
Abstract
Background:
The contributions of cognitive and behavioral work of patients' family members in intensive care units remain largely unrecognized.
Objective:
The objective of this study was to develop a framework of outwardly observable family work, with specific focus on describing the physical space.
Methods:
We conducted approximately 50 hrs of naturalistic observations of family activities on a medical intensive care unit (MICU) at a large, Midwestern teaching hospital.
Results:
We created a framework of activities that include requesting, receiving, or delivering either information or action, along with examples. Further, we identified clinician and staff roles with whom families interact and characterized the physical spaces in which interactions take place.
Conclusions:
Knowledge contribution is a proposed framework of family activities in the MICU. It has the potential to guide and be further described by future research and to inform development of human-centered family-facing interventions to support cognitive and behavioral cognitive and behavioral work.
The emotional work of family members of patients in intensive care units (ICUs), associated with managing stress and uncertainty, is commonly recognized (Abdul Halain et al., 2022; Jo et al., 2019; Naef et al., 2021). However, the work that family members carry out is not just emotional but also cognitive and behavioral. Ranging from decision making regarding treatment planning and end-of-life (Scott, 2022); to patient care activities such as grooming or feeding (Hetland et al., 2022); and to identifying unique, valid, and clinically relevant safety issues (evidenced in pediatric inpatient settings; Khan et al., 2022), family members may engage in a variety of ways. The contributions of their work are largely unrecognized and unsupported (McAdam et al., 2008), with active barriers to meaningful engagement persisting within and outside of the healthcare system (Beesley et al., 2016).
Background
The value of family presence in the ICU is evidenced in the literature. For example, investigators conducted a qualitative study characterizing family participation in rounds in Canadian hospitals and concluded that although quality of rounds was not impacted, family presence may support relationship building and shared decision making between families and clinicians (Au et al., 2018). Some investigators have sought perspectives from multiple stakeholders on family participation. A French survey study concluded that patients, families, and clinicians had generally favorable perceptions of family participation in ICUs (Garrouste-Orgeas et al., 2010). A mixed-methods Australian study characterized family perception of their contribution to patient’s emotional and psychosocial well-being as crucial (Wong et al., 2020). On the other hand, a 2022 integrative review highlighted that the research gap of capturing perspectives of all stakeholders still remains. Authors stressed that family participation (Wong et al., 2020) in care activities needs to be supported by training and education, not just for healthcare providers but also families (Dijkstra et al., 2022). For instance, a customized family- and patient-centered intervention implemented in a Korean cardiovascular ICU reduced anxiety and improved satisfaction in families (Yoo & Shim, 2021). Of note is the caution of generalizing findings across national healthcare systems given structural, financial, and societal differences.
Objective
In this study, we took a human factors science perspective. Human factors science uses systems-thinking to study and characterize behavioral and cognitive work of target users in service of developing human-centered tools and interventions. In their human factors framework of Systems Engineering Initiative for Patient Safety 2.0 (SEIPS 2.0), authors highlight that patients and families conduct effortful activities, referred to as patient or caregiver work (Holden et al., 2013). However, there is a research and operational gap in characterizing the work of family members in ICUs. Further, ICUs are complex work systems and families may lack knowledge or comprehension of roles and responsibilities of clinicians and staff, as well as of clinical processes. Although numerous studies have examined clinician performance in complex settings (characterized by high patient acuity and clinician workload, as well as stress, noise, short timelines, and uncertainty; Ahmadi et al., 2022; Bueno et al., 2019; Koomen et al., 2021), family work and associated support needs are rarely considered.
Health and well-being, psychosocial support, and satisfaction are themes associated with unmet family needs identified by authors of a 2019 scoping review (Scott et al., 2019). Authors suggested that to address these needs, families need to be engaged in the design and implementation of interventions. Stressing that family needs are diverse, authors of a 2022 systematic review found that nurse-led interventions, including education and information, intervention bundles, and emotional support, resulted in improved family outcomes (Kiwanuka et al., 2022). This is evidence that interventions need to support not just emotional work and that metrics of family experience need not be limited to satisfaction. To develop effective interventions, there is a need to characterize family work in intensive care settings with qualitative methods that allow the capture of context and depth (Pope & Mays, 2020).
Our research question was: What types of work do families conduct in an ICU? The objective of this study was to propose a framework informed by outwardly observable family work, with specific focus on describing the physical settings in which it is conducted. Through naturalistic observations, we captured family activities engaging with clinicians and staff, providing nonclinical patient care, and the physical spaces where these activities took place.
Method
This research complies with the American Psychological Association Code of Ethics and was approved by the institutional review board at our institution and determined to be exempt.
