
Abstract
Purpose:
The purpose of this study was to explore the relationship between situation awareness (SA) and the physical environment in patient rooms through building a conceptual model.
Background:
Nurses work in very complicated and dynamic environments where having high levels of SA could be critical for their performance. Studies have also shown that nurses’ awareness of the physical environment and patient room is a part of their awareness of dynamic situations in which nurses’ spatial awareness may play a role in SA. Despite literature outlining the importance of SA, there is a lack of studies exploring the relationship between the two.
Method:
A literature review was conducted for the study from nursing and psychology databases. Thirty-three articles, books, and dissertations from a scoping review were included for in-depth review.
Results:
An in-depth review of the harvested literature indicated that there is in fact a relationship between these two phenomena. Founded on Endsley’s model of SA, the literature review in this study offers a conceptual model that articulates a plausible causal pathway between the physical environment and SA.
Conclusions:
There are a lot of studies focusing on SA and various aspects of it related to nursing, but almost none mention the physical environment and its impact on SA. The current inquiry suggests that spatial awareness plays a prominent role in SA.
Introduction
“Situation awareness [SA] is the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future” (Endsley, 1995, p. 36). SA is an important and critical aspect of dynamic and complex situations where decision making and performance of individuals are critical for properly accomplishing tasks in high-risk environments (Brady & Goldenhar, 2014; Endsley, 1995; Endsley & Jones, 2012; Gaba et al., 1995; Hamilton, 2017; Hinton, 2011; Orique & Despins, 2017; Schulz et al., 2013; Sitterding et al., 2012; Stubbings et al., 2012; M. C. Wright et al., 2004). There is a growing body of literature in which SA has been thoroughly explored in various fields that require split-second decision making, such as aviation, military, large systems, safe driving, power plants, emergency management, and healthcare (Endsley, 2015, 2021; Orique & Despins, 2017).
Although SA has been examined in the context of healthcare facilities (Brady & Goldenhar, 2014; Endsley, 1995; Endsley & Jones, 2012; Fore & Sculli, 2013; Gaba et al., 1995; Hamilton, 2017, 2020; Hinton, 2011; Orique & Despins, 2017; Schulz et al., 2013; Sitterding et al., 2012; Stubbings et al., 2012; M. C. Wright et al., 2004), few studies have considered the ambient physical environment as a potential contributor to SA. After all, all situations occur in a physical setting. It may be plausible that the physical environment plays a role in SA, thereby leading to a key unexplored question about the role of the awareness of the ambient physical environment of care delivery in enhancing SA. According to Hamilton (2017, p. 40), “being continuously aware of the physical environment and one’s location within space describes spatial awareness.”
Among the clinicians, most impacted by SA are nurses. Those who serve in acute care units work in complicated environments with high cognitive load and multitasking. According to published literature, they usually perform 100 tasks per shift with interruptions that add to their cognitive load (Potter et al., 2005; Sitterding et al., 2012; Tucker & Spear, 2006). Quality of care and patient safety are among the most important aspects of care delivery, in which having higher levels of SA is deemed necessary for providers to make the right decisions and improve clinical outcomes (Fore & Sculli, 2013; Hamilton, 2017; Stubbings et al., 2012; Tower et al., 2019). Nontechnical skills including SA play an important role in improving cognition and consequently enhancing decision making among clinicians (Fletcher et al., 2003; Guimond et al., 2009; Marshall & Finlayson, 2018; Mitchell & Flin, 2008).
Consequently, if spatial awareness does impact SA, it is incumbent upon healthcare design researchers to examine the association to reduce or eliminate avoidable errors such as failure in rescue, falls with injury, medication errors, and patient misidentification. Two questions drove this inquiry: (1) Is there a plausible conceptual/theoretical link between SA and spatial awareness; and (2) What elements/attributes of the physical environment could potentially affect SA? The inquiry focused exclusively on nursing tasks.
Method
The first step in establishing the literature review that was used to build the conceptual model in this study was to complete a scoping review of relevant literature linked to SA. A comprehensive search of three prominent databases in healthcare, nursing, and psychology— Medline Complete, CINAHL Complete, and APA PsychInfo—was conducted to locate and extract data that either supported or rejected different elements of SA. The search started with the key term “Situation Awareness” and was then expanded to include terms related to SA or the study subject, such as “Spatial Awareness,” “Nurse,” “Acute Care,” “Clinical Awareness,” and “Decision Making.” The search began in April 2021, concluded in May 2021, and was limited to peer-reviewed articles and dissertations in English published after 2010. This delimitation meant that the results were limited to recent studies, as SA is a relatively new area of exploration in nursing and healthcare. This initial search resulted in 424 publications, of which 106 duplicated publications were excluded. Next, 192 and 88 studies were excluded after reviewing titles and abstracts, respectively, as they were off topic of SA among nurses in healthcare. An additional 13 studies were excluded as they were not related to the scope of this study. At this point, the reference sections of the remaining publications were reviewed, resulting in an additional eight publications being added. In total, 33 articles and dissertations were selected (Table 1).
Overview of Reviewed Literature Sources.
