
Abstract
Background
Autologous bone graft is the gold standard in orthopedics, with the iliac crest the most common harvest site. In an attempt to minimize morbidity with open bone graft harvest from the iliac crest and still maintain the benefit of collecting and transplanting live cells and growth factors, bone marrow aspirate concentrate (BMAC) from the iliac crest has become increasingly popular. However, any harvest procedure can potentially cause pain and complications. The purpose of this study was to evaluate the safety and complications of BMAC from the iliac crest for use in foot and ankle fusion procedures.
Methods
A retrospective chart review was performed on all patients who underwent BMAC harvest from the iliac crest with their foot or ankle procedure by 1 of 4 fellowship-trained surgeons (2014-2017) with a minimum of 6-month follow-up. Patients were evaluated for complications, pain, and functional limitation secondary to the harvest. The final outcome follow-up was conducted using a specifically designed telephone questionnaire to assess patient satisfaction. A total of 55 patients were included, with a median age of 58 years (range 31-81 years) and 69% were women.
Results
Out of 55 patients, 52 (94.5%) reported good to excellent results, and satisfaction with the procedure at the time of the questionnaire. Three patients reported persistent complications and some element of dissatisfaction after 6 months. Some patients reported transient complications (hematomas and numbness) that eventually resolved. Fifty percent of patients reported some element of immediate post-operative pain. However, at the time of final follow-up, only 2 reported persistent pain at the harvest site lasting up to 6 months, but it was not activity limiting.
Conclusion
BMAC harvest is a safe procedure with a high rate of patient satisfaction and minimal morbidity.
Levels of Evidence
Level IV: Case series
Keywords
“The iliac crest is well established as the gold standard harvest site for autologous bone grafting in orthopaedic procedures . . .”
Arthrodesis remains the gold standard surgical option for end-stage arthritis of the various joints of the foot and ankle. Achieving bone healing at the fusion sites can be challenging. Nonunion rates up to 40% have been reported in high-risk patients, even in primary foot and ankle fusion procedures.1-4 Thevendran et al 5 developed a nonunion risk assessment model to identify “total nonunion risk” in foot and ankle surgery. Several risk factors have been reported to increase the risk of nonunion, such as smoking, diabetes, immunocompromise, and avascular necrosis.1-5 Adjuncts are frequently needed to enhance healing and increase the likelihood of successful fusion in foot and ankle arthrodesis procedures.
Thordarson and Kuehn 6 reported comparative union rates with use of demineralized bone matrix (DBM) versus DBM plus crushed cancellous allograft bone chips for hindfoot and ankle fusion.
Bibbo el al 7 reported a high union rate of 96%, a mean time to union of 11 weeks, and an excellent safety profile with use of recombinant human bone morphogenetic protein–2 (rhBMP-2) in high-risk patients undergoing clean, elective ankle and hindfoot fusion surgery. High-risk factors in their study included smoking, diabetes, high-energy trauma, and history of avascular necrosis of the talus. 7
DiGiovanni et al 3 reported comparable fusion rates, less pain, and fewer side effects with use of Recombinant human platelet-derived growth factor-BB and beta-tricalcium phosphate (rhPDGF-BB/β-TCP) as compared with autograft in patients requiring hindfoot or ankle arthrodesis. Only patients who required supplemental bone graft on the basis of a number of clinical risk factors, including obesity, diabetes, prior surgery, smoking, and severe deformity, and radiographic risk factors, including periarticular erosion and bone voids not requiring structural graft, were enrolled in their prospective, randomized, controlled clinical trial. 3
McAlister et al 8 reported a 97% union rate with use of bone marrow aspirate (BMA) in 33 patients (29 forefoot, hindfoot, and ankle fusions, and 4 fractures).
