
Abstract
Background:
The intensive care environment in hospitals has been the subject of significant empirical and qualitative research in the 2005–2020 period. Particular attention has been devoted to the role of infection control, family engagement, staff performance, and the built environment ramifications of the recent COVID-19 global pandemic. A comprehensive review of this literature is reported summarizing recent advancements in this rapidly expanding body of knowledge.
Purpose and Aim:
This comprehensive review conceptually structures the recent medical intensive care literature to provide conceptual clarity and identify current priorities and future evidence-based research and design priorities.
Method and Result:
Each source reviewed was classified as one of the five types—opinion pieces/essays, cross-sectional empirical investigations, nonrandomized comparative investigations, randomized studies, and policy review essays—and into nine content categories: nature engagement and outdoor views; family accommodations; intensive care unit (ICU), neonatal ICU, and pediatric ICU spatial configuration and amenity; noise considerations; artificial and natural lighting; patient safety and infection control; portable critical care field hospitals and disaster mitigation facilities including COVID-19; ecological sustainability; and recent planning and design trends and prognostications.
Conclusions:
Among the findings embodied in the 135 literature sources reviewed, single-bed ICU rooms have increasingly become the norm; family engagement in the ICU experience has increased; acknowledgment of the therapeutic role of staff amenities; exposure to nature, view, and natural daylight has increased; the importance of ecological sustainability; and pandemic concerns have increased significantly in the wake of the coronavirus pandemic. Discussion of the results of this comprehensive review includes topics noticeably overlooked or underinvestigated in the 2005–2020 period and priorities for future research.
Keywords
Environmental design research has evolved significantly over the past 50 years to be recognized as a distinct discipline centered on the transactional relationship between the built environment, design excellence, and the improvement of the human condition. In the past 25 years, a subdiscipline of evidence-based research and design has focused on health and the built environment. This research is recognized as a distinct knowledge base addressing the spectrum of healthcare building types including hospitals, hospices, long-term care facilities, pediatric facilities, psychiatric and substance abuse treatment centers, and community-based outpatient clinics (Verderber, 2010). Correspondingly, the published literature has become increasingly complex and multifaceted, including the role of the built environment in infection control and the prevention of adverse medical events, furthered by the 2003 Institute of Medicine report Crossing the Quality Chasm (Zimring et al., 2013). As a consequence, it has become necessary to take stock of recent literature on the topic of the intensive care built environment. In the medical literature, the number and location of beds housed in intensive care units (ICUs) in hospitals have greatly expanded in the past decade (Wallace et al., 2017). A review of recent peer-reviewed quantitative and qualitative investigations and theoretical essays on critical care built environments can yield insight—particularly now—as the world endeavors to control and eradicate the virulent COVID-19 pandemic. This pandemic fueled an acceleration of new medical knowledge but has yet to fully impact the realm of architecture. The generation of new knowledge on the ICU built environment can aid direct caregivers, patients, and families worldwide. This review of hospital ICUs, including neonatal ICUs (NICU) and pediatric ICUs (PICU), is focused on person–environment transactions. These settings are conceptualized here as constituting a typology, a prism of sorts, to achieve an overview of current best practices and theoretical perspectives vis-à-vis a comprehensive literature review. This systematic review consists of peer-reviewed research investigations, pertinent recent theoretical essays, and prognostications for the future.
This review directly builds upon a comprehensive literature survey on evidence-based healthcare design and the built environment published 13 years ago (R. L. Ulrich et al., 2008). In it, nearly 450 peer-reviewed research publications were summarized. It addressed patient safety issues, patient–staff outcomes, and insights on the interventional role of the physical environment. Health status outcomes reviewed included nosocomial infections, medical errors, pain, sleep, stress, patient satisfaction, length of stay, privacy, communication, social supports, workplace injuries, staff stress, and satisfaction. Built environment interventions included single-bed rooms, access to daylight and appropriate lighting, views of nature, dedicated family zones within the patient room, noise reduction, workspace attributes, and acuity-adaptable patient rooms. ICUs were but one of many in-hospital units, freestanding building types, and user constituencies addressed. Since its publication, advances in critical care medicine, ecological sustainability, therapeutic benefits of person–nature connectivity, and best practices with respect to the COVID-19 global pandemic underscore the need for a comprehensive up-to-date review. The primary aim of the present review is to assess the current state of the art and science to better inform design choices to reduce adverse medical events, improve infection control and patient safety, better engage patients and families, examine person–nature interactions, and identify policies to improve caregiver work performance, satisfaction, and well-being.
Method
The methodology consisted of a broad review of published, peer-reviewed quantitative and qualitative investigations and essays. The first step consisted of a key word search to identify potentially relevant peer-reviewed publications. Forty key words were used, referring to patient and staff outcomes, that is, infection control, disease control, medical error, pain, sleep deprivation, respiratory disease, stress, privacy, and COVID-19. Second, referring to physical environment factors, that is, hospital; therapeutic gardens; COVID-19 field hospital; ICU design and layout; ICU unit layout; nursing station design; critical care medicine; critical care nursing; pulmonary medicine; ICU, NICU, and PICU design and features; acuity adaptability; and healthcare facilities. Third, referring to related issues, that is, staff productivity, stress, family-centered care, noise mitigation, nature, views, landscape, nature representations, patient safety, the future of the ICU, theoretical prognostications, telemedicine, and ICU planning and design. Fourth, referring to healthcare facility infrastructure, that is, carbon neutral hospitals, sustainable design and operations, nontoxic materials, and hospital renovation and retrofitting. Extensive cross-searches were then conducted using combinations of key words and phrases through the JSTOR and Google Scholar databases and further searches combing multiple databases including EBSCO, ScienceDirect, PsychINFO, MEDLINE, Ovid, ProQuest, PubMed, Web of Science, Science Digest, and NIH Public Access. This search included any study or article that alluded or referred to the healthcare physical built environment in its title or abstract, published between January 2005 and February 2021. The decision was made at the outset to include both empirical and qualitative research investigations, as well as relevant theoretical and opinion essays, in order to broadly capture the scope, depth, and nuance of a rapidly evolving subject.
