
Abstract
Purpose
This paper presents an integrated framework combining perspectives from nursing, environmental psychology, and critical space theory. The framework is intended to support the study of materiality in ICUs and to inform future research on stakeholders’ needs and guiding design interventions for more supportive, healing care environments.
Background
Intensive care units (ICUs) are paradoxical spaces designed to save lives yet often experienced by patients as environments of dependency, disorientation, and loss of control. Materiality of the ICU environments can exacerbate stress and compromise recovery. While interventions addressing the material environment show promise in improving care experiences, existing approaches remain limited by single-theory perspectives that fail to capture the complexity of ICU materiality.
Methods
The integrated conceptual framework was developed through theory-informed synthesis guided by relevance to ICU settings and theoretical complementarity. Three established theories were synthesized—Roy's Adaptation Model, Ulrich's Theory of Supportive Design, and Lefebvre's Critical Theory on Space Production—using conceptual mapping across ontological, interactional, and interventional levels.
Results
The analysis revealed convergent points and complementary relationships across the three theories. The integrated framework synthesizes these perspectives across three interconnected dimensions: environmental stimuli and adaptive response, spatial production and power relations, and evidence-based supportive design.
Conclusions
The integrated framework demonstrates that healing ICU environments require interdisciplinary approaches addressing interconnected biological, psychological, social, and material dimensions simultaneously. Effective interventions must target adaptive physiological needs, reduce psychological stress through supportive design, and challenge spatial power relations that marginalize patients and families. This framework provides a foundation for research and practice that empowers all care-related stakeholders to actively shape healing ICU environments.
Keywords
Intensive Care Units (ICU) are paradoxical spaces, primarily designed to save lives, yet often experienced by patients as environments of dependency, disorientation, and loss of control (Tronstad et al., 2021a; Yang, 2016). Patients find themselves suddenly immersed in high technological and unfamiliar environments, where they often lose autonomy over their health, surroundings, decisions, and bodies (Tronstad et al., 2021a; Wilson et al., 2019). The material environment of the ICU, including constant noise, artificial lighting, and unfamiliar equipment, exacerbates stress, disrupts circadian rhythms, and impairs sleep (Kotfis et al., 2022; Oldham et al., 2016; Simons et al., 2018). These environmental stressors are strongly associated with physical, cognitive, and psychological complications that compromise recovery and overall well-being (Colbenson et al., 2019; Flaws et al., 2024; Kotfis et al., 2022; Tronstad et al., 2021a, 2021b; Tronstad et al., 2023; Wilson et al., 2019).
Despite these challenges, interventions addressing the material environment have shown promise in improving care experiences and fostering healing spaces (Tronstad et al., 2021a, 2021b; Tronstad et al., 2023). The concept of healing environment, first articulated by Florence Nightingale as “manipulating the environment to be therapeutic” (Nightingale, 1859), emphasizes optimizing the patient's capacity to recover. Since 1960, this notion has evolved alongside evidence-based design, supported by a growing body of research demonstrating its benefits for patients, families, and staff (Dovjak & Kukec, 2019).
Extending this perspective, the notion of materiality offers a deeper lens for understanding how healing environments are configured in ICUs. Design culture transcends simple dichotomies of “good” or “bad” design, adopting a more nuanced, interdisciplinary approach that acknowledges the complex social and cultural dimensions of designed environments (Attfield, 2000). Within this perspective, materiality refers to the intrinsic properties and sensory capacities of objects and spaces: the walls that structure space, lighting systems that regulate circadian rhythms, acoustic materials that shape sound environments, and medical equipment whose presence defines spatial relationships (Woodward, 2020). Material culture, in turn, provides the theoretical and methodological tools to analyze how these material elements are woven into daily life, conditioning gestures, interactions, and habits in ICU settings (Csikszentmihalyi, 1991; Saito, 2001; Woodward, 2020).
