
Abstract
Objectives
This systematic review aims to explore virtual reality (VR) applications for rehabilitation purposes among people with intellectual and developmental disabilities (IDD), identify their effects on rehabilitation outcomes, explore themes to consider in VR intervention design, and provide guidance for designers and researchers in creating therapeutic environments using VR technology.
Background
VR has gained increasing attention in healthcare settings to assist in achieving rehabilitation goals for people with IDD. VR is particularly advantageous since it simulates the real world while providing controllable, safe, and versatile environments. It is necessary to expand the current body of knowledge on VR intervention's outcomes by synthesizing further information on VR application characteristics as well as identifying design considerations regarding feasibility, usability, safety, and other aspects that will benefit future VR intervention design and research.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framed the current review. Multiple databases were searched to identify studies published between 2001 and 2023. The review qualitatively organized VR environment design considerations according to three themes: feasibility, usability, and safety.
Results
This review included 27 articles and included 868 participants. The overall findings indicated that VR interventions are promising in enhancing rehabilitation outcomes among people with IDD, such as physical, cognitive, emotional, and functional independence domains.
Conclusion
This review provides design recommendations to create effective, usable, and safe VR interventions for individuals with IDD. The suggested design implications should be applied with the awareness that VR is a relatively emerging technology with rapidly evolving features.
Keywords
Introduction
IDD is a broad term that describes conditions affecting cognitive functioning, adaptive behaviors, and development (NIH, 2021). It is common for individuals with IDD to have multiple co-occurring conditions such as autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), cerebral palsy, Down syndrome, intellectual disability, specific learning disabilities, and others (Wills, 2014). A range of health conditions that people with IDD exhibit are related to various risk factors affecting their overall well-being and quality of life. For instance, individuals with IDD tend to experience worse health outcomes compared to people without disabilities (Magaña et al., 2016), and they are vulnerable to mental health conditions such as anxiety and depression (Hsieh et al., 2020). Additionally, sensory processing disorders (SPDs) are common among individuals with IDD. SPDs cause individuals to react to environmental sensory stimuli with either hyper- or hyposensitivity, preventing them from fully participating in society (Case-Smith et al., 2015). Furthermore, research has also shown lower levels of self-esteem and overall quality of life in this population (Nota et al., 2007).
This empirical evidence demonstrates the potential benefits of rehabilitation for people with IDD. It is important to note that rehabilitation is a process that helps people enhance essential abilities, foster independence, and improve overall quality of life (Ryan Oakes, 2022). In consideration of the unique needs associated with IDD, rehabilitation interventions for this population have aimed at improving their independent living skills (e.g., activities of daily living, sensory integration, adaptive strategies, and self-care skills), physical abilities (e.g., gross motor skills, mobility, coordination, strength, and balance), behavioral challenges (e.g., positive behavior reinforcement, and adaptive skills), communication skills (e.g., speech and expressive and receptive language), and vocational skills (e.g., job skills and employment opportunities).
Environmental psychology has shown that the rehabilitation and behavioral outcomes of people with IDD can be better supported by providing an adequate environment (Ellis & Yi, 2023; Yi, 2017, 2021; Yi et al., 2018; Yi & Ellis, 2023). In addition to physical environments, VR has received growing attention as a promising technology to foster rehabilitation goals (Ryan Oakes, 2022). VR is particularly advantageous for supporting rehabilitation purposes since it simulates the real world while being controllable and flexible (Yi & Heidari Matin, 2024). Specifically, VR enables healthcare professionals to repeat certain conditions as necessary to meet therapeutic goals. In addition, VR can provide personalized clinician plans controlling different variables suited to the patient's needs. VR has the potential to create scenarios beyond real-life limitations (Yi & Bhattacharjee, 2023). Also, it is capable to be used as a starting point where patients can safely practice certain scenarios before engaging in the real world (Bryant et al., 2020; Foloppe et al., 2018; McCleery et al., 2020; Standen & Brown, 2005). Additionally, VR has become significantly more affordable and accessible fostered by technological advancements. For these reasons, VR has been increasingly used in healthcare settings such as rehabilitation, pain management, surgery simulation, and patient education and training (Chen et al., 2022; Ryan Oakes, 2022).
Virtual Reality: Immersive Levels and Modes
This study defines VR as a computer-generated, three-dimensional environment that provides users with immersive and interactive experiences. Compared to similar technologies such as augmented reality (AR) or mixed reality (MR) in which virtual information and reality co-exist, VR has the merit that users can be entirely immersed in a simulated environment.
VR environments can provide different degrees of immersion and interaction modes. The degree of immersion ranges from immersive, semi-immersive, to non-immersive (Bamodu & Ye, 2013; Salatino et al., 2023). Non-immersive VR uses computer or console game systems and interface devices (e.g., mouse, keyboards, and joysticks). In this immersion level, users are still aware of the surrounding real world. Semi-immersive VR is administered using a large screen with advanced interface devices (e.g., gloves, haptic feedback devices, and infrared cameras). Users typically experience partial immersion and a sense of presence. Immersive VR consists of head-mounted displays (HMD) and 3D input devices (e.g., VR controllers and haptic gloves). The user can be fully immersed and interact with the virtual environment. This study focuses on immersive and semi-immersive VR to provide design information toward relatively up-to-date immersive and semi-immersive technologies.
VR also supports various modes of human–environment interactions such as stationary mode where users remain immobile, and movement mode which allows users to navigate and move around within a designated area. Figure 1 further illustrates the characteristics of the three different degrees of immersion and the two interaction modes.
Immersion levels of virtual reality
Related Literature
A growing body of research has explored VR technologies used for people with IDD. Previous systematic reviews have investigated VR applications for IDD (Ryan Oakes, 2022) or specific diagnoses, including ASD (Chen et al., 2022; Mesa-Gresa et al., 2018), intellectual disabilities (Standen & Brown, 2005), and ADHD (Bashiri et al., 2017). However, a gap in these previous reviews is that the extracted data primarily focused on intervention outcomes and efficacy. There has been little information about VR intervention design considerations that could benefit future interventions and research design. There have also been previous efforts to establish VR accessibility guidelines for people with disabilities (Heilemann et al., 2021). However, a gap still exists in identifying specific VR intervention design implications for people with IDD in therapeutic settings. For instance, considering various methods (such as immersive, semi-immersive, and non-immersive) and modes (stationary or movement-based) can optimally support rehabilitation purposes for this population. Appropriate use of VR can reduce the need for physical equipment and allow for repeated practice without additional cost. This not only makes the rehabilitation process more scalable but can also enhance accessibility for patients who might not be able to afford or access traditional treatment. To enhance our understanding of VR interventions, expanding the current body of knowledge about VR application features (such as immersion levels, guardian mode, session frequency, and duration) is necessary. Additionally, identifying design considerations related to feasibility, usability, safety, and other aspects will contribute to better VR intervention design and research.