The iliac crest is well established as the gold standard harvest site for autologous bone grafting in orthopaedic procedures, including foot and ankle. Complications associated with donor site harvest from the iliac crest are well documented, including infection, hematoma, lateral femoral cutaneous nerve injury (neuroma), chronic pain, persistent numbness, fracture, and hernia. Additionally, increased operating time, prolonged hospital stay and delayed recovery from the index procedure have been reported as other potential disadvantages of standard iliac crest bone graft harvest procedures.9-13
Given the morbidity associated with bone grafting, there continues to be a growing interest in finding alternatives, specifically in patients without bone voids or defects requiring a structural auto or allograft. An appealing alternative is bone marrow aspirate concentrate (BMAC). The use of BMAC to enhance bone healing outside the foot and ankle field has been reported in several studies particularly for the management of nonunion of tibia fractures 14 and for osteonecrosis of the femoral head as an adjunct to core decompression.15,16
BMAC has emerged as an option for obtaining bone cells and growth factors in foot and ankle surgery, including foot and ankle arthrodesis procedures to enhance healing, particularly in high-risk patients where nonunion rates up to 40% have been reported.1-4
The appeal of BMAC is that it allows the transplant of live cells and growth factors but is harvested via a percutaneous procedure. 17 With any procedure, however, there exists potential morbidity and complications possibly including hematoma, seroma, infection, lateral femoral cutaneous nerve injury, neuroma formation, chronic numbness, chronic pain, fracture of the harvest site, and incisional hernia.
The indications for the use of BMAC have been expanding and there has been a concomitant increase in the literature describing the use of BMAC in a variety of foot and ankle surgical procedures.8,17-25 The purpose of this study was to evaluate the safety of the BMAC harvest procedure from the anterior iliac crest performed as a part of various foot and ankle procedures.
Methods
After obtaining approval from our institutional review board, a retrospective chart review was performed of all patients who underwent BMAC harvest from the iliac crest at the time of their foot or ankle surgical procedure by 1 of 4 fellowship-trained foot and ankle orthopaedic surgeons between 2014 and 2017. The decision to use BMAC was at the surgeon’s discretion. For fusion procedures, BMAC was used mostly in high-risk patients, and with no bone defect or void that would requires a structural auto or allograft. The patients were identified using the appropriate Current Procedural Terminology (CPT) codes for bone marrow aspiration. Clinical charts and operative reports were reviewed for each patient and demographic information was documented. The procedure and follow-up time were also documented. Final outcome follow-up data for the cohort was obtained via a telephone questionnaire at least 6 months postoperatively evaluating complications, postoperative pain, functional limitation, and patient overall satisfaction with the BMAC harvest procedure.
BMAC Harvest Operative Procedure
The patient is positioned supine on the operating table. The harvest is done from the ipsilateral hip of the planned foot and ankle surgery. A bump is placed underneath the hip to help expose the iliac crest. The hip was prepped and draped in a standard sterile fashion. The anterior superior iliac spine (ASIS) is palpated and marked. Local anesthetic is placed around the harvest site. Then the BMAC harvest needle with a sharp trocar is introduced percutaneously through the skin approximately 3 cm proximal to the anterior superior iliac spine to avoid injury to the lateral femoral cutaneous nerve. The inner and outer tables of the iliac crest are palpated with the trocar, then the trocar is advanced in the midpoint of the iliac crest between the inner and outer tables, and in a trajectory parallel to the iliac crest. The sharp trocar is then pulled out and then 30 to 60 cm3 of bone marrow is aspirated, based on surgeon discretion. The harvested bone marrow is then processed per manufacturer’s instructions. The harvest site is then infiltrated with additional local anesthetic. Dressing was then performed using a gauze sponge and a small tegaderm.
In fusion procedures, which represent the majority of patients included in our study, the BMAC was mixed with Vitoss synthetic bone graft substitute (Stryker), either 2.5 or 5.0 cm3 based on the joint being fused, and surgeon discretion.
When used for osteochondral lesions of the talus, the BMAC was used with microfracture either alone or mixed with micronized allograft cartilage matrix (BioCartilage, Arthrex) based on size of the lesion and surgeon discretion.
