
Abstract
Objective:
This study examines the impact of ambulatory waiting room characteristics on patients’ emotional states and investigates whether these states are universally experienced or influenced by social and cultural factors among women aged 18–35 from the three largest demographic groups in the United States: Black, Hispanic/Latina, and White.
Background:
Patients typically spend more time waiting for routine medical appointments than receiving care, and evidence suggests that waiting can reinforces power dynamics that benefit privileged groups, leading to different experiences for minority women seeking preventative care. Still, literature addressing the impact of waiting areas is largely limited to universal measures, and little is known about how different ethnic/race groups respond to waiting spaces.
Methods:
This inquiry used a questionnaire assessing 15 waiting room characteristics and testing four variables (furniture arrangement, room-scale, color saturation, and quantity of positive distractions) in a 2 × 3 quasiexperiment using a fractional randomized block design with 24 waiting room images.
Findings:
Responses from 1,114 participants revealed mutual preferences for sociopetal seating, positive distractions, neutral colors, and welcoming and calming environments. Yet, Black participants indicated significantly greater importance in seeing ethnically/racially similar patients and healthcare providers and strategies that promote transparency, including image-based provider directories and views into the clinic.
Conclusion:
By investigating the impact of the waiting room environment on patient affect and comparing perceptions across three demographic groups of women, this study offers insights into potential strategies for improving access to preventative care services by creating more welcoming ambulatory care waiting environments.
Keywords
The path to preventative care is paved with waiting, as patients can spend more time waiting for their care providers than receiving care. For instance, Gulwadi et al. (2009) concluded that patients typically experience a 24-min wait at a doctor’s office, whereas Rao et al. (2019) observed that the actual time spent with physicians during primary visits averaged 21.6 min. Pati and Nanda (2011) contended that modulating the waiting experience was an essential component of healthcare praxis, and there is little evidence suggesting that zero-wait-time operations will soon become the norm. Even as telehealth and vehicular waiting became more prevalent during the height of the COVID-19 pandemic, those arriving by public or medical transport still needed waiting spaces (Anderson, 2021). Patient waiting helps ensure efficiency but can also engender anxiety (Gordon et al., 2010; Waltz, 2017), which may be contributing to the declining prevalence of young adults having a primary care physician (Levine et al., 2020). The shift away from primary care services may be especially deleterious to those from minority, underrepresented groups, who are less apt to seek healthcare and visit a usual care provider (Chan et al., 2020; Cohen et al., 2021; Levine et al., 2020).
Waiting areas are liminal spaces largely occupied by individuals symbolically and physiologically impaired by illness or injury (Tanner, 2002). In exposing patient vulnerabilities, waiting areas can aggravate power imbalances between patients and staff (Liddicoat, 2020; Waltz, 2017), reinforce gendered hierarchies (Waltz, 2017), and potentially elicit strong emotional reactions (Akerstrom, 1997; Liddicoat, 2020; Tanner, 2002). Moreover, evidence suggests that those from minority race/ethnicity communities spend more time waiting than those from majority groups in some healthcare settings, such as emergency care (Johnson et al., 2022; Lu et al., 2021; Park et al., 2009). Still, literature addressing the impact of the waiting room’s physical environment is primarily limited to nonrace/ethnicity differentiated measures regarding anxiety mitigation (Fenko & Loock, 2014), human perception (Higuera-Trujillo et al., 2020), the assessment of environmental features (Bazley et al., 2016; McDonald et al., 2020), and those components of the patient experience that may impact approach and avoidance behaviors (Juliá Nehme et al., 2021). Consequently, the existing literature offers little insight into how women from different ethnic and racial backgrounds perceive and experience ambulatory waiting spaces.
Purpose
This exploratory research sought to understand which elements of ambulatory waiting rooms influence (i.e., elicit or regulate) patients’ affective states and the universality of these states by comparing insights from the three largest demographic groups of women in the United States (i.e., African American/Black, Hispanic/Latina, and non-Hispanic, White).
Significance
By examining the impact of the waiting room environment on patient affect and comparing perceptions across demographic groups, this study offers insights into potential strategies for improving access to preventative care services by creating more welcoming ambulatory care environments. These findings hold particular relevance in light of the numerous health inequities faced by traditionally underserved or marginalized women, including the disproportionately increasing rates of maternal mortality and early-onset breast cancer (Davis et al., 2017; Hoyert, 2022; Passmore et al., 2017).
Conceptual Framework
To understand how patients perceive and react to waiting environments, this inquiry draws upon theories of affect, exploring both the immediate and unmediated aspects of emotion, as well as the cognitive processes involved in emotional regulation and environmental appraisals.
Literature Review
Health environments have been shown to influence patient impressions (Becker & Douglass, 2008; Jacobs, 2016), impact patient engagement (Haddox, 2018), ameliorate anxiety (Fenko & Loock, 2014), and enhance healing (Andrade & Devlin, 2015; Ulrich, 1991). However, scholars contend that by highlighting injury and illness, waiting environments can signal the loss of agency, in turn, violating psychological privacy, and perpetuating negative stigmas and marginalization (Akerstrom, 1997; Haddox, 2018; Liddicoat, 2020; Pritchett & Buckner, 2004; Tanner, 2002). Consequently, patient affect can influence service judgments and approach and avoidance behaviors (Nehme et al., 2021; Van Rompay & Tanja-Dijkstra, 2010).
