
Abstract
Aim:
The study aim was to co-design new pediatric procedure room prototypes with children, caregivers, and healthcare providers (HCPs).
Background:
Medical procedures can cause pain and anxiety for children and their families. If spaces are not designed for patients’ needs, procedures may take longer, require sedation, and result in an inferior care experience. Involving HCPs in co-designing optimal spaces can result in more efficient and safer environments. co-designing spaces with patients and their families can inform psychologically safer and less traumatic environments.
Methods:
We followed human-centered design methodology. Data were collected via semi-structured interviews, field observations, and two multidisciplinary design workshops with patients, caregivers, and HCPs. Themes from the data were extracted using a content analysis and used to make evidence-informed recommendations for design features.
Results:
The study took place from October 2021 to February 2022. Patients, families, and HCPs reported similar needs: (1) control over the environment, including the ability to adjust lighting, temperature, and sound; (2) space that supports patient privacy; (3) the use of evidence-based pain reduction and distraction methods; (4) attention to the sensory environment, including visual (light, color), tactile (textures of furniture and equipment), auditory, and olfactory stimuli; (5) human factors organization of the space and equipment; (6) accessible and equitable spatial design; and (7) the significance of the journey leading up to and after the procedure.
Conclusions:
It is feasible to co-design procedure rooms that support evidence-based psychological, physical, and pharmacological interventions that are known to minimize pain for children.
Keywords
Introduction
Pain from medical procedures can be a traumatic part of children’s experience in healthcare settings (Dewan et al., 2023; Trottier et al., 2019). Painful procedures are common among children in hospital and outpatient settings (Stevens et al., 2011). In pediatric outpatient settings, painful procedures are common for a variety of reasons, such as diagnostic testing, vaccination, blood draws, and minor surgical procedures. Such procedures are necessary for the prevention and treatment of disease and trauma but can cause anxiety, pain, and distress. In the quest to promote comfort and reduce pain, it is important for healthcare providers (HCPs) to consider the varying needs of children and adolescents.
Poorly managed procedural pain has short- and long-term consequences, such as increased fear about future healthcare interactions and ongoing cycles of procedural distress (Kennedy et al., 2008; Shave et al., 2018). Painful procedures and inadequate pain management early in life lead has implications in brain development of children and adolescents (M. D. Williams & Lascelles, 2020). Anxiety and fear related to procedural pain can often be prevented or largely reduced. However, many evidence-based interventions, tools, and methods to reduce procedural pain and fear remain underutilized in the pediatric population (Bice et al., 2014; Jiang, 2020; Young, 2005). The importance of the built environment and its proven ability to have a positive influence on patients’ health outcomes, specifically by reducing pain, anxiety, and stress is often underappreciated (Laursen et al., 2014).
Hospitals don’t intentionally have poorly designed spaces, but often, the fragmented nature of additions and workarounds result in less-than-ideal spaces for healing. When the space is not intentionally designed for the patient or clinician, procedures may take longer or need to be done using sedation medications, patient and staff safety may be negatively impacted, and patients, caregivers, and staff may have a poor care experience (MacAllister, 2016). Conversely, several studies in evidence-based facility design demonstrate that well-designed built environments can encourage healing (DuBose et al., 2018; McLaughlan et al., 2019; Mourshed & Zhao, 2012; Schweitzer et al., 2004; Ulrich et al., 2008). In pediatrics, child-friendly environments can facilitate improved patient and caregiver outcomes, including reported higher quality of service, increased satisfaction with care, less fear and anxiety for caregivers, reduced pain perception, and reduced use of pain and sedation medications (Malenbaum et al., 2008). Children’s hospitals are unique spaces that foster family and child-centered care (Casimir, 2019). Rooms in which painful procedures take place must not only include the right equipment and team members but must also support the different needs of children and adolescents, the centrality of the family in facilitating care, and the many cultural and social differences between the patients and families. Unfortunately, hospitals often don’t have the knowledge, resources, or opportunity to collaboratively design spaces with and for patient’s and family’s needs.