Setting
The setting was the Medical Intensive Care Unit (MICU) at a Midwestern, large teaching hospital. The hospital is staffed by over 600 active physicians, has 495 beds, and serves an inner-city population. The MICU has 19 single-patient rooms to provide acute care for critical adult patients. It is located on the west side of the sixth floor of the hospital and has 19 beds split between two parallel hallways, with 10 beds (one of the rooms has two beds) in one hallway and nine in the other. Visitation policy allowed two visitors at a time during the visiting hours of 10 a.m. to 7 p.m.. We are not aware of any policy changes to visitation that occurred during the study.
To gain access to the MICU, the principal investigator (E.L.P.) coordinated with the unit nursing director. Following an email exchange, we provided them with the background and objective of the study in a face-to-face meeting. They gave us a tour of the unit and introduced us to clinicians and staff. We negotiated and agreed upon a process to notify them of our planned days and hours for observations on a weekly basis. They posted our weekly schedule along with a study description in the staff lounge on a dry erase board. On at least three occasions, we provided snacks (e.g., donuts) in appreciation for cooperating with our presence on the unit.
Observers and Materials
Observations and analysis were conducted by two researchers, one with a PhD in human factors psychology (E.L.P.), with training and experience in applying qualitative research methods, and the other an undergraduate student (U.A.).
We developed and iteratively revised an observation guide. During observations, a researcher took notes on a printed copy of the observation guide (as well as in a notebook) using a clipboard and pen.
Procedure
Two researchers (E.L.P. and U.A.) conducted the first 6 hr of observations to establish reliability and consistency. For the rest of the observation period, one researcher (U.A.) conducted the observations. On each observation session, they arrived on the unit and commenced observations by first capturing whether visitors are present, their location (inside or outside patient room), and what activities they are engaged in. Observations were limited to outside of patient rooms. However, visual access into patient rooms was available through open doors and unobstructed windows, unless a patient was undergoing a private procedure (in which case, the door was closed and window curtains drawn). In the former cases, the researcher could visualize presence, location, and activities of visitor(s). Across the observation sessions, the researcher regularly walked up and down the MICU hallways to capture any changes to visitor status. The researcher made efforts to remain unobtrusive during the observations. Observation sessions lasted from 1 to several hours in duration. The researcher typed notes in Microsoft Word within 24 hr of conducting observations and uploaded to a secure shared folder.
Analysis
Data collection yielded typed observation notes. We (E.L.P. and U.A.) met weekly across the duration of the data collection effort to conduct analysis. Prior to each meeting, both researchers reviewed the notes independently. In Phase 1 of the analysis, we documented the roles of individuals with whom family members interacted and the associated physical spaces. We iteratively updated the list. In Phase 2, we conducted data analysis guided by Braun and Clarke’s (2006) reflexive thematic analysis. We identified examples of observable family activities and organized them into two categories: (1) information exchanges with clinicians and staff and (2) nonclinical patient care. In Phase 2, we organized the two categories into subcategories indicating directionality—for example, request versus deliver information or patient care. We reached consensus through discussion. We documented analysis products (e.g., examples and descriptions) in a Microsoft Excel spreadsheet.
Results
Over a period of 18 months in 2017–2018, we conducted approximately 50 hr of observations on the MICU. Observations occurred at varying times on weekdays and weekends. None of the observations occurred during the night shift (outside of visiting hours) or on holidays.
Clinician and Staff Roles
Families of MICU patients may interact with over 20 individuals in various roles on a given shift. We observed and identified the following roles of clinicians and staff with which families may be co-located and engage with while on the unit and/or in the patient room: attending physician, fellows (multiple), residents (multiple), medical students (multiple), nurse (multiple accounting for shift changes and breaks), respiratory technician, patient care assistant (PCA) or nurse technician, physical therapist, occupational therapist, consulting physician teams (multiple specialties, multiple individuals in each team), chaplain, palliative care assistant, social worker, pharmacist, dietician, dietary services, unit clerk, custodial services, police, and sitter (if patient is a risk to themselves).
Physical Spaces
There are three primary areas in which information exchanges between families and clinicians take place: (1) patient room: ad hoc information exchanges and requests; (2) hallway, including nurses’ station: time-sensitive information exchanges and requests of clinicians; and (3) family conference room: end-of-life decisions and organ donation meetings that include family, physicians, and chaplain.
Further, we identified several insights through our observations of the use of physical spaces. Physical spaces in which interactions with families take place are determined by privacy (freedom from visual and auditory attention) and topic sensitivity and urgency. Given most activities take place within the patient room, several implications of its use emerged. We observed that during rounds and consults, the presence of multiple clinicians in the patient room created a physical barrier to visual and auditory access to information for families and other clinicians. In other words, people in the back may not be able to see and/or hear. On the other hand, closing doors and curtaining windows by the family created a barrier to immediate healthcare delivery. Specifically, we observed nurses verbally expressing uncertainty on whether they can enter the room (e.g., “Did the family draw the curtain?”) before knocking or announcing themselves. Thus, the way that physical spaces are used by individuals in different roles can contribute to uncertainty and create barriers to information flow.