Seen through this lens, ICU environments are not neutral backdrops but active participants in care, conditioning how patients, families, and healthcare providers experience and enact healing. Importantly, healing environments must be defined inclusively, integrating the perspectives of all care-related stakeholders—patients, families, and healthcare professionals—as well as hospital administrators, facility managers, and public health policy makers who shape the organizational and resource contexts in which ICU environments are created and maintained. ICUs are not only technologically intensive but also socially and relationally intensive settings where continuous interactions occur among individuals and with the material environment itself (Hupcey, 2000; Leong et al., 2023; Tronstad et al., 2021a; Wilkinson, 1995). Understanding these multifaceted dynamics requires an interdisciplinary approach capable of capturing the interplay between human actors and material surroundings. Such a perspective is essential to conceptualize, design, and implement more supportive, human-centered ICU spaces (Bazuin & Cardon, 2011; Tronstad et al., 2023; Wilson et al., 2019).
Importantly, healing environments must be defined inclusively, integrating the perspectives of all care-related stakeholders—patients, families, and healthcare professionals…
Building on this need for an interdisciplinary and human-centered perspective, a conceptual framework that addresses both the material and experiential dimensions of ICU spaces becomes essential. Three theories are particularly relevant in this context: Roy's Adaptation Model (Roy, 2009), Ulrich's Theory of Supportive Design (Ulrich, 1991) and Lefebvre's Critical Theory on Space Production (Lefebvre, 1974). Each offers a distinct yet complementary lens. Roy's model explains how individuals physiologically and psychosocially adapt to environmental stressors (Roy, 2009). Ulrich's theory emphasizes the therapeutic potential of design elements in reducing stress and supporting recovery in healthcare settings (Dodeler, 2014; Ulrich, 1991), and Lefebvre's critical theory situates space as socially produced, shaped by experiences and embedded in power (Lefebvre, 1974; Shields, 2011).
The present paper presents the development of a conceptual framework that integrates these multidisciplinary and critical theories. The framework is intended to inform and guide future qualitative and quantitative research on ICU environmental materiality, in a perspective of a healing space. It was developed in the context of a master's thesis in nursing and will be applied to provide preliminary empirical exploration of how essential care-related stakeholders perceive a healing ICU environment, with attention to both materiality and design principles (Buse et al., 2018). By drawing on diverse yet complementary theoretical perspectives, this integrated framework aims to address the limitations of existing siloed approaches and offers a more nuanced analysis of how material environments impact care experiences in critical care settings.
Aim
This paper presents an integrated framework combining perspectives from nursing, environmental psychology, and critical space theory. The framework is intended to support the study of materiality in ICUs and to inform future research on stakeholders’ needs and guiding design interventions for more supportive, healing care environments.
Methodology
This is an integrated conceptual framework development through theory-informed synthesis guided by both relevance to ICU settings and theoretical complementarity. Unlike empirical qualitative studies that involve data collection from participants [and would follow SRQR reporting guidelines (O’Brien et al., 2014)], this work engages in conceptual analysis—systematically examining, comparing, and integrating existing theoretical perspectives to create a new analytical framework (Jabareen, 2009). The methodology follows established approaches for conceptual framework building in the health sciences.
The process involved identifying, analyzing, and integrating concepts from three established theories that address the concept of environment: Roy's Adaptation Mode (nursing science), Ulrich's Theory of Supportive Design (environmental psychology), and Lefebvre's Critical Theory on Space Production (social sciences and critical geography). These were selected based on three inclusion criteria: 1) their explicit focus on the interactions between individuals and their environments; 2) their applicability to healthcare or spatial ICU contexts; and 3) their capacity to inform material, perceptual, and experiential dimensions of healing environments (Figure 1).