Human-centered design methods in healthcare environmental design can be used to create hospital spaces that are uniquely suited to patient needs (Lorusso, Lee, & Worden, 2021). The value of co-creation at the front end of development projects can drive change and innovation, which is critical for future-focused transformation projects (Candel et al., 2020). Involving patients, families and HCPs in designing optimal spaces may result in more efficient, comfortable, and safer solutions, and potentially fewer resources trying to retrofit spaces to meet specific needs after the fact. This may be a new era of healthcare spatial design that is multidisciplinary and collaborative (Pentecost, 2022).
=In our hospital, children who need outpatient medical procedures are treated in one of several procedure rooms. A procedure room in a pediatric setting is a specialized area within a hospital or clinic that is specifically designed for performing nonsedated or minimally sedated ambulatory procedures on children. Common procedures that may take place in the procedure room include feeding tube insertions, skin biopsies, intravenous catheter insertions, removing sutures, burn or surgical dressing changes or removal, surgical pin removal, range of motion stretches or exercises, or compression garment measuring. Most procedure rooms tend to be uncomfortable and frightening clinical spaces that don’t consider the patient’s or family’s emotional or psychological experience.
As the hospital undergoes a capital redevelopment plan, our research team of clinician designers (occupational therapist, nurse, and physician) were tasked with reimagining optimal procedure rooms. We describe the human-centered design methods used to co-design new procedure rooms that are intentionally designed to reduce fear and support adaptive pain responses.
Significance
Human-centered design methods can be used to inform the design of pediatric hospital spaces that are optimized to patient, caregiver, and HCP needs.
Aim
Our aim was to gather insights from children, families, and HCPs to inform the design of outpatient procedure rooms that support psychological, physical, and pharmacological interventions known to minimize pain and anxiety in children.
Framework Guiding the Study
Human-centered design is an iterative, participatory, and qualitative approach to research and problem-solving (Greenhalgh et al., 2016; Liedtka & Ogilvie, 2011; Ku & Lupton, 2022; Kumar, 2012).
Method
Study Design
This project was conducted using the methodology of human-centered design. Co-design activities were conducted with patients, caregivers, and HCPs. The project received administrative ethics approval from the hospital’s campus redevelopment project team. The project was conducted to address operational requirements within the hospital’s ongoing campus redevelopment project. Informed consent to participate in interviews and design workshops was obtained verbally at the start of each session.
Setting
The hospital is a 370-bed, tertiary care, freestanding academic children’s hospital in a large urban area. It cares for patients from birth to 18 years of age. The hospital is undergoing a large, multiphased capital redevelopment plan with the aim of transforming pediatric care. The redevelopment process presented an opportunity to redesign outpatient procedure rooms to better meet the needs of children undergoing procedures their accompanying caregivers and the staff involved in performing the procedures. The outpatient procedure rooms are used for nonsedated or minimally sedated ambulatory procedures, such as feeding tube insertions, skin biopsies, and intravenous catheter insertions.
Participants
Participants were selected by purposeful sampling. We aimed to include a diverse group of individuals, including current and past patients who have been treated in procedure rooms, their caregivers, HCPs (physicians, nurses, child life specialists) who work in procedure rooms, pain specialists, and hospital administrators (Table 1).