Ulrich’s (1983) psychoevolutionary framework asserted the centrality of affect research in understanding aesthetic responses to healthcare environments. Still, a central dichotomy in affect research is whether affect is pre- or postcognitive (Reeve, 2018; Zajonc, 1980)—the former being derived from biological predispositions and evolutionary needs, while the latter is influenced by socialization, learned cultures, and individual experiences. Similarly, affective appraisals of the physical environment are dichotomized into those that are direct and unmediated and those cognitively processed (Kaplan, 1987; Nanda et al., 2012; Parsons, 1991).
Evolutionary Models of Environmental Perception
Some scholars argue that environmental assessments primarily operate at a precognitive level, emphasizing the biological basis of emotions (Ekman, 1999; Izard, 2007; Kowalska & Wrobel, 2017). Accord to this premise, environmental responses are motivated by rapid adaptations aimed at enhancing survival (Joye, 2007; Ulrich, 1983), and reacting positively to environments endowed with features that promote well-being is advantageous (Parsons, 1991). The premise that affects precedes cognition implies that emotional responses to environmental stimuli may exhibit relative universality across diverse ethnic and racial groups, as they are thought to be driven by our innate biological needs.
Mediated Models of Environmental Perception
Other environmental perception models offer space for sociocultural influences by either positioning mediators between an occupant’s environments and their emotions or use moderators to explain this relationship. The stimulus–organism–response (S-O-R) paradigm proposes that physical environments are evaluated through cues that trigger emotional responses and subsequent behavioral reactions (Mehrabian & Russell, 1974). Juliá Nehme and colleagues (2020) expanded S-O-R by introducing the spatial user experience framework, which conceptualizes behavioral responses with two superordinate dimensions: the occupant’s goals and their affective responses to their environment. Their ensuing study, conducted in two Chilean healthcare facilities, revealed that emotional reactions had the most significant impact on user experience and behavioral intentions (Juliá Nehme et al., 2021).
Emotional Regulation in the Built Environment
Given the prevalence of negative emotions in healthcare settings (Eggleton et al., 2017; Gordon et al., 2010), patients may need to employ regulatory strategies involving endogenous factors (i.e., cognitive reappraisals) or exogenous influences that leverage the built environment through means of situational selection, situational modification, or attentional focus (Lazarus, 1991; Reeve, 2018). While situational selection involves making choices regarding approach and avoidance behaviors toward healthcare settings (Juliá Nehme et al., 2021), the execution of these choices requires some level of certainty and spatial coherence (Antonovsky, 1987; Dilani, 2009; Mazzi, 2021), which can be challenging in incompatible healthcare environments (Juliá Nehme et al., 2021) or those with inadequate wayfinding (Jacobs, 2016; Jamshidi & Pati, 2021).
Situational modification allows patients to regulate their emotions by modifying their environment, including healthcare settings, which can be facilitated by offering choices or perceived controls to confer degrees of autonomy (Devlin, 2022; Devlin et al., 2023; Liddicoat, 2020; Pearson & Wilson, 2012; Zhu et al., 2020). Attentional focus entails the redirection of one’s attention away from negative cues (Reeve, 2018), which can be influenced in waiting environments by factors involving socialization opportunities (e.g., sociopetality), room scale, color saturation, and positive distractions.
Literature suggests that patients may utilize a range of strategies to regulate negative emotions arising from biological dispositions or socialized factors. Yet, it remains unclear which features best assist patients in this regard. Accordingly, the overarching research questions (RQs) of this study are as follows:
Sociopetality
Tanner (2002) argued that rigid seating layouts underscore communal vulnerability, creating an uncomfortable intimacy among patients. To address these tensions, waiting rooms can foster feelings of intentional inclusion (Jacobs, 2016) and social support (Andrade & Devlin, 2015; Dilani, 2009; Zhu et al., 2020) through furniture arrangements that encourage interpersonal communication (Holahan & Saegert, 1974; Ulrich, 1991), a concept known as sociopetality (Nasrallah & Pati, 2021). Still, some patients may prefer privacy (Devlin, 2022) and the extent to which patients appreciate sociopetality as a component of regulating positive affect while waiting is unclear.
Room scale
Patients’ attentional focus can be impacted by room scale, with larger waiting rooms offering more visual stimuli. Some evidence suggests patients may prefer larger waiting rooms in hospital settings (Qi et al., 2021; Xuan et al., 2021), possibly due to a lower incidence of crowding (LaVela et al., 2016). Although patient flow simulations and observations can help determine the optimal number of seats for a waiting room (Ai et al., 2016), extant literature offers little guidance on how waiting room-scale preferences may differ among demographic cohorts.
Color saturation
Valdez and Mehrabian’s (1994) pleasure-arousal-dominance work revealed that saturated (i.e., pure and vivid) colors were considered more pleasant and arousing, while less bright and more saturated colors induced greater feelings of dominance. Yet, saturated colors have been linked to greater anxiety (Ireland et al., 1992), while moderate color use has been associated to positive moods (Küller et al., 2009), which may be why the color most often associated to hospitals is a soothing blue (Kaya & Crosby, 2006). While research has shown that color saturation predicts mood differences between genders in work environments (Kwallek et al., 1996), little empirical evidence links color saturation to affect in healthcare settings.
