
Abstract
Objectives
This study proposes an evidence-based design guideline for oncology inpatient rooms that addresses the physical, emotional, and psychosocial needs of cancer patients.
Background
Cancer inpatients frequently experience long hospital stays with emotional vulnerability and clinical stress. Growing evidence suggests environmental design can shape patient experience, comfort, and recovery. Yet, current literature lacks an integrated framework for the spatial and sensory needs of this population.
Method
A systematic literature review was conducted across Web of Science, Scopus, and PubMed. From an initial pool of 1004 records, 36 studies met the inclusion criteria. Data were thematically analyzed and interpreted using established healthcare design theories.
Results
The synthesis coalesced a wide range of findings into five core thematic domains: (a) the patient's personal sphere of privacy, control, and identity; (b) the social dimension of balancing solitude with connection; (c) the sensory environment of nature, art, and acoustic well-being; (d) the integration of embedded safety and hygiene; and (e) a culture of responsive and participatory design. The analysis reveals a critical tension between clinical necessity (e.g., infection control) and psychological well-being (e.g., avoiding isolation), highlighting the need for integrated solutions.
Conclusions
The physical environment is an active agent in the cancer care experience. This review presents a comprehensive, patient-centered design framework translating empirical evidence into practical strategies. Despite study design limitations, the findings emphasize creating adaptable, psychologically supportive environments for patients’ evolving needs. The proposed guideline is a foundation for future design standards and evidence-driven practice in oncology care.
Keywords
Introduction
Cancer remains one of the most complex and demanding health challenges globally. Characterized by diverse types, prolonged treatment trajectories, and multifactorial impacts on patients’ physical and mental health, oncology care requires a multidisciplinary and resource-intensive approach (Mäurer et al., 2023). Cancer affects not only the body but also the mind and emotions. Up to 25% of cancer patients develop clinical depression, yet only a third are diagnosed and treated (National Institutes of Health State-of-the-Science Panel, 2003). Depression and anxiety among cancer patients are further aggravated by long hospital stays (averaging 29 days per inpatient) and complex treatments such as chemotherapy, radiation, and immunotherapy (Schneider et al., 2007; Skalla & McCoy, 2006). In this context, the physical environment is increasingly recognized as a key determinant of patient well-being and clinical outcomes.
Cancer inpatients, unlike outpatients, interact with hospital spaces not only for treatment but as living environments. This sustained exposure to architectural, sensory, and spatial elements significantly influences their emotional states, behaviors, and perceptions of care (Karlin & Zeiss, 2006; Kwon & Iedema, 2022; Tekin et al., 2023a, 2023b). Empirical studies have demonstrated that well-designed environments can help mitigate stress, reduce pain, improve sleep, and foster healing (Murphy & Mansfield, 2017; R. Smith & Watkins, 2016; T. J. Smith et al., 2009; Ulrich et al., 2008). Moreover, even subtle environmental changes, such as color palettes or window placement, can alter a patient's experience of space, potentially alleviating fear or psychological burden (Schweitzer et al., 2004).
Within this discourse, several theoretical frameworks have shaped our understanding of how design influences health. One of the most influential is Stress Recovery Theory (SRT), proposed by Ulrich (1983), which explains how natural environments support rapid, positive psychophysiological responses. Based on evolutionary psychology, SRT suggests that humans are biologically predisposed to respond favorably to nature, leading to stress reduction and emotional restoration (Ulrich, 1993; Ulrich et al., 1991). Complementing this, Attention Restoration Theory (ART) by Kaplan and Kaplan (1989) focuses on the cognitive dimension of recovery, positing that natural settings provide “soft fascination,” which replenishes directed attention and reduces mental fatigue. While SRT emphasizes emotional recovery, ART contributes a cognitive lens, both affirming the therapeutic potential of biophilic elements in healthcare settings. Besides, Biophilic design theory, which emphasizes the innate human affinity for nature, has increasingly influenced healthcare architecture by demonstrating that integrating natural elements into built environments can reduce stress, enhance emotional resilience, and promote faster recovery among patients (Kellert et al., 2008; Tekin et al., 2025; Tekin & Urbano Gutiérrez, 2023).
Building on SRT, Ulrich later developed the supportive design theory, which argues that healthcare environments should not only be medically efficient but also psychologically supportive. This framework identifies three core design goals: enhancing perceived control, enabling social support, and offering positive distractions (Hamilton & Watkins, 2008; Ulrich, 2000). For oncology inpatients, whose sense of autonomy and social connectivity may be diminished during treatment, such design priorities are especially relevant (Browall et al., 2013).
Similarly, Therapeutic Environment Theory extends these ideas by incorporating principles from environmental psychology, neuroscience, and psychoneuroimmunology. It proposes that healthcare spaces must minimize environmental stressors, offer positive sensory input, and provide spatial opportunities for control and connection (R. Smith & Watkins, 2016). Recommendations from this theory include access to daylight, acoustic comfort, standardized room layouts, and “off-stage” areas for staff and patient respite, elements shown to benefit both patients and caregivers.
The field of evidence-based design (EBD) operationalizes these theoretical insights into a structured decision-making process. As defined by the Center for Health Design, EBD is “the process of basing decisions about the built environment on credible research to achieve the best possible outcomes” (The Center for Health Design, 2022). Its subdomains, access to nature, social support, reduction of environmental stressors, and patient choice, are increasingly applied in the architecture of hospitals and cancer care centers (Freimane, 2015; Ulrich et al., 2008).
More recent theoretical contributions have expanded this foundation. Salutogenic design, based on Antonovsky's (1979) theory of health promotion, shifts focus from disease to well-being. It emphasizes the creation of environments that foster comprehensibility, manageability, and meaningfulness, a triad that aligns with cancer patients’ needs for clarity, support, and emotional grounding. Psychosocially supportive design proposed by Dilani (2009). Similarly, calls for built environments that engage the senses, support social interaction, provide privacy, and offer visual and symbolic cues of hope, dignity, and coherence.
Despite the growing body of interdisciplinary theory and evidence, there is a conspicuous lack of comprehensive guidelines that address the visual and spatial experience of oncology inpatients. Furthermore, much of the literature neglects the inpatient perspective, especially in cancer care contexts where emotional vulnerability is acute and the need for therapeutic support is high (Hatamipour et al., 2015; Skalla & McCoy, 2006). To address this gap, our study applies an integrative lens, rooted in restorative environmental design and the frameworks above, to explore how visual and spatial characteristics of inpatient rooms can positively influence cancer patients’ well-being. This inquiry is particularly timely given the rising incidence of cancer, the intensification of hospital care, and the growing call for patient empowerment in treatment environments (Castro et al., 2016; Lancet, 2012; Tritter, 2009). We respond to this call by systematically reviewing academic studies that investigate the design of cancer inpatient rooms and synthesizing them into a practical, evidence-informed guideline for patient-centered design.