Purpose
The purpose of this review is to synthesize design considerations that can guide designers and researchers in developing VR environments for people with intellectual and developmental disabilities (IDD). The presented systematic review aims the following: (a) exploring the applications of VR for rehabilitation purposes among people with IDD; (b) identifying its effects on rehabilitation outcomes, (c) exploring emerging themes to be considered in VR intervention design; and (d) providing recommendations for designers and researchers in creating therapeutic environments using VR technology.
Methods
Procedure
PRISMA framed the current review (Moher et al., 2010). The Effective Public Health Practice Project (EPHPP) protocol also guided the presented systematic review process. The EPHPP considered seven stages: question formulation, searching and retrieving the literature, establishing relevance criteria, study quality assessment, data extraction and synthesis, report writing, and dissemination (Thomas et al., 2004).
Search Strategy
In this study, the researchers conducted keyword searches on November 13, 2023. Keywords were selected considering the study's population, intervention, and setting: (disability*) AND (virtual reality) AND (therap*) OR (rehabilitation). Different combinations of the key terms were searched using multiple databases using EBSCO: MEDLINE, Academic Search Complete, CINAHL, Health Source (Nursing/Academic Edition), Psychology and Behavioral Sciences Collection, PsycINFO, and ERIC. The search was restricted to full-text, peer-reviewed studies published between 2001 and 2023.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (a) Population. People with intellectual and/or developmental disabilities; (b) Intervention. VR; (c) Outcomes. Possible therapeutic outcomes after using VR interventions such as improvement in mental health, behavioral changes, and independent living skills; (d) Context. Therapeutic setting; (e) Language. English; and (f) Publication dates. 2001–2023.
The exclusion criteria were as follows: (a) individuals with disabilities other than IDD (e.g., unilateral spatial neglect and physical disabilities); (b) interventions using AR, MR, or non-immersive VR; (c) settings other than healthcare (e.g., education); (d) studies written in languages other than English (e.g., Spanish); and (e) studies published before 2001.
Selection Procedure and Data Extraction
After removing duplicates, the predetermined inclusion criteria were used to screen the searched studies’ titles and abstracts. Once the initial abstract and title screening was completed, two independent researchers screened the studies’ full texts against the same eligibility criteria. Additionally, researchers reviewed the reference sections of the selected articles and included relevant articles after the title, abstract, and full text screening process.
From the selected studies, researchers extracted data using a matrix that included information on study design, evidence level, participants (i.e., description, number, and age), comparison, intervention (i.e., name; type—stationary, movement; immersion degree—non-immersive, semi-immersive, immersive; and other descriptions—session number, time, interval, etc.), and outcome. Synthesized results were gained from the related design strategies for the outcome behaviors. Following the directed content analysis process (Assarroudi et al., 2018), design considerations were coded and categorized according to the three domains: feasibility, usability, and safety. The researchers added emerging themes under each category while reviewing the full text and analyzing word clouds and word frequency using NVivo (Elliott-Mainwaring, 2021). Meta-analysis was not conducted in this research because most quantitative data involved small participant numbers. Instead, the results were narratively summarized.
Quality Appraisal
For each study, three investigators independently evaluated the study quality using the JBI critical appraisal tools (Tufanaru et al., 2020). JBI tools provide separate appraisal checklists according to study types. The following tools were used to assess the studies included in this systematic review: JBI tools for randomized controlled trials (RCTs), quasi-experimental studies, case reports, qualitative studies, and systematic reviews (Aromataris et al., 2015; Barker et al., 2023; Gagnier et al., 2013; Lockwood et al., 2015; Tufanaru et al., 2020). After completing the checklist for each study, the overall quality was determined using a domain-based approach such as RoB2 or ROBIN-I (Barker et al., 2023). Specifically, this study considered a low risk of bias if 0–3 criteria are no or unclear, moderate risk if 4–6 criteria are no or unclear, and high risk if 7 or more criteria are no or unclear. Additionally, the evidence levels of the studies were also evaluated following the Oxford Centre for Evidence-Based Medicine criteria (American Occupational Therapy Association, 2020; Center for Evidence-Based Medicine, 2009). Table 1 describes the details. Any disagreements between the two primary reviewers were addressed by discussion.
Levels of Evidence.
Note. The levels and strengths of evidence are adopted from Center for Evidence-Based Medicine (2009), and the American Occupational Therapy Association (2020).
RCT: randomized controlled trial.
Results
As reported by the PRISMA flow diagram (Figure 2), the initial search identified 945 records from seven databases. After removing duplicates, 939 studies were screened for their titles and abstracts against the predetermined inclusion and exclusion criteria. The remaining 21 studies’ full texts were screened and 10 articles were included. In addition, 17 articles were identified through a citation search. Finally, 27 studies were included in this systematic review.
Study selection process.
The selected studies consist of nine RCTs, seven quasi-experimental studies, one case report, three qualitative studies, seven systematic reviews, and one mixed-methods research that used quasi-experimental and qualitative studies. A total of 868 individuals with IDD were involved in the empirical studies included in this systematic review. Table 2 describes the characteristics of the included studies by study design, participants, VR interventions, and their outcomes.
Characteristics of the Selected Studies.
Note. IDD: intellectual and developmental disabilities; ASD: autism spectrum disorder; ADHD: attention-deficit/hyperactivity disorder.
Evidence levels of the selected study are based on the Center for Evidence-Based Medicine (2009) and the American Occupational Therapy Association (2020).
Modes: stationary (immobile), movement (supports participants’ mobility), and unclear (report does not explicitly specify).
Immersion degrees: immersive—fully immersed using head-mounted displays (HMD) and 3D input devices (e.g., VR controllers, haptic gloves, etc.); semi-immersive—partially immersed using a large screen with advanced interface devices (e.g., gloves, haptic feedback devices, and infrared cameras).
As a result of the quality appraisal, each of the included studies was rated as acceptable with minor methodological limitations (Tables 3–6). Regarding the evidence level of the selected studies, the review consists of nine RCTs of Level 1B, seven quasi-experimental studies of 3B, and eleven empirical and review studies of Level 4.
Quality Assessment: Randomized Controlled Trials.