Family Activities
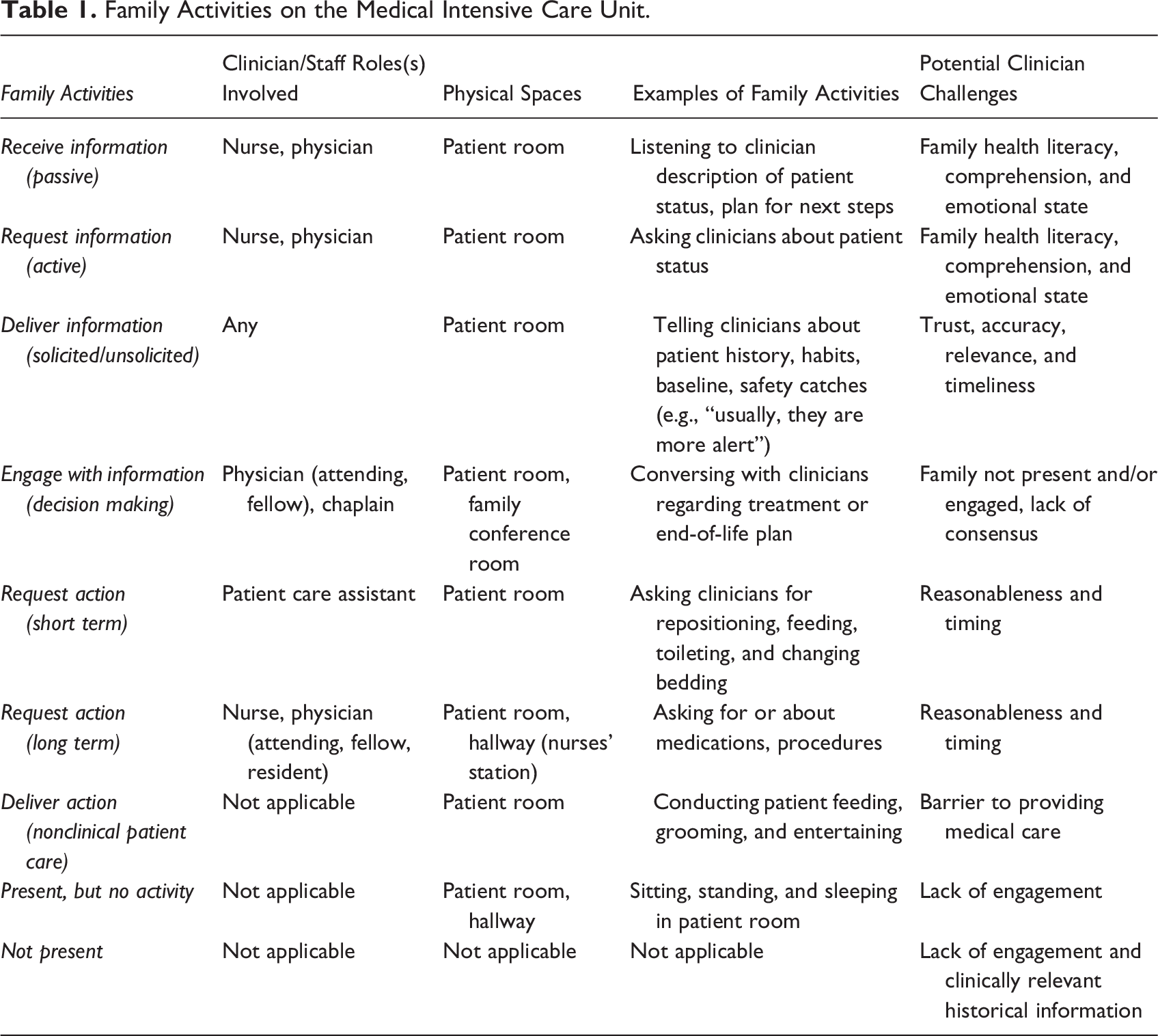
In addition to passive presence, we identified two categories of observable behaviors or activities that families engaged in: (1) information-related (via engaging with clinicians and staff) and (2) nonclinical patient care. Further, we broke down the information-related category into receive, request, deliver, and engage with. Examples of receiving and/or requesting information included topics such as patient status, treatment plan on the short- and long-term, and end-of-life planning—for example, weaning off the ventilator. Examples of delivering information included family members sharing of patient status (e.g., level of alertness) before they came to the MICU. Examples of engaging included information exchanges with clinicians for the purposes of family decision making. We broke down the nonclinical patient care category into deliver and request and on a short- versus long term. Examples of requests included bedding changes or medications and delivery included feeding, grooming, and comforting. Informed by these observational data, we developed a framework of activities in Table 1 which includes examples, clinicians, and potential challenges.