Positive distractions
Artwork, graphics, and access to nature have been shown to divert a patient’s attention from psychological (Andrade & Devlin, 2015; Dijkstra et al., 2008; Pati & Nanda, 2011; Tse et al., 2002) and physical stressors (Karnik et al., 2014; Vincent et al., 2010), as well as promote feelings of support (Liddicoat, 2020). Literature suggests that offering positive distractions, including those that affirm one’s identity (Bansfield, 2022; Kreuter & Haughton, 2006; Wang & Arpan, 2020) and accommodate family members (Andrade & Devlin, 2015; Waltz, 2017; Zhu et al., 2020), may enhance a woman’s affect while waiting, though the degree of this effect is uncertain.
Literature summary
Extant research has not conclusively established the impact of waiting room characteristics, such as sociopetality, room scale, color saturation, and positive distractions, on patients’ emotions during their waits for medical appointments. Moreover, it remains unclear whether patient responses to these characteristics are universally consistent based on innate preferences or influenced by social and cultural conditioning.
Methodology
This inquiry utilized a questionnaire as a component of a 2 × 3 quasi experimental and randomized block design testing four factors (Kirk, 2007, 2013). Three images were selected to represent two levels of each favor: (1) sociopetality via seating arrangement (sociopetal vs. sociofugal), (2) room-scale (institutional vs. residential), (3) color (saturated vs. neutral), and (4) stimulation (more than three manifest positive distractions vs. one positive distraction; totaling 24 images).
Setting
A U.S.-based national Qualtrics panel was used for data collection. This protocol was approved by the researchers’ institutional review board in May 2022.
Sample and Recruitment
The target population for this study was African American/Black, Hispanic/Latina, White, and non-Hispanic women aged 18–35. As indicated in Table 1, the sampling frame reflected a nationally representative sample of these cohorts according to U.S. Census data.
Purposive Sample Recruitment Criteria.
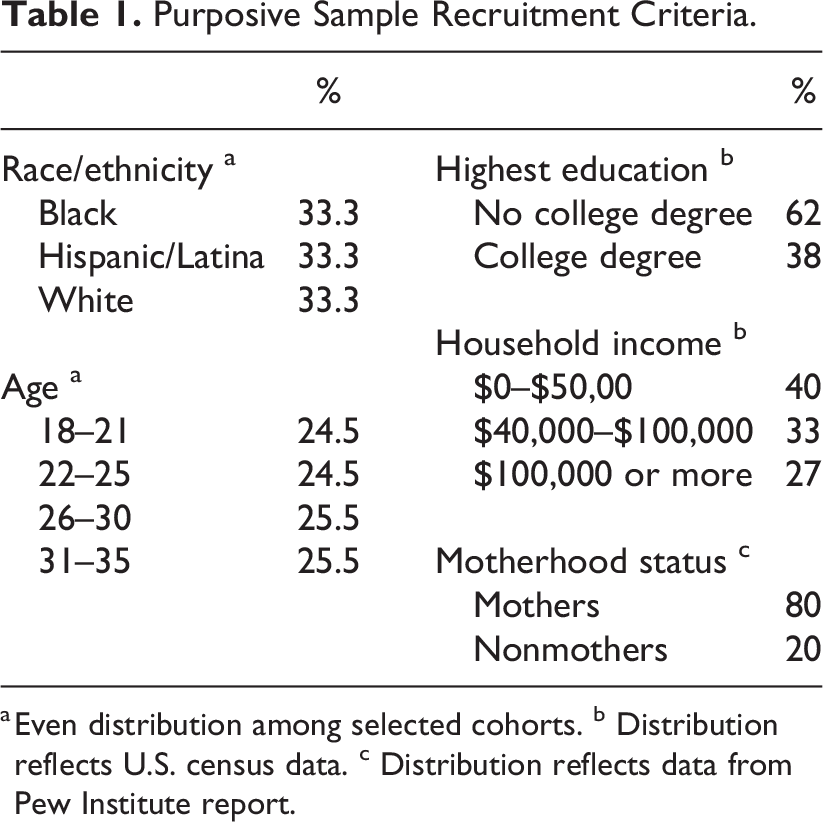
a Even distribution among selected cohorts. b Distribution reflects U.S. census data. c Distribution reflects data from Pew Institute report.
A priori power analysis was conducted in G*Power 3.1.97 to determine the necessary sample size (Faul et al., 2007). Results indicated that to achieve a 90% power for detecting a small to medium size effect (f = .20) with an F test between three demographic groups at a significant criterion of α = .05, a sample size of 270 from each demographic cohort was needed.
Instrument
Part 1. Affective states and waiting room preferences
Participants used 7-point Likert-type scales to rate their desired affective states and indicate the waiting room features, such as seating options and provider credentials, that best assist them in achieving those states.
Part 2. Waiting room image assessment
All images used in the quasi experimental waiting room assessments were sourced from U.S.-based trade publications or design competition press releases within the last 5 years from either the American Institute of Architects, the International Interior Design Association, or Healthcare Design Magazine. Each participant used three 7-point semantic differential affect scales (i.e., anxious/calm, suspicious/trusting, and despairing/hopeful) to evaluate one randomly assigned image representing each condition from each variable (for a total of eight images).