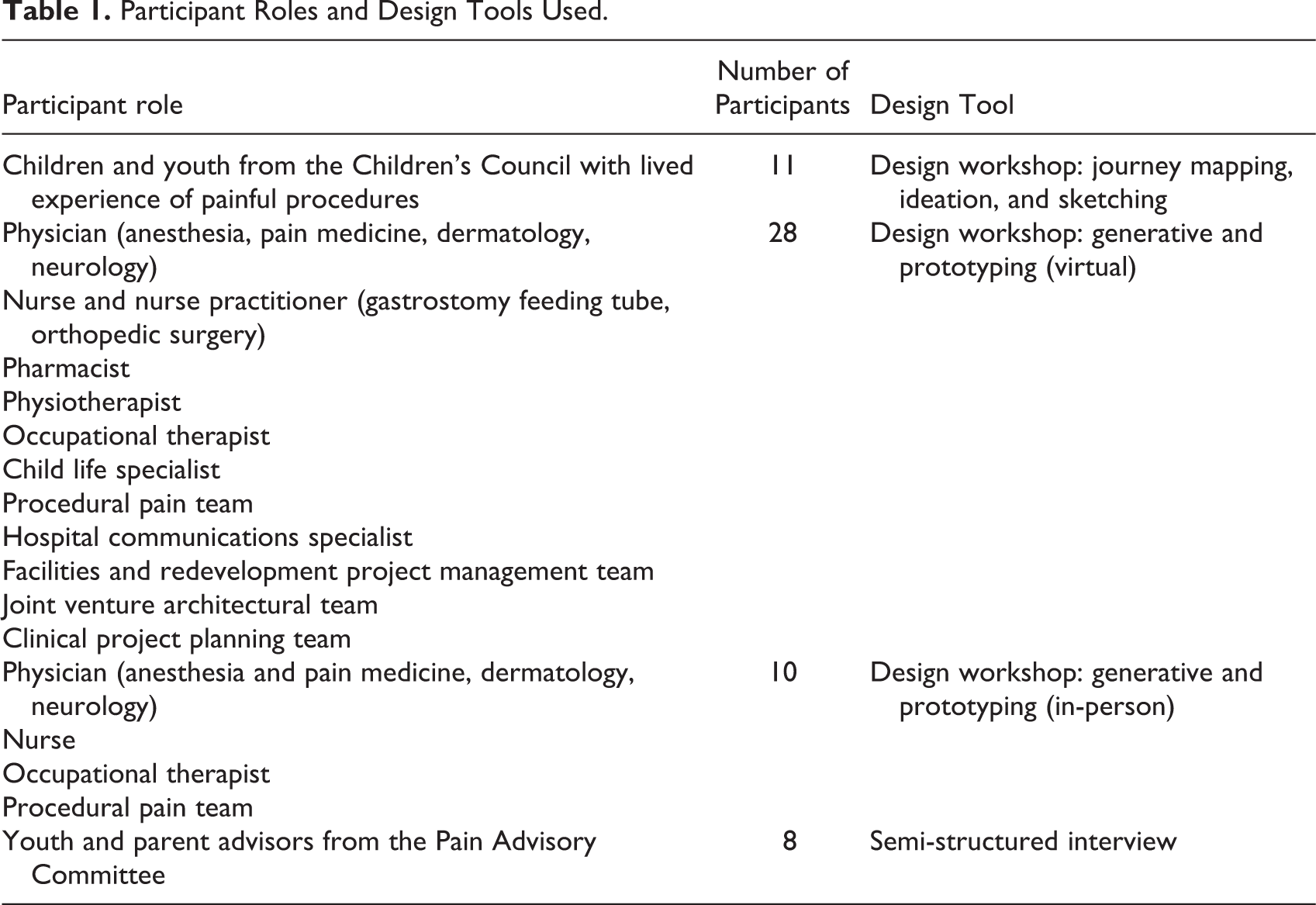
Participant Roles and Design Tools Used.
Data Collection
To gain insight from multiple stakeholders, we conducted field observations, semi-structured interviews, and co-design workshops. Research was led by clinician designers who are experienced with design research facilitation (S.L., L.C., and J.C.).
Ethnographic research
Our initial research included ethnographic observations, which is a method of inquiry originating from anthropology and sociology in which shared patterns of behavior, language, and actions are studied in their natural setting (Jones & Smith, 2017). For this study, we conducted unstructured observations in the current procedure rooms to determine personnel, equipment, and environmental issues.
Co-design workshops
We conducted a 1 hour design workshop with 11 children and youth from the hospital’s Children’s Council. The Children’s Council is a group of children and youth aged 9 to 17 years who are past or current patients of the hospital. The Children’s Council meet regularly to contribute to various hospital initiatives by providing insights based on their lived experience. Their role can involve consulting on clinical policies, hospital guidelines, and research initiatives to ensure the child and youth voice and perspective is central to hospital projects and programs.
