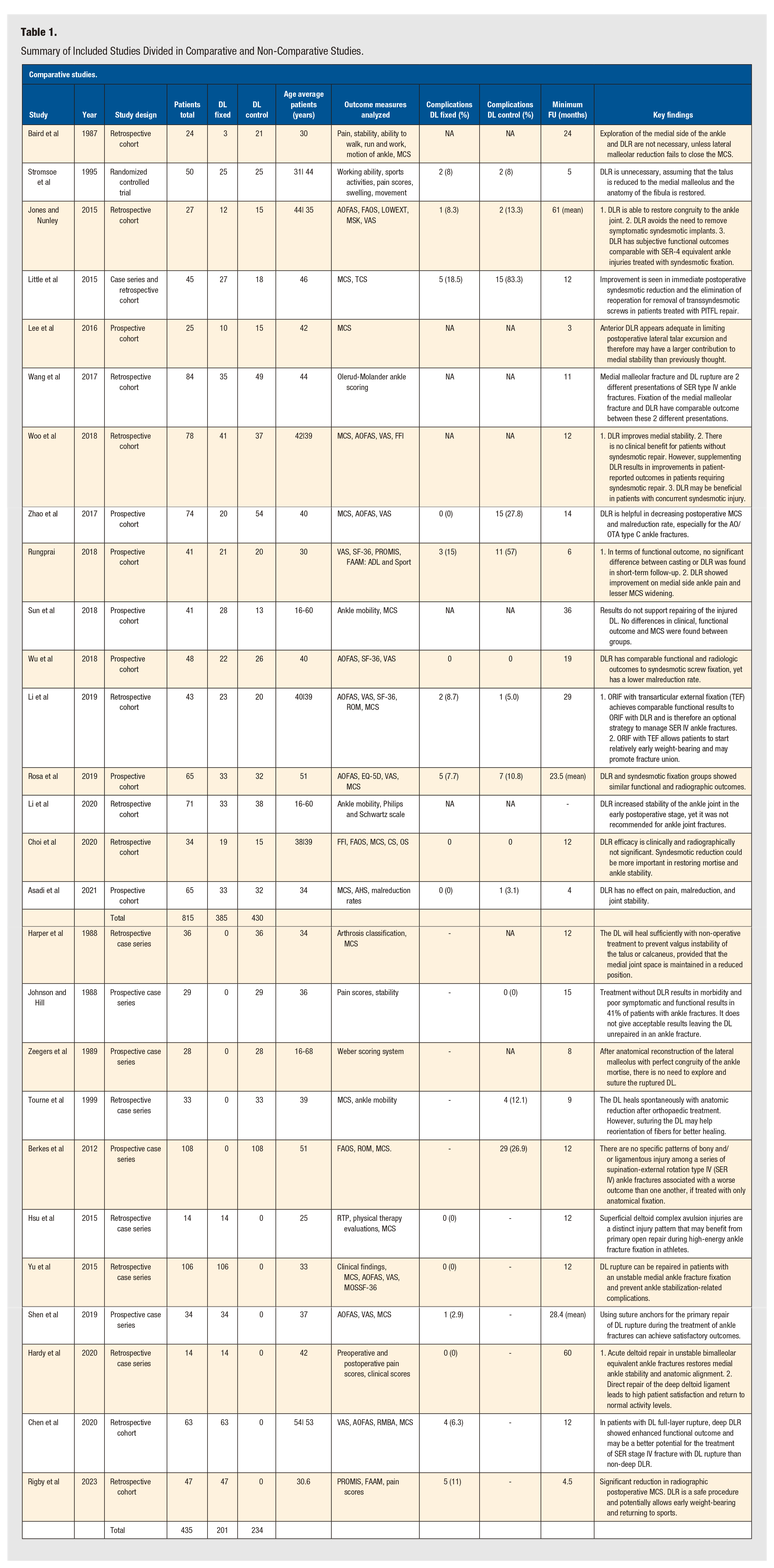

DLR: deltoid ligament repair. FU: follow-up, MCS: medial clear space, AOFAS: The American Orthopaedic Foot and Ankle Society score, VAS: visual analog scale, FFI: foot function index, NA: not available, ROM: range of motion, SF-36: 36-item short-form health survey, PROMIS: patient-reported outcomes measurement information system, RMBA: range of motion bilateral ankles, RTP: return to play, LOWEXT: lower extremity function scale, MSK: short musculoskeletal function assessment, EQ-5D: EuroQol survey, CS: clear space, OS: overlap space, FAAM: foot and ankle ability measure, MOSSF-36: 36-item short-form survey, AHS: Ankle Hindfoot Score.