The initial search phase yielded 219 primary sources, subsequently reduced in the second-stage assessment to 147 peer-reviewed sources. These met or exceeded the team’s benchmark for rigor. In the third-stage assessment, these sources were further examined and reduced to a compendium of 135 sources (reported below). The research team carefully screened three types of sources: (1) empirically based studies that examine the role and impact of the built environment or natural environment on patient, staff, and/or family outcomes; (2) qualitative studies that examine these same relationships; and (3) theoretical essays that examine the relationship between intensive and critical care medicine, nursing best practices, pulmonary medicine, COVID-19, and the general planning and design of medical ICU built environments. Non-peer-reviewed white papers, research reports, minimum standards guidelines publications, and books on this subject were eliminated in the first wave of the screening process.
The final compendium was then structured into nine content categories deemed by the research team to best capture the current state of the art and science. The 2005–2020 period witnessed numerous innovations including acuity adaptability, debates between patient/family privacy versus semiprivacy in the ICU patient room, telemedicine, acknowledgment of the therapeutic affordances of nature and landscape in the hospital setting, participatory planning and design tools to meaningfully elicit ICU design input from caregiver stakeholders, and ICU built environment impacts of the global COVID-19 pandemic that originated in China in late 2019.
Results
Table 1 contains the compendium of 135 research investigations, critical essays, and policy reviews presented in nine content categories: nature engagement and outdoor views—studies examining the influence of exposure to nature as well as representations of nature in critical care hospital inpatient units, with specific focus on measure of stress and stress reduction outcomes; family accommodations in the ICU environment—studies on the role of family involvement in the ICU experience and the influence of family input in ICU design and amenities provided; ICU spatial configuration and amenity—factors impacting the physical layout and associated amenities, associated staff affordances, and proxemic relationships, that is, travel distances, staff–patient sight lines, single versus semiprivate rooms; noise considerations in ICU environments—deleterious effects of excessive noise and involuntary distractions on patient and staff well-being, patient delirium, and the influence of noise mitigation measures on patient outcomes; artificial and natural lighting in ICU environments—adverse effects of excessive light on occupant well-being, the benefits of informative views, the utility of ventilation systems, and optimal ambient light levels on patient outcomes; ICU patient safety and infection control—studies addressing the types and prevalence of adverse medical events in critical care settings and measures to mitigate their occurrence and improve patient outcomes; portable field hospitals and disaster mitigation including COVID-19—the role, efficacy, and assessment of portable, critical care field hospitals for deployment in the aftermath of natural disasters and pandemics with specific focus on the global COVID-19 pandemic; ICU ecological sustainability—recent advancements in energy efficiency, sustainable materials of construction, and resilient facility design and operation with direct applicability to critical care hospital units; and recent design trends and prognostications—essays on the present and future of critical care settings in hospitals, including therapeutic design affordances, and performance-based trends, that is, new technologies, acuity adaptability, and the ICU of the future.
Table 1 summarizes this knowledge compendium vis-à-vis the nine content categories with key background information and findings summarized. This consists of the author(s), date of publication, topic and scope of the study/essay, conceptualization of the built environment and the principal study setting, research design and sample (as applicable), outcome measures of well-being, physical environment features, and key findings of the investigation/discussion. As mentioned, only peer-reviewed publications are included. These empirical investigations and qualitative studies and essays emphasize day-to-day operations and the experience of frontline caregivers, patients, and family members. Early on, it was decided to not categorize NICU or PICU settings separately since many issues addressed in these settings were of equal relevance to the entirety of the built environment typology as defined above.
Summary of ICU Built Environment Comprehensive Literature Review—Content Areas 1–9.

Note. ICU = intensive care unit; NICU = neonatal ICU; PICU = pediatric ICU; MRSA = methicillin-resistant Staphylococcus aureus.
Nature Engagement and Outdoor Views
Wilson’s biophilia hypothesis suggests that humans possess an “innate tendency to focus on life and life-like processes” and is often cited as a key consideration for using natural elements in the healthcare setting (Grinde & Patil, 2009; Minton & Batten, 2015). Despite U.S. Centers for Disease Control and Prevention guidelines suggesting that restriction of plants/flowers in hospital settings be limited to immunocompromised patients, live plants are often uniformly prohibited in ICUs (Sehulster et al., 2004). Eight studies were identified describing the integration of nature elements in an ICU or ancillary settings (waiting rooms and shared outdoor gardens) and patient (n = 4), staff (n = 3), and family (n = 1) outcomes. Interventions primarily focused on the use of live plants, access to outdoor therapy gardens, and exposure to outdoor nature views (Table 1).
Plants and Gardens
Plants and gardens are often employed in hospitals to facilitate nature engagement within the healthcare environment. Patients exposed to either plants or images of plants in hospital waiting rooms report greater stress reduction as compared to controls (Beukeboom et al., 2012). Similarly, subjects presented with photos of hospital rooms containing plants report less stress compared to those shown photos of rooms without plants (Tanja-Dijkstra et al., 2008). Visiting an outdoor garden can reduce sadness and stress scores in families of hospitalized patients (R. S. Ulrich et al., 2020). Nursing staff have reported less burnout, feelings of depersonalization, and emotional exhaustion after taking breaks in outdoor gardens (Cordoza et al., 2018). These studies demonstrate that live plants and hospital gardens are likely of therapeutic benefit to patients, staff, and families.
Nature Views
Windows and nature views are interventions to promote positive distraction and stress reduction in the ICU. Surgical ICU patients admitted to rooms with nature views experience a slightly shorter ICU length of stay compared to those in rooms with views containing industrial informational content, although notably, there is no difference in hospital and ICU mortality, ICU readmission rate, or delirium occurrences (Kohn et al., 2013). Similarly, patients with acute brain injury admitted to windowed ICU patient rooms demonstrate no difference in functional status, ICU–hospital length of stay, or mortality compared to those admitted to windowless rooms (Wunsch et al., 2011). The effect of nature views in the intensive care environment on hospital staff has also been examined. A single-center study evaluating outcomes after moving to a new ICU with more windows and nature views showed a statistically significant decrease in staff absenteeism and employment vacancy rates (Shepley et al., 2012). Pati and colleagues (2008) also evaluated exterior nature views experienced by nursing staff, reporting improved alertness levels and a decrease in stress. These studies suggest that while nature-content views per se are not associated with traditional ICU patient outcomes measures, they likely contribute to an improved work environment for healthcare providers.