During the workshop, we facilitated a journey mapping exercise of the patients’ experiences with pain and painful procedures using the current procedure rooms. Journey mapping is a design research technique that helps designers understand a person’s experience of a product, service, or space over time (Marquez et al., 2015; Miller & Flowers, 2016). Journey maps allow the designer to capture insights beyond the process to understand the emotional experience. Ultimately, this exercise enables the designer to build empathy for the people they are designing for while also identifying opportunities for innovation within the existing product, service, or space. After journey mapping, children and youth described and drew pictures of their ideal procedure room space.
We facilitated two design workshops with groups of interprofessional HCPs who perform or assist with nonsedated or minimally sedated procedures in the current procedure rooms. Thirty HCPs from a variety of professional backgrounds took part in the workshops (Table 1). The first 2-hour workshop was held virtually and focused on eliciting challenges and brainstorming solutions. Activities included a presentation of the data collected, an opportunity to validate or refute the themes from the data, a series of independent and team-based brainstorming activities and an opportunity to share and provide feedback about potential solutions. The second 2-hour workshop was in-person and was focused on ideation and generating physical prototypes of solutions (Babich, 2020). The workshops consisted of sharing insights on the patient experience by presenting the children’s journey map, brainstorming ideas in small design teams, followed by low-fidelity prototyping with craft supplies. Participants presented their prototype concepts to the group for feedback.
Data from the design workshops were synthesized and presented to the Pain Advisory Committee for validation. The Pain Advisory Committee is comprised of current and past patients and parents who have lived experience with managing procedural pain, acute pain, postoperative pain, and/or chronic pain. Similarly to the Children’s Council, members of the Pain Advisory Committee meet regularly to consult on various hospital projects and programs relating to pain.
Semi-structured interviews
We conducted seven semi-structured interviews with youth advisors and one semi-structured interview with a parent advisor from the hospital’s Pain Advisory Committee by telephone or video call (Online Appendix 1). Interviews were conducted virtually and lasted approximately 45 minutes. Interviews were audio recorded and transcribed.
Data Analysis