Particular attention should also be given to the technique of aspiration. It has been shown that the aspiration speed is also important for cell yield. While rapid aspiration of large volume can have the potential advantage of saving operative time; however, it has been shown that it creates peripheral blood dilution of the bone marrow with subsequent reduction of the osteogenic progenitor cell count. In one study by Hernigou et al, 26 the authors compared the use of 10- and 50-mL syringes and reported improved cell yield with aspiration of small volumes of bone marrow using small syringes.
The BMAC harvest procedure did not require any additional specific postoperative limitation or dictate any specific activity/weightbearing restrictions, all patients were nonweightbearing postoperatively as dictated by the concomitant foot and ankle procedure. The dressing at the BMAC harvest site was removed by the patient after 4 to 5 days.
Results
A total of 125 patients underwent BMAC harvest from the iliac crest during the study period. Fifty-five patients responded to the final outcome follow-up telephone questionnaire and were included in this cohort. Among the respondents, the following procedures were performed: 21 midfoot fusions, 9 ankle fusions, 6 triple arthrodesis, 4 combination procedures (1 ankle and tarsometatarsal [TMT] fusion, 1 hallux and TMT fusion, 1 subtalar and TMT fusion, and 1 triple and TMT fusion), 3 subtalar fusions, 4 osteochondral defect excision w/ microfracture, 2 pan-talar fusions, 2 tibiotalocalcaneal fusions, 1 distal tibia/fibula syndesmotic fusion, and 1 revision total ankle arthroplasty.
The median age was 58 years (range 31-81 years) at the time of the procedure. A total of 69% were women. All patients had a minimum of 6-month follow-up (range: 6-45 months).
Complications
Sixteen percent (9 out of 55) of patients developed transient complications (Table 1) directly related to the BMAC procedure. Four patients developed a hematoma at the harvest site. All the hematomas were nonsignificant and were treated conservatively with eventual resolution and no sequelae in all 4 patients. Five patients reported numbness at the harvest site. The numbness resolved spontaneously in 4 patients, with 1 patient reporting persistent numbness at 6 months when the follow-up questionnaire was conducted. No patients developed an infection at the BMAC harvest site. No patients reported a fracture of the iliac crest. None of the patients in our cohort required any additional hospital stay related to the harvest procedure. Also, none of the patients in our series required any admission during the postoperative follow-up period as a result of a complication related to the BMAC harvest procedure.
Postoperative Complications.
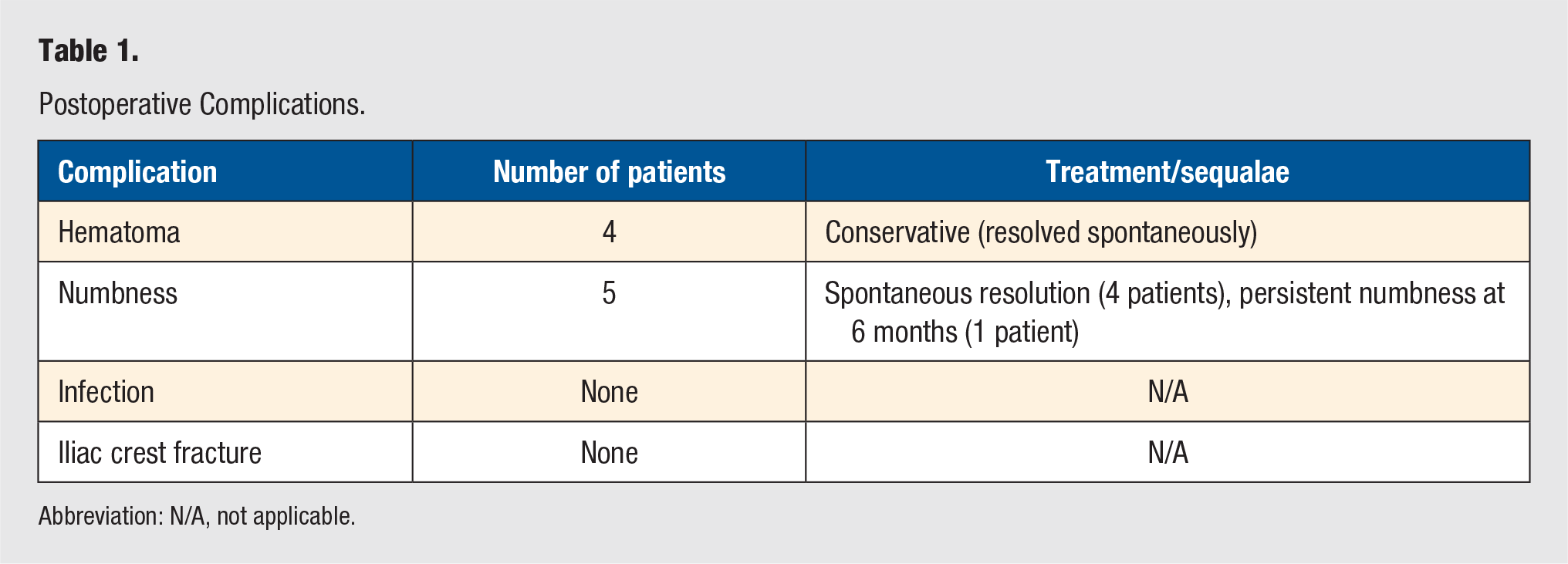
Abbreviation: N/A, not applicable.