This study seeks to answer the central question: How can the design of inpatient oncology wards be optimized to support the holistic well-being of patients by integrating evidence-based strategies? The goal is to identify the visual priorities and design strategies that reduce environmental stress, promote comfort, and align with both patient needs and theoretical best practices. While previous reviews have explored aspects of healing environments or biophilic principles in healthcare, the design of oncology inpatient rooms, spaces where patients often spend prolonged periods under conditions of high emotional, physical, and clinical vulnerability, is underexplored. This review addresses that gap by synthesizing diverse empirical findings into a comprehensive, patient-centered design framework tailored to cancer inpatient care. Beyond describing environmental influences, the study translates evidence into a set of actionable spatial, sensory, and operational design strategies, structured to support autonomy, well-being, and healing. In doing so, it bridges disciplinary boundaries between architecture, clinical care, and environmental psychology, offering practical guidance for healthcare designers, planners, and policy makers.
Method
This study employed a systematic review methodology to critically examine the existing body of academic literature addressing the architectural and interior design of inpatient rooms for cancer patients. The objective was to evaluate the current state of evidence concerning how spatial design impacts the experience, safety, and healing of oncology inpatients, and to derive recommendations for future practice and research.
To ensure a comprehensive and inclusive review, a structured search was conducted on May 31, 2025 across three major academic databases commonly used in the fields of architecture, healthcare design, and clinical research: Web of Science, Scopus, and PubMed using the Boolean phrase: (Cancer OR oncology) AND (inpatient) AND (room OR ward) AND (design). The search strategy was intentionally broad to capture all relevant peer-reviewed studies on inpatient room design for cancer patients, restricted to English-language publications and excluding gray literature to ensure academic rigor (Figure 1).
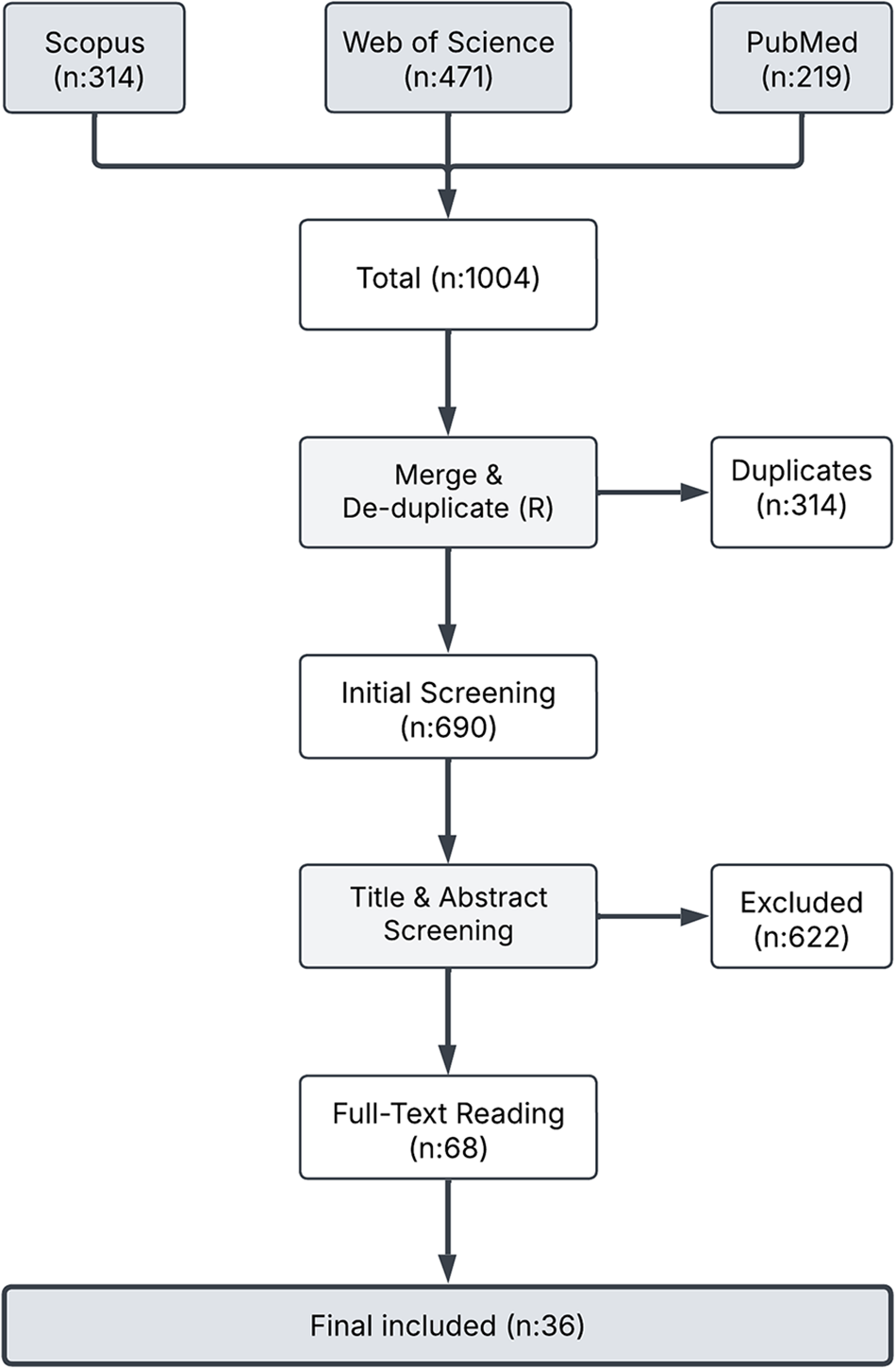
PRISMA 2020 flow diagram of study selection process.