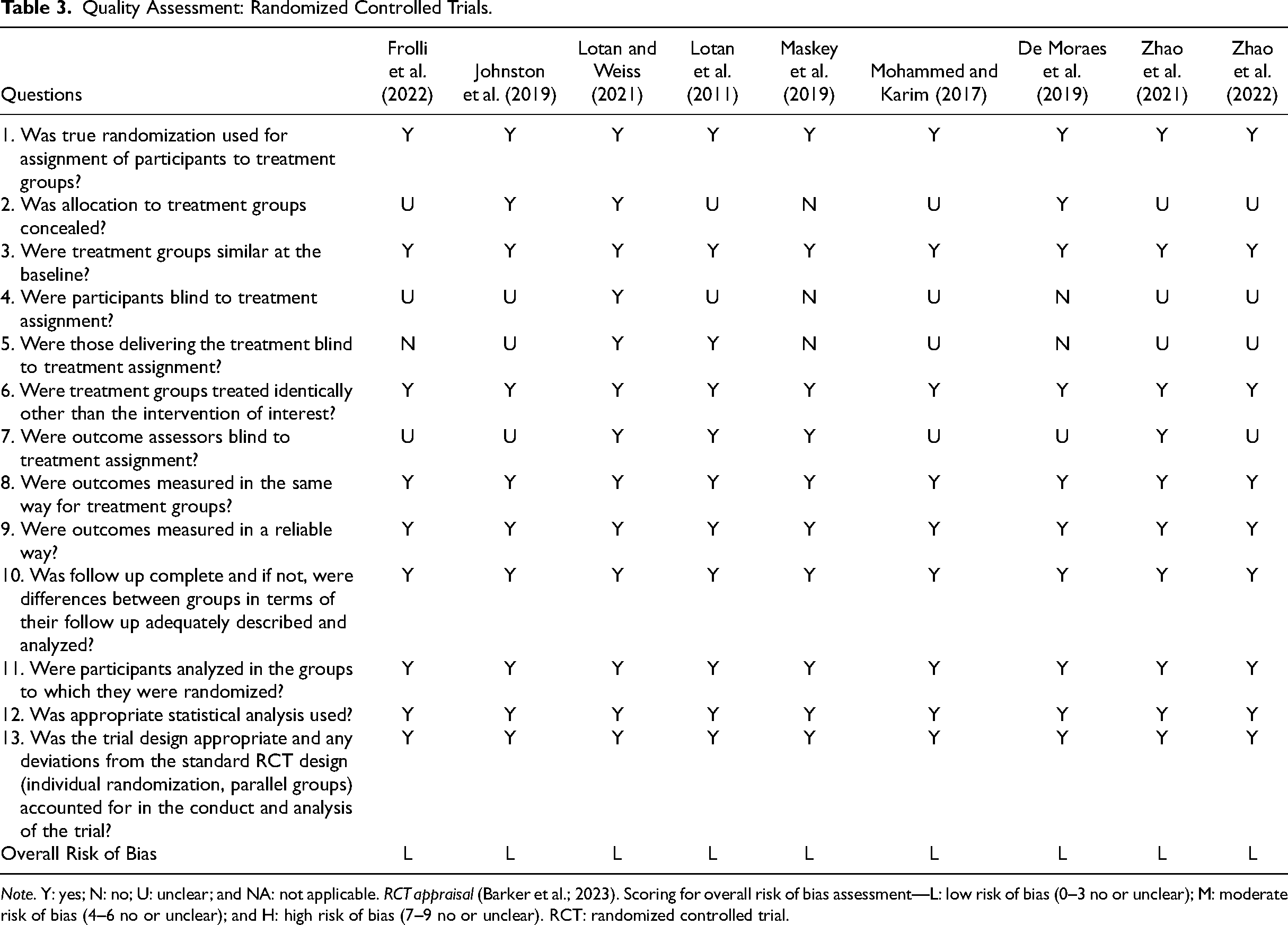
Note. Y: yes; N: no; U: unclear; and NA: not applicable. RCT appraisal (Barker et al.; 2023). Scoring for overall risk of bias assessment—L: low risk of bias (0–3 no or unclear); M: moderate risk of bias (4–6 no or unclear); and H: high risk of bias (7–9 no or unclear). RCT: randomized controlled trial.
Quality Assessment: Quasi-Experimental Studies.
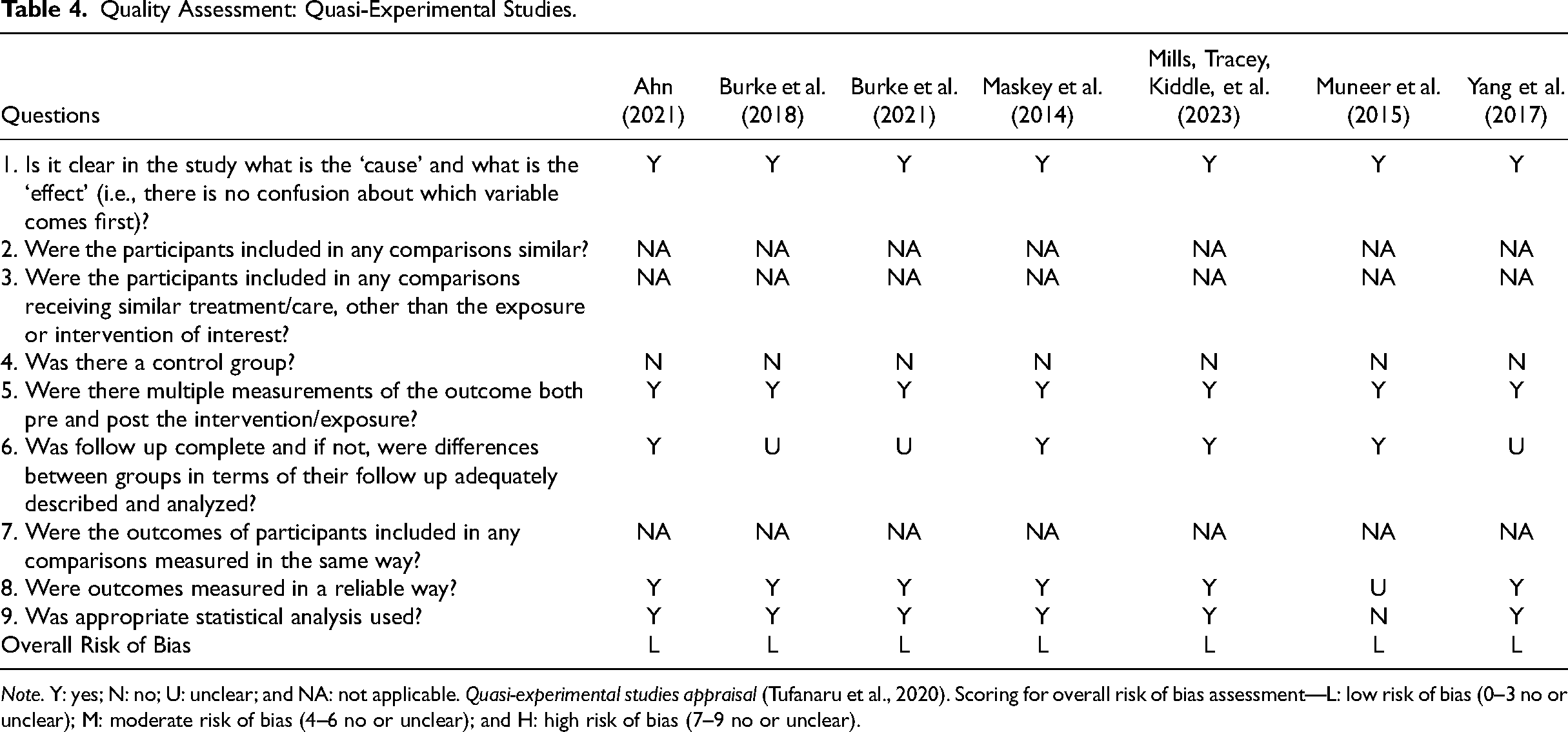
Note. Y: yes; N: no; U: unclear; and NA: not applicable. Quasi-experimental studies appraisal (Tufanaru et al., 2020). Scoring for overall risk of bias assessment—L: low risk of bias (0–3 no or unclear); M: moderate risk of bias (4–6 no or unclear); and H: high risk of bias (7–9 no or unclear).