Data were synthesized to extract themes using content analysis. This approach involves reading through the raw text (transcripts, notes from field observations) to identify meaningful segments and allow themes to emerge. The objective of the analysis was to transform themes into actionable design criteria and opportunities (Thomas, 2006). Themes were used to guide ideation sessions with the research team. Solutions, including low fidelity prototypes, were presented to teams of key stakeholders, including pain subject matter experts and project planning teams for validation and refinement.
Results
Data collection took place from October 2021 to February 2022. The research team analyzed data, conducted ideation sessions, and presented prototypes to pain experts and the architectural, planning, and clinical teams in April 2022.
Six themes were extracted from the data. The following are the themes, descriptions of the themes, supporting quotations or examples, and actionable design opportunities.
Themes, Descriptions, and Recommendations.
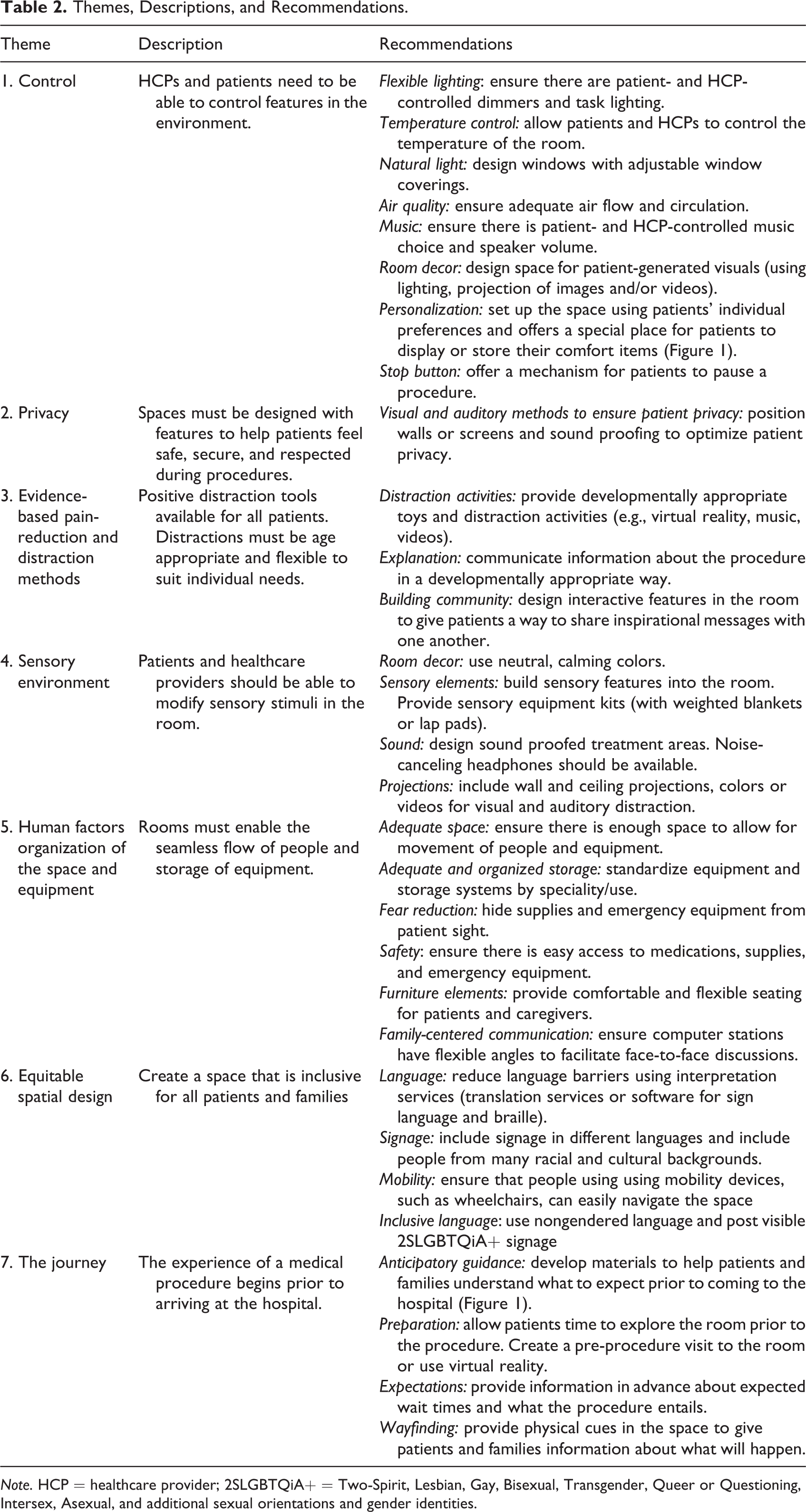
Note. HCP = healthcare provider; 2SLGBTQiA+ = Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer or Questioning, Intersex, Asexual, and additional sexual orientations and gender identities.
Theme 1: Control
Both HCPs and patients emphasized that the ability to control and personalize aspects of the environment would improve their experience and better meet their specific needs. Control over the environment included the ability to more easily adjust the room’s temperature, lighting, and volume of sound systems. HCPs and patients described examples of the discomfort from inappropriate temperature for the type of procedure, for example, a cold room for a procedure requiring undressing. Lighting was very important to both groups. HCPs described procedures which would be much easier to perform with task lighting that is adjustable in brightness and direction, for example, when removing a skin lesion. Giving patients control to change the overhead lights in the room would offer the autonomy to watch or not watch the procedure. Regarding lighting, one patient commented: “It is important that there is softness when you walk in a procedure room. Make it less scary.” HCPs and patients described music as a stress reliever and favorite distraction method, so emphasized that both HCPs and patients should be able to control the sound system. One prototype generated during the design workshop was the concept that the room could be personalized with each patient’s preferred environment. Children could predetermine color, light, music, and decor theme specifications, particularly for children who have frequent procedures. Another prototype idea was a storage or display “cubby” for children’s favorite toys which could be set up in advance of their visit to make the space more familiar (Figure 1).