Family Accommodations in the ICU Environment
Familial presence within the ICU environment is increasingly recognized as a vital component of the care of critically ill patients. In a qualitative study examining the experiences of families of children hospitalized in a PICU, MacDonald and colleagues (2012) described a frequent disconnect between family-centered medicine and the modern medical practice of intensive care. They described this conceptually as a conflict between the need for the ICU room to serve as the sick child’s “bedroom” as well as a workplace for healthcare professionals, and noise, privacy policies, and visitation restrictions may affect families and healthcare providers in opposite ways. The principle of a “healing environment of care” can be utilized to facilitate the engagement of families in the ICU by both promoting a therapeutic relationship between patients, caregivers, and families as well as highlighting environmental design strategies to support healing (Rashid, 2010). Guidelines for family support in the ICU environment have suggested that single rooms should be utilized to improve patient privacy and should include dedicated family space (Davidson et al., 2007). It has also been suggested that graphics and wayfinding systems be implemented and waiting rooms be placed close in proximity to patient rooms (Davidson et al., 2007). Updated guidelines have reinforced the importance of providing single-bed rooms and noise reduction strategies as well as sleep surfaces for families as environmental design interventions to facilitate family integration and suggest a checklist to assess ICU readiness for family-centered care (Davidson et al., 2017). However, the authors also acknowledge the paucity of research on how the physical setting can optimally improve family engagement in the ICU. Review of the recent literature revealed 12 studies describing various environmental design interventions in support although there have been no randomized trials, to date. These measures have focused on improving family and patient privacy, including designation of “family” corridors adjacent to or within the ICU (Table 1).
Dedicated Family Spaces
Dedicated family space at bedside is associated with an increased proportion of visitors at night (Hunyh et al., 2020). Family-initiated conversations with healthcare providers are higher in ICUs that utilize a shared provider–family hallway space as opposed to units with separate hallways for healthcare staff and families (Rippin et al., 2015). Critical care units that employ noise-reduced, single-bed patient rooms that incorporate daylight and dedicated washroom facilities for families have been associated with higher family satisfaction scores (Jongerden et al., 2013). For families of patients admitted to a neurotrauma ICU, physical environment attributes that correlated with family satisfaction included noise level, size of the waiting room, private spaces, and washroom facilities (Peterson et al., 2020). Structured interviews with nurses of dying patients in the ICU have highlighted that families commonly desire spaces allowing both privacy and togetherness and connection with other family members (Fridh et al., 2009). In a multisite family satisfaction survey evaluating family sleep location, the caregivers of children admitted to PICUs were most likely to report sleeping in the child’s room, followed by their own home and then a shared family accommodation program (Franck et al., 2015). However, other studies demonstrate a substantial proportion of family members reporting sleep disturbance and poor sleep quality in ICU waiting rooms, suggesting that hospital accommodations are inadequate for quality sleep (Day et al., 2013; Stremler et al., 2014). These studies suggest that design interventions such as single-bed rooms, dedicated family space, family sleep accommodations, and common areas for interaction with staff may help improve family engagement at bedside in support of the critically ill.
ICU Spatial Configuration and Amenity
Despite extensive research regarding ICU configuration and ergonomics, performance obstacles related to the physical environment continue to be frequently identified by nurses, such as room disorganization, noisy and crowded workspaces, and insufficient areas dedicated to medical documentation (Gurses & Carayon, 2009). The review team found 22 articles, with 10 nonrandomized comparative studies, nine cross-sectional studies, two opinion essays, and one systematic review. Interventions have focused on single versus multibed room modules, nursing station typology, visibility patterns in the ICU, and workplace performance obstacles (Table 1).
Nurse Station Design and ICU Layout
In a review of adult ICU design in the United States, Catrambone and colleagues (2009) identified four predominant unit configurations, with a “U-shaped design” being most common, followed by “spokes/no end station,” “parallel corridor,” and “surrounded” configuration. Spatial configurations are often classified as centralized, decentralized, and hybrid based upon nursing station type. Unit layout affects interactions and communication patterns between healthcare providers, with a reported lower frequency of physician–nurse communications and social interactions in decentralized ICUs (Zborowsky & Hellmich, 2011). Layout design, visibility patterns, and accessibility were identified in a systematic review of healthcare physical design attributes that impact teamwork and communication (Gharaveis et al., 2018). In consideration of the general hospital built environment, decentralized nursing stations have been associated with improved documentation practices, less steps taken, decreased energy expenditure by healthcare providers, and better utilization of medication and supply rooms; however, they have also been associated with a decrease in nurse-to-nurse collaborations and teamwork (Copeland & Chambers, 2017; Pati et al., 2015; Real et al., 2016). In a systematic review evaluating decentralized nursing station design, there was a notable decline in nursing teamwork in the decentralized models (Fay et al., 2019), highlighting systems-level challenges posed by the introduction of the decentralized unit (Real et al., 2016). In a theoretical essay, Hamilton and colleagues (2018) indicated that concerns regarding travel distance and visibility challenges in the decentralized unit may be related to corridor design and overall size of the ICU. Systematic field observations have also demonstrated an association between spatial design and healthcare worker interaction–related behaviors in adult ICUs (Rashid et al., 2014). In this study, interactions that occurred while sitting tended to occur in areas that facilitated environmental awareness and visibility.
As a method to better understand the complex interaction between ICU spatial configuration, healthcare provider interactions, and communication patterns, Cai and colleagues proposed a system of spatial measures to better evaluate nursing station typology (Cai & Zimring, 2012). In this approach, integration, team distance, and peer distance were utilized as spatial metrics to understand unit layouts, demonstrating a strong correlation with nurses’ physical location, awareness of colleagues, and interactions with other providers. This suggests it may be useful to consider team distance and peer distance in addition to patient visibility patterns when evaluating nursing station and ICU spatial configuration.
Visibility remains an important component of ICU design with implications for both healthcare provider workflow and patient outcomes. Physicians and nurses often differ in preferred workflow locations, with nurses proportionally favoring areas with higher targeted visibility toward patient beds and physicians favoring areas with generic visual connectivity and large open spaces (Lu & Zimring, 2011). In a single-center study evaluating the PICU environment, O’Hara and colleagues (2018) concluded that maximization of visibility through the design of corner work zones can enhance team interactions and patient observation, creating opportunities for macrocognition and cognitive adaptation to complex situations. For severely ill patients admitted to the ICU, one study found a significantly higher hospital mortality rate in patients admitted to rooms with low visibility from the central nursing station (Leaf et al., 2010). Lu and colleagues (2014) further evaluated visibility patterns and demonstrated that both the field of view of the patient’s head and the room’s distance from the nursing station accounted for differences in mortality. Patient visibility can also be improved through the design of wider corridors; fewer small, convex spaces; and shorter travel distances (Hadi & Zimring, 2016).