Quality Assessment: Case Report & Qualitative Studies.
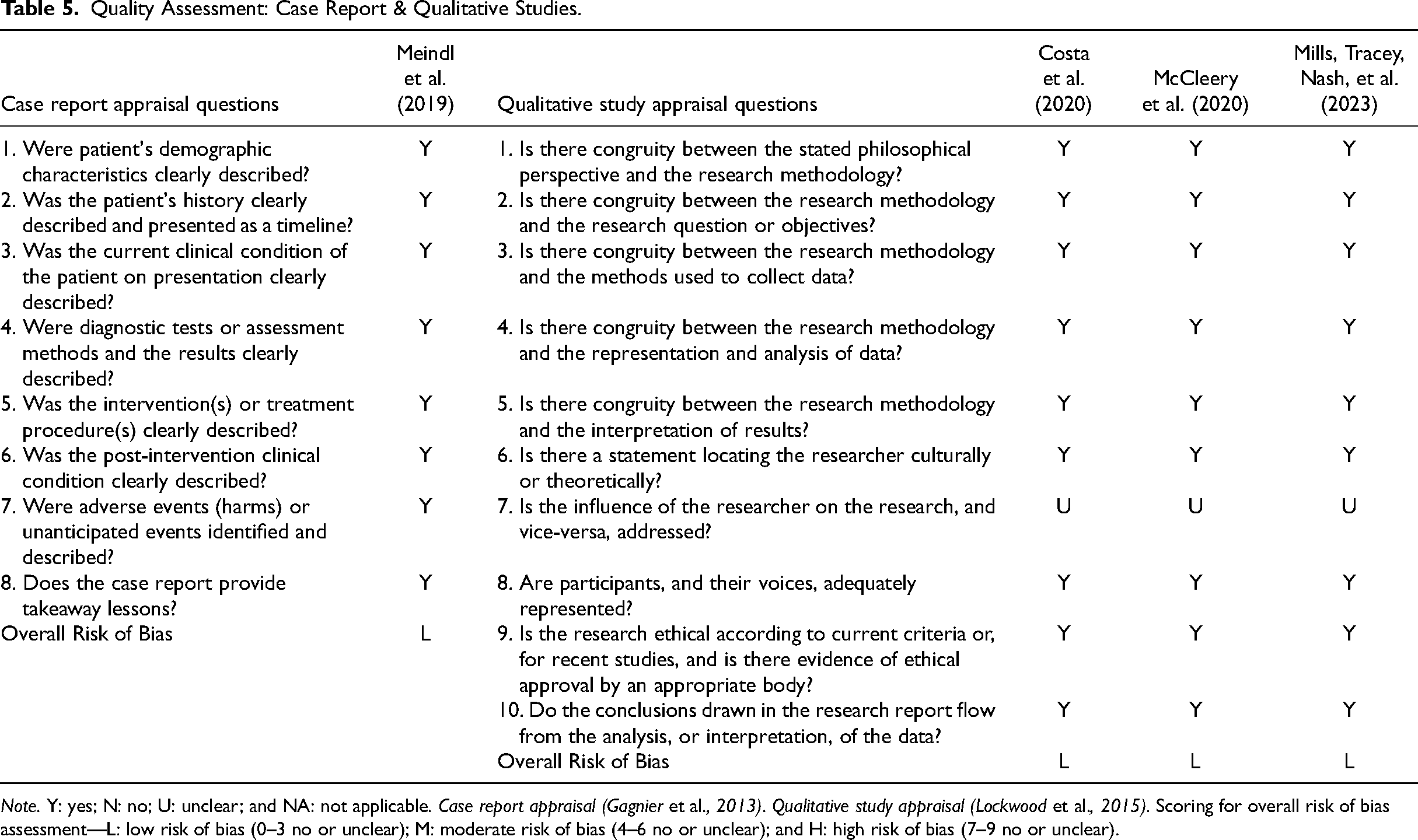
Note. Y: yes; N: no; U: unclear; and NA: not applicable. Case report appraisal (Gagnier et al., 2013). Qualitative study appraisal (Lockwood et al., 2015). Scoring for overall risk of bias assessment—L: low risk of bias (0–3 no or unclear); M: moderate risk of bias (4–6 no or unclear); and H: high risk of bias (7–9 no or unclear).
Quality Assessment: Systematic Review.