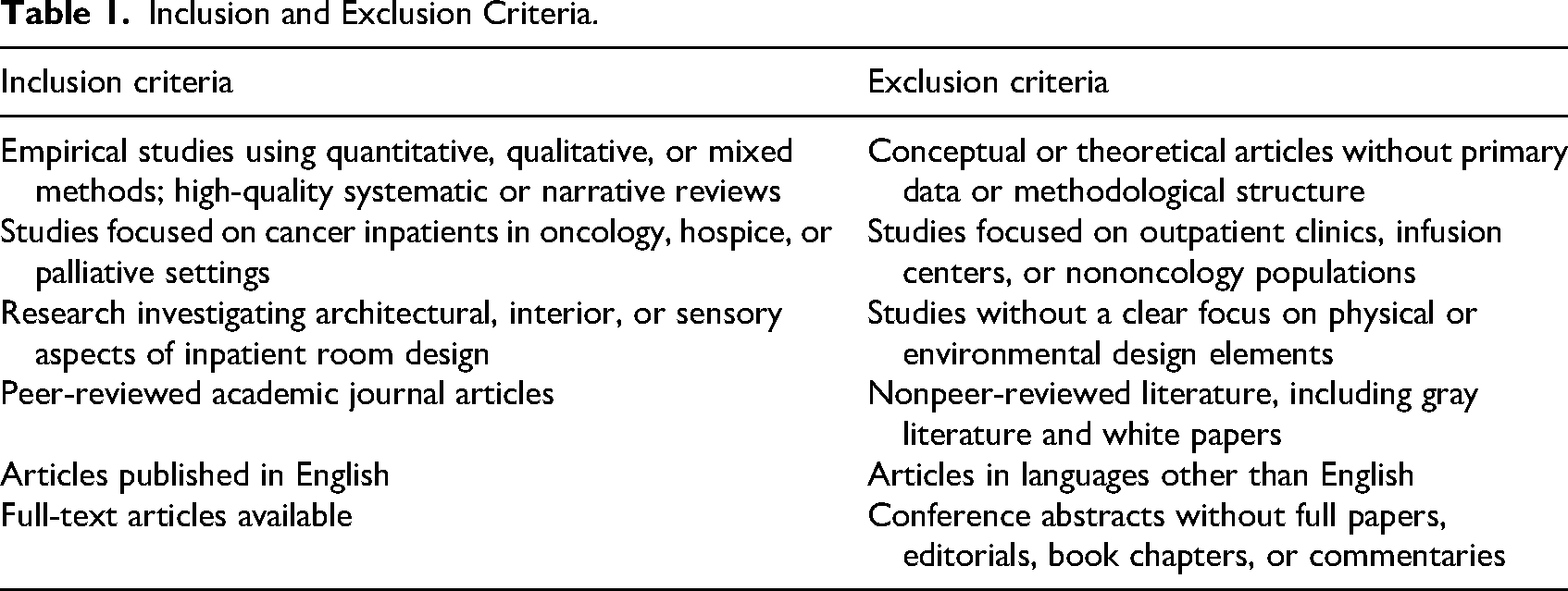
The database search yielded 1004 records (Web of Science: 471; Scopus: 314; PubMed: 219). After removing 314 duplicates, 690 unique articles were screened based on title, abstract, and keywords using Rayyan.ai (Ouzzani et al., 2016). Based on predefined criteria (Table 1), 68 studies were selected for full-text review, and 36 met all inclusion requirements for final synthesis (Table 2).
Inclusion and Exclusion Criteria.
General Overview of the Included Studies.
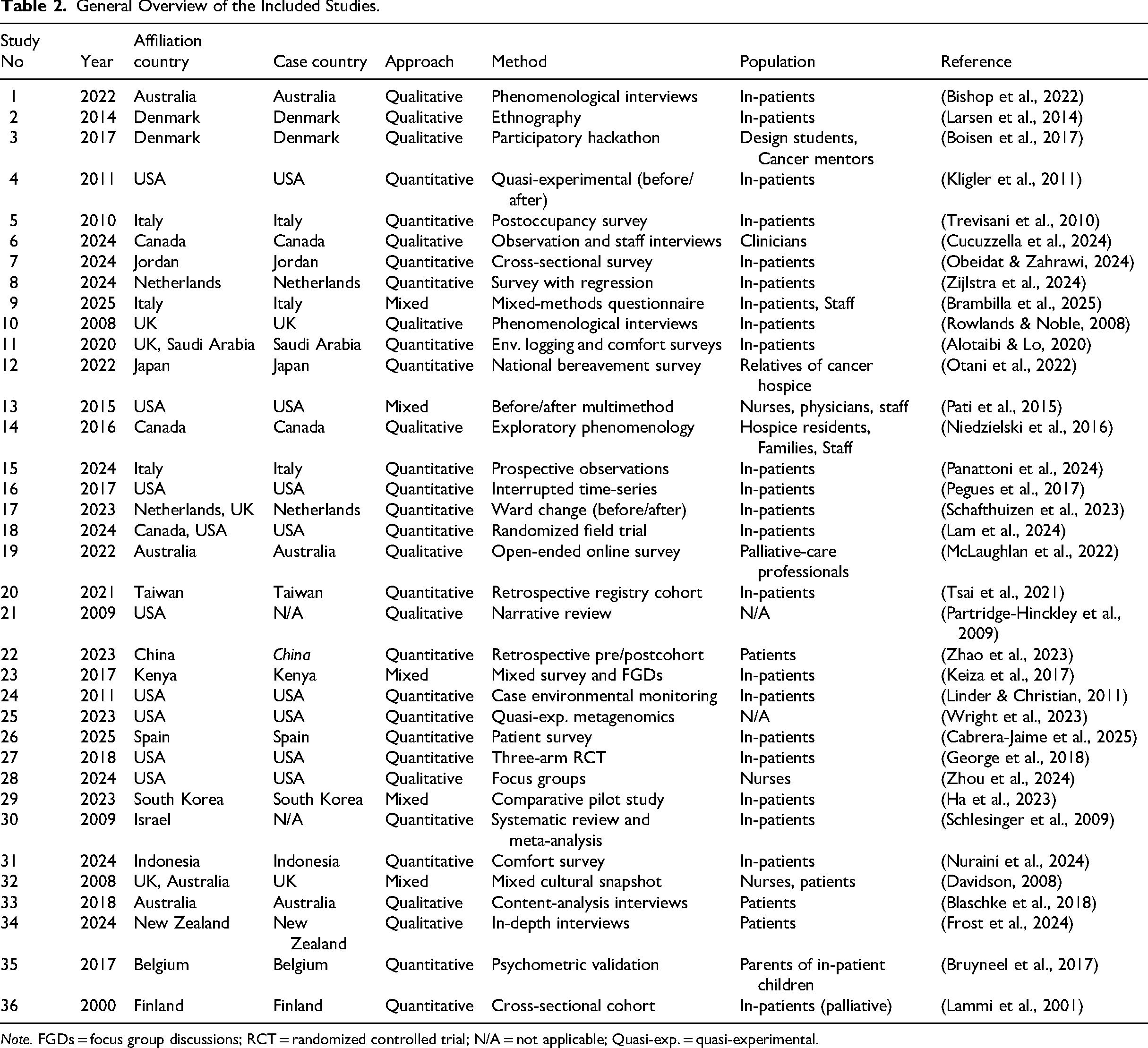
Note. FGDs = focus group discussions; RCT = randomized controlled trial; N/A = not applicable; Quasi-exp. = quasi-experimental.
The included studies represent a diverse range of methodological approaches, geographic settings, publication outlets, and participant groups. This heterogeneity enriches the evidence base but also introduces variability that limits synthesis and generalizability. The most frequent journal of publication was Health Environments Research and Design Journal (four studies), followed by Cancer Nursing and Journal of Advanced Nursing (two studies each). Most other journals appeared only once, reflecting the interdisciplinary and dispersed nature of this research across architecture, nursing, oncology, and public health domains.