Single and Multibed Rooms in Intensive Care
The adoption of the all single-bed ICU unit has provided an opportunity to evaluate corresponding patient, staff, and family outcomes. Numerous studies have reported higher family satisfaction scores in single-bed ICU rooms as compared to multibed rooms and often cite enhanced privacy as a key driver of this association (Apple, 2014; de Matos et al., 2020; Stevens et al., 2012). Hospital staff have also reported improved quality of the work environment and enhanced patient safety in single-bed rooms (Bosch et al., 2012; Stevens et al., 2012). Conversely, single-bed rooms have been associated with higher staff stress (de Matos et al., 2020), increased travel distances, steps per nursing shift (Stevens et al., 2012), and feelings of staff isolation and difficulty with obtaining assistance from colleagues (Apple, 2014). Hybrid room designs consisting of two single-patient rooms connected by a shared space for documentation and monitoring have been proposed as a solution to the competing interests between single and multibed rooms. Hospital staff working in hybrid ICU room configurations report efficient patient observation, enhanced collaboration between healthcare workers, and improved patient privacy as compared to multibed rooms (Apple, 2014).
The prevention of ICU-associated delirium has gained increased focus due to its association with length of stay, patient morbidity, and mortality, with room configuration emerging as a modifiable environmental risk factor. Adult patients admitted to multibed ICU rooms are four times more likely to develop delirium compared to those admitted to single-patient rooms (Caruso et al., 2014). Age also appears to be an important factor in understanding the relationship between ICU room configuration and delirium. Arenson and colleagues showed that there was no difference in delirium prevalence between single- and multibed rooms for those greater than 65 years of age; however, patients less than 65 years of age demonstrated a greater proportion of delirium days when admitted to multibed ICU rooms compared to single-bed rooms (Arenson et al., 2013).
Noise Considerations in ICU Environments
Various organizations have proposed noise-level guidelines for the hospital setting. The World Health Organization has recommended hospital noise levels not exceed 35 decibels during the day and 30 decibels at night, with nighttime noise peaks less than 40 decibels (Berglund et al., 1999). The American Academy of Pediatrics (1997) has recommended noise levels not exceed 45 decibels in the NICU setting. There have been 15 recent studies published regarding noise levels in the ICU environments (n = 5 NICU, n = 4 PICU, n = 6 adult ICU). Published studies focus on the themes of measured ambient noise in the ICU versus common noise sources, the effect of ambient noise on patients and staff, and design-based mitigation strategies (Table 1).
Noise Levels and Stress
Measured ambient noise often exceeds recommended levels in adult ICUs (Christensen, 2007; Macedo et al., 2009; Ryherd et al., 2008), PICUs (Carvalho et al., 2005; Kawai et al., 2019), and NICUs (H. L. Chen et al., 2009; Lasky & Williams, 2009), with average noise levels ranging from 48 to 70 decibels and maximum levels ranging from 67 to 120 decibels. Temporal studies of ambient noise demonstrate higher levels during morning shifts compared to evening/night shifts (Carvalho et al., 2005; Kawai et al., 2019; Matook et al., 2010) and during weekdays, compared to weekends (Christensen, 2007). Noise levels also increase over time in the NICU setting and appear to be attributable to age-related changes in bed type and respiratory support equipment needs (Lasky & Williams, 2009). Common sources of ambient noise include equipment such as monitors and alarms, hospital staff conversations at nurses stations, and handovers between ICU and operating room teams at bedside (Carvalho et al., 2005). Careful consideration of noise pollution must occur when introducing new equipment and technologies, as evidenced by a report describing a marked increase in noise levels after the addition of motion-sensing motorized paper towel dispensers and a new audio communication system (Brandon, et al., 2007). Postdischarge surveys demonstrate that patients often recall various ICU noises and sounds (Johansson et al., 2012). Healthcare workers in the ICU environment also report that elevated noise levels contribute to feelings of fatigue, difficulty concentrating, and tension headaches (Ryherd et al., 2008).
Design Interventions to Decrease Noise
Multiple environmental interventions have been evaluated as potential modifiers of ambient noise. Some studies have reported that single-bed ICU rooms have lower sound levels compared to multibed rooms (H. L. Chen et al., 2009; Kol et al., 2015), although others have shown no difference (Kramer et al., 2016). Wang and colleagues (2013) reported a decrease in average and maximum noise levels in patient care areas after the addition of a dedicated service corridor. Architectural features such as soundproof headwalls to separate patients from medical equipment and an anteroom between the patient room and corridor result in reduced average and maximum sound levels in ICU rooms (Leutz et al., 2016). A multiphase quality improvement initiative in a NICU demonstrated that lowering equipment alarm sounds was associated with an overall reduction in noise levels (Chawla et al., 2017).
Artificial and Natural Lighting in ICU Environments
Hospital building codes emphasize that lighting should be tailored to facilitate the diverse needs of healthcare staff, with a recommended level of 30 lux for circulation areas, 300 lux for observation and medical documentation areas, and between 3,000 and 10,000 lux in critical examination and procedural areas (Shepley et al., 2012). The American Academy of Pediatrics (2002) has recommended a maximum light level of 646 lux in NICU environments. Measured light levels in the ICU often fall within guideline recommendations (Lasky & Williams, 2009). A total of 10 recently published studies on lighting in the ICU were identified (n = 5 NICU, n = 5 adult ICU), focusing on ambient lighting levels, light sources, light-mitigating interventions, and patient outcomes (Table 1).
Light Interventions in the ICU Environment
Light source and level of illumination are frequently identified as modifiable variables. Infants exposed to lower minimum and maximum illumination levels in the NICU experience less periodic breathing and awake time (Stevens et al., 2007). An NICU-cycled light strategy throughout the day versus continuous bright light, or near darkness, resulted in shortened hospital length of stay in premature neonates (Morag & Ohlsson, 2015). Subtle variations in ambient light levels have also been associated with increased awakening in premature neonates, suggesting that design interventions to modify abrupt changes in lighting may affect NICU outcomes (Zores et al., 2018). In a systematic review, it was concluded that changes in light level should be gradual, light mitigation protection should be used for infants less than 32 weeks corrected gestational age, and premature infants should not be exposed continuously to high light levels (Zores-Koenig et al., 2020).