Note. ICU=Intensive Care Unit, ED=Emergency Department, OR=Operating Room
During the initial phase of the review, the authors located an original model on SA by Endsley (1995). This model, alongside research conducted previously by one of the authors, was used to construct the conceptual model included in this study. The research collected was then used to validate its elements based on the data from the literature. Due to its size, the model was separated into five categories: the levels of SA, sources of perception, types of comprehension, SA and attention, and SA and clinical action decisions. Each of the 33 research sources were thoroughly reviewed and any information related to SA, whether directly or indirectly, was extracted into these five categorized sections.
Results
Data analyses identified a complex network of associations between various aspects of human cognition, clinical decision making, SA, elements/attributes of the physical environment, and spatial awareness in a theory-driven plausible relationship structure. Key findings are sequentially presented in the following sections: the levels of SA, sources of perception, types of comprehension, SA and attention, and SA and clinical action decisions. These categories were derived from a literature review and analysis of the collected research sources, utilizing the conceptual model developed by Endsley (1995) and the prior research conducted by one of the authors. It is important to note that these categories are not mutually exclusive but rather interconnected components of the theoretical framework. The relationships between the categories demonstrate the complex interplay between different aspects of situation awareness, cognition, and clinical decision making. For example, the sources of perception directly impact the levels of SA, and the types of comprehension significantly contribute to the accuracy and depth of nurses’ SA. Additionally, SA and attention interact closely, as attentional processes shape the acquisition and maintenance of SA. Ultimately, SA and clinical action decisions are closely interconnected, as nurses’ SA directly influences their ability to make informed decisions and take appropriate actions.
Three Levels of SA
According to Hamilton (2017) and Endsley (1995), SA begins as a cognitive process (perception), leading to comprehension, and then to action initiation. SA is a split-second process, and these three levels begin and end almost simultaneously without being temporally separated (Figure 1). Endsley (1995, 2015) categorized SA into three ascending levels. The first level of SA is to perceive the situation including status, attributes, or elements (Endsley, 1995), in which relevant clinical information from the environment is acquired, without any associated processing of data (Fore & Sculli, 2013; Sculli & Sine, 2011). In the second level, the mechanism of information processing including attention and memory plays an important role in SA and are often affected by time, goals, and objectives (Endsley, 1995; Endsley & Jones, 2012; Fore & Sculli, 2013). The translation of received data occurs based on a nurse’s education and experience, resulting in comprehension of a situation. And finally, the ability to predict and project possible future actions and status, in the near future, forms the third and highest level of SA (Fore & Sculli, 2013). In essence, failure in perception can negatively affect the interpretation of information, which can lead to compromised projection and decision making, all decreasing the level of SA (Stubbings et al., 2012; Woodward, 2010; Yule et al., 2008).
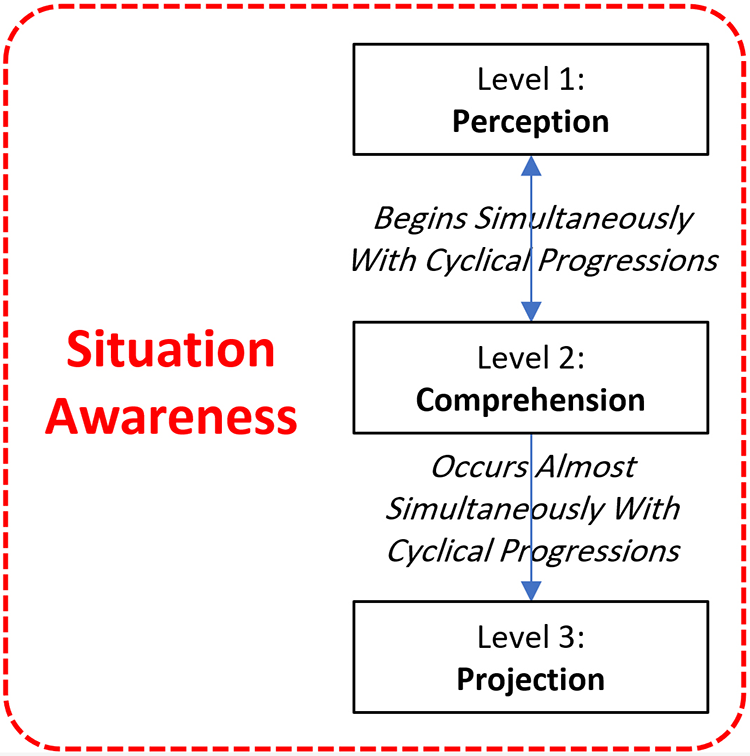
Three levels of situation awareness.