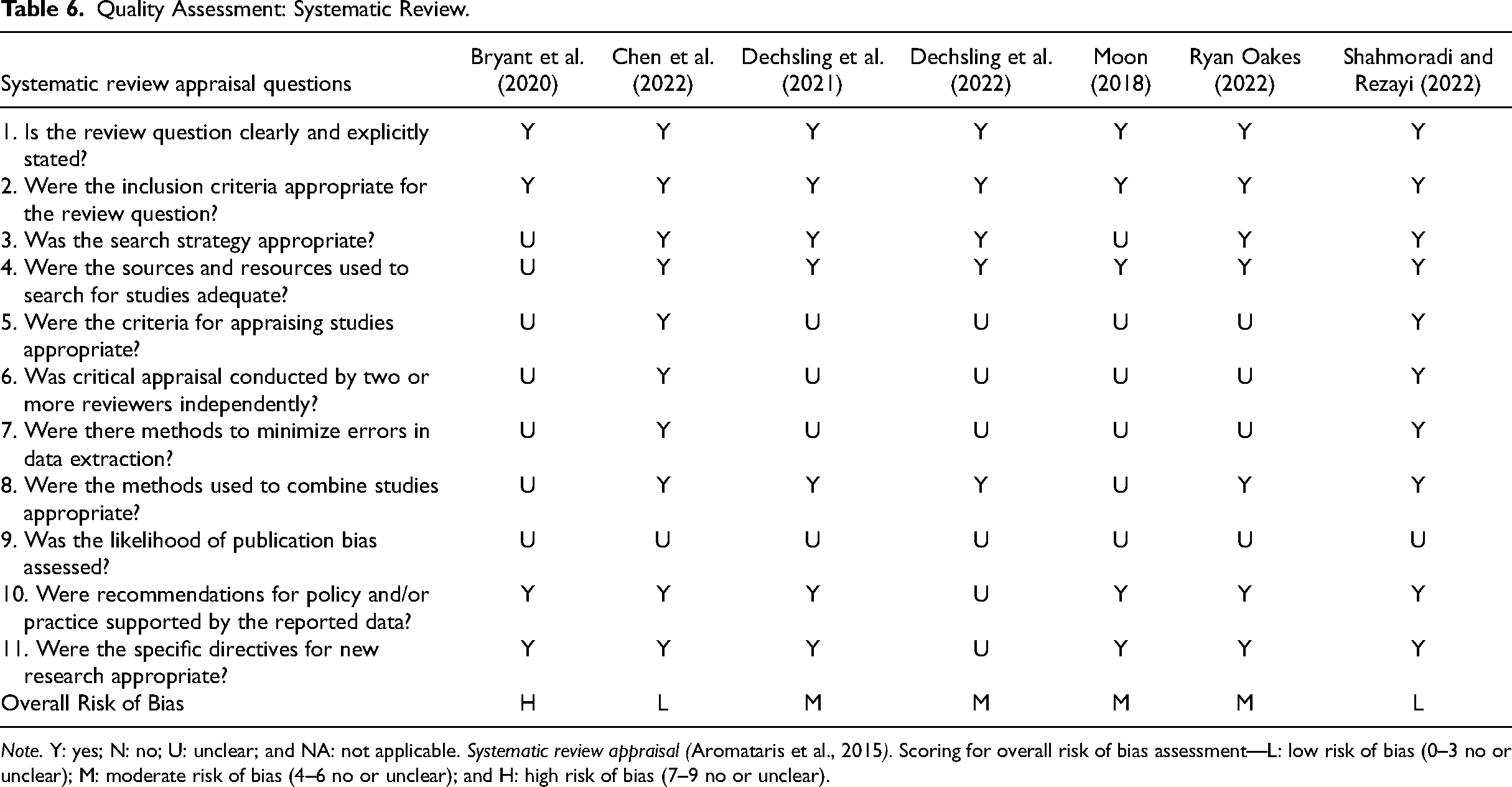
Note. Y: yes; N: no; U: unclear; and NA: not applicable. Systematic review appraisal (Aromataris et al., 2015). Scoring for overall risk of bias assessment—L: low risk of bias (0–3 no or unclear); M: moderate risk of bias (4–6 no or unclear); and H: high risk of bias (7–9 no or unclear).
Applications of VR for IDD and Rehabilitation Outcomes
For research aim one of exploring the applications of VR for rehabilitation purposes among people with IDD, this section focuses on VR interventions in 21 empirical studies, excluding review papers. While one study did not explicitly describe intervention types, twelve utilized stationary modes where VR users remained seated or standing in place and eight studies employed the modes that facilitated participant movement. In terms of immersion levels, twelve studies implemented immersive interventions, and nine used semi-immersive approaches. (Figure 3).
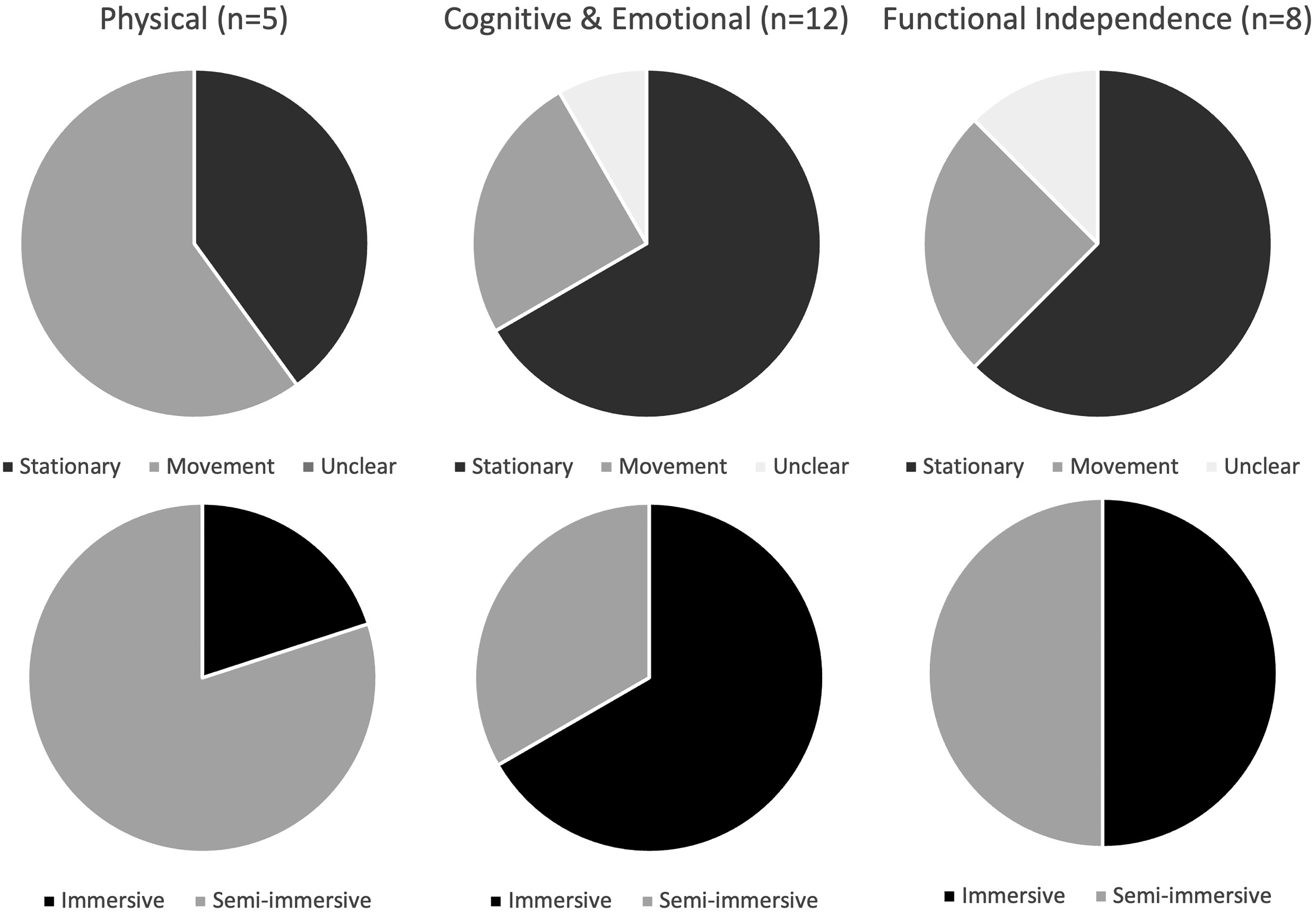
Virtual reality application characteristics by rehabilitation goals.