Light exposure has been studied as a modifiable intervention. Rompaey and colleagues (2009) evaluated ICU environmental risk factors and demonstrated a lack of natural light as a risk factor for delirium. The technique of dynamic light therapy involves periodic variation of ambient light levels in indoor environments and has been suggested as an intervention to decrease the incidence of ICU delirium. However, a recent randomized control trial evaluating the effect of dynamic light application on the incidence of delirium was concluded early due to futility and lack of improved outcomes (Simons et al., 2016). Adult ICU patients admitted to rooms with natural daylight experience slightly shorter length of stays compared to those with primarily artificial light sources, although notably, there appears to be no difference in hospital and ICU mortality, ICU readmission rate, delirium, sedative use, and analgesic requirement (Kohn et al., 2013; Verceles et al., 2013). Together, these data suggest further research is needed to better understand targeted patient populations and outcomes in the use of light as a therapeutic modality.
ICU Patient Safety and Infection Control
Hospital built environments have been modified to decrease medical errors and improve patient safety and infection control. Design interventions employed include minimizing ambient noise, judicious use of lighting to facilitate task completion, and single-bed patient rooms. The review team identified 11 studies evaluating these types of environmental design interventions (Table 1).
ICU Environment Infection Control Measures
Single-bed ICU rooms have been investigated as a design intervention to decrease nosocomial infections. In a single-site study, Levin and colleagues (2011) demonstrated that adult patients admitted to a single-bed room acquired fewer antibiotic-resistant infections during their stay. Bracco et al. (2007) demonstrated that patients admitted to single-bed rooms had lower relative risk of acquisition of methicillin-resistant Staphylococcus aureus (MRSA), Pseudomonas aeruginosa, and Candida spp. compared to those in multibed rooms. Bloemendaal and colleagues (2009) also reported less acquisition of MRSA in single-bed rooms. Similarly, Teltsch and colleagues (2011) demonstrated that conversion from multibed to single-bed ICU rooms was associated with a lower nosocomial infection rate compared to a control multibed unit. However, moving adult ICU patients with documented MRSA to isolation rooms or cohorted multibed rooms does not significantly reduce cross-infection rates (Cepeda et al., 2005). Stiller and colleagues collected data on structural design elements in German ICUs to examine hospital architecture in the context of nosocomial infection occurrences. The findings demonstrated only minor associations between architectural design factors and ICU-based infection, suggesting that design features were subordinate to more primary drivers of infection control (Stiller et al., 2017). Additional design interventions, such as the introduction of a whole-room atomization system for use in conjunction with standard cleaning practices, have been demonstrated to decrease bacterial counts in vitro (Reynolds et al., 2020).
Adverse Outcomes and Patient Safety
Healthcare environmental design has been utilized to promote patient safety. Lighting, nature and nature representations, and virtual reality (VR) interventions have correlated with improved pain management (Malenbaum et al., 2008). For severely ill patients admitted to the ICU, a significantly higher mortality rate occurred for those admitted to rooms with low visibility from the central nursing station compared to rooms with higher visibility (Leaf et al., 2010). However, admission to a room with high visibility was not associated with an improved outcome for trauma patients (Pettit et al., 2014), indicating that visibility is but one factor in understanding the complexities of ICU patient safety. New frameworks to facilitate incorporating human factors and ergonomic principles into systems engineering models for improved patient safety often incorporate elements of the physical environment (Carayon et al., 2020), thus underscoring the need for continued research to better understand this dimension of ICU hospitalization.
Portable Field Hospitals and Disaster Mitigation Including COVID-19
The rapid proliferation of the deadly coronavirus in 2020 prompted healthcare provider organizations globally to confront a major public health crisis and reassess their in-house facility infrastructure (Auerbach et al., 2020; S. Chen et al., 2020; Z. Chen et al., 2020; Keenan, 2020). COVID-19 precipitated innovative responses in ICU built environments, and in telemedicine, in particular. Wosik et al. (2020) examined telemedicine applications in numerous hospitals in the context of the pandemic, specifically, ICU patient respiratory functions, and space requirements for ventilator equipment (Doshi et al., 2020). Fortis et al. (2014) demonstrated that telemedicine, effectively implemented, can reduce healthcare costs while improving patient outcomes, enabling patients to be cared for vis-à-vis virtual bedside consultation (Table 1).
Rapid Responsiveness
In France, direct care provider involvement is urged from the earliest facility planning stages to operationalization and staffing (des Déserts et al., 2020). In Wuhan, China, two 10,000-bed Fangcang shelter hospitals were constructed in March 2020 (S. Chen et al., 2020; Z. Chen et al., 2020; Owens et al., 2005); building information modeling (BIM) technology and modular composite building finished products were utilized to design and construct the modular Wuhan Leishenshan Hospital in 2 weeks. All interior floors, exterior walls, and heating, ventilation, and air-conditioning (HVAC) systems were designed using BIM (L. Chen et al., 2021). Best practices in biocontainment unit facility planning and design have been developed (Flinn et al., 2020; Lenaghan & Schwedhelm, 2015). These facilities are reliant on preexisting technological infrastructure, that is, site utilities, access to transport routes to maintain supply chain continuity, telecommunications support, and availability of installation sites ranging from community centers to sports stadiums and to open fields (Fang et al., 2020). Field hospital installations must be quickly constructible, cost-effective, and reduce capacity pressures on nearby conventional medical facilities (Keenan, 2020; Louri et al., 2020; Pucher et al., 2014; Zhou et al., 2020). The Fangcang shelter hospitals had the advantage of constructability on immediately available land parcels. As noted by both Kreiss et al. (2010) and Burnweit & Stylianos (2011), traditional medical technologies must be adaptable to emergency field hospital environments, specifically, negative air filtration HVAC system design (Santos et al., 2020). Ten strategies were recently outlined to guide the design and operations of resilient hospital environments (Capolongo et al., 2020). During the COVID-19 pandemic, a regional hospital in Italy was repurposed for cardiovascular emergencies. This new role required an increase in ICU bed capacity and support spaces (Zangrillo et al., 2020). In the United States, the MED-1 mobile vehicular field hospital, first deployed in the aftermath of Hurricane Katrina in New Orleans in 2005, has proven adaptable in diverse site installation contexts (Blackwell & Bosse, 2007; Burnweit & Stylianos, 2011) Vehicular-based and modular surge field hospitals must house advanced equipment allowing for rapid reconfiguration in the field as needs evolve (Lee et al., 2019). A recent review was conducted of nine COVID-19-inspired hospital prototypes put forth by international architectural firms. The major findings include individualized patient treatment modules, dedicated service corridors, and negative air pressurization filtration systems (Sonmez, 2020).