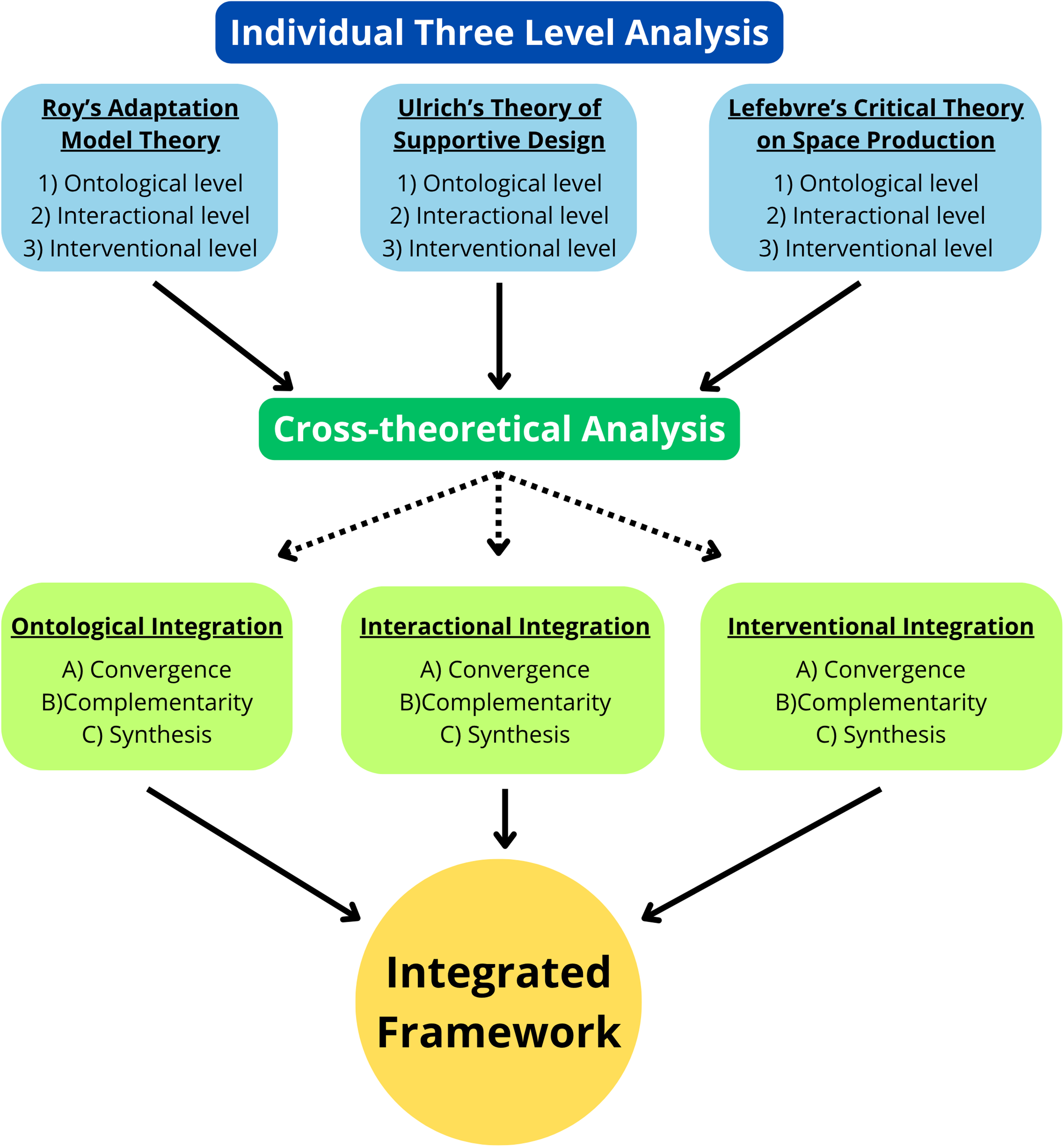
Graphical representation of the applied methodology for development of the integrated framework. Note. The figure illustrates the systematic three-step approach used for the building the integrated framework: 1) Individual three level analysis of Roy's Adaptation Model Theory, Ulrich's Theory of Supportive Design, and Lefebvre's Critical Theory on Space Production: analysis on ontological, interactional, and interventional levels; 2) Cross-theoretical analysis: triangulation of the individual analyses and synthesis from ontological, interactional and interventional integration perspectives; and 3) Integrated Framework: result of the integration of the three theories to create an integrated framework.