Pain
Patients were asked to rate their postoperative pain (Table 2) at the harvest site on the visual analogue scale (range 0 = no pain to 10 = unbearable pain). A total of 50% of patients reported some level of immediate postoperative pain. In all, 64% (35 out of 55) rated their pain as 3 or less. A total of 20% (11 out of 55) rated their pain as between a 4 and a 6, and 16% (9 out of 55) rated their pain as greater than 7. At the time of the follow-up questionnaire, patients were also asked if their pain form the BMAC harvest limited their activities, and for how long. When asking the patients about activity limitation, we made sure to differentiate between activity restriction from the BMAC harvest and weightbearing status since all patients were nonweightbearing postoperatively as dictated by the concomitant foot and ankle procedure. Examples given for activity restriction during the telephone questionnaire include moving, sitting and showering. Of the 55 patients, 67% (37 out of 55) felt their activities were not limited at all. Of the 18 patients who felt their activities were limited secondary to the BMAC harvest pain, 56% (10 out of 18) were back to their usual activities within a few days, 22% (4 out of 18) were back within 1 to 2 weeks, 17% (3 out of 18) were back within 3 to 6 weeks, and 5% (1 out of 18) were back within 4 to 6 months. Of the patients who reported postoperative pain at the harvest site, only 4 patients reported more pain at the BMAC harvest site than from their foot/ankle procedure, and 3 patients reported the pain was similar in intensity at both the harvest site and the foot/ankle surgical site. The rest of the patients (48 out of 55) reported less pain at the harvest site as compared with the foot/ankle surgical site. At the time of the final follow-up telephone questionnaire, only 2 patients reported some persistent pain at the harvest site lasting up to 6 months postoperatively; however, it was not considered an activity-limiting pain.
Postoperative Pain.