Intensive care must be adaptable to on-site determinants in humanitarian disaster relief contexts (Blackwell & Bosse, 2007; Lee et al., 2019). Organizational effectiveness, appropriate technical support, and staff intercommunication are of paramount importance in effective facility operations (Lee et al., 2019). First response pediatric care, including NICUs, should be available in postdisaster contexts (Burnweit & Stylianos, 2011). The provision of triage assessment is of utmost priority (Kreiss et al., 2010). Cross-cultural differences between patients, caregivers, and families must be accounted for in the delivery of healthcare in unfamiliar postdisaster strike zones (Owens et al., 2005). The ethical integration of ethical, humanitarian principles in critical care emergency response contexts preserves human dignity (Lee et al., 2019).
ICU Ecological Sustainability
Sustainability and Efficiency
The day-to-day operations of hospital ICUs contribute to the depletion of the earth’s natural resources (McGain & Naylor, 2014). The Green Guide for Health Care program articulated planning and architectural design criteria for sustainable best practices in hospital design, construction, operation, and maintenance (Marshall-Baker, 2006). Ecologically based energy efficiency is increasingly a baseline minimum criterion essential to achieving longer term facility operational efficiency. An ICU’s physical layout impacts energy consumption; single-bed rooms in hospitals have been linked with reduced infection rates but can contribute to higher overall energy consumption levels (Huffling & Schenk, 2014). Trades-offs are necessary to balance higher initial construction costs with reduced recurring, life-cycle operational expenses. Further research is needed on this issue including the impacts of floor template size, configuration, and the use of energy-star-rated equipment (McGain, 2014).
Flexible space has been demonstrated as the key in achieving ecologically efficient ICU built environments. Flexible space includes spatial buffer zones, efficient internal circulation (without sacrificing spaciousness), variable ceiling heights and configurations, phased campus design and construction, and the sensitive integration of buildings into their environmental contexts (Paterson et al., 2014). ICUs can benefit in this regard from multifunctionality, that is, acuity-adaptable patient rooms, equipment, and interior amenities. Ecological efficiency in ICUs is attainable by means of standardization and modularity without compromising flexibility and adaptability (Abo & Nour, 2017). Ecological design variables include the structural system, cladding type, window/wall system, window-to-wall area ratio, number of treatment bays, and bay width (Valentin, A., & Ferdinande, P, 2011). Innovative geometries have been studied in the design of ecologically efficient specialized care units. Recent origami-inspired critical care structures with thermally insulated rigid walls include the Level Shelter Module, a system featuring polymorphic shape optimization in the attainment of life-cycle energy efficiencies (Quaglia et al., 2014).
Reduction of Carbon Emissions and Biohazardous Waste
ICU environments require highly energy-intensive equipment that produces significant toxins and as such can pose a threat to the well-being of building occupants (Huffling & Schenk, 2014). McGain et al. (2014) selectively studied hospital occupants’ energy consumption patterns: water consumption, materials procurement, toxic waste generation, and closely related in-unit behaviors. Larger scale systems including cogeneration, solar thermal, and ground-sourced heat pumps have also been studied recently. Research is needed to further understand the behaviors, attitudes, and organizational culture imperatives, that is, staff dismissiveness, within ICUs to further increase ecological sustainability quotients, with increased collaboration between key stakeholders, including clinicians, engineers, architects, and equipment specialists (McGain, 2014). Nursing staff are encouraged to advocate for energy-star-rated equipment, programmable diagnostic and monitoring equipment, and window screens blocking solar gain during the day and operable at night. ICU staff should routinely recycle–reuse equipment thereby reducing overall material consumption, participate in “green teams,” and initiate commuter carpools and community outreach programs to minimize the hospital’s ecological footprint (Huffling, 2014).
The sustainable design movement, to date, has had relatively little direct influence on hospital intensive care built environments. Finish wall, flooring, and ceiling materials are often problematic insofar as they possess substances that can emit toxins into the ambient room environment. In response, recent data suggest these finish surface materials are specified to be nontoxic, including all ceilings, waste management, water-efficient fixtures, wall and floor surfaces, and furnishings that are easily cleanable. Off-gassing of materials remains a persistent concern due to the potential deleterious impact of airborne toxins, with particular attention accorded infant incubators (Marshall-Baker, 2006; Shepley, 2016). Smart lighting systems produce full-spectrum lighting—a health-promoting alternative to conventional fluorescent fixtures, combined with natural daylighting and person–nature biophilic affordances. Standards currently exist for sustainable NICU design and construction, that is, floor plan layouts, materials of construction, and equipment and furnishings (White et al., 2013). These resources include Health Care Without Harm, Envirofacts Master Chemical Integrator, Leadership in Energy and Environmental Design, The Green Guide for Healthcare, and the sixth edition of the Recommended Standards for NICUs (Marshall-Baker, 2006).
Recent Design Trends and Prognostications
ICU–NICU Spatial Configuration (Circulation, Flow, Size, and Amenity)
A distinct shift is underway from mixed-specialty to single-specialty ICUs featuring innovative “racetrack” circulation typologies (Rashid, 2014). Such wraparound circulation pathways help to avoid bottlenecks, undue congestion, and promote wayfinding. In addition, along with efficiently configured circulation, patient room numbers should be clearly marked, with systematic directional signage. Currently, same-handed, single rooms are increasingly preferred versus larger, multibed rooms (Table 1). The rationale is patient safety, although concern persists with regard to fitting medical equipment into these reduced-in-size spaces. In addition, discrete yet layered multiple zones are advocated, consisting of patient room, family support, unit-wide support, and clinical support zones (Thompson et al., 2012). Sundberg et al. (2017) concluded that the involvement of critical care nursing staff in the design of evidence-based ICU environments has a direct impact on subsequent staff well-being and caregiving behaviors. This was found through interviews with critical care nurses combined with qualitative analysis (Sundberg et al., 2017).