To address research aim two of identifying VR's effects on rehabilitation outcomes, the selected studies investigated the feasibility and/or effectiveness of VR uses for therapeutic outcomes in areas such as physical, cognitive, and functional independence domains.
Physical Domain
Within the included studies, five studies were designed to improve physical rehabilitation goals; for example, balance (Lotan & Weiss, 2021), fine motor skills (De Moraes et al., 2020; Mohammed & Karim, 2017), and engagement in physical therapy (Costa et al., 2020; Lotan et al., 2011). The five selected studies reported positive rehabilitation outcomes. The studies implemented one immersive and four semi-immersive VR systems. Regarding the VR modes, three VR interventions used the mode that assists users’ movement, while two studies used the stationary mode.
Cognitive and Emotional Domain
This section addresses cognitive and emotional rehabilitation goals and considers cognitive behavioral therapy which comprehensively involves thoughts, emotions, and behavioral changes. VR interventions in 12 studies aimed to improve cognitive and emotional aspects such as perception and attention (Ahn, 2021; De Moraes et al., 2020; Johnston et al., 2019; Muneer et al., 2015), emotion recognition (Frolli et al., 2022; Yang et al., 2017), sensory processing and well-being (Mills, Tracey, Kiddle, et al., 2023, Mills, Tracey, Nash, et al., 2023), and coping with phobia and anxiety (Maskey et al., 2014, 2019; Meindl et al., 2019). While the majority of the studies showed improvement in the above rehabilitation goals, one quantitative research reported no statistically significant differences in pre- and post-VR intervention scores on well-being, measured by the Personal Wellbeing Index–Intellectual Disability (PWI), 3rd edition, adaptive behavior, measured by the Adaptive Behavior Assessment System (ABAS-3), and anxiety level, measured by the Glasgow Anxiety Scale for People with ID (GAS-ID) (Mills, Tracey, Kiddle, et al., 2023).
Among the twelve studies relevant to the cognitive and emotional domain, eight used immersive VR goggles, and four studies employed semi-immersive screens. Regarding the VR modes, eight studies used stationary modes and three supported movement modes. The details of the VR intervention mode in one study were unclear.
Functional Independence Domain
Eight studies mentioned rehabilitation goals relevant to the functional independence of people with IDD. The areas included social communication/interaction (McCleery et al., 2020; Muneer et al., 2015; J. Zhao et al., 2021, 2022), social skills (Frolli et al., 2022; Yang et al., 2017), and vocational/interview skills and self-efficacy (Burke et al., 2018, 2021). There were four immersive, and four semi-immersive VR systems. In terms of VR modes, two employed movement modes, five used stationary modes, and one was not clearly described in the report.
VR Intervention Design Considerations
As for research aim 3 of exploring emerging themes to be considered in VR intervention design, the following sub-sections synthesize the design considerations for VR environments and interventions according to three main themes: feasibility, usability, and safety.
Design Considerations for Feasibility
Feasibility involves the viability of implementing VR for people with IDD in healthcare settings and its potential to achieve the intended rehabilitation goals. Bowen et al. (2009) examined feasibility by studying economic, technical, operational, and ethical aspects. This theme also explores any obstacles that potentially make VR use impractical for people with IDD. To examine feasibility, this study considered previous studies’ completion rates and identified any obstacles if individuals with IDD could not complete the study tasks.
Session time/frequency. According to the selected studies, a substantial majority of people with IDD who initiated the VR session completed the entire session. The studies conducted VR sessions with frequencies ranging up to three sessions per week, and the intervention period varied from one-time session to six months. McCleery et al. (2020) highlighted that a single immersive VR session is highly feasible for people with IDD. Each session duration varied within the range of 15 min to 45 min in the reported cases. Mills, Tracey, Kiddle, et al. (2023) revealed that the average length of one-instance usage was 4 min and 32 s, ranging from a few seconds to 45 min when people with IDD were given autonomy to freely engage with VR on their own agenda and timeline.
Sensory sensitivity challenges. Despite showing a high completion rate in VR intervention studies, two studies reported that people with IDD refused to wear VR goggles (Ryan Oakes, 2022; Zhao et al., 2022). These instances aligned with earlier findings that individuals with IDD declined the VR headset due to sensory sensitivity challenges (Roberts-Yates & Silvera-Tawil, 2019). Neurodivergent populations often exhibit SPD, which causes them to react to environmental sensory stimuli with hyper or hyposensitivity. There are different patterns of sensory dysfunction, and particular conditions of head-mounted VR headsets can cause people with IDD to experience sensory sensitivity challenges.
Responding to the sensory challenges, Zhao et al. (2022) adopted desensitization therapy a week before the intervention. Desensitization therapy is a psychological treatment designed to help individuals manage anxiety and reduce emotional sensitivity. This process gradually exposes individuals to the situation in a controlled and safe environment and involves trained therapists to guide these incremental steps. For successful participation, Ryan Oakes (2022) also emphasized the role of certified therapeutic recreation specialists in clinical judgment and skills to moderate sensory stimuli and guide headset usage.