As shown in Table 2, the distribution of studies reveals a strong bias toward high-income countries, with limited representation from low- and middle-income contexts. This geographic imbalance may constrain the applicability of findings to underresourced settings with different cultural, infrastructural, or policy conditions. Methodologically, the evidence base is dominated by quantitative studies, while qualitative and mixed-method approaches remain underutilized. This limits the integration of subjective, narrative-based insights with measurable environmental or behavioral outcomes, an important gap given the complexity of inpatient cancer care. While most studies involved oncology patients directly, several relied on proxy respondents such as staff or caregivers. Though valuable, these risks omit the lived experience of the primary end-users. Moreover, few studies engaged patients in participatory or codesign processes, despite the emphasis on patient-centered care.
Sample sizes varied considerably, with most studies involving small to moderate cohorts (Table 3). While eight studies had ≤25 participants, useful for exploratory insights, they lack statistical robustness. The majority (26–100 range) allows basic analysis but limits generalizability. Only five studies exceeded 300 participants, offering stronger power but often constrained by single-site, retrospective designs.
Distribution of Included Studies by Sample Size Band.

As detailed in Table 4, the dataset is marked by several recurring methodological limitations. Most studies relied on single-site recruitment and lacked control groups, limiting generalizability and causal inference. Small sample sizes, qualitative-only designs, and proxy perspectives further constrained analytical depth. Cultural specificity and pandemic-era disruptions also impacted the ecological validity of several findings.
Common Methodological Limitations Across Included Studies.
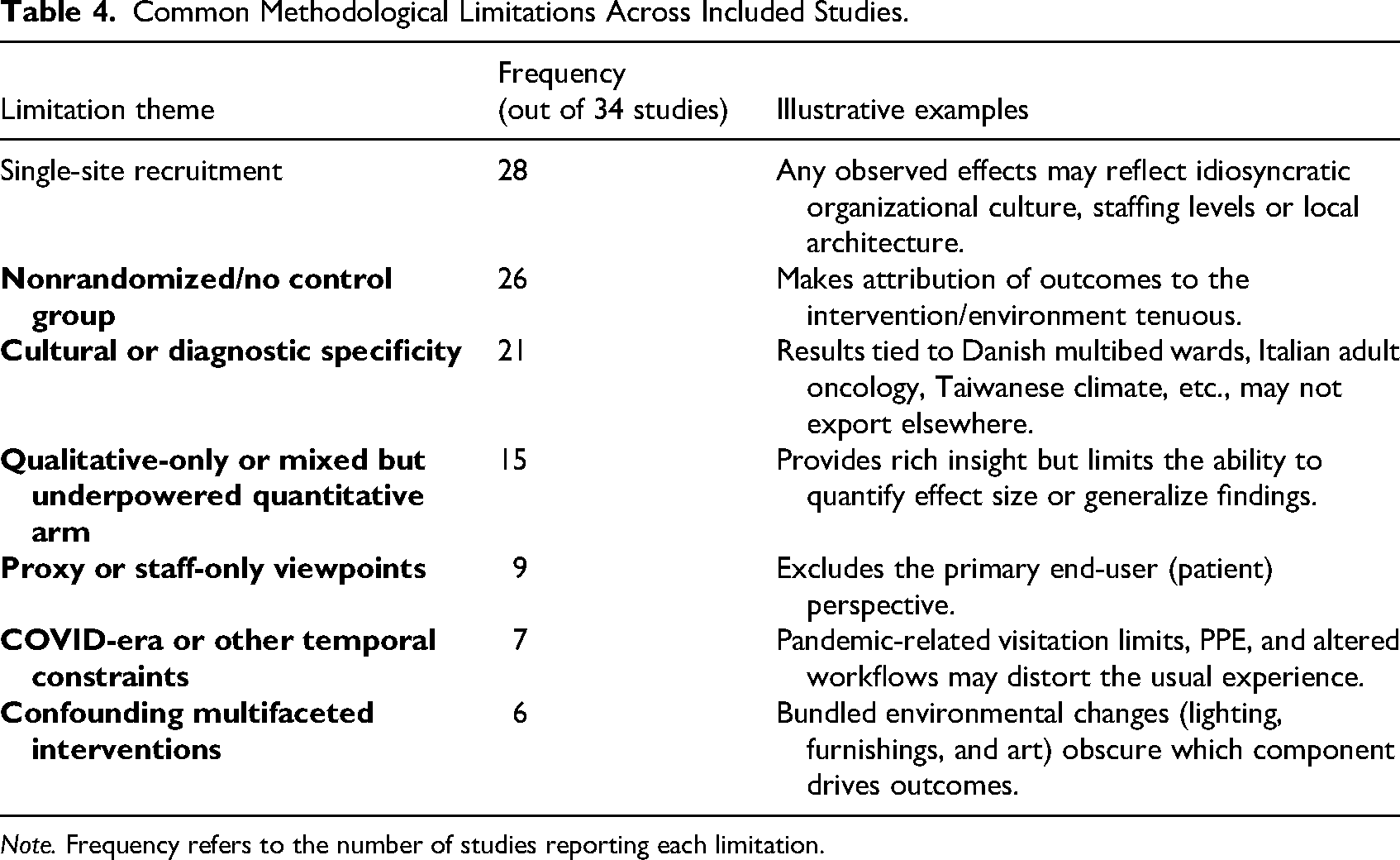
Note. Frequency refers to the number of studies reporting each limitation.
To evaluate the methodological quality of the included studies, the Mixed Methods Appraisal Tool (MMAT)—Version 2018 was applied. This tool allows for structured assessment across five methodological domains, tailored to qualitative, quantitative, and mixed-methods research designs. Of the 36 studies reviewed, 15 (41.7%) met 100% of the MMAT criteria, demonstrating high methodological rigor (Table 5). An additional 11 studies (30.6%) scored 85.7%, and only one study (Study 32) fell below 50%, scoring 42.9%; this study was retained as it did not fail any criteria entirely but showed partial or moderate alignment with all domains. Two studies (Studies 21 and 30) were not applicable to MMAT scoring as they were narrative and systematic reviews, respectively. However, both were judged to be well-structured, high-quality reviews that provided critical insights relevant to the design synthesis and were therefore included in the final analysis.
Critical Appraisal Results Using MMAT Tool.