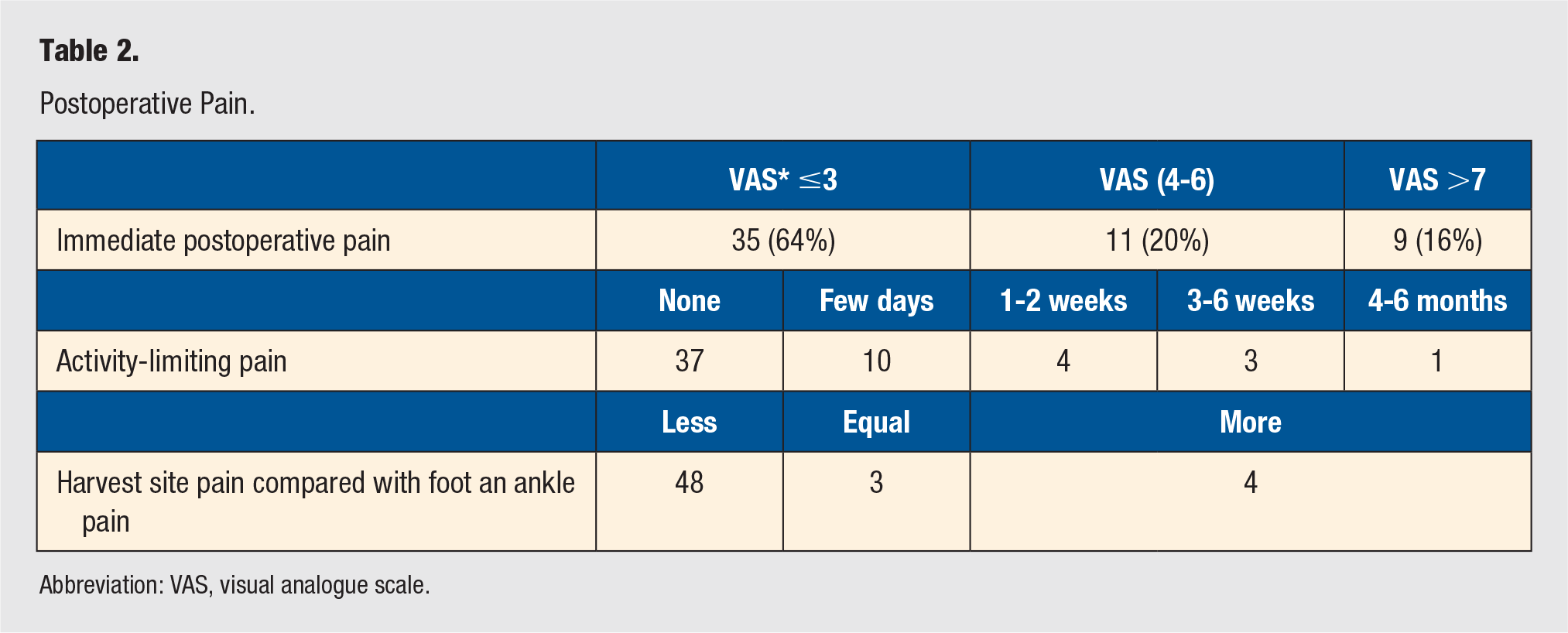
Abbreviation: VAS, visual analogue scale.
Overall Patient Satisfaction
Out of the 55 patients, 52 patients (94.5%) reported good to excellent results and were satisfied with the procedure at the time the questionnaire was conducted. Forty-seven patients (85.5%) would choose BMAC again and would recommend it to other patients. The 8 patients (14.5%) who would not choose or recommend the BMAC procedure include 7 patients who had greater than 7 pain at the harvest site postoperatively, and 1 who had persistent numbness at the harvest site. It is possible that these patients were also affected by the outcome of the concomitant foot and ankle procedure which was not assessed and is out of the scope of this study.
Discussion
BMAC is an increasingly appealing bone grafting option as it allows the implantation of live cells into the surgical site. BMAC from the iliac crest contains a high concentration of mesenchymal stem cells, hematopoietic stem cells, and endothelial progenitor cells in addition to various growth factors, including platelet-derived growth factor, transforming growth factor-β, and bone morphogenetic proteins 2 and 7.21,26,27 Mesenchymal and hematopoietic stem cells, with the assistance of growth factors, have the potential to differentiate into osteogenic progenitors. 22 The proposed benefit of the growth factors includes anabolic and anti-inflammatory effects. 27 Additionally, it is proposed that BMAC has a high concentration of interleukin-1 receptor antagonist, which inhibits catabolism and is thought to be partially responsible for pain relief. 27
BMAC can be harvested from numerous locations, including the iliac crest, proximal or distal tibia and calcaneus. While the distal tibia and calcaneus could be very convenient harvest locations in foot and ankle surgery, several studies have demonstrated that the iliac crest contains a more robust cell population with significantly higher mean concentration of osteogenic progenitor cells in comparison to the distal tibia and calcaneus. 27 Thus, we elected to harvest from the iliac crest.
Despite the relative paucity of literature in foot and ankle surgery regarding the use of BMAC, the few studies evaluating BMAC have reported positive outcomes, including decreased time to osseous union and decreased complications.