Theme 2: Privacy
Patient privacy is governed by hospital policies and Personal Health Information laws but is often suboptimally realized. Both patients and HCPs wanted to ensure the space would be set up to optimize patient privacy. Patients reported that they wanted control over their bodies, their personal information, and what would happen to them. Patients wanted to feel secure that they would be treated with appropriate dignity and respect. For example, several patients and HCPs shared the experience of someone opening the current procedure room door, causing the patient to be exposed during a sensitive procedure. Both HCPs and patients described the importance of a space where private conversations could take place without caregivers or others nearby seeing or hearing. Youth also expressed not wanting to hear other patients’ confidential information. It is important to ensure patients feel comfortable, supported, and safe disclosing sensitive and personal information so that HCPs can provide appropriate care. For example, it is important for patients and HCPs to be able to discuss sexually transmitted infection testing or for HCPs to conduct genital examinations after the disclosure of child sexual assault. Each individual patient will have their preference for whether they want their caregivers involved in certain aspects of their care.
Theme 3: Evidence-Based Pain Reduction and Distraction Methods
Patients describe positive experiences with painful procedures where evidence-based pain-reduction and distraction measures were used (AboutKidsHealth, 2018; Eijlers et al., 2019; Gates et al., 2020). One evidenced-based practice recommended by patients and HCPs was comfort positioning. Comfort positioning means allowing the child to take a position of comfort during the procedure, which is most often with the patient sitting up or on a caregiver’s lap. These positions can be supported by adequate and flexible seating, for example, a chair that allows for the child and caregiver to sit together during procedures. During the generative design workshop, one group prototyped a chair designed to hold the caregiver-child dyad during a procedure (Figure 1). HCPs noted the importance of support from a Child Life Specialist who could provide age-appropriate explanation and distraction. Patients and caregivers should be able to change distraction methods during the procedure. Further, HCPs wanted to ensure that the procedure room would store and promote the use of pain-reducing medications, such as topical numbing medications. Both patients and HCPs describe that the patient’s physical and psychological comfort improved the experience for all involved and improved the ability of the HCP to perform the procedure.
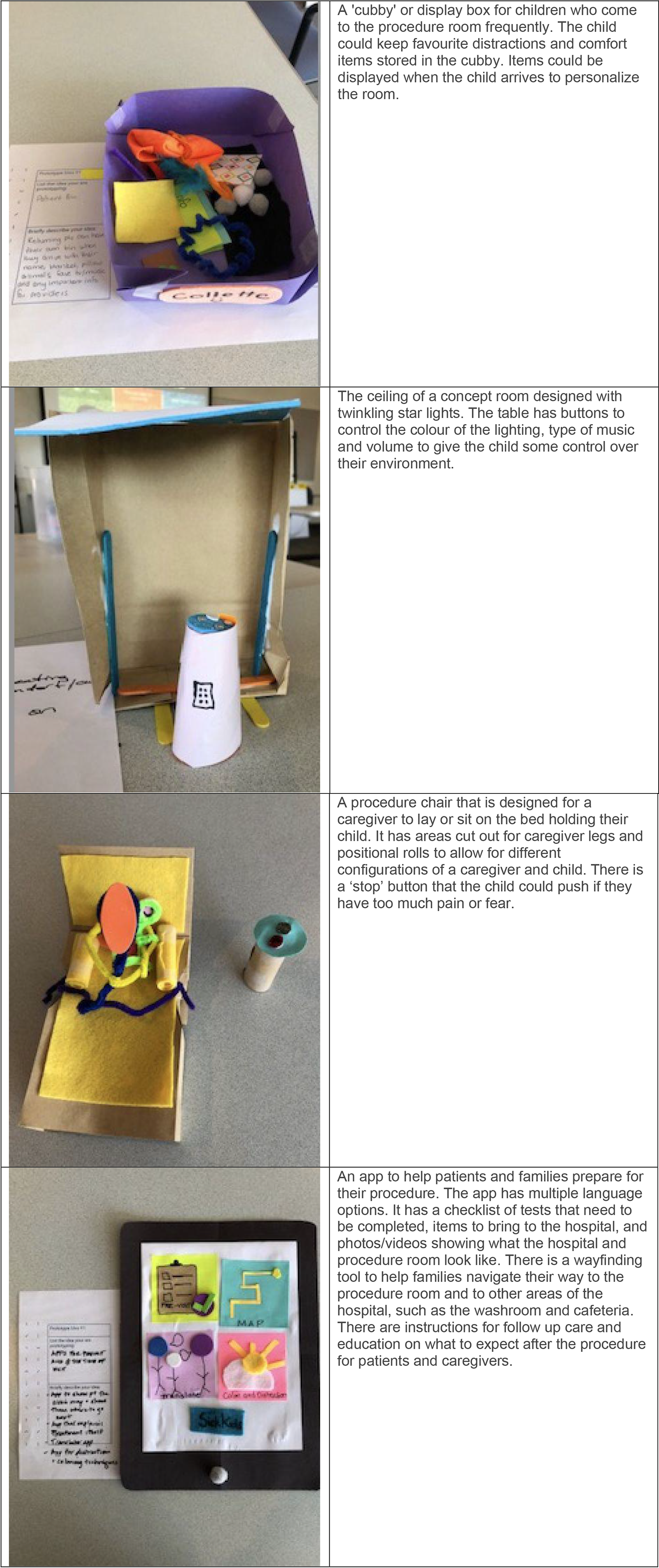
Prototype concepts from the generative design workshop.
Theme 4: Sensory Environment