Part 3. Healthcare utilization and demographic questions
In addition to demographic questions, participants were queried about their utilization of primary care facilities, specifically regarding attendance to annual checkups, current vaccination status, and the occurrence of major medical issues within the last 5 years, which was characterized as giving birth, undergoing surgery, or experiencing a sudden or chronic illness.
Data Analysis Methods
The responses were analyzed using SPSS Version 26. The reliability of the image ratings across the three affect scales was evaluated using Cronbach’s α. The lowest scoring image had an α coefficient of .767. To generate a composite score for each image, the three affect scores were averaged. Repeated measures analyses of variance (ANOVAs) with Bonferroni correction and Tukey post hoc tests investigated group differences across the two levels of each factor using these composite scores.
Findings
4,802 women responded to the Qualtrics invitation, of whom 1,114 were included in the study after exclusions for not meeting demographic qualifiers, nonconsent, attention check failures, incompletion, and response times that were below one-half of the median soft launch time of 5 min. As indicated in Table 2, approximately one-third of respondents reported from each of the selected ethnicity/racial groups. Fifty-nine percent of respondents were in their 20s. The vast majority (83.8%) had health insurance coverage and had attended a routine medical visit within the last year (73.2%). Nearly 40% had obtained a bachelor’s degree or more, and 78.1% had children in their household. Over half reported having a major medical issue within the past 5 years.
Participant Characteristics.
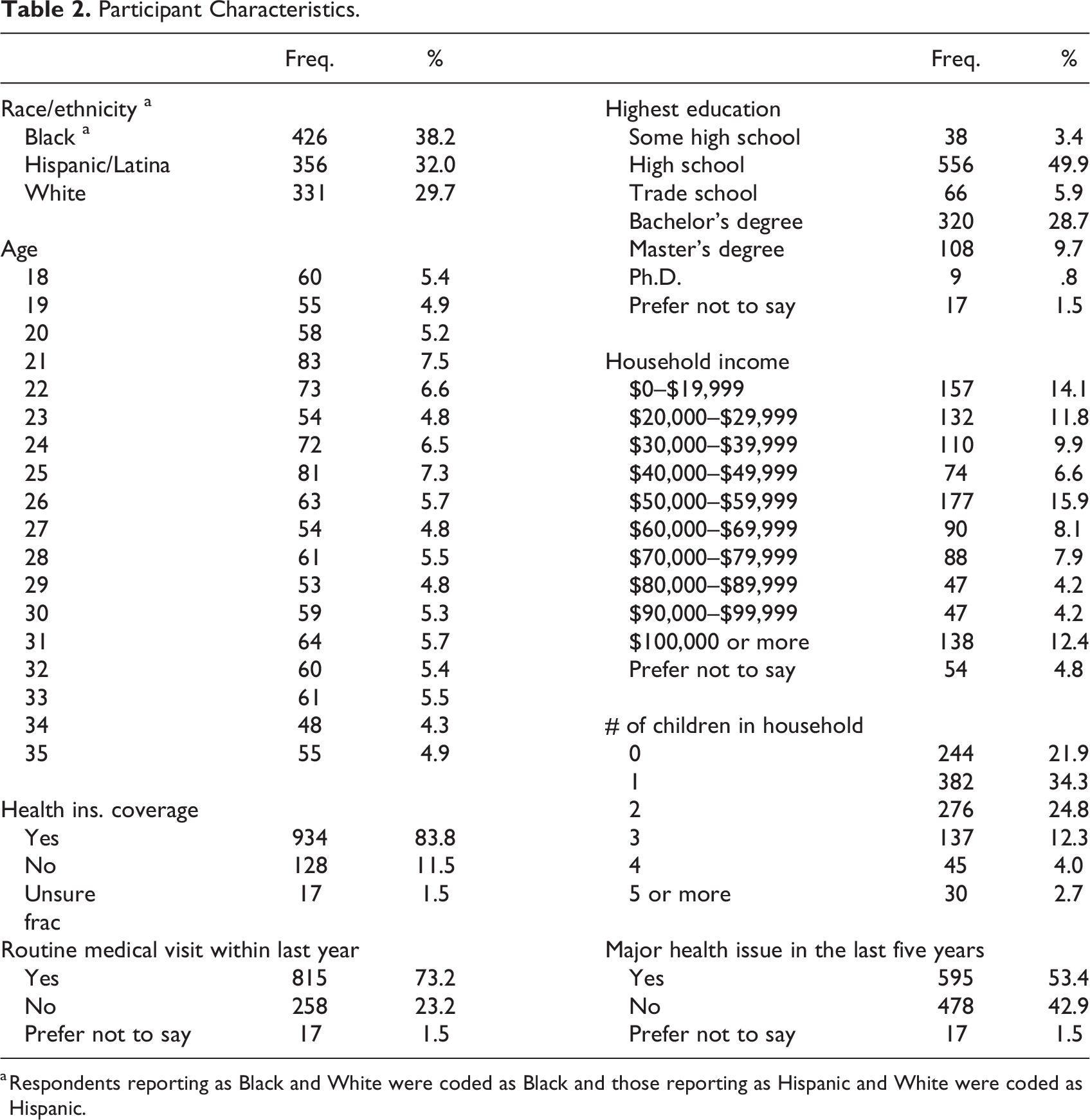
a Respondents reporting as Black and White were coded as Black and those reporting as Hispanic and White were coded as Hispanic.