Hernigou et al 23 performed a case control study involving diabetic patients who sustained ankle fracture non-unions. These nonunions were treated with either iliac crest bone grafting or BMAC. Increased union rates were reported in the BMAC group (70 out of 86 patients, 82.1%) as compared with the bone graft group (53 out of 86 patients, 62.3%). Additionally, fewer complications were reported in the BMAC group (2%) as compared with the bone grafting group (11%). The complications seen in those who received bone grafting reached a statistically significant higher rate of skin necrosis, infection, amputation, and malunion. 23
Murawski and Kennedy 24 reported the results of 26 patients who underwent percutaneous internal fixation of proximal fifth metatarsal (Jones) fractures with concomitant BMAC injection. They reported union at a mean of 5 weeks postoperatively in 24 of their patients. They concluded that BMAC provides a more predictable result with few complications. 24
O’Malley et al 25 performed a similar study where they retrospectively reviewed the charts of 10 professional basketball players who sustained Jones fractures. Seven patients were treated with percutaneous fixation and BMAC injection and 3 patients had open bone grafting in addition to fixation and BMAC. The bone graft was obtained percutaneously through the same entry point for the aspiration, where the hollow trocar needle was used to obtain cores of tricortical bone graft from the iliac crest. They reported an average time to healing of 7.5 weeks; however, 3 patients refractured. 25
McAlister et al 8 reported a 97% union rate with use of BMAC in 33 patients (29 forefoot, hindfoot and ankle fusions, and 4 fractures).
There are several potential downsides to the BMAC harvest procedure. Although BMAC would be expected to have fewer complications as compared with the standard open bone graft harvest from the iliac crest, it is not without risks. Major complications were reported by Hernigou et al, 28 including retroperitoneal hemorrhage and death, although these complications were determined to be related to patients’ hematologic related pathology of myeloproliferative disorder and thrombocytopenia. The vast majority of their complications were considered minor, including small hematomas, numbness, superficial infections. 28
The incidence of complications in our study is in line with the documented results in other studies. Despite the concern for potential various morbidities and complications, there were only minor mostly self-limiting complications amongst our cohort. Although 50% of patients reported some element of postoperative pain, the majority of patients reported the pain as mild and did not consider the pain to be activity limiting. Only 2 patients reported some persistent, nonlimiting pain at the harvest site lasting up to 6 months postoperatively.
Another potential concern regarding the bone marrow harvest procedure is the potential increase in operative time associated with the procedure. However, the harvest is performed percutaneously, and the operative time is much less as compared with the standard bone graft harvest from the iliac crest. Additionally, the BMAC harvest procedure did not change the postoperative activity restrictions or weight bearing instructions for any patient. None of the patients in our cohort required any additional hospital stay related to the harvest procedure. Also, none of the patients in our series required any admission during the postoperative follow-up period as a result of a complication related to the BMAC harvest procedure.
There are several limitations of our study. First, this is a retrospective study with a relatively small number of patients. Second, the final patient evaluation was conducted via a telephone interview rather than a clinical evaluation. Patient response and willingness to participate in the survey was only 44% (55 out of contacted 125 patients). However, the goal of this study was to evaluate patient satisfaction and long-term safety, which we believe is adequately assessed via the phone interview. Third, there is recall bias from the retrospective nature of the study as patients were asked to remember their pain experience and incidence of complications up to 45 months after their procedure. Last, it is possible that the patients were affected by the outcome of the concomitant foot and ankle procedure which was not assessed and is out of the scope of this study.
There is a need for future studies to further evaluate the efficacy of BMAC in foot and ankle fusion procedures. This was outside the context of our study, as the aim of this study was to evaluate the potential morbidity associated with BMAC harvest.
Conclusion
The use of BMAC harvest in foot and ankle surgery is increasing. This study was intended to evaluate the safety of the BMAC harvest procedure from the anterior iliac crest in foot and ankle surgery. We conclude that the BMAC harvest is a safe procedure with a high rate of patient satisfaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.