Sources of Perception
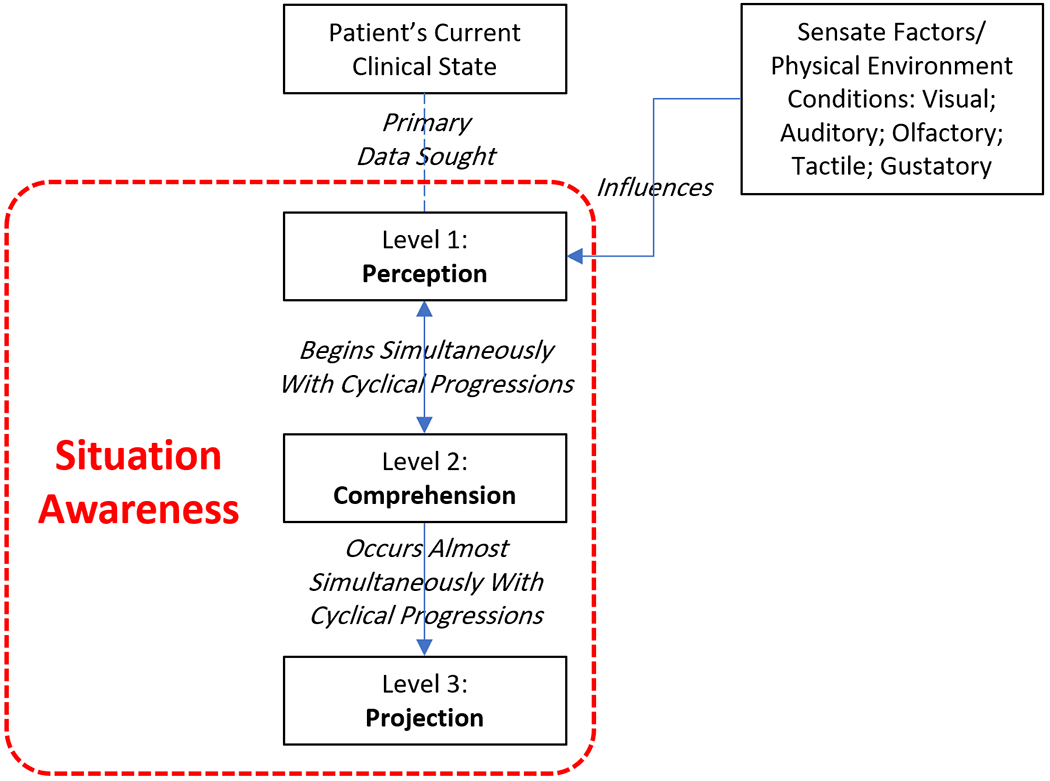
The first level of SA is to perceive the situation including status, attributes, or elements (Endsley, 1995). Among the information instantaneously acquired on initial exposure to a patient are the patient’s current clinical condition, equipment and life support systems attached to them, and readings/status indicated on the latter during the first level of SA (Hamilton, 2017). As shown in Figure 2, acquiring this information is not independent of sensate factors including ambient visual, auditory, olfactory, tactile, and gustatory stimuli (Hamilton, 2020; Rew, 1996). Of the sensate factors, visual, auditory, and tactile stimuli are directly determined by the physical design of the care environment. Olfactory and gustatory stimulus, it could be argued, are partially affected by the design of the environment, depending on ventilation design, materials, and other factors. Received physical environment stimuli also include valuable information on potential affordances in the ambient care environment, which are critical for the comprehension and projection phases of SA. In simple terms, affordance represents qualities/properties of the physical environment that offers possibilities of different use scenarios—“According to the ecological approach, what we perceive are the affordances of the environment” (Heft, 1997, p.80). Perceived affordances could vary from person to person—potential use scenarios an individual sees or senses in the environment might not be seen or sensed by another person, or depending on the location, people may see or sense it differently (Clapper et al., 2018). This phenomenon is related to training and experience, which is addressed later, but is an essential aspect of the perception phase of SA that is directly linked to the physical environment.
Parameters influencing the perception level of situation awareness.
Two Types of Comprehension in SA
In order to make the most effective decisions, healthcare professionals must efficiently recognize the relevant information about the situation including patient and environment (Stubbings et al., 2012). According to Dominguez, continuous extraction of information from the environment, incorporation of knowledge, and creation of a clear picture in mind to direct perception and expect future events are very important for safe decision making (Dominguez, 1994; Stubbings et al., 2012). Comprehension level of SA can be categorized into two types: clinical comprehension, which has been examined in current literature, and physical environment comprehension, which is absent in published literature (Figure 3). In the second level of SA, information processing mechanisms including attention and memory play an important role in SA and are often affected by cue salience, goals, and objectives (Endsley, 1995; Fore & Sculli, 2013). Nurses rely on their education, training, and experience for clinical comprehension. It can be argued that clinical comprehension may not achieve optimization without comprehension of the physical environment. Decisions on potential actions in case of emergent situations are affected by things that are possible within the constraints of the ambient physical environment. Hamilton (2017) asserts that SA incorporates knowledge of the space and physical resources, which is consistent with a broader human factors perspective. The knowledge of the ambient space and physical resources is spatial awareness. According to Hamilton (2017, p. 40), “being continuously aware of the physical environment and one’s location within space describes spatial awareness.” Implicit awareness of the physical environment and its elements might enhance the efficient and effective use of the space in reaction to emergent situations, which could be considered as spatial competence (Hamilton, 2017). The nurses’ awareness of the broader physical environment, in general, and the patient room, in particular, is a part of a nurse’s awareness of the dynamic situation, in which spatial awareness of the nurse may play a role in SA (Hamilton, 2017). Spatial abilities, visual scanning, and high rates of interruptions are other factors affecting SA (Sitterding et al., 2014; Weigl et al., 2020). An individual’s spatial description of an environment stored in long-term memory is called a cognitive map (Hamilton, 2017). A cognitive map of the broader physical environment and the patient room is unconsciously generated and continuously updated in a nurse’s mind, according to information processing theories, which is moderated through experience and knowledge (Hamilton, 2017). According to Hamilton, “A mental model or mental map of the unit floor plan, or the arrangement of the patient room and its features, can serve as a cognitive artifact that reduces the nurse’s memory load” (2017, p.35). Implicit and explicit awareness of the physical environment and its elements might impact the efficient and effective use of the room. There is a relationship between the awareness of the physical environment and sequencing and ordering of planned activity and efficiently navigating within clinical environments (Hamilton, 2017). Consequently, it could be reasonable to assert a connection between spatial awareness of nurses and spatial competence in a patient room environment (Hamilton, 2017).