Patients reported that they notice sensory details in the environment, including light, color, sound, smell, and touch. Attention to sensory details in the environment may be even more important for patients with neurodiversity, including those with Autism Spectrum Disorder and other sensory sensitivities. “I look at everything when I’m in the space having a test. Give me something to look at,” explained one patient. According to another patient, “the rolling paper on the exam tables sticks to you, rips and is just awful.” Patients described the importance of lighting to create a soothing and calm ambiance in the room. According to one patient, “[being in the] ultrasound [room] was a calming experience, it’s quiet, the lights aren’t intense, it’s not overstimulating, you can find time to breathe.” Another important feature noted in the environment was the comfort, color, texture, and size of the furniture items. Some furniture items were requested that were sized to accommodate small children, while some would need to accommodate larger children, adults, and those using mobility devices. A patient commented, “the chairs [for parents] are so uncomfortable, I feel bad for my mom.” Calming wall colors and natural light was emphasized by both HCPs and patients. Patients described wanting auditory (music, stories) and visual (movies, pictures, posters) distractions help them cope with painful or uncomfortable procedures. During the generative design workshop, one group prototyped a room with glowing stars on the ceiling for children to look at while lying down (Figure 1). Patients recommended interactive wall features or a way to share inspirational messages with other children and youth.
Theme 5: Human Factors Organization of the Space and Equipment
There was a unanimous sentiment among patients, caregivers, and HCPs that the current procedure rooms are “crowded,” “unfriendly,” “hazardous,” “scary,” “stark,” and “old”. When asked what an ideal procedure room would look like, the sentiment was “welcoming,” “warm,” “distracting,” “practical,” “comforting,” “functional,” “enchanting,” “calm,” and “bright.” Both patients and HCPs commented on the storage of equipment and supplies. HCPs frequently reported that they needed an efficient and logical organization of the space and equipment. Cramped spaces were felt to be inefficient and unsafe as providers spent time searching for needed equipment or had to leave the room to find or replenish supplies, which increased the length of time of the procedure. HCPs wanted the equipment to be stored in an organized and standardized system to ensure it would be easily accessible. For patients, cluttered and scary-appearing equipment increased anxiety. Medical equipment was particularly frightening when it seemed to be “old.” “It felt like an old place with old equipment. I would have expected something more kid friendly, more modern,” said one patient. Another patient commented, “there are drawings on the walls of body parts that are not great. That can be really scary for little kids.” Patients reported that they did not want to see medical equipment and suggested that it be stored in covered or hidden storage areas. The size of the room was noted to be very important. HCPs requested a larger space to facilitate good clinical outcomes and minimize delays. Both groups expressed that there must be flexibility to adjust the space and furniture. For example, computer screens must rotate so HCPs can face the patient when speaking. The room must allow for flexibility of different seating arrangements, for example, for different caregiver configurations, strollers and wheelchairs.