Several alternative theories were considered during the selection process but were not included in the final framework. Antonovsky's Salutogenesis theory, while relevant to health promotion, lacks specific focus on spatial and material environments (Antonovsky, 1996). Actor-Network Theory, though potentially valuable for material analysis, presented complexity challenges and lacks healthcare-specific applications (Latour, 2005). Planetary Health frameworks focus on macro-environmental rather than micro-environmental (bedspace) scales. The three selected theories were determined to offer the most comprehensive and complementary coverage of the phenomena of interest.
Addressing Epistemological Complementarity
The integration of these three theories requires acknowledgment of their different epistemological foundations. Ulrich's Theory of Supportive Design operated from a positivist/post-positivist paradigm, emphasizing measurable outcomes, controlled studies, and evidence-based interventions (Ulrich, 1991). Lefebvre's Critical Theory of Space Production adopts a social constructionist and critical lens, emphasizing how spaces are produced through social processes, power relations, and lived experiences (Lefebvre, 1974). Roy's Adaptation Model bridges these perspectives, as nursing science has historically integrated both empirical (physiological) and interpretive (psychosocial) approaches to holistic patient care (Roy, 2009).
We adopt a pragmatic approach to theoretical integration, similar to justifications used in mixed-methods research (Creswell & Plano Clark, 2018). While these theories emerge from different paradigmatic traditions, they address different dimensions of the same complex phenomenon—human experience in ICU environments. The integration occurs at the phenomenological level, seeking to understand the multifaceted nature of patient, family, and staff experiences, rather than attempting to reconcile fundamentally different truth claims. This theoretical pluralism enables the framework to capture both: (1) the measurable effects of design interventions; and (2) the socially constructed meaning of ICU spaces. Rather than viewing epistemological diversity as a limitation, we position it as a strength that reflects the irreducible complexity of human-environment interactions in healthcare settings.