In this comprehensive analysis, we reviewed a cohort of 1327 patients, with 663 patients receiving DLR treatment and 664 patients undergoing non-DLR treatment for acute ankle fractures. The repair techniques varied across studies, with some employing suture anchors and some utilizing fiber wire sutures. Researchers focused on various facets, including functional outcome, clinical evaluations, radiographic outcome, and post-treatment complications, all aimed at diagnosing deltoid instability.
The collective stance of the included studies toward DLR is illustrated in Figure 1 of the Supplementary Files, spanning different decades. During the 1980s and 1990s, Johnson and Hill found promising results for DLR following acute ankle fractures. 26 Among the patients treated without DLR, 41% exhibited morbidity and poor functional and symptomatic results. In contrast, 3 studies concluded that DLR was unnecessary for recovery and maintaining that anatomical reconstruction of the ankle mortise sufficed.15,23,27
Between 1990 and 2000, Stromsoe et al did not favor DLR, asserting that it showed no differences in long-term outcomes or early mobilization in cases where mortise anatomy was restored. 25 Tourne et al argued that DLR was unnecessary as it tended to heal spontaneously after anatomical reduction. However, Tourne et al also leaned toward DLR, because it might assist the deltoid ligament in reorientation of its fibers, which results in better healing. 28
Between 2000 and 2010, no studies meeting our criteria were identified. However, from 2010 to 2023, an impressive 14 studies presented promising results in favor of DLR after acute ankle fractures. Notably, DLR consistently led to enhanced ankle stability and a reduction in MCS.11,16,21,29 -33,34-37 Additional advantages included a reduced need for reoperation due to transsyndesmotic screw removal, as well as a lower incidence of malreduction and associated complications.21,29,38 Rungprai 33 underscored the significance of DLR in mitigating medial ankle pain, whereas Chen et al 34 concluded that deep DLR showed superior clinical outcome in terms of range of motion and pain scores, especially in cases involving full-layer deltoid ligament rupture. Nevertheless, 7 studies concluded that DLR had no better outcome than treatment without DLR.20,37,39 -43 When we narrow our focus to comparative studies exclusively, 8 studies favor DLR for achieving better outcomes, whereas 8 other studies suggest that DLR does not provide superior results compared with non-DLR treatment.17 -21,23-25,29 -33,36,38,40,42,44 This is illustrated in Figure 2 of the Supplementary Files.
Discussion
In this descriptive review, we delved into the question of whether DLR proves beneficial in the treatment of acute ankle fractures. Our study encompasses an analysis of 27 studies published between 1987 and 2023, aimed at providing a comprehensive overview of trends and outcomes over recent decades. We analyzed a total of 1327 cases, comprising 663 patients treated with DLR. Our review has unveiled a shift in recommendations concerning DLR.
Early studies predominantly advocated that DLR was unnecessary in the management of acute ankle fractures, emphasizing the importance of anatomical restoration. However, recent research paints a contrasting picture, suggesting that DLR significantly enhances long-term clinical outcomes. This shift is particularly noticeable in non-comparative studies, whereas comparative studies exhibit a more balanced division of support for DLR and studies with no better outcome when the deltoid ligament was restored. This discrepancy underscores the ongoing debate regarding standardizing deltoid ligament suturing during ankle fracture treatment.
Regardless of their stance on deltoid ligament suturing, all studies point out the imperative of restoring ankle anatomy to pre-fracture conditions to optimize clinical outcomes. Most studies converge on the notion that deltoid ligament suturing contributes to enhanced ankle joint stability, although in certain cases, there was no significant difference in the outcome. This suggests that the decision to suture the deltoid ligament may depend on the specific patient’s ankle joint stability and anatomy. Thus, the need for guidelines specifying when DLR is beneficial arises.