Design Considerations for Usability
Usability regards how easily and effectively people with IDD can use VR technology to accomplish the sessions and achieve specific goals. This theme encompasses users’ perceptions and experiences when interacting with technology, including ease of learning, intuitiveness, satisfaction, efficiency, minimal errors, and so on (Kamińska et al., 2022). This study also considers users not only people with IDD but also the involved stakeholders such as therapists and caregivers.
Ease of use. Previous studies have examined the usability of VR technology both quantitatively and qualitatively. McCleery et al. (2020) implemented immersive VR for safety training and reported that the System Usability Scale–Autism Spectrum Disorder (SUS-ASD) scores averaged 83.58% (SD: 12.49%; range: 52.5%–100%), indicating good usability for ASD. This result corresponds with previous studies’ findings of high usability among children with ASD (Halabi et al., 2017; Ravindran et al., 2019).
Repeated use is beneficial for people with IDD to efficiently use VR technology. Several studies reported that people with IDD first displayed difficulty understanding immersive VR; however, the individuals got familiar with the virtual environments and tended to show increased outcomes with repeated use (Costa et al., 2020; Maskey et al., 2014, 2019).
Personalization. It is recommended to personalize each experience for individuals with IDD to meet their specific needs (Ryan Oakes, 2022). Incorporating therapists’ guidance is crucial for the personalization process. Suggested adaptations include optimizing the VR controller for intuitive use, differentiating control types for hand and foot motions, providing cues for anticipated experiences, and employing a sequential guide for tasks (Costa et al., 2020; Ryan Oakes, 2022; Shaker et al., 2019).
Perceived advantages. Navigating challenging scenarios in a virtual setting is notably more manageable compared to real-life situations. Therefore, this aspect potentially fosters novel treatment approaches (Ahn, 2021). When therapists expand the complexity of the world in controlled and safe VR environments, people with IDD can practice their underdeveloped skills while improving their therapeutic goals (Ahn, 2021). One study, moreover, demonstrated that in-house caregivers were able to motivate people with IDD to participate in activities using VR technology (Lotan et al., 2011; Ryan Oakes, 2022). This finding widens the spectrum of the usability of VR technology.
Perceived satisfaction. According to Costa et al.'s (2020) interview analysis and engagement scale, people with IDD demonstrated positive engagement responses to the VR system. In addition to verbally expressing their fondness for the VR during interviews, the children displayed satisfaction through smiles and positive reactions. Parents noted an enhanced engagement of their children during VR therapeutic exercises. Despite the extra time needed for VR introduction, therapists expressed satisfaction and perceived benefits of the treatments with the added virtual element.
Design Considerations for Safety
Safety considers any unfavorable events that can occur during the use of VR. McCleery et al. (2020) addressed potential safety issues associated with VR, such as motion sickness, prolonged use, addiction, and psychological impacts. Although no serious adverse events were reported across the selected studies, it is still critical to review the safety concerns raised by researchers, people with IDD, and/or their caregivers.
Motion sickness. Ensuring balance is crucial for the safety of people with IDD. Especially in the use of VR, it is important to minimize the risk of motion sickness that can cause nausea, dizziness, headaches, and disorientation due to visual-physical mismatch and disorientation (Kim et al., 2018). Motion sickness, also called cybersickness, refers to a condition arising from conflicting sensory inputs during VR use; in other words, a discrepancy between what the eyes see and what the body senses. Strategies to minimize motion sickness include using postural supports, maintaining the participant in a seated position, limiting continuous exposure time to the VR environment, and allowing the participant to actively control their movement within the virtual environment (Bryant et al., 2020).
VR Headset. Safety concerns also exist regarding VR headsets. Caregivers’ concerns were reported regarding the weight of the headset that might cause discomfort, and potential falls or collisions due to obstructed real-world vision (Costa et al., 2020). To ensure safety and prevent accidents, it is advised that VR sessions be closely supervised by therapists. Previous research also noted that some models are prone to damage or breakage (Roberts-Yates & Silvera-Tawil, 2019), so therapists and researchers should analyze the VR model's durability in advance.
Cognition. The individual is aware that the computer-generated environment is not real, yet their body and mind react as if it were real (Ahn, 2021). On the positive side, these simulations can offer a safe, controlled environment as a starting point for training or therapy for people with IDD. Unlike traditional settings, virtual environments are predictable, repeatable, and free from the complexities of social interaction. While this is promising, controversial concerns about the psychological well-being of VR users exist. On the other hand, some concerns about disorientation and psychological safety of VR users also exist. Some users might experience disorientation such as depersonalization or dissociation from reality, especially after prolonged exposure. It is crucial to limit continuous VR exposure, initiating sessions with a few minutes and gradually increasing based on the individual's comfort. Monitoring discomfort indicators such as dizziness or nausea and incorporating breaks between sessions is essential. Supervision by therapists or caregivers during these sessions becomes pivotal for managing the individual's response to the VR experience (Bryant et al., 2020).
Discussion
Existing evidence supports that VR interventions are promising for enhancing rehabilitation outcomes among people with IDD. VR technology was implemented for the improvement in physical domains (e.g., balance, motor skills, and engagement in physical therapy), cognitive/emotional domains (e.g., perception, attention, emotion recognition, sensory processing, and coping with phobia and anxiety), and functional independence domains (e.g., social communication, interaction, vocational and interview skills, and self-efficacy). The previous studies provided design considerations, which fall under the feasibility, usability, and safety themes.
Design Implications
This study's ultimate aim was to provide recommendations for designers and researchers in creating therapeutic environments using VR technology. The insights from previous research are made into design implications that help create effective, usable, and safe VR interventions for individuals with IDD as shown in Table 7.
Virtual Reality Intervention Design Strategies for People with Intellectual and Developmental Disabilities.