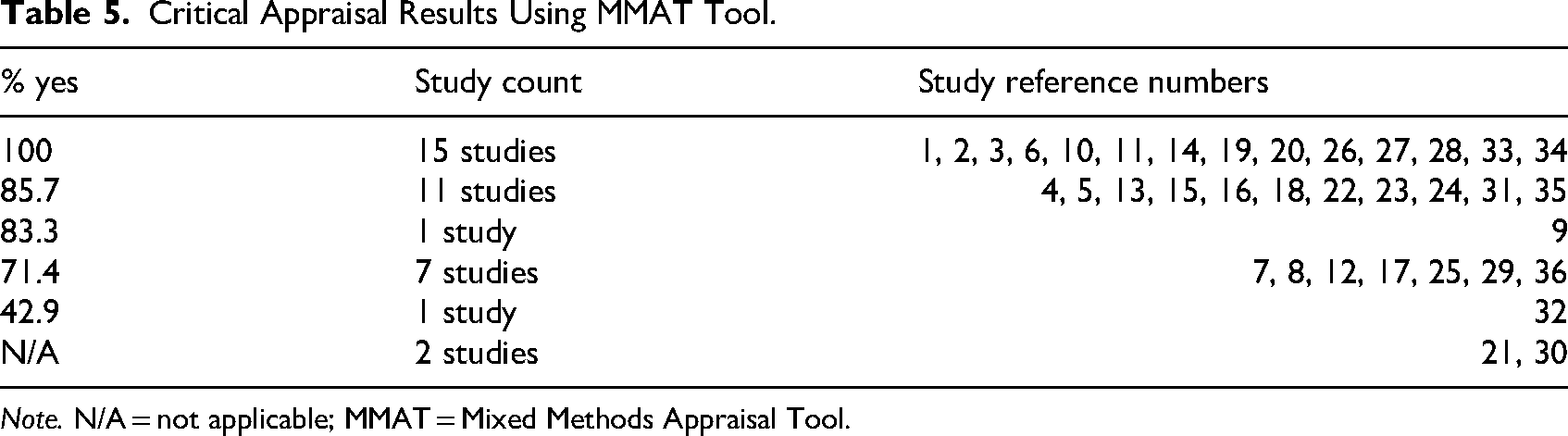
Note. N/A = not applicable; MMAT = Mixed Methods Appraisal Tool.
Each of the 36 studies was qualitatively analyzed to extract design-relevant data, which were inductively grouped into thematic domains. Due to heterogeneity across methods and outcomes, a narrative synthesis was used instead of meta-analysis, leading to a design framework to inform patient-centered oncology inpatient environments.
This review adhered to the PRISMA 2020 guidelines for transparent and standardized reporting. The completed PRISMA checklist is provided in the Supplemental Materials.
Synthesis of Evidence: Core Themes in Patient-Centered Oncology Design
An extensive body of evidence highlights the central role of the built environment in shaping the experiences of cancer inpatients. Across diverse clinical contexts, patients and staff consistently identified recurring spatial and sensory priorities. These findings coalesce into five core themes: (a) the patient's personal sphere of privacy, control, and identity; (b) the dynamic balance between solitude and social connection; (c) the impact of the sensory environment on well-being; (d) the integration of hygiene and safety; and (e) the need for a participatory design culture. Together, these themes form the basis for an evidence-based framework that reframes the hospital room from a site of passive recovery to an active agent in the healing process.
The Patient's Personal Sphere: Privacy, Control, and Identity
For patients grappling with a loss of control over their bodies and schedules, the ability to maintain dignity and exercise personal agency over their immediate physical space becomes a foundational psychological need. The evidence consistently shows that this begins with the fundamental provision of privacy and the capacity for personal control.
For patients grappling with a loss of control over their bodies and schedules, the ability to maintain dignity and exercise personal agency over their immediate physical space becomes a foundational psychological need.
Privacy and Autonomy
Private, single-occupancy rooms with ensuite bathrooms were widely valued not merely as amenities, but as essential tools for enhancing comfort, autonomy, and hygiene (Study 1). The ability to manage bodily care independently and with dignity is paramount, with more than 75% of patients and staff identifying a private bathroom with a bidet or hygiene spray as “essential” (Study 9). The positive effects of this autonomy are clear, as single-bed layouts were correlated with higher ratings of cleanliness and quiet (Study 35). In hospice settings, such rooms were described as core features in creating a dignified and emotionally responsive environment (Study 19). Underscoring its importance, privacy was rated as the single most significant contributor to healing (mean score 4.99/5), a concept that encompassed both visual and acoustic dimensions, protecting patients from unwanted exposure and intrusion (Study 7). Conversely, when these principles were violated, such as through mixed-gender rooming, it led to significant distress and shame, with one study noting, “All participants shared the view that male occupancy in the same room was inappropriate … feelings of anxiety and embarrassment” (Study 34).
Environmental Control and Personalization
Beyond the room's layout, patients emphasized the importance of regulating their immediate environment, as issues with temperature, bedding, and lighting were recurring contributors to poor rest (Study 26). The ability to control light, temperature, and air quality was linked to both physical comfort and emotional stability, giving patients a rare and vital sense of autonomy (Studies 1 and 6). This empowerment was eloquently captured in one study: “Adjusting the light with their mood gives them a feeling of flexibility and a right of choosing their own space” (Study 6). The quality of light was also influential on mood, with one patient noting, “If it's bright and not dismal, it makes you feel better…” (Study 10), while, conversely, dim rooms could lead to disorientation and distress (Study 10). This extends to a multisensory approach, incorporating patient-driven choices in smell and sound to further improve comfort. One hospice resident reflected, “Even small choices … are very important,” such as choosing what scent to diffuse or when to eat meals (Study 14). However, this control must be effective to be meaningful. Poor thermal control from heating or air-conditioning devices was a major source of discomfort (Study 26), and even with individual thermostats, patients described feeling cold due to light cotton gowns and the inability to open windows, underscoring how passive design choices and institutional protocols can inadvertently undermine user autonomy and create frustration (Study 11).
This sense of control extends to personalization, which allows the space to become a psychological refuge. The ability to bring in personal items was associated with psychological stability, with one study participant echoing that “Bringing personal items such as … decorations is promising for them,” an act which not only aided self-expression but also offered a crucial sense of continuity with life outside the hospital (Study 6). Patients and families also responded favorably to movable furniture and soft room features that mimicked residential comfort, contributing to what one study described as a “nonhospital” feeling. In this “very calming environment,” elements like piano music, aromatherapy, and linen textures allowed patients to “rearrange furniture” and adapt the room layout to their personal preferences, reinforcing dignity through small but significant acts of autonomy (Study 14). Adequate storage was also vital for maintaining a sense of order and control amidst the chaos of treatment (Study 3).
Technology and Ergonomics
While technological enhancements like motorized beds promise to increase independence, they often fail without proper user training, sometimes paradoxically leading to an increase in assistance calls. True empowerment requires intuitive design and clear instruction; as study authors emphasized, “specific training … or information brochures on the operation of the beds and the support of specific aids” are necessary for technology to be meaningfully empowering rather than a source of confusion (Study 15).