Family Activities on the Medical Intensive Care Unit.
Discussion
There are several limitations in the current study including the observations taking place on a single unit at one institution and over a period of 18 months. However, this institution primarily serves lower socioeconomic status, inner-city populations impacted by health disparities that are in urgent need of research and operational attention. Also, given our inability to enter patient rooms, we were limited in our observations. Finally, data collection in this study took place prior to the COVID-19 pandemic that impacted visitation policies that continue to be variable and dynamic across and within healthcare systems.
Presence and engagement of families during a hospital stay plays a role in patient outcomes (Gwaza & Msiska, 2022). In the current study, we characterized the (1) types of observable activities and information exchanges that families in the ICU engage in (what), (2) along with the physical spaces in which they take place (where), and (3) and clinician/staff roles (with whom). This characterization is novel because much literature of family engagement in critical care is focused on emotional work and information support (provision of information to patients and families regarding patient status). Further, this description is critical in highlighting that families in the ICU conduct behavioral and cognitive activities in complex situations—interacting with multiple clinician and staff teams and individuals carrying out formal and informal activities and processes, within physical settings that are unfamiliar, noisy, and dynamic. Human factors scientists have historically focused on considering and capturing the impact of system complexity on professional (e.g., clinicians, soldiers, nuclear power plant operators) performance (Carayon et al., 2014). However, there continues to be lacking literature in characterizing family activities (beyond emotional) in critical care settings from a human factors perspective. This is necessary to inform and appropriately tailor solutions, tools, or interventions. It is fitting to apply the same sociotechnical lens (as to professionals) when examining the work of families as they engage in information seeking and delivery and provision of nonclinical patient care within complex clinical settings.
Recommendations
Historically, considerations for families in ICUs have been of an emotional nature (through intervention of a chaplain or social worker). However, family support needs to go beyond emotional to include creating proactive (rather than reactive) information flow between families and clinicians (with effort to not further exacerbate clinician workload). Such support has the potential to contribute to progress in family–clinician teaming in adult care.
Despite the existence of much patient- and family-facing educational materials on clinician and staff roles and responsibilities (Society of Critical Care Medicine, n.d.), knowing “who is who” is only part of the big picture. Given that families deliver potentially relevant clinical information, engage in decision making, and conduct patient care activities, there is a continued need to gain a deeper understanding of family roles in the ICU. Informed by this understanding, researchers can identify family needs and requirements for education, training, and decision support tools. Suggested recommendations include family education regarding roles and responsibilities of clinicians and staff regarding information and workflow, preexisting (and formal) opportunities and channels to engage with clinicians (e.g., family-centered rounds) while mitigating avoidable disruption, and effective ways of being present and active. Implications may even reduce workload for clinicians and burden for families by preventing the following situations: (1) seeking interactions with clinicians across time and physical spaces that lack necessity or urgency (e.g., searching for an attending physician to ask questions or voice concerns); (2) providing or requesting redundant information across clinicians such as residents, fellows, and attending physicians; and (3) making requests of clinicians and staff that are not consistent with their roles/responsibilities (e.g., asking the PCA or a nurse for suction, rather than the respiratory therapist, asking a nurse to change the sheets). Aside from frustration for all, such requests may fail to be handed off to the relevant party, resulting in further communication challenges and delays.
Conclusion
There is a limited understanding of the behavioral and cognitive work of family members in critical care, with many research questions to be asked. We proposed a framework of their observable activities informed by using qualitative methods. Findings can serve as a guide for future research and inform development of support solutions.
Implications for Practice
The way that physical spaces are used by individuals in different roles can contribute to uncertainty and create barriers to information flow.
In addition to passive presence, we identified two categories of observable behaviors or activities that families engaged in, including information-related (via engaging with clinicians and staff) and nonclinical patient care.
Inherent to families navigating processes and interactions with multiple clinicians and staff in the ICU that is noisy, and dynamic is the cognitive and behavioral work of managing complexity.
There is a gap in sufficient understanding by families of clinician decision making responsibilities and processes. This gap may not just contribute to frustration by all parties but increase clinician workload and potentially impede clinically relevant information exchange between families and clinicians.
Footnotes
Acknowledgments
We are tremendously grateful to the Medical Intensive Care Unit (MICU) at our institution and to Gail C. Tagney for being our champion and supporting access to the unit.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UIC Honors College Research Grant (2019) and UIC Honors College Travel Grant (2019).