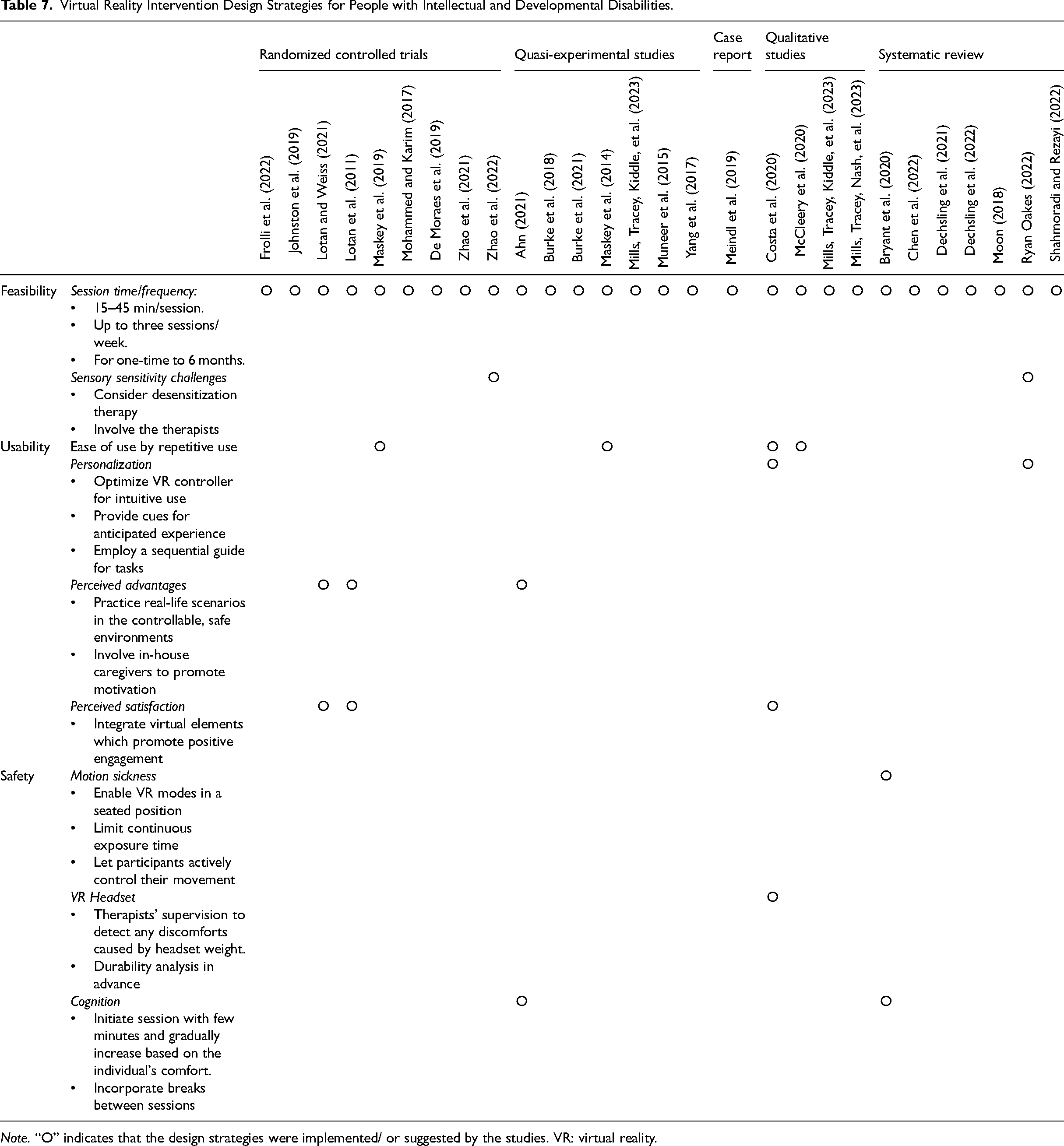
Note. “O” indicates that the design strategies were implemented/ or suggested by the studies. VR: virtual reality.
While these implications provide a starting point for VR environment design, it is crucial to acknowledge that the selected studies have limitations. There is a limited number of RCTs, and 92% of empirical studies involved small sample sizes of fewer than 50. To address these limitations, future studies should conduct larger-scale investigations to validate the inconclusive findings related to VR effectiveness for people with IDD.
Additionally, the suggested design implications should be applied with the awareness that VR is a relatively emerging technology with features fast changing. Its dynamic nature introduces an additional layer of ethical considerations. For instance, VR research must take into account privacy and confidentiality because VR applications may collect sensitive information (Bryant et al., 2020). During the informed consent process, participants need to be sufficiently informed about this aspect. It is important to avoid creating unrealistic expectations that this new technology may lead to complete recovery of function.
It is also beneficial to acknowledge VR technologies’ heavy reliance on visual and auditory information while supplementary support on tactile information offers novel methods for stimulation, enhancement, or augmentation. For instance, haptic vests, gloves, and suits can provide tactile feedback, allowing an alternative dimension of environmental awareness for patients with visual and hearing disabilities. Further examples include non-invasive corneal stimulation, transcutaneous stimulation, devices like OrCam MyEye, and a haptic vision system (Shull & Damian, 2015). Future studies can further explore the application of these technologies to assist people with IDD associated with different types of sensory challenges.
Lastly, the design implications suggest involving therapists in diverse stages of VR application, from inspecting the device to operating it with people with IDD. It is important to emphasize that therapists play a vital role in delivering VR applications and to counter any misconceptions that VR can replace the expertise of qualified therapists (Bryant et al., 2020).
Conclusion
As interest in VR technology continues to grow, there is an undeniable need to integrate VR interventions into healthcare settings to enhance rehabilitation outcomes. This systematic review provided a comprehensive summary of evidence of VR's effectiveness in improving physical, cognitive, emotional, and functional independence outcomes for people with IDD. This review also identified key considerations for future VR intervention design in terms of feasibility, usability, and safety. While these findings offer promising insights for future research, it remains imperative to adjust recommendations as technology evolves. Furthermore, considering the selected studies’ quality and quantity in the current review, conducting high-quality, larger-scale investigations is beneficial to validate and generalize the findings to a broader population.
Implications for Practice
VR interventions using immersive (e.g., VR goggles) or semi-immersive setups (e.g., large monitors) have demonstrated positive therapeutic outcomes for people with IDD in previous studies.
Prior to implementing VR interventions, therapists and researchers should conduct a comprehensive analysis of the VR model's durability. Additionally, incorporating desensitization therapy, guided by a therapist, is essential to address the sensory sensitivity challenges of the target population.
To enhance feasibility, it is recommended to adhere to session time limits, not exceeding reported durations (as observed in the selected literature, typically up to 45 min). Continuous exposure should be avoided to prevent potential negative effects such as discomfort or fatigue in participants.
To promote usability, consider repetitive uses and personalization features to tailor the VR experience to individual preferences and needs.
To ensure safety, VR modes should be designed to allow individuals with IDD to be seated while actively controlling their movements in VR, all under the supervision of therapists and/or caregivers.
Footnotes
Acknowledgements
The authors thank Iman Moradi Naftchali for assistance in writing the manuscript.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health, Well-Being, and the Built Environment Seed Grant and the Data Institute for Societal Challenges (DISC) seed grant, provided by the OU Norman Office of the Vice President for Research and Partnerships, the OU Health Sciences Center Vice President for Research, and the Christopher C. Gibbs College of Architecture.