Positive Affect Eliciting Waiting Room Features
A repeated-measures ANOVA determined main effects among positive affect-eliciting features in waiting rooms, F(9.3, 1,096) = 572.65, p = <.001, η2 = .340, and ethnicity/race, F(2, 1,110) = 6.608, p = .001, η2 = .37. Additionally, there was a significant interaction effect between these variables, suggesting that the relationship between positive affect-achieving feature scores was influenced by ethnicity/race, F(18.7, 1,105) = 5.57, p = <.001, ηpartial = .01. Mauchly’s test indicated a violation of the sphericity assumption, χ2(20) = 1,713.94, p = <.001, and results are reported from the Greenhouse–Geisser correction.
Positive Affect Eliciting Waiting Room Features, Means, and Standard Deviations.
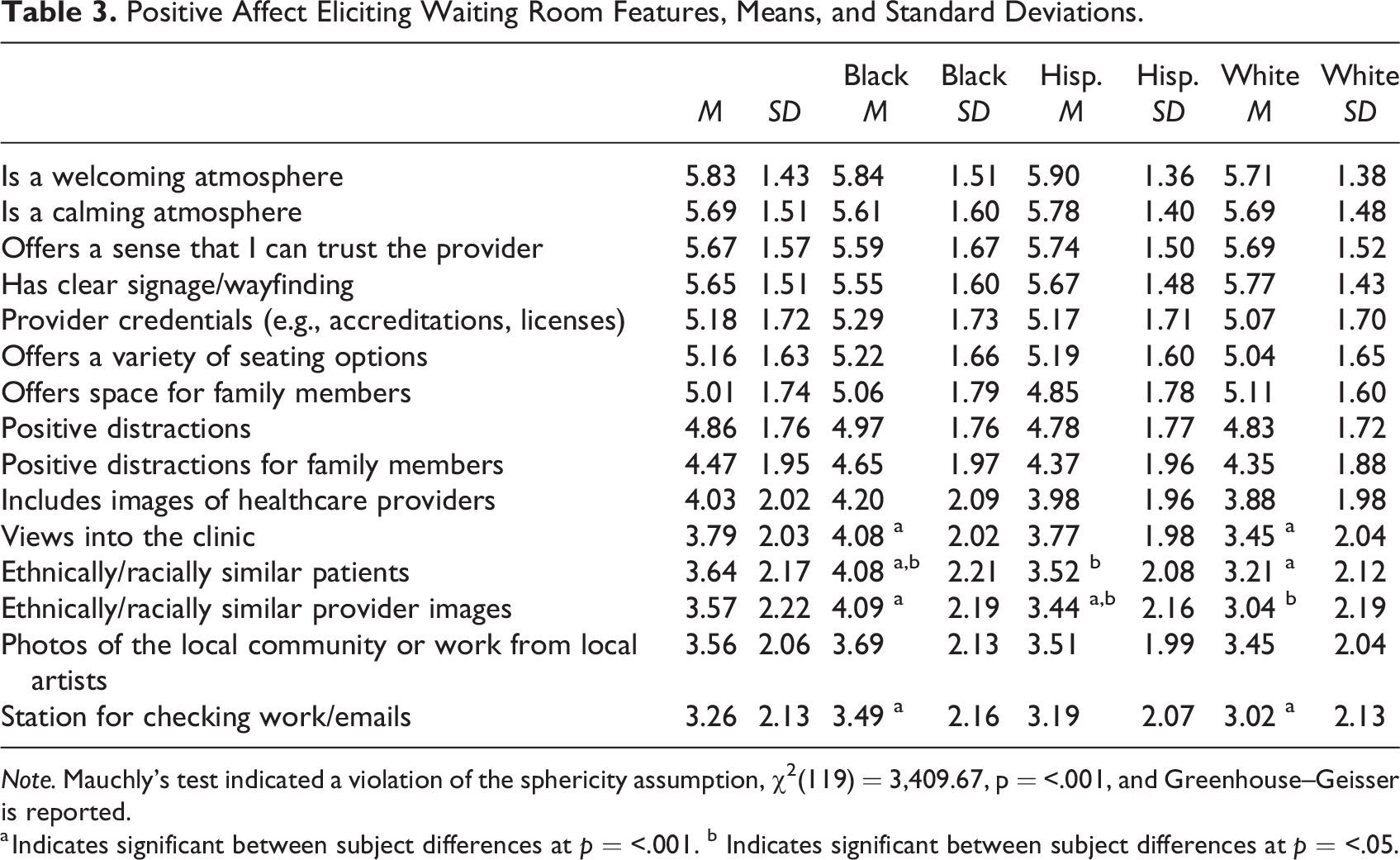
Note. Mauchly’s test indicated a violation of the sphericity assumption, χ2(119) = 3,409.67, p = <.001, and Greenhouse–Geisser is reported.
a Indicates significant between subject differences at p = <.001. b Indicates significant between subject differences at p = <.05.