Theme 6: Accessible and Equitable Spatial Design
Patients and HCPs reported that it was essential to design the space for all people who might use it. This included children with neurodiversity, such as Autism Spectrum Disorder, physical impairments, varying ages, developmental or intellectual abilities or gender identities, children and families speaking different languages, and those from different cultures. For patients and HCPs, feeling included created a sense of psychological safety. Patients and families described that feeling welcome was an important part of the healthcare journey that was often overlooked in their previous experiences. Specific suggestions included valuing diversity and representing the local community, for example, (1) signage, illustrations, and wording featuring children and adolescents from all backgrounds and abilities, with words from many languages; (2) ensuring spaces are easily navigated by patients using mobility devices, such as wheelchairs and strollers; (3) reducing language barriers for those who speak different languages or have visual or hearing impairment by using translation software (tablet devices for sign language interpretation, language interpretation, braille); and (4) language and an environment that is 2SLGBTQiA+ inclusive (2SLGBTQiA+ is an acronym that stands for Two-Spirit, Lesbian, Gay, Bisexual, Transgender, Queer or Questioning, Intersex, Asexual, and additional sexual orientations and gender identities), for example, using gender-neutral language, respecting patients’ pronouns, and displaying signs of inclusion such as a Progress Pride Rainbow Flag (V&A, 2022).
Theme 7: The Journey
Patients and caregivers reported that their experience before arriving to the procedure room had a significant impact on how comfortable they felt about the procedure. According to patients, the journey began even before arriving at the hospital. For children who are anxious, sensitive, or scared, or for those who have experienced previous painful procedures or have had negative experiences at the hospital, it was beneficial to start the emotional, psychological, and logistical planning and preparation several days in advance of the procedure. Patients report that having information about what to expect before, during, and after the procedure, what the space will look like, and the personnel that they will meet would help to reduce their anxiety and improve their coping. During the design workshop, a team of HCPs suggested that touchpoints throughout the journey could be designed to help patients feel prepared. Patients suggest having a greeter welcome patients and families to the procedure room space and provide information about what the experience will be like and who they will meet.
Design recommendations
Based on themes from the data, the research team created a list of recommendations for the facilities and redevelopment project management team, joint venture architectural team, clinical project planning team, and procedural pain team (Table 2).
Discussion and Conclusions
In this study, we used a human-centered design approach to co-design pediatric procedure rooms as part of the hospital’s capital redevelopment plan. We co-designed ideal procedure room concepts with patients, their families and HCPs, with the aim of going beyond facility guidelines to meet the physical, psychological, and emotional needs of those who use the space. This approach gave us insight into the lived experience of those who are cared for and who work in the procedure rooms, including their current challenges, unmet needs, and ideal future. We used these findings to inform the design of the new space.
The most important feature of an ideal procedure room was the ability of patients and HCPs to be able to control aspects of the space. Control included being able to personalize the sensory environment, such as lighting specific for each use case, or playing a favorite song to distract during a painful procedure. Colors, sounds, and smells all impacted the way patients felt in the space. In one research study in the emergency department, ambient lighting and sound reduced patients’ stress (Robinson & Green, 2015). The literature supports this finding that features in the hospital environment influence patients’ perceptions of control over their health experience. In a qualitative study including interviews and field observations, adult patients’ sense of personal control was often reduced while in hospital. Changes to the hospital environment could increase their sense of personal control and their emotional comfort (A. M. Williams et al., 2008).
Patients and HCPs wanted a space that could promote patient confidentiality. Research supports the concept that the environment can be designed for better patient confidentiality as found by interviewing patients attending an obstetric emergency department before and after renovations of the space (Hartigan et al., 2018). Hospital environments can be designed so patients feel secure and informed about their care (A. M. Williams et al., 2008). Anticipatory guidance