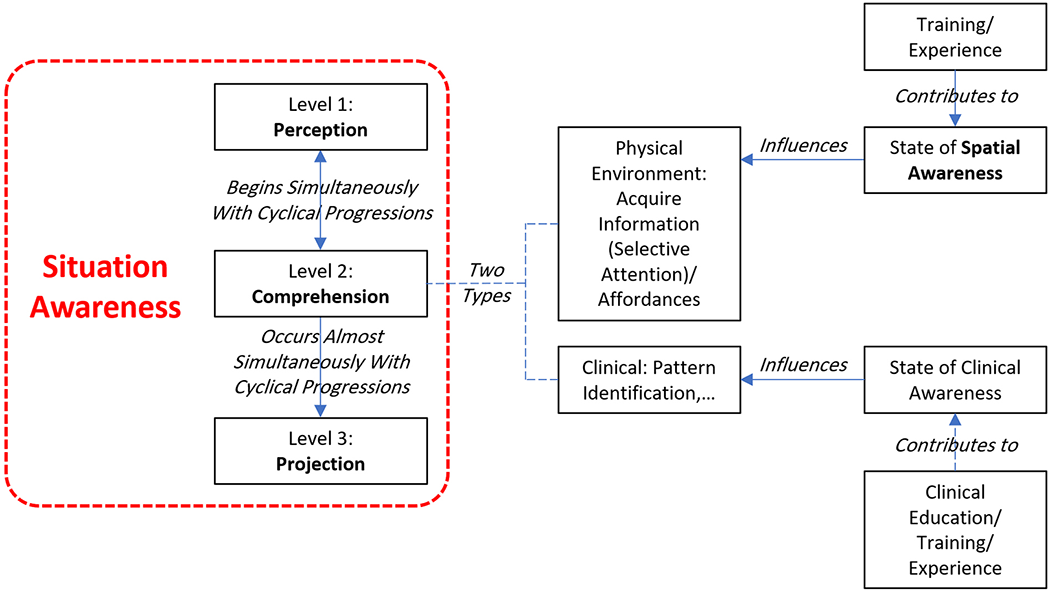
Two types of comprehension level of situation awareness.
According to Stubbings and her colleagues (2012, p.8), “achieving consensus on SA in clinical settings is greatly enhanced by education and training practices that incorporate interprofessional learning.” However, the authors of a research (Nibbelink & Brewer, 2018) believe that the relationship between education and clinical decision making is not clear and education should not be considered as only factor on efficiency of decision making. When professionals take training, certification, or recertification, they are, in fact, increasing their capability for maximizing situational awareness (Fore & Sculli, 2013; Stomski et al., 2018). Training can enhance SA and consequently decision making among nurses (Despins et al., 2019; Endsley & Garland, 2000; Stubbings et al., 2012).
SA and Attention
There is a possible association between conscious and unconscious attention and SA (Figure 4). Since attention affects human performance, it is important to explore and examine it in the context of SA. To perceive and understand the nature of a clinical situation, it is crucial for nurses to optimize attention (Sitterding et al., 2012). Healthcare providers need a constant state of attention to appropriately respond to unexpected situations with the capacity to perceive multiple points of data, conditions, and disparate decision making (Sitterding et al., 2012). According to Weigl and his colleagues (2020), SA is a cognitive capacity, in which interruptions can negatively affect cognitive processes and decision making. There are many distracting factors, which can potentially decrease the level of SA among nurses including stress, fatigue, interrupted workflow, time pressure, noise, multitasking, and physical factors like tiredness affecting attention (Stubbings et al., 2012; Woodward, 2010; Yule et al., 2008). Attention should also be viewed in relation to memory, both of which are elements of information processing that can impact SA (Fore & Sculli, 2013). Interruptions can increase memory load, and working in low interruption environment has direct relation with increased SA (Weigl et al., 2020). When people face any breakdown, interruption to the flow of tasks, or an imbalance between demand and capacity of mind, it is considered a situation described as cognitive overload (Sitterding et al., 2012). There is also another concept that might be related to physical awareness. The concept of proprioception is a form of bodily self-awareness that explains an individual’s understanding of their environment and how they are oriented in the physical environment and among objects (Hamilton, 2017).