Between 1980 and 1990, the prevailing belief was that operative deltoid ligament reconstruction was unnecessary if the lateral malleolus was anatomically reconstructed and the ankle mortise was perfectly aligned.15,23,27 However, Johnson and Hill’s 1988 study marked an early indication that DLR yielded more favorable outcomes. 26 From 1990 to 2000, Stromsoe et al 25 set ground with a randomized controlled trial, asserting that DLR is unnecessary when fibular anatomy was restored and the talus was reduced to the medial malleolus. In 1999, Tourne et al concluded that the deltoid ligament could heal spontaneously, yet suturing it could aid in fiber reorientation and lead to improved healing. 28 This period marked a turning point in the recommendations for deltoid ligament suturing.
Between 2010 and 2023, numerous studies were published—all indicating that DLR has beneficial outcomes in ankle fracture treatment. These studies emphasized improved ankle stability, enhanced restoration of ankle anatomy and MCS, lower malreduction rates, and reduced postoperative pain scores as notable benefits of DLR. This trend toward more DLR could be the result of new techniques including bone anchors and arthroscopic approaches. Despite the evolving consensus, controversy surrounding DLR persisted. Five studies found similar clinical and radiographic outcomes in both DLR and non-DLR groups, further highlighting the need for more level I evidence.16,20,34,39,40
Complications following surgery with and without DLR were reported in 10 of 16 comparative studies, but the data were not sufficient to support definitive conclusions. Similarly, complications were documented in 9 of 11 non-comparative studies, with 3 studies reporting complications in the non-DLR group and 6 studies in the DLR group. The most common complications included malreduction, implant removal, and infection; however, the available data do not establish a causal relationship between these complications and the surgical method used. A detailed assessment of individual ankle joint instability and anatomical restoration in each ankle fracture could facilitate the development of more refined guidelines for the indication of DLR. Our data suggest that DLR is particularly beneficial when it aids in achieving closure of the MCS and restoring ankle anatomy, which is shown in Figure 2. However, when DLR does not contribute to these objectives, its impact appears minimal. Notably, patients who underwent potentially unnecessary DLR did not demonstrate worse clinical outcomes compared with those who did not receive DLR. Incorporating DLR into ankle fracture repair protocols could potentially improve clinical outcomes for a subset of patients, whereas the remainder may experience neither significant benefits nor drawbacks from the procedure. Finally, a number of DLR methods have been described, including the use of one or more suture anchors, bone anchors, and additional sutures.11,25,32,43,45 A strength of this review lies in the inclusion of the relatively large number of studies, both comparative and non-comparative, compared with previous reviews. However, limitations include the possibility of undiscovered bias in the included studies, heterogeneity among the studies, and the inclusion of only Dutch, German, and English studies. We also noted heterogeneity in the study designs and outcome measurements, which prompted us to analyze multiple outcome measurements to capture the nuances of the available data.

Pronation-external rotation type 4 ankle fracture with severe capsular and deltoid rupture and persistent instability (talar tilt, left picture) for which a bone anchor was added (middle and right picture). (No color).
Conclusion
The recommendation regarding deltoid ligament suturing in acute ankle fractures has evolved over recent decades. Although earlier studies suggested that DLR was unnecessary if ankle anatomy was adequately restored, more recent research and evolving techniques support DLR, citing superior clinical and radiographic outcomes. Nevertheless, debate persists regarding the standardization of DLR in ankle fracture treatment. Incorporating DLR into ankle fracture repair protocols could potentially enhance clinical outcomes for a subset of patients, whereas others may experience no significant benefit or harm from the procedure. In recent years, a growing attention is demonstrated in the literature toward repair of the deltoid ligament, which, combined with improved surgical techniques and implants, warrants further investigations. This will contribute to a more nuanced understanding of when and in which patients DLR is beneficial.
Supplemental Material
sj-docx-1-fas-10.1177_19386400241307817 – Supplemental material for Repairing the Deltoid Ligament in Ankle Fractures Is it time for a Paradigm Shift?
Supplemental material, sj-docx-1-fas-10.1177_19386400241307817 for Repairing the Deltoid Ligament in Ankle Fractures Is it time for a Paradigm Shift? by Joy Van den Berg, Diederick Penning, Sebastian Baumbach and Tim Schepers in Foot & Ankle Specialist
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.