RQA. As indicated in Table 3, each of the 15 positive affect-eliciting features was deemed at least neutral in importance for achieving a positive affect. Among them, a welcoming atmosphere scored statistically significantly higher than all but a calming atmosphere (M = 5.68, SD = 1.51), trust-eliciting features (M = 5.69, SD = 1.57), and clear signage (M = 5.63, SD = 1.51) at p = <.05. Each of these variables were deemed very important by the survey’s parameters. A calming atmosphere scored statistically significantly higher than all features except for trust-eliciting features and clear signage at p = <.05.
Black participants scored a welcoming atmosphere scored statistically significantly higher than all but a calming atmosphere at p = <.0001. Among Hispanic/Latina participants, a welcoming atmosphere scored more similarly to other variables but was statistically higher than seating options (M = 5.19, SD = 1.60), provider credentials (M = 5.17, SD = 1.71), space for family (M = 4.85, SD = 1.78), distractions for family (M = 4.37, SD = 1.96), images of providers (M = 3.98, SD = 1.96), views into clinic (M = 3.77, SD = 1.98), other patient ethnic/racial similarity (M = 3.53, SD = 2.08), local photos/art (M = 3.51, SD = 1.99), provider ethnic/racial similarity (M = 3.44, SD = 2.16), and station for work/emails (M = 3.19, SD = 2.07) at p = <.001. The highest scoring feature among the White participants was clear signage (M = 5.77, SD = 1.43), which scored statistically significantly higher than all but a welcoming atmosphere (M = 5.71, SD = 1.38), a calming atmosphere (M = 5.69, SD = 1.48), and trust-eliciting features (M = 5.69, SD = 1.52) at p = <.001.
Furniture Arrangement Preferences, Means, Standard Deviations, and Confidence Intervals (CIs).
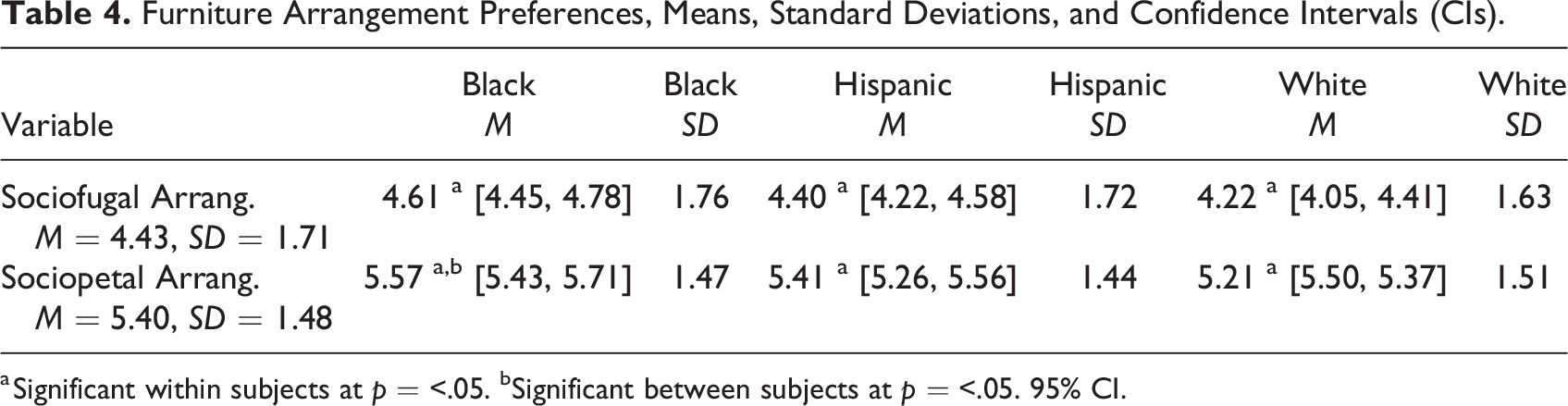
a Significant within subjects at p = <.05. bSignificant between subjects at p = <.05. 95% CI.
Room Scale preferences, Means, Standard Deviations, and Confidence Intervals (CIs).
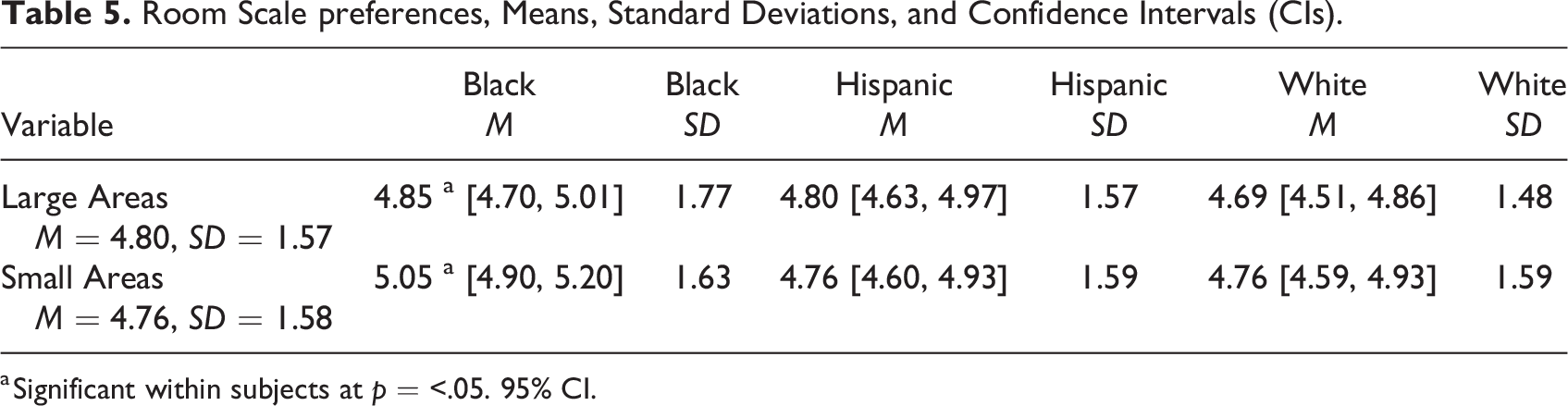
a Significant within subjects at p = <.05. 95% CI.