In contrast to the challenges of physical hardware, digital infrastructure was consistently seen as a successful form of ambient personalization. Adolescent and young adult patients in particular appreciated platforms for social connection, distraction, and entertainment, which were cited as vital coping tools, with one study noting that “Design concepts included robust digital infrastructure and optional platforms for connection and motivation” (Study 3). This importance was widespread, with over 90% of staff and 63% of patients rating access to Wi-Fi and television as “very important” (Study 9), reinforcing the integral role of digital access in modern patient-centered environments. When implemented correctly, physical technologies like fully electric beds with fall-prevention sensors also enhance both patient safety and caregiver workflow, contributing to better physical care experiences and minimizing manual handling risks (Study 29).
The Social Dimension: Balancing Solitude With Connection
While privacy is paramount, it exists in a delicate and often precarious balance with the fundamental human need for connection. The evidence reveals a nuanced and dynamic relationship between restorative solitude and supportive social interaction, suggesting that the ideal environment must accommodate both.
The “Cost” of Privacy and the Need for Peer Support
The benefits of private rooms can be offset by a significant psychological burden. As one patient poignantly noted, “Privacy was a right … but privacy came at a cost of isolation,” which often led patients to rely heavily on nursing staff to address their “social deficit” (Study 1). This finding suggests that simply “living in calm circumstances” can mask deeper, unmet needs for interpersonal engagement and shared understanding (Study 4, Study 12). To counteract this profound sense of loneliness, patients placed a high value on peer interaction, especially when feeling physically and emotionally stable. The shared experience of illness provides a unique and irreplaceable form of mutual support, with one patient affirming, “When you’re with other people who are in the same boat … you get on top of things” (Study 10). This sentiment was quantified in another study, where 18 out of 20 participants preferred multibed rooms when they felt well enough to interact, challenging the assumption that private rooms are universally superior and highlighting the therapeutic power of community (Study 2).
Dynamic Needs and the Importance of Choice
Room preferences are not static; they fluctuate with a patient's physical condition, emotional state, and even personality. A recurring theme was the desire to move between room types as conditions change. Patients expressed “a strong preference for a multi-bedded room when they were well enough to interact and a single cubicle when they were very ill or dying” (Study 12). This underscores the critical need for flexible spatial configurations that can adapt over time. The choice itself is a form of empowerment, and its emotional impact was also mediated by personality traits. Extraverted patients reported greater satisfaction in four-bed rooms due to opportunities for interaction, while more introverted individuals preferred the solitude of single or double rooms (Study 8). The study concluded that “Hospitals should inform patients about the benefits of the different room types and potential influences of personality … so patients are empowered,” making informed choice integral to psychological agency and emotional comfort (Study 8). Furthermore, enhancing autonomy within the room itself is crucial; rooms equipped with mobile toilets, in-room sinks, shower aids, and air mattresses enable patients to avoid frequent, and sometimes risky, hallway movement, an important consideration for immunocompromised cancer patients (Study 29).
Family as Part of the Care Ecology
Family participation is a central component of the social ecosystem, and the built environment can either facilitate or hinder their role. When design actively includes family, it reframes them from mere visitors into essential partners in the care ecology. Satisfaction was higher when rooms were sized to accommodate overnight stays with features like “family sleeper chairs and in-room storage” (Study 13). In home-like hospice settings, families participated more frequently in care, and the design of “Family Suites” and open kitchens facilitated multigenerational presence and shared rituals, reinforcing familial bonds and creating a supportive, holistic care environment (Studies 14 and 36).
The Sensory Environment: Nature, Art, and Acoustic Well-Being
The sensory quality of the inpatient environment profoundly impacts patient stress, rest, and emotional state. The research points to three key areas for intervention: biophilic design, art integration, and acoustic comfort, which together can transform a sterile space into a therapeutic one.
Nature Access and Biophilic Design
In line with theories of stress recovery and attention restoration, access to natural light, greenery, and outdoor views was consistently linked to emotional resilience and even reduced hospital stays. Patients repeatedly expressed a deep-seated desire for rooms with large windows and views of nature, a connection to the outside world that provides both orientation and calm (Studies 6 and 10). Even when satisfaction with existing views was low, they were still correlated with shorter stays, suggesting a powerful, perhaps subconscious, restorative effect (Study 7). Biophilic interventions extended beyond windows to include ceiling murals depicting skies and trees, live flowers, accessible gardens, and even high-quality artificial green walls. All of these elements were reported to create more comforting and restorative environments, helping patients “secure a basic and unburdened place to operate from” during the rigors of treatment (Studies 6, 19, and 33).
Art as an Emotional and Social Catalyst
Art installations emerged as another powerful tool for humanizing institutional spaces and providing positive distraction. In one oncology ward, 72% of patients reported that exhibited artwork “made their stay in the hospital more pleasant” (Study 5). The benefits were more than esthetic; art served a crucial social function, sparking conversation among patients and visitors and fostering connection in otherwise isolating environments (Studies 4 and 5). However, autonomy remains crucial in this domain. Imposed artwork, no matter how well-intentioned, can lead to alienation if it does not resonate with the patient, prompting recommendations for patient-led selection to reinforce a sense of dignity and personal agency (Study 27).
Acoustic Comfort and Sleep Protection
Noise was consistently identified as one of the most disruptive and pervasive environmental stressors, directly affecting sleep, emotional stability, and the perceived quality of care. The cacophony of a typical ward, with primary sources including other patients, call-bells, monitors, and staff activity, creates a relentlessly stressful soundscape (Study 22). Even in private HEPA-filtered rooms, overnight sound levels reached 49.5 dB(A), far exceeding the WHO's ≤ 35 dB recommendation and causing significant “physiologic and psychologic stress” (Study 24). Staff echoed these concerns, reporting profound acoustic fatigue from the incessant beeping of alarms and proposed specific design changes such as acoustic insulation and workflow modifications, with a particular focus on “smart alarm routing.” As one nurse stated, advocating for alarms to route directly to wearable devices, “There's no reason the patient needs to hear beeping…” (Study 28). Multipronged interventions combining architectural strategies (acoustic ceilings), operational changes (clustering care into quiet hours), and technological tools were shown to significantly reduce anxiety and depression and improve the quality of restorative sleep (Study 22).
Noise was consistently identified as one of the most disruptive and pervasive environmental stressors, directly affecting sleep, emotional stability, and the perceived quality of care.
Embedded Safety: Invisible Infection Control and Visual Clarity
For immunocompromised cancer patients, safety and hygiene are nonnegotiable. However, the evidence strongly suggests that these critical measures must be embedded seamlessly and almost invisibly into a comforting environment to avoid causing additional psychological distress.