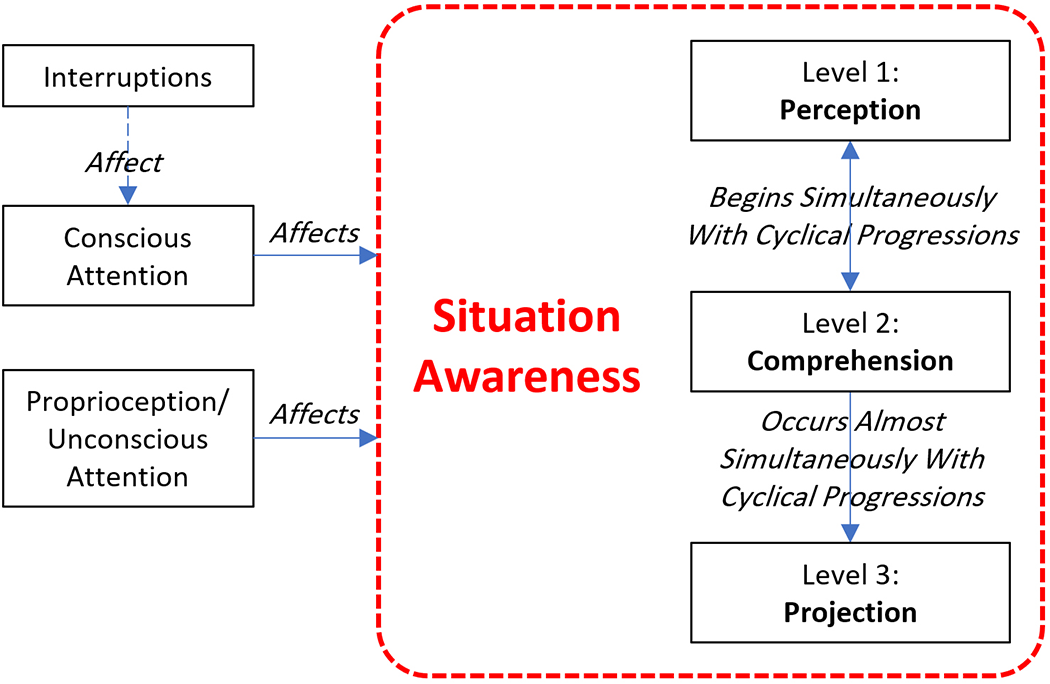
Situation awareness and attention.
SA and Clinical Action Decisions
Clinical action decision or clinical decision making is a daily process that is repeatedly undertaken by nurses to deliver the best needed action for patients based on their health situation (Krishnan, 2018). The first and important step of decision-making process is SA that provides an understanding of “what is going on” and “what is likely to occur next” (Stubbings et al., 2012). Decision making is the core purpose of SA and consists of other important elements (Figure 5). As a result, when SA is incomplete or inaccurate, the correct action for a situation is not known or any factor that limits an individual’s ability or poor performance can occur (Endsley, 1995). According to the literature, SA plays an important role in improving cognition and consequently enhancing decision making among people (Fletcher et al., 2003; Fore & Sculli, 2013; Guimond et al., 2009; Mitchell & Flin, 2008; Nibbelink & Brewer, 2018; Stubbings et al., 2012). Cognitive load is the consequence of increase in cognitive processes that remain on an individual’s working memory (Hamilton, 2017). Any loss or decrease in the level of SA among nurses can decrease performance (Hamilton, 2017) and consequently might be related to errors in decision-making and adverse patient outcomes (Brady et al., 2013; Endsley, 2006; Koch et al., 2013; Muething et al., 2012; Orique & Despins, 2017; Sitterding, 2014; Stomski et al., 2018; Stubbings et al., 2012; S. M. Wright & Fallacaro, 2011). SA is among nontechnical factors, which, based on estimations, are responsible for more than two thirds of medical errors (Dunn et al., 2007; Glavin & Maran, 2003; Stomski et al., 2018). A research study reported that one of the nine major nontechnical skills related to patient safety and error in the emergency department is SA (Flowerdew et al., 2012; Munroe et al., 2016). Situated learning is a learning process through which people can learn nontechnical skills needed to practice effectively (O’Meara et al., 2014). Clinical action decisions can contribute to situated learning through memory capture. This learning process includes both technical and nontechnical aspects that can enhance decision-making effectiveness (Stubbings et al., 2012). There are two possibilities for clinical decision making for any situation in a patient room: when clinical action is truly required and when is not required. When a clinical action is not required based on the SA of nurses, the situation is nonthreatening, and the nurse does not need to do anything specific. But when a clinical action is required, the situation may demand clinical actions only, or a combination of clinical and physical environment actions.