Each theory contributed a distinct analytical lens. The perspectives of the three theories were synthesized using a conceptual mapping process, identifying shared and complementary concepts across three dimensions:
Ontological level: how space and environment are conceptualized Interactional level: how humans engage with the environment Intervention level: how the material environment can be shaped to support healing
Results
Roy's Adaptation Model Theory
Ulrich's Theory of Supportive Design
Lefebvre's Critical Theory of Space Production
Cross-Theoretical Analysis: Building the Integrated Framework
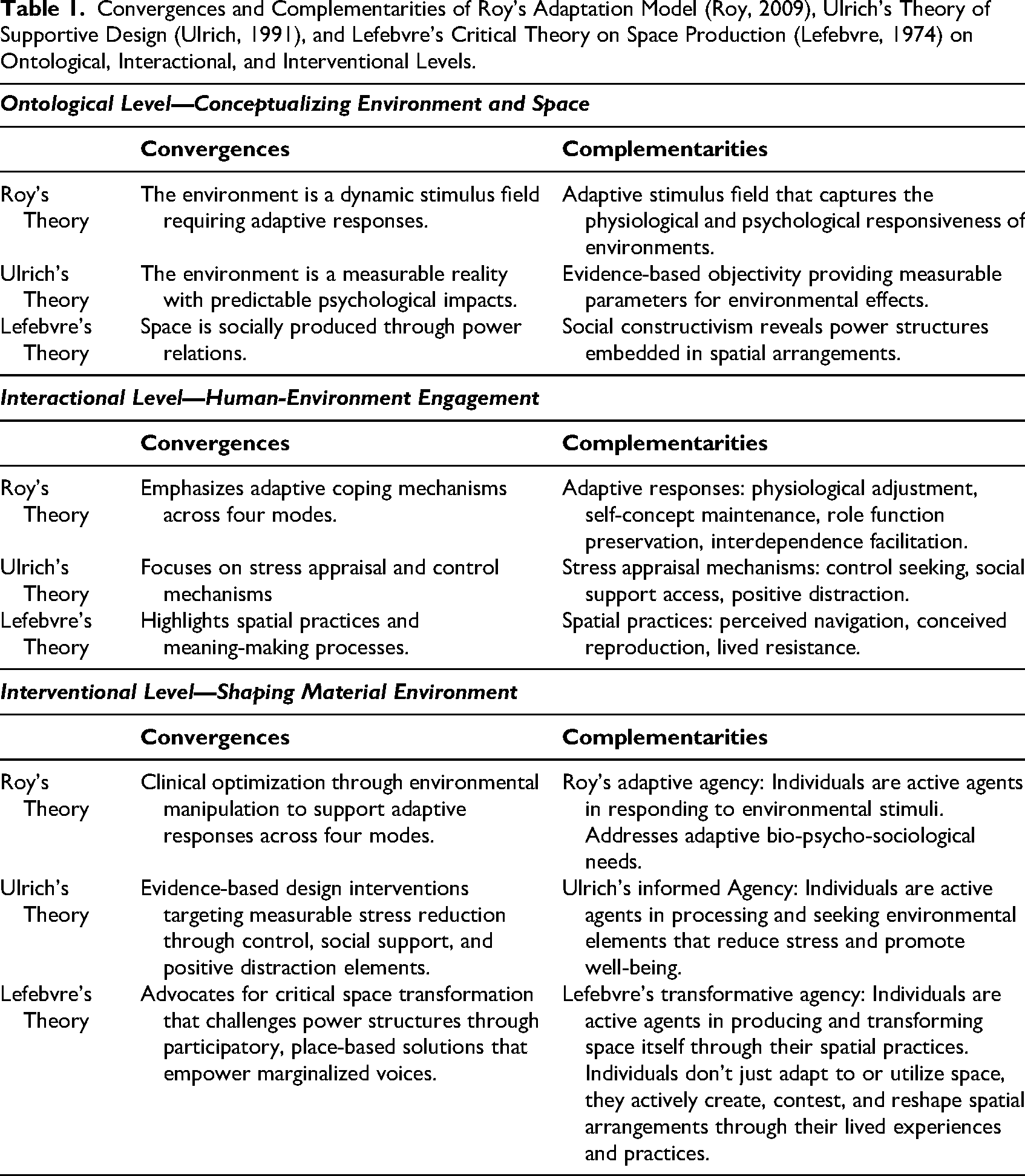
A comparative analysis across the three theoretical perspectives revealed convergent points and complementary relationships between them. Building on the three-level analysis of each theory presented in the previous section, the following table demonstrates the convergence and complementarity of these theories at the ontological, interactional, and interventional levels of analysis (Table 1).
Convergences and Complementarities of Roy's Adaptation Model (Roy, 2009), Ulrich's Theory of Supportive Design (Ulrich, 1991), and Lefebvre's Critical Theory on Space Production (Lefebvre, 1974) on Ontological, Interactional, and Interventional Levels.
Integrated Framework
The integrated framework synthesizes elements from three complementary theoretical perspectives to understand how ICU material environments can support rather than hinder healing and well-being: Roy's Adaptation Model, Ulrich's Theory of Supportive Design, and Lefebvre's Critical Theory of Space Production (Figure 2). The framework operates across three interconnected dimensions through which materiality transcends: Environmental stimuli and adaptive response, spatial production and power relations, and evidence-based supportive design.