Waiting Room Color Saturation Preferences, Means, Standard Deviations, and Confidence Intervals.
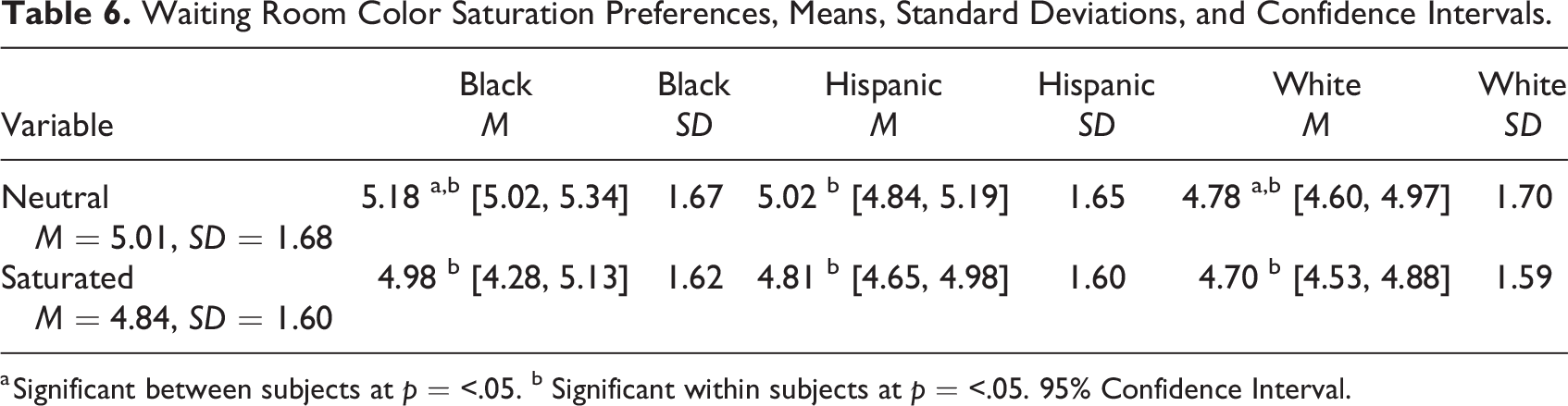
a Significant between subjects at p = <.05. b Significant within subjects at p = <.05. 95% Confidence Interval.
Waiting Room Stimulation Preferences (>Three positive Distractions vs. One positive Distraction), Means, Standard Deviations, and Confidence Intervals (CIs).
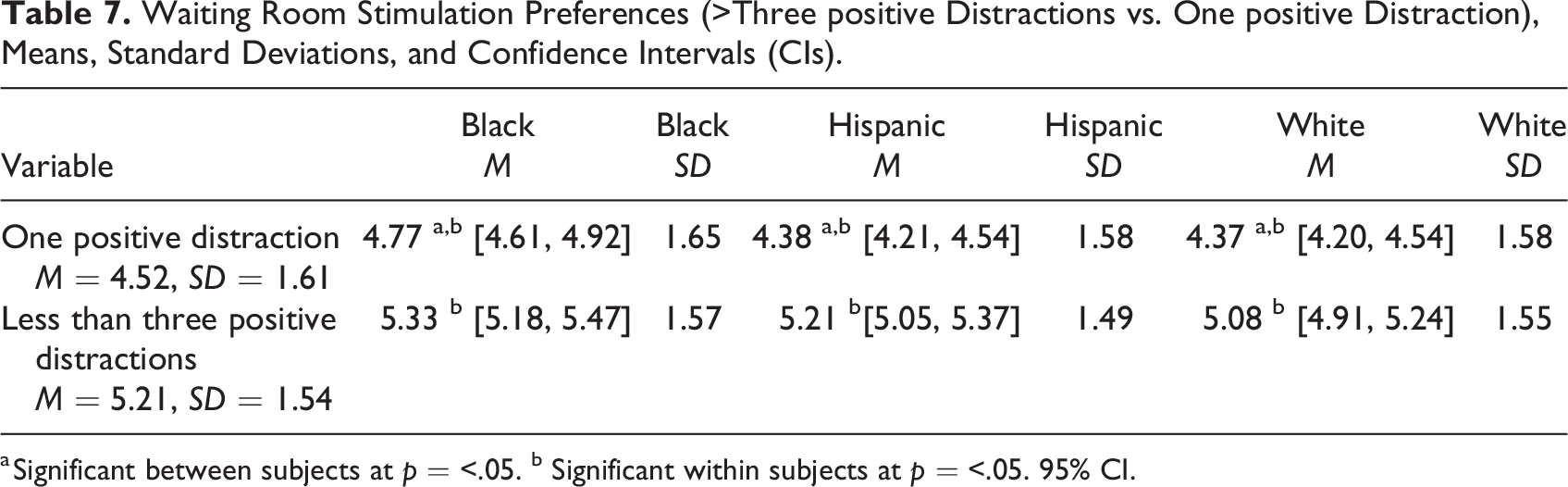
a Significant between subjects at p = <.05. b Significant within subjects at p = <.05. 95% CI.