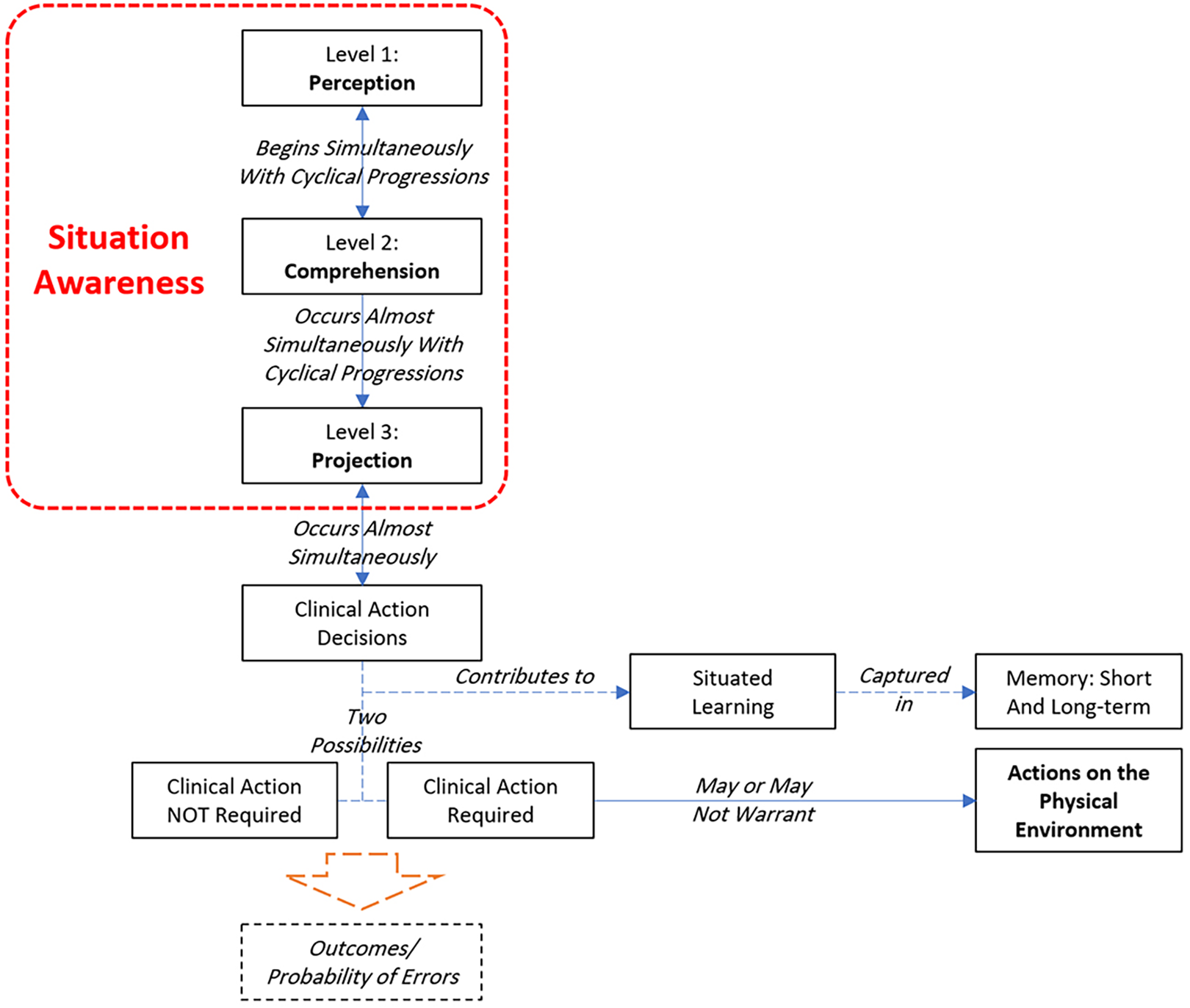
Situation awareness and clinical action decision.
To summarize, high SA is essential to prevent undesirable outcomes. Healthcare professionals must be aware of the situation to collect the vitally needed information to make a clinical decision in the shortest time (Stubbings et al., 2012). Memory is one of the factors that might influence SA (Endsley & Garland, 2000). SA includes processes that require significant demands from a human’s working memory (Endsley & Garland, 2000; Kridalukmana et al., 2020; Tower et al., 2012), and depleting working memory can impact SA (Price & LaFiandra, 2017). High levels of acute stress can negatively affect the process of decision making and attentional focus through collection of limited and poorly organized data from the environment, which can create cognitive tunnel vision and prevent the flow of information (Price & lafiandra, 2017). Complicated tasks are more susceptible to stressors, and an individual with high levels of stress may end up with less accurate decisions (Price & LaFiandra, 2017). In addition to clinical information, information from the physical environment appears to play a meaningful role in SA.
Discussion
This study articulated the elements and relationships associated with SA in an attempt to examine any plausible conceptual/theoretical association between spatial awareness and SA. The results of the analyses are illustrated in Figure 6 in a conceptual model of associations. Endsley’s (1995) SA model provided the initial foundation for exploration, which was then further developed to include other factors associated with nursing. The literature review suggests a plausible association between spatial awareness and SA; thus, it may be asserted that there exists a relation between elements of the fixed (static) and mobile (dynamic) elements of the physical environment and SA. What attributes of the patient room physical environment, then, are possibly important toward optimizing SA?