NICUs are shifting toward single-family rooms (SFRs) but for slightly different reasons: to facilitate families’ greater engagement, improve infection control, and minimize exposure to adverse environmental stimuli (Denham et al., 2018). Infant maternal bonding, noise mitigation, improved staff satisfaction and morale, family zones, privacy, adequate space for routine activities on the part of staff and families alike, and staff–family communications are of high priority (Harris et al., 2006; Stevens et al., 2010). From the perspective of staff direct caregivers, excessive noise and poor illumination are persistent hindrances in ICU built environments (Stevens et al., 2010). The utilization of VR technology in the planning and design process has been demonstrated to improve the ICU experience (Ong et al., 2019). Also, the use of “meditative VR” has been shown to reduce anxiety and depression among patients, although it has not yet been linked with significantly improved sleep or pain management outcomes (Harris et al., 2006). The ability of patients and families to self-regulate lighting and temperature levels has been empirically linked with improved well-being and satisfaction (Thompson et al., 2012).
Zborowsky & Hellmich (2011) discussed the importance for healthcare design professionals to better understand the needs and preferences of patients, families, and staff and that this goal is best achievable by means of data transparency and reliance on the synthesis of qualitative as well as quantifiable health status outcomes. Nurses, ideally, can function as lead standard-bearers in this evidence-based research effort as they are most directly immersed, daily, and as such can inform design professionals in understanding patient safety and infection control measures, quality improvement, and the key support role of the built environment regarding occupant satisfaction and well-being (Zborowsky, 2011). Valentin & Ferdinande (2011) discussed an environmental assessment tool (ESICM) that seeks to capture functional criteria in construction. This tool records on an ICU room-by-room basis daily and hourly activity-occupant needs criteria and recommends feasible spatial configuration templates, equipment requirements, life safety criteria, and central hospital support interdependencies. Kesecioglu et al. (2012) examined the recent literature on ICU design in relation to patient-centered care, unit functionality, infection control, building-related life safety issues, and “futureproofing.”
Halpern et al. (2017) examined the efficacy of the Biosphere Capsule in capturing the essential aspects of an ICU through the application of VR headsets as a means to improve user participation. Hamilton (2020) discussed in detail the future of the ICU in terms of its spatial configuration, equipment, furnishings, the therapeutic function of natural daylight, and increasing role of tele-ICU and e-ICU protocols in improving the design support provided by the built environment. Using an architectural university design studio as a laboratory, Rashid (2014a), Rashid et al (2014b) examined innovative medical and building technologies, and Sessler (2014) examined the potential role of Smart ICU built environments in improving unit functionality, patient health status, and staff performance.
Acuity Adaptability
The acuity-adaptable room unit model and its manifestations in hospital intensive care have been the subject of increasing research attention. This concept can yield enhanced individualized zones for patients, families, and staff and is adaptable to ever-evolving technological innovation (K. K. Brown & Gallant, 2006). Its core variants—flex-up, flex-down, universal room, and single-stay units—in addition to the core original acuity-adaptable patient room template first introduced in the 1990s, are predicted to be more widely incorporated in ICUs in the coming years (Kwan, 2011).
Single Family Versus Semiprivate Rooms
Many NICUs in North America are being transformed from small-scale open wards to single rooms. Rybkowski et al. (2012) presented a set of facility planning principles defined as Target Value Design for application in the transition from all semiprivate (open bay) to SFR NICUs. In addition, the SFR model and its ramifications for patient, nursing, and family satisfaction with the physical setting are described as a recent evidence-based, applied strategy for renovating existing and constructing new ICUs. It is predicted that the SFR model will become more widely advocated by clients and their commissioned design teams (Stichler, 2012).
Holistic Strategies
Hamilton (2013) has argued for further application of evidence-based design in the medical intensive care milieu, as this will improve the quality of care for patients, families, and yield more supportive work conditions for direct caregivers. Huisman et al. (2012) examined the physical environment’s fundamental, timeless effects on health status outcomes. This is achievable through systematic assessment of occupant well-being, that is, the experience of patients, family, and staff together with systematic, iterative assessment of technical support systems including materiality, space planning attributes, interior amenities, and relationship to central hospital support services. Therapeutic design interventions in critical care units have been shown to provide positive distractions for patients and their direct caregivers. Artwork, natural and artificial lighting, views to the exterior environment and landscape, access to gardens, noise minimization on the unit, ambient music and soundscapes, therapeutic color palettes, maximizing one’s sense of personal control and privacy, the provision of social supports, healthful air quality, cleanliness, and maintenance collectively contribute to a positive hospitalization experience (Iyendo et al., 2016). In short, a reduction in physical setting–emanating environmental stressors in the ICU can mitigate adverse outcomes (Rubert et al., 2007).
Summary and Conclusions
In 2004, R. S. Ulrich, et al. concluded that evidence-based research and design had by then demonstrated meaningful engagement with nature and landscape is preferred during hospitalization. Staff, family, and patient-centric built environment amenities have positive impacts on satisfaction, with a role in decreasing patients’ pain. Their investigation, however, did not include the 2003 SARS pandemic nor general pandemic considerations in planning and designing ICU built environments—because scant evidence-based research existed on that subject at the time. Since then, pandemic concerns in the ICU milieu have dramatically risen in importance in conventional hospitals, adjunctive surge capacity isolation settings, and in postdisaster portable field hospital contexts.
The ICU multiuser environment, as a workplace for ICU professionals, a place of care for patients, and a place for connection with patient families and other loved ones, is of enduring, central importance. This comprehensive review has underscored the therapeutic importance of nature and outdoor views, the deleterious impact of noise as a stress source, the increasingly important interventional role of families, the acceptance of the all-private-room ICU, and the continued call for evidence-based research on reducing medical errors and concomitantly increasing patient safety and infection control. Also underscored is the role of ecological sustainability in design, construction, and daily operations—and climate change–related disaster-responsive and pandemic architecture for health in support of public health crises (Verderber, 2021). As for the plight of direct caregivers, the COVID-19 pandemic has been difficult for frontline nurses and others who witnessed firsthand such widespread suffering and death (T. Brown, 2021).