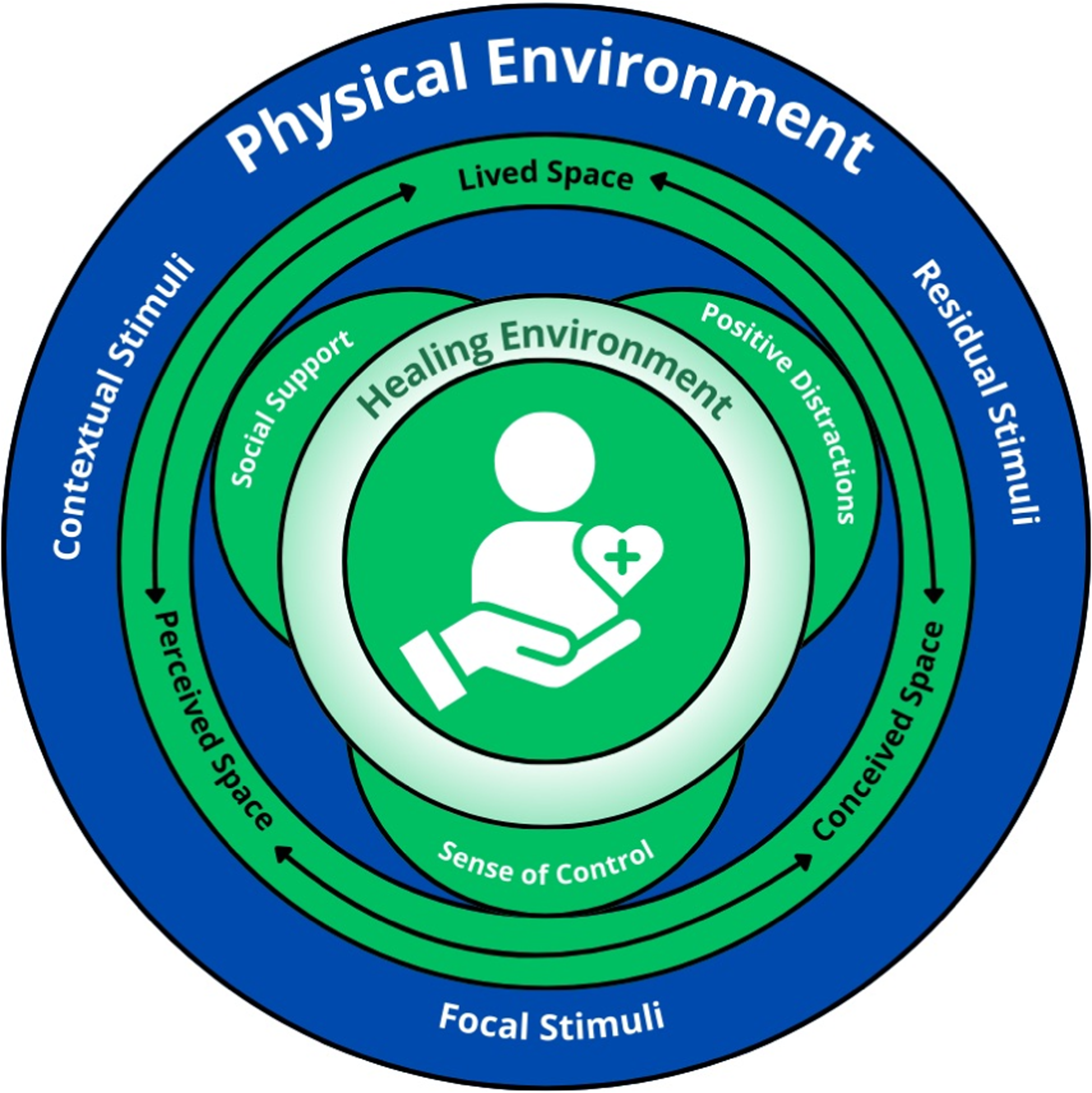
Integrated Framework for Healing Environments in the Intensive Care Unit (ICU). Note. The Integrated Theoretical Framework for Healing ICU Environments. This diagram presents the synthesized framework showing: (Center) The ICU healing environment as the goal of the analysis; (Three outer circles) Each theory's contribution— Ulrich's supportive design principles, Lefebvre's spatial triad, and Roy's Adaptation processes, (Connecting circles) The multidimensional and conceptual relationships between theories; (Inner ring) The framework should be read as a dynamic system where interventions at any point affect all other dimensions, requiring simultaneous considerations of adaptive, supportive, and critical perspectives.