Discussion
This study aimed to disentangle universal medical waiting preferences from those potentially influenced by socialization and cultural factors coinciding with race and ethnicity in the United States.
Implications
These findings suggest that some waiting room preferences may be relatively consistent across Black, Hispanic, and White women in the United States. For one, a welcoming and calming atmosphere was considered important for establishing or maintaining a positive affect by each cohort. These preferences support the premise that waiting environments considered inclusive and attractive can improve patients perceptions and decrease anxiety (Becker & Douglass, 2008; Jacobs, 2016; Pearson & Wilson, 2012). Yet, further research is needed to investigate the components that contribute to creating a welcoming atmosphere in medical waiting rooms.
The analysis of image reactions revealed that all groups expressed a preference for sociopetal seating arrangements, neutral color schemes, and multiple sources of positive distraction, in turn, suggesting that a range of attentional focus strategies may be used when waiting. Additionally, sociopetal furniture arrangements, which promote social interaction, may offer patients perceived emotional benefits (Andrade & Devlin, 2015; Reeve, 2018), even if they prefer not to actively participate in conversation (Devlin, 2022). Findings also lend support to Tanner’s (2002) assertion that inflexible chair arrangements may levy negative effects on patients’ emotional states, possibly because such environments lack opportunities for modulation. These findings are also consistent with existing research suggesting that a moderate use of color can enhance moods (Küller et al., 2009) and reduce anxiety (Gray et al., 2012). Additionally, the findings affirm the benefits of incorporating positive distractions in waiting rooms (Andrade & Devlin, 2015; Dilani, 2008; Karnik et al., 2014), which were well-received across different demographic cohorts.
The data also revealed differences among cohorts, with the most prominent variances emerging between White and Black participants, with Hispanic scores situated between the two. Black participants placed a higher importance on cultural similarity with fellow patients and healthcare providers, which aligns with the findings of Townes and colleagues (2022) regarding the significance of race and gender similarity between service providers and Black female patients. Additionally, these participants valued design elements that promote transparency and potentially help alleviate their uncertainty, such as image-based provider directories and glimpses into the clinic. Still, White participants indicated signage as most likely to elicit a positive affect (ahead of a welcoming atmosphere). This finding may suggest that White patients may already feel relatively more welcomed in ambulatory medical environments.
Limitations
The limitations of this study include its cross-sectional design, which may not fully account for the dynamic and multifaceted nature of healthcare experiences and the built environment in which they occur. Additionally, the ecological validity of online surveys may be constrained, and the use of only three waiting room images may not comprehensively encompass all potential environmental features, potentially affecting construct validity. Future studies should replicate these findings with different stimuli. Lastly, it is important to acknowledge that ethnic/racial identity is a complex construct. While this study aimed to consider learned and socially constructed preferences, it provided a limited assessment of waiting priorities among the three largest demographic cohorts of women in the United States. Therefore, further investigations utilizing alternative research methods should be conducted to extend or refute these findings.
Conclusion
This study’s findings help to prioritize design strategies that contribute to positive affect in ambulatory care waiting rooms for women in the three largest demographic groups in the United States. The results suggest that a welcoming, socially imbued environment with positive distractions and a neutral color palette is likely preferred, thus necessitating a balance of stimulating and calming features. These findings also underscore different perceptions, namely, regarding the importance of representation and design strategies aimed at promoting transparency among Black women in medical waiting environments. Taken together, this study provides insights to inform the design of healthcare waiting room environments and potentially contribute to improving women’s preventative healthcare-seeking behaviors. Future research can build on these findings to explore additional factors that influence patient experiences in waiting rooms and develop design interventions that promote positive affect.
Implications for Practice
Understanding the preferences of patients from different racial and ethnic backgrounds is crucial for creating welcoming and inclusive healthcare environments. Based on the findings of this study, healthcare designers should consider the following: Balancing stimulating and calming features to create a welcoming, socially imbued environment with positive distractions and a neutral color palette. Recognizing the potential for different perceptions among Black women regarding representation and design strategies aimed at reducing uncertainty in medical waiting environments.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231204979 - Designing Worthy Waiting Spaces: A Cross-Cultural Study of Waiting Room Features and Their Impact on Women’s Affective States
Supplemental Material, sj-pdf-1-her-10.1177_19375867231204979 for Designing Worthy Waiting Spaces: A Cross-Cultural Study of Waiting Room Features and Their Impact on Women’s Affective States by Amy Huber and Rachel Bailey in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.