In Table 2, a summary of the findings of this comprehensive review of the literature is presented. The 135 source citations are categorized in two groupings: quantitative investigations and qualitative investigations/essays. Within each type, findings or assertions of positive outcome, no effect, or a negative outcome are denoted. This overview can serve as a basis for identifying areas warranting further research. Research content gaps in this literature became apparent, notably the need to conduct more in-depth research on the physical and psychological benefits of engagement with nature, art, and multisensory stimulation. Aspects of salutogenic design, and biophilia, warrant further research, perhaps within the umbrella afforded by an ecohumanist perspective—a perspective that fuses these concerns with ecological sustainability concerns (Verderber & Peters, 2017). Evidence-based research is warranted on attention restoration theory in ICU settings, perhaps combined with the phenomena of nature-deficit disorder as postulated by psychologist Richard Louv (2008). Also underrepresented were studies and essays on cost containment policy and best practices, ecological/resiliency determinants, or the role of advanced digital technologies, with none on robotics, and few on the subject of “Smart ICU” planning and design.
ICU Built Environment Literature (2005–2020): Quantitative Investigations, Qualitative Investigations/Essays, and Associated Outcomes.
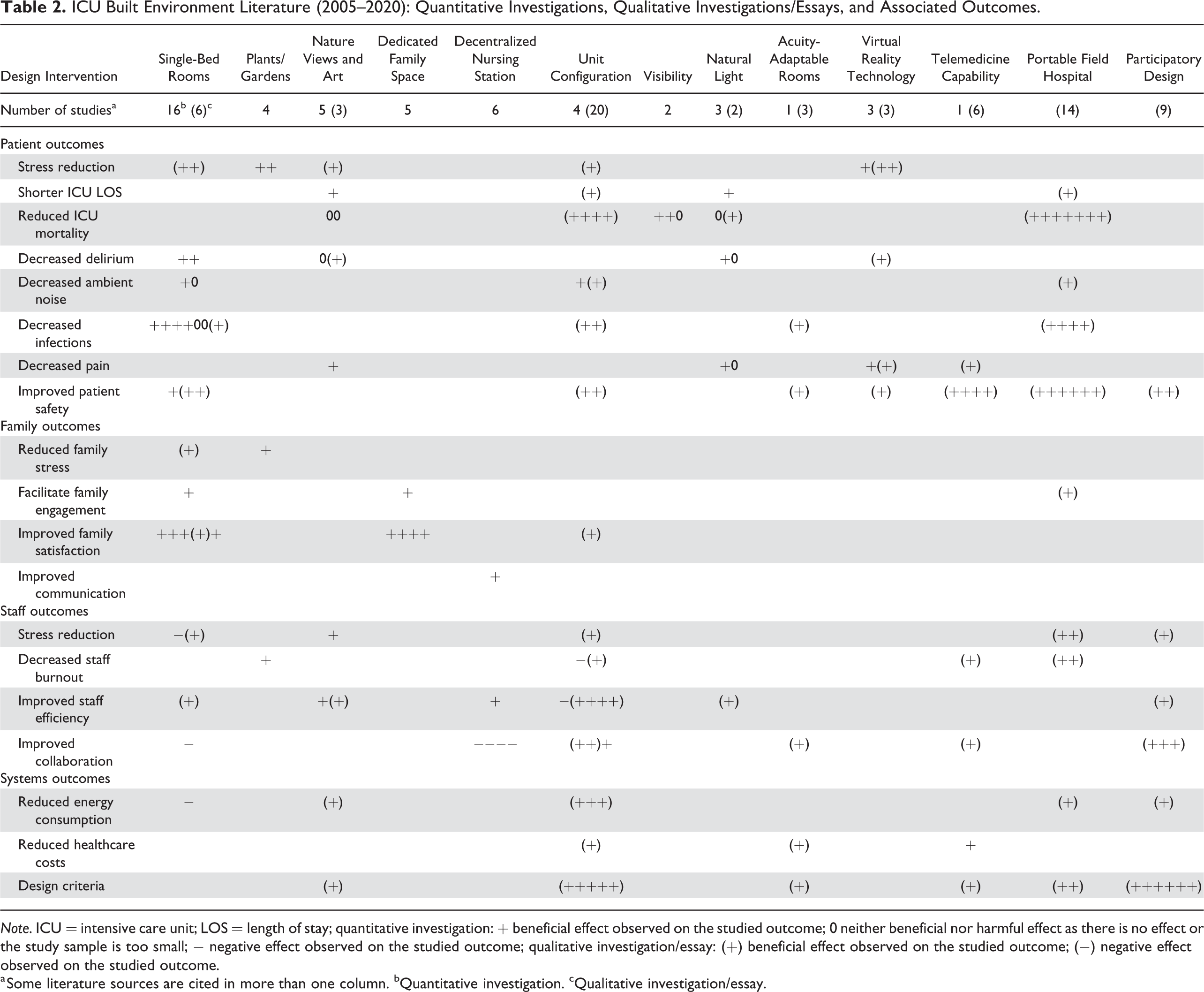
Note. ICU = intensive care unit; LOS = length of stay; quantitative investigation:
a Some literature sources are cited in more than one column. bQuantitative investigation. cQualitative investigation/essay.
Suffice to say, pandemic considerations in intensive care built environments will continue to warrant research-based design attention. Cross-cultural, interdisciplinary collaborations will be essential between health policy experts, direct care providers, researchers, and the many specialists who plan and design these built environments. Architects, landscape architects, interior designers, artists, lighting, and equipment specialists have much insight and expertise to offer if hospital intensive care environments are to more therapeutically support the needs of their occupants in the future. It is expected the most important overarching design considerations will continue to center on mitigating adverse medical event occurrences and on improving the experience of all who work and receive care in these specialized environments worldwide.
Implications for Practice
– Evidence-based research findings are presented on the state of the art in ICU built environments over the past 15 years. This knowledge base has direct implications for facility planning, design, and management.
– Case studies in disaster response and pandemic healthcare facilities are reviewed, including architectural proposals and field hospitals constructed in response to the COVID-19 global pandemic.
– Prognostications for the future of ICU and related critical care built environments in hospital and field hospital settings are presented.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by John H. Daniels Faculty of Architecture, Landscape, and Design, University of Toronto.