By mobilizing this integrated perspective, the individuals immersed in the ICU are seen as individuals confronted with a continually changing material environment, loaded with stimuli to which they must adapt. The material environment thus becomes a lever for adaptation when it fosters elements that procure a sense of control, support social interactions and incorporate elements that act as pleasant, comforting distractions (Andrade & Devlin, 2015; Dodeler, 2014; Roy, 2009; Ulrich, 1991). These conditions foster a more favorable adaptive response and can reduce the stress associated with ICU hospitalization. To intervene appropriately on this material environment, it is essential to understand that spaces are simultaneously perceived through embodied navigation experiences, conceived through institutional design logic prioritizing clinical efficiency, and lived through emotional and symbolic meanings. Recognizing this spatial triad reveals how power structures are embedded in and can be challenged through material arrangements thus empowering individuals to challenge inequities and sculpt their material environments (Lefebvre, 1974).
The integration of the multiples perspectives resulted in identifying three common fundamental principles on which the framework is built. Firstly, emphasizing the centrality of human-environment relationships in health and well-being outcomes, the framework rejects passive conceptualizations of environmental influence in favor of dynamic, reciprocal interactions. Secondly, acknowledging the importance of human agency, whether through adaptive coping mechanisms, stress appraisal, control and social support seeking or spatial practices and meaning-making. Thus, referring to the capacity of individuals to act independently, make choices, and exert influence on their circumstances and environment. Thirdly, recognizing that environmental experiences are mediated by individual characteristics, contextual factors, and ongoing processes rather than deterministic cause-effect relationships.
Discussion
Framework Applications
The integrated model provides practical guidance for ICU design research and practice across multiple domains. For environmental assessment, the framework suggests evaluating ICU spaces simultaneously as adaptive stimulus fields (identifying focal, contextual, and residual stimuli), supportive design environments (measuring stress-reduction elements), and socially produced spaces (analyzing whose interests current designs serve). In intervention design, the model guides the development of comprehensive environmental modifications that optimize adaptive responses, implement evidence-based stress reduction strategies, and create opportunities for spatial reclamation. For hospital administrators and facility managers, the framework provides multi-dimensional justification for design investments by demonstrating how environmental interventions simultaneously address clinical outcomes (adaptation), patient/staff experience (supportive design), and equity considerations (critical spatial analysis). For public health policy makers, the framework illustrated how ICU design intersects with health system priorities including patient safety, workforce well-being, and healthcare quality improvement.
Illustrative Application: ICU Bedspace Redesign
To demonstrate the framework's practical utility, we present a detailed application to a common ICU design challenge: redesigning the patient bedspace. This example illustrates how the integrated framework produces more comprehensive analysis and intervention than any single-theory approach.
Integrated Intervention Design
The framework guides the development of interventions addressing multiples dimensions simultaneously. Example intervention: A “Family Zone” within the bedspace that includes comfortable convertible seating (Addressing interdependence adaptation AND social support), a small personal storage area for family belongings and patient's personal items (supporting self-concept adaptation AND challenging clinical dominance of space), adjustable lighting separate from clinical lighting (enhance sense of control AND supporting physiological adaptation to circadian rhythms AND enabling spatial reclamation for rest periods). This single intervention addresses Roy's four adaptive modes, Ulrich's three supportive design principles, and Lefebvre's call for challenging institutional spatial dominance—demonstrating the integrative power of the framework.
Framework Adaptability Across Contexts
Novel Insights for Healing ICU Environments
The framework demonstrates that healing environments cannot be achieved through single-theory approaches, as biological, psychological, social, and material dimensions of environmental experience are fundamentally interconnected. Environmental interventions may have contradictory effects across analytical levels—for example, technologically advanced adaptive features may support physiological needs while simultaneously reinforcing institutional power structures that marginalize patients. Sustainable environmental improvements require addressing not only immediate adaptive needs and stress reduction but also the underlying spatial practices and power relations that reproduce problematic environmental conditions over time. Effective healing environments emerge when interventions simultaneously address adaptive physiological needs, reduce psychological stress through supportive design elements, and challenge spatial power relations that marginalize patients and families.