Air Quality and Protective Environments
The control of airborne pathogens is a primary and nonnegotiable concern in oncology care. Essential design features for protective environments include single-bed rooms with 99.97% HEPA filtration, ≥ 12 air changes per hour (ACH), positive pressure systems, and airtight construction detailing, particularly for highly vulnerable allogeneic HSCT patients (Study 21). These engineering controls represent the gold standard for clinical safety. However, their implementation reveals a critical tension between physical protection and psychological well-being. The very features that ensure sterile air, sealed windows, constant airflow, and physical separation can create a profound sense of confinement. The resulting isolation can erect a psychological barrier between patients and their medical team, with one study noting that “Isolation carries a psychological burden to patients” (Study 30). This burden is not trivial; it can manifest as heightened anxiety, depression, and a feeling of being disconnected from the world and from human touch. Furthermore, the clinical benefits are not always clear-cut enough to justify this psychological cost. One study found that while half of multiple myeloma patients received transplants in HEPA rooms, it did not affect 100-day mortality, and these high-cost rooms were associated with longer hospital stays (Study 20). This highlights the complex challenge of achieving rigorous air quality control without imposing undue emotional and financial costs, forcing designers and clinicians to question whether the psychological harm of such profound isolation might, in some cases, counteract the intended physical benefits.
Surface Hygiene and Material Innovation
Beyond air quality, patients strongly associated environmental cleanliness with feelings of safety and trust in their care (Study 31). The challenge, therefore, is to achieve rigorous hygiene without creating a visually sterile or alienating atmosphere. Innovative solutions can provide this “invisible” hygiene. Electrochromic glazing, for example, reduces bacterial abundance on surfaces while eliminating the need for dust-harboring blinds (Study 18). Similarly, copper–silver ion mats reduce pathogens on high-touch surfaces without disrupting workflow (Study 25), and integrated Ultraviolet Germicidal Irradiation (UVGI) systems for terminal cleaning can reduce infections without increasing room turnover times (Study 16). Also, wider bed spacing, 1.5 m compared to 1.0 m in standard settings, allows room for patient equipment and visitor seating while reducing infection transmission risk (Study 29).
The challenge, therefore, is to achieve rigorous hygiene without creating a visually sterile or alienating atmosphere.
Visual Simplicity and Clarity
Safety also relates to reducing cognitive load. In a state of heightened anxiety, a confusing or cluttered environment can be another source of stress. Patients reacted negatively to visible clinical clutter, as “Medical devices with a complex appearance … can cause them distress,” with some preferring such equipment to be hidden in panels, stored out of sight, or kept in adjacent corridors (Study 6). Environmental clarity extended to signage and wayfinding. Color-coded lines, large-font instructions, and visual icons all helped reduce navigational anxiety and cognitive load: “The use of distinct colors for each room remarkably aids patients in easily finding their room” (Study 6). Ambiguous layouts or mixed-gender rooming also caused significant distress and embarrassment, compromising patients’ sense of security (Study 34).
A Culture of Responsive and Participatory Design
A final, overarching theme from the evidence is that static environments cannot meet the dynamic and deeply personal needs of cancer care. A responsive design culture, rooted in authentic user participation, is essential for creating and maintaining truly therapeutic spaces.
Stakeholder Alignment and Codesign
Studies repeatedly revealed a frequent and significant mismatch between the environmental priorities of staff and patients. For instance, staff might strongly prefer single rooms for ease of surveillance, while only 31% of patients rated them as “very important,” prioritizing other factors instead (Study 9). Such disagreements highlight the critical need for codesign workshops and prototype testing to bridge this empathy gap and align the final design with the lived experience of its primary users. Processes that actively involve patients, such as serving on design juries or engaging in participatory photography, lead to greater satisfaction and foster a powerful sense of ownership and morale among both patients and staff (Studies 3 and 32).
Enabling Ritual and Fostering Emotional Expression
The built environment can be a powerful facilitator of rituals that promote continuity with everyday life, such as tea gatherings and community meals in shared lounges or kitchens, which help maintain a sense of normalcy (Study 14). Furthermore, an emotionally safe environment can unlock crucial emotional expression. In hospices, nurses reported more anxiety and depression in patients not because their condition had worsened, but because the private, dignified design made it safe for them to express their feelings (Study 36). This powerful finding demonstrates that a well-designed environment is not just a passive container for care, but an active agent in the therapeutic process, one that must remain aligned with changing human needs through continuous feedback and adaptation.
Design Guidelines for Cancer Inpatient Environments
The following design guideline presents a rigorous, evidence-informed framework for cancer inpatient environments. Grounded in established healthcare design theories such as Supportive Design, EBD, and Salutogenic principles, it translates the findings from the preceding synthesis into a set of actionable strategies. Organized into five interdependent domains, the framework combines spatial interventions with psychosocial and clinical considerations, aiming to foster environments that support healing, autonomy, emotional well-being, and staff resilience.
The first domain, The Patient's Personal Sphere, is grounded in the principle of restoring dignity and agency. This aligns directly with Ulrich's supportive design theory, which posits that enhancing a patient's sense of control is critical to reducing stress. Private rooms with ensuite bathrooms, therefore, are not just amenities but the structural foundation of therapeutic design, preserving bodily autonomy and providing a tangible sense of control in a context where many choices have been stripped away.
The second domain, The Social Dimension, treats relatives, peers, and cultural identity as integral therapeutic resources. The guiding principle is to recognize that human connection is a structural need, not an ancillary service. This requires a dynamic model that moves beyond the rigid binary of single versus shared rooms, offering adaptable configurations that respect the patient's fluctuating need for both restorative solitude and the unique emotional support that comes from peer and family interaction.
Next, The Sensory Environment focuses on reducing physiological stress and cognitive load. This principle is consistently supported by biophilic design theory, SRT, and ART, which demonstrate the cognitive and physiological benefits of nature engagement. The goal is to create a restorative atmosphere through the careful calibration of sound, light, air, and nature cues, using them as intentional therapeutic tools to promote calm, protect restorative sleep, and mitigate the sensory overload common in clinical settings.
The fourth domain, Embedded Safety, addresses the challenge of delivering rigorous infection prevention without compromising the normalizing character of the environment. The guiding principle is to embed infection control as an invisible logic. While hygiene infrastructure is crucial, it must not override psychological comfort. By leveraging material innovations and thoughtful design, safety measures can be seamlessly integrated, enhancing physical safety without creating a visually sterile or anxiety-inducing atmosphere.
Finally, a culture of responsive and participatory design sustains the therapeutic quality of the environment over time. This principle emphasizes that design is not a static product but an iterative process. It calls for actively protecting the well-being of caregivers and implementing a continuous feedback loop, through codesign and postoccupancy evaluations, where the lived experiences of patients, families, and staff are used to inform ongoing adaptations and improvements.
Collectively, these domains offer a holistic model of therapeutic space-making, one that recognizes the built environment as an active agent in healing and resilience. The following table (Table 6) operationalizes these principles, providing a detailed list of integrated design specifications for each domain.
An Integrated Design Framework for Patient-Centered Oncology Environments.