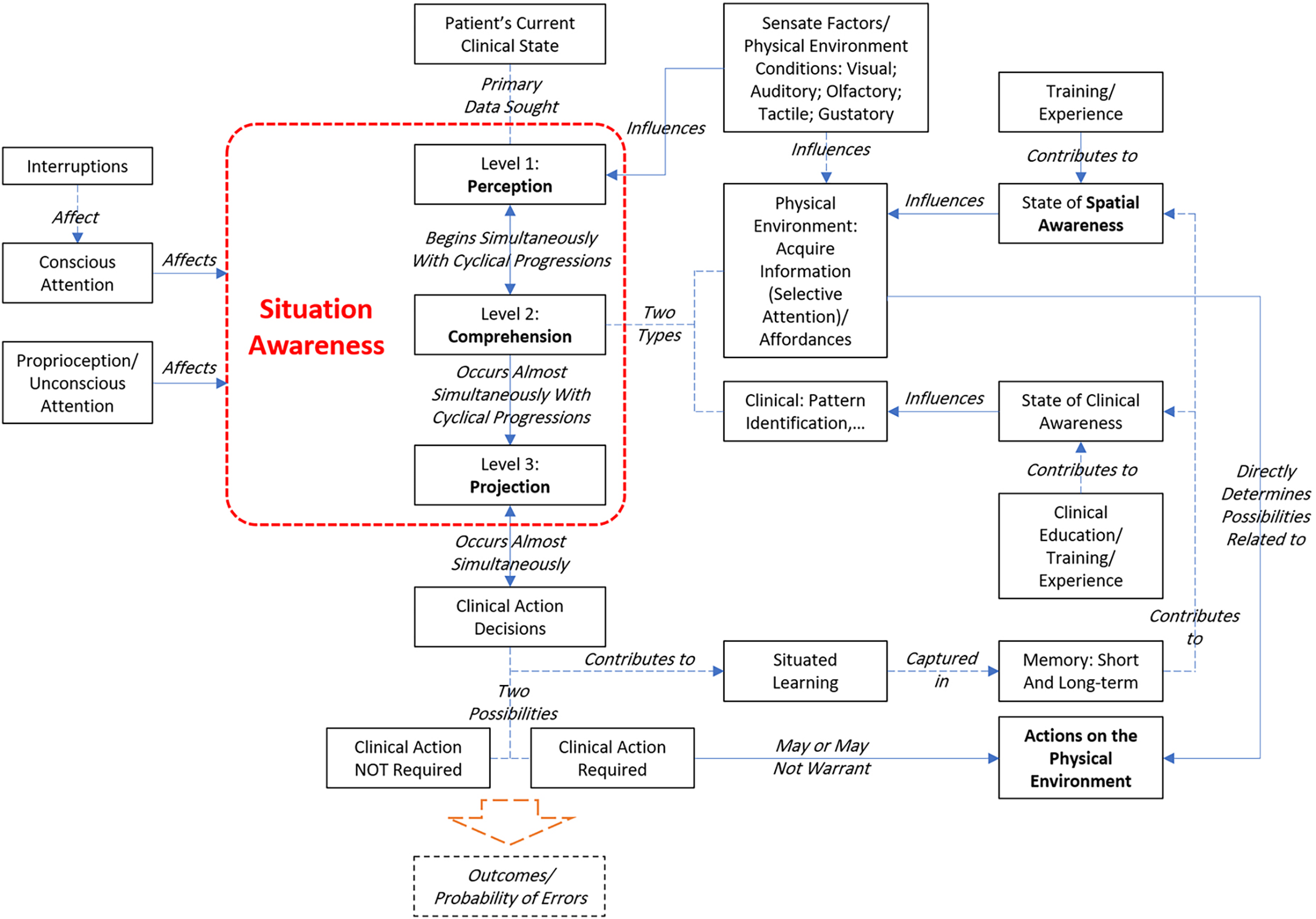
A conceptual model associating physical environment with situation awareness among nurses.
A clearer understanding of the role of the physical environment may be possible by following Endsley’s (1995, 2015) categorization in the initial model on which this thesis is founded—perception, comprehension, and projection. Note that, as stated earlier, these levels of SA are not temporally separated and occur almost simultaneously.
Perception refers to the phenomena of perceiving environmental stimulus. Humans constantly receive stimuli from the ambient environment, irrespective of whether they process the information or not (Schreuder et al., 2016). Of special relevance in this context, as suggested earlier, are the visual, auditory, and tactile stimuli, which rely on different environmental factors. Furthermore, more reliable stimuli are those that are directly perceived, in contrast to those that are constructed by the human brain to fill in the information gaps, such as in visual illusions (Shams et al., 2002).
At the very fundamental level, ensuring accurate visual stimuli depends on three factors—illuminance, luminance, and glare (Konstantzos et al., 2020). All three are directly and significantly affected by the physical design of the patient care environment. Clarity and comprehensibility of stimuli arriving within a nurse’s visual field, controlling for personal factors, are directly dependent on visual acuity, which is impacted by illuminance, luminance, and glare. From being able to assess a patient’s condition from the color of their facial skin to reading the equipment attached to a patient are all affected by these three fundamental factors.
In the domain of the auditory environment, numerous issues have been discussed in literature, including speech privacy, speech clarity, noise, and sound transmission, among others (Pope & Miller-Klein, 2016). From a SA perspective, two issues warrant particular attention. First is the audibility of equipment alarms as a part of the perception phase of SA. Second, reception of sound originating from patients as a result of pain or change in health condition is also critical to optimizing perception. For clear reception of sounds originating from alarms and patients, the background noise level and frequency spectrum of the noise are critical. An additional issue of concern is alarm fatigue (Cvach, 2012; Hamilton, 2017), which may introduce the danger of selective filtering out of important stimulus information. Generally, codes and guidelines could be depended upon for appropriate visual acuity and ambient background noise level in healthcare settings originating from building systems associated sounds or those from sources external to a building. Noise from human sources and unit operations are a separate matter, which can affect SA, but are not a factor associated with spatial awareness.
The comprehension phase may be associated with more complex issues. While lighting and color design decisions could deliver appropriate visual acuity, it does not guarantee optimal visibility (unobstructed lines of sight). Since optimal comprehension depends, among other factors, on optimal perception, not being able to see what a nurse needs to see, to be able to accurately comprehend a situation, could be highly detrimental. This raises several patient room design issues including (a) location of bed vis-à-vis door, (b) orientation of bed vis-à-vis door for facial monitoring, and (3) direct lines of sight from the entry area to all equipment attached to a patient on both sides of the bed. Evidence supporting the last issue was forthcoming in an earlier study on room-handedness (Pati et al., 2010), which underscored the importance of visibility of the entire clinician zone, and equipment within it, to nurses, irrespective of whether a room is left-handed or right-handed. The static aspects of the environment, such as walls, floors, doors, and some equipment, can be perceived and understood although they will remain fixed into the future. The dynamic aspects of the environment, such as equipment, furnishings, supplies, and other objects, can be moved, so need to be perceived, to be understood, and may have a role in projection.