Effective healing environments emerge when interventions simultaneously address adaptive physiological needs, reduce psychological stress through supportive design elements, and challenge spatial power relations that marginalize patients and families.
Limits
This theoretical integration has several limitations that should be acknowledged. First, as a conceptual framework synthesis, this work does not include empirical validation of the proposed integrated model in actual ICU settings. The framework was developed within the context of a master's thesis employing a qualitative approach to explore the materiality of adult ICU environments, with the aim to conceptualize the creation of healing ICU spaces. As such, future empirical research is needed to validate its practical applicability and effectiveness in guiding environmental interventions. Second, the selection of three specific theories, while justified by the inclusion criteria, may have excluded other relevant perspectives. Third, the interpretive synthesis may reflect the authors’ theoretical positioning in the way concepts were integrated across disciplines. Fourth, the framework's complexity, encompassing biological, psychological, and social dimensions, may pose challenges for implementation in practice settings where single-theory approaches are more familiar to healthcare teams. Fifth, although the framework addresses power relations and social justice through Lefebvre's theory, it may not fully account for specific cultural, ethnic, or socioeconomic factors influencing how different populations experience ICU environments. Sixth, the framework focuses primarily on the care experience and would benefit from fuller integration of organizational and economic perspectives relevant to administrative decision-making. Finally, while guidance has been provided on adapting the framework for different resource levels and populations, empirical validation in these varied contexts remains necessary.
Conclusions and Recommendations
The integrated framework developed in this study offers a novel, multi-dimensional, and interdisciplinary approach to examining the perceptions of key stakeholders regarding healing environments in ICUs. It underlines the limits of a single theory approach for capturing the complexity of ICU materiality and demonstrates how the integration of disciplinary and critical perspectives provides a more comprehensive foundation for research and practice encompassing biological, psychological, social, and material dimensions of healing environments simultaneously. By bridging theory and practice, this framework offers a structured lens to explore materiality in the ICU environment although its future validation through applied research is needed.
To support its application, several recommendations can be proposed: (1) Use the framework as a boundary object to facilitate interdisciplinary dialogue among stakeholders from clinical, design, administrative, and patient/family perspectives. (2) Adapt the framework to local resource contexts while maintaining attention to all three theoretical dimensions. (3) Validate the framework through empirical research across diverse ICU settings. (4) Consider its potential to inform policy development for ICU design standards that address not only clinical functionality but also patient experience and equity.
This framework holds significant implications for ICU practice by informing design and organizational interventions aimed at enhancing the overall care experience. By emphasising person-centred care and the humanization of ICUs, it contributes to advance knowledge on healing environments and supporting improved patient experiences and outcomes. The framework thus provides a foundation for future research aimed at better conceptualizing, understanding and operationalizing the healing environment across varied ICU contexts.
Footnotes
Implications for Practice
It provides the first systematic integration of nursing, environmental psychology, and critical spatial theories specifically addressing ICU materiality It offers practical guidance for ICU design research and practice across multiple domains, from environmental assessment to comprehensive intervention design It empowers all care-related stakeholders—patients, families, and healthcare professionals—to actively shape healing ICU environments It bridges theory and practice, providing structure for both researchers and practitioners working to create more supportive critical care spaces.
Acknowledgements
The authors would like to thank the Canadian Institutes of Health Research (CIHR), the Ministry of Higher Education (MES), the Bureau de coopération interuniversitaire (BCI), the Faculty of Graduate and Postdoctoral Studies (FESP) at Laval University, and the Canadian Nurses Foundation (CNF) for the various grants that EP obtained for this project.
Ethical Considerations
Ethical approval was not required for this theoretical research paper.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EP received funding support from the Canadian Institutes for Health Research (CIHR), the Bureau de coopération interuniversitaire (BCI), Quebec's Ministry of Higher Education, the Laval University Faculty of Higher Education and Postdoctoral Studies (FESP) and holds a Canadian Nurses Foundation (CNF) Scholarship. This funding supported his master's degree in nursing research, of which this publication forms part of his thesis work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Not applicable.