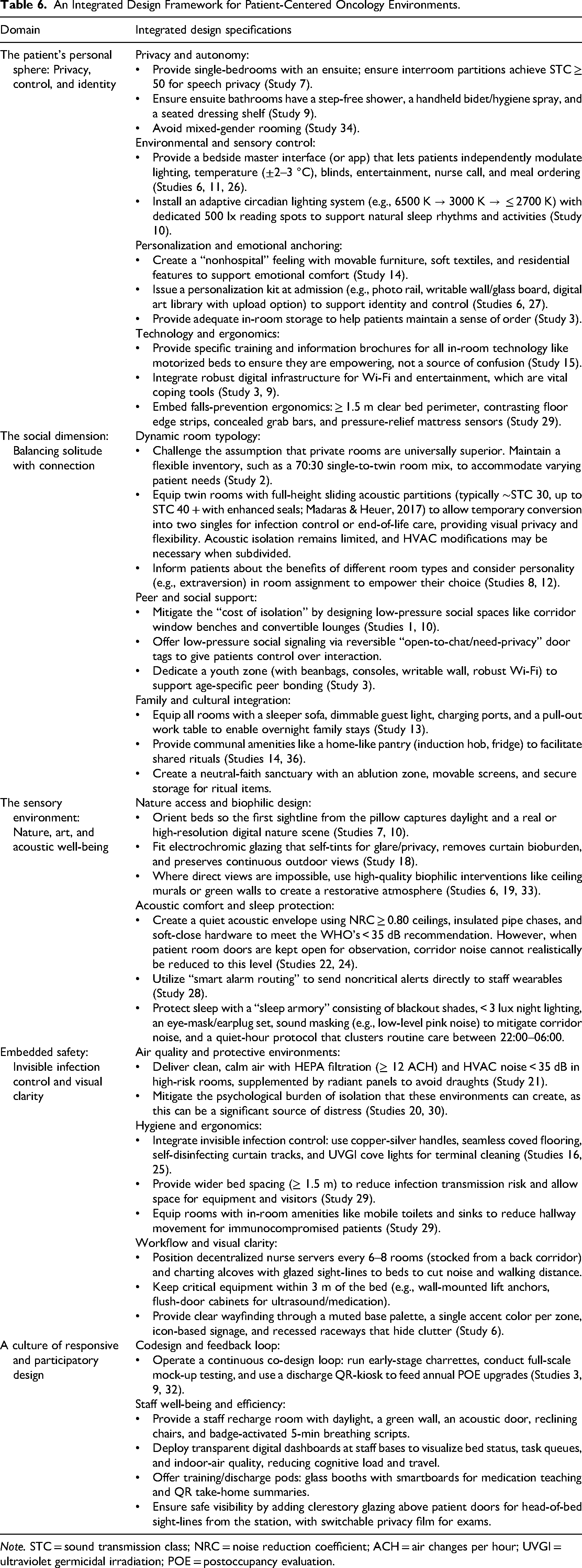
Note. STC = sound transmission class; NRC = noise reduction coefficient; ACH = air changes per hour; UVGI = ultraviolet germicidal irradiation; POE = postoccupancy evaluation.
Conclusion
This study provides a comprehensive synthesis of evidence on the design of inpatient rooms and wards for cancer patients, highlighting how physical environments influence patient experience, emotional well-being, and clinical outcomes. By drawing on a diverse body of research, this review consolidates a wide range of findings into five core thematic domains: the patient's personal sphere of control, the social dimension of care, the sensory environment, embedded safety, and a culture of participatory design. The resulting framework is rooted in established healthcare design theories, including supportive design and biophilic design, and is translated into a set of actionable architectural strategies.
The findings underscore that oncology environments are not merely clinical containers but active therapeutic agents. The evidence reveals that patient needs are nuanced and dynamic; room types must flex with disease trajectory, personality, and emotional state, while features that enhance control, facilitate social connection, and provide sensory comfort are critical to the holistic experience of care. A recurring theme is the tension between clinical necessity and psychological well-being, whether in the context of privacy versus isolation or infection control versus sensory comfort, highlighting the need for integrated and empathetic design solutions. Similarly, integrating the voices of patients, families, and staff into the planning process is essential to aligning healthcare spaces with real-world functional and emotional demands.
The findings underscore that oncology environments are not merely clinical containers but active therapeutic agents.
Despite its breadth, this study is not without limitations. Many of the included studies were single-site investigations, limiting generalizability across diverse healthcare settings. The predominance of nonrandomized or observational research designs restricts causal inferences regarding the effects of design interventions. Additionally, a reliance on qualitative data and proxy perspectives in several studies may have introduced subjectivity or bias. Cultural and regional representation was also skewed, with most studies conducted in high-income countries, raising questions about applicability in other contexts. Finally, the absence of standardized outcome measures and the heterogeneity of methodologies limited the feasibility of a formal meta-analysis.
Nevertheless, this review offers a robust evidence base for guiding the future design of cancer inpatient environments. It encourages architects, healthcare providers, and policy-makers to adopt a multidimensional, patient-centered approach that aligns architectural form with emotional function and operational logic. Future research should focus on longitudinal and multicenter studies, particularly in underrepresented geographic regions, and develop standardized tools to assess the impact of the built environment on patient outcomes across the five domains identified in this paper. As the demand for oncology care rises globally, responsive, EBD will be key to delivering not only clinical excellence but also dignified and humane care.
Implications for Practice
Prioritize Patient Control to Restore Agency: Provide patients with direct control over their environment and opportunities for personalization. Restoring a sense of control is a powerful tool for reducing stress. Staff should be trained to introduce these features as an integral part of the care plan.
Design for Dynamic Social Needs: Recognize that patient needs for privacy and social connection fluctuate with their health and personality. Incorporate flexible room typologies, such as twin rooms with full-height acoustic partitions that can be converted into private spaces, and develop protocols to assess patient preferences upon admission.
Treat the Sensory Environment as a Clinical Priority: Actively manage the sensory environment to reduce stress, with a focus on noise as a clinical harm. This requires a combined approach of architectural solutions, technological tools, and operational protocols to protect restorative sleep.
Mandate a Participatory Codesign Process: To address the frequent mismatch in priorities between stakeholders, hospital leadership should mandate the inclusion of patients, families, and frontline clinical staff in all phases of design and renovation. Utilize tools like full-scale mock-up testing and postoccupancy feedback to ensure the final design is grounded in the lived experience of its users.
Footnotes
Acknowledgments
The author would like to thank the researchers and clinicians whose work contributed to the body of literature reviewed in this study. Gratitude is also extended to the patients, families, and healthcare staff whose lived experiences have informed the design insights presented here. Special thanks are extended to my beloved wife, Tugba Tekin, for her unwavering support, encouragement, and patience throughout the research and writing process. Language editing and proofreading support was provided with the assistance of ChatGPT-4o (OpenAI), under the author's direction.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.