In conjunction with visibility, standardization may play a crucial role in optimizing comprehension. Higher cognitive loads may hamper reception of environmental stimulus and, thus, comprehension of a situation. Standardization of the clinician zone could reduce cognitive load and hence improve comprehension. Two important factors warrant discussions at this juncture. First, standardization is a complex concept. The physical design standardization could occur at the building level at one end of the scale and micro care-setting levels at the other end. Standardization of the headwall and other elements of the clinician zone, including nurse work area and supplies/medicine cabinets, could improve caregiver familiarity with the clinician zone, thereby reducing one’s cognitive burden on quickly comprehend an emergent situation. One could refer to this as familiarity with the room layout, which includes among other fixed items such as cabinets, sinks, and wall-mounted objects. Second, it should be noted that despite standardization of the clinician zone, variations will exist, since each patient’s condition will be unique. Thus, the type and range of equipment in the clinician zone could vary from room to room and could change within one room over time. Standardization and visibility could help in easy creation of a cognitive map of the environment, thereby reducing the cognitive load originating from variations in patient care locations. For the nursing staff responsible for assisting doctors with the equipment in a room, for instance, storing the physical environment details in the memory and interacting with a cognitive map of the patient’s room are the key components of SA, allowing the nurse to access equipment easily and efficiently.
Given optimal levels of perception, comprehension, and projection, the subsequent clinical action decisions may be influenced by one’s spatial awareness. As presented previously, a clinical action decision may result in a “clinical action not required” decision or a “clinical action required” decision. The latter may warrant actions associated with the physical environment. One’s spatial awareness could substantially improve decision making in such situations. In a 2009 study (Pati et al., 2009), the authors identified 23 factors important to patient room design, including visibility and standardization visited above. Several of those factors are also relevant to the current discussions. Notable among those include (a) whether there is clear unobstructed access to both sides of a patient. Objects on the floor, furniture, and so on could hamper clear urgent access to a patient. Spatial awareness could help develop a strategy to quickly rearrange a room: (b) sufficient clearance around the patient bed—partly related to the previous factor. It may affect the number and type of additional personnel and equipment that could be accommodated safely without affecting teamwork. Spatial awareness could help develop a strategy to quickly rearrange the room: (c) access to data and supplies. Emergent conditions demand quick access to data, medical supplies, and medications. Locations of data and supplies/meds access points become critical, especially in higher acuity conditions involving multiple personnel and equipment. Spatial awareness could expedite planning for the positioning of personnel and equipment: (d) access to patient’s head. In certain situations, clear unobstructed access to a patient’s airways becomes vital and is directly affected by the spatial attributes of a room and size/location of smaller room elements. Spatial awareness could help develop an optimal strategy for safely and efficiently accessing a patient’s airways—and (e) urgently transporting a patient to another part of a hospital such as surgery or imaging. Transporting a patient in and out of a room easily and quickly is a direct function of spatial design, such as space adjacent to a bed, turning space, and width of access and doorways. Spatial awareness could help develop a strategy to quickly rearrange the room, if needed, in such situations.
Even when a clinical action decision does not involve patient transport, just plugging in the myriad of equipment in the highest acuity conditions could require quick and careful planning in an emergent situation. In a 2008 study (Thomas et al., 2008), optimizing equipment locations vis-à-vis a patient and a team of clinical personnel warranted careful planning to avoid trip hazards from cables lying on the floor. Spatial awareness of the care environment could substantially reduce the cognitive burden for safe location and plugging in of equipment posed in such situations.
Several unit-level design attributes could also affect SA and hence clinical decision making in emergent situations. A 2008 study offers some insight into unit design attributes most sought after by nursing staff (Pati et al., 2008). Among those are (a) the knowledge regarding easy visual and auditory access to other caregivers in the case of emergencies, (b) patient visibility as presented above, and (c) proximity to support services or the knowledge regarding the availability of support services when urgently needed. These represent unit-level attributes, knowledge regarding which could optimize SA, and in turn safe care delivery.
For this conceptual model, only those factors associated with SA were considered. There are other factors associated with safety and efficiency, which were excluded from the analyses. Also, there are different types of SA, including individual, team, shared, and distributed SA (Brady & Goldenhar, 2014), of which only individual SA was considered for this inquiry. Finally, the findings and assertions in this inquiry are limited to the information available from the literature search. It is conceivable that other pertinent literature is available that were not harvested in the search, and which could have influenced the model development.
Conclusions
There are many studies focusing on SA and its different aspects related to nursing, but almost none mention the physical environment and its impact on SA. The current inquiry developed a conceptual model of relationships among key factors present in high-acuity patient care environments based on published literature, which suggests that spatial awareness plays a prominent role in SA.
Implications for Practice
If spatial awareness is an element of SA, then it might be taught to improve clinicians’ SA. Recognizing that spatial awareness may impact nursing performance, architects and designers should further study patient room environments in relation to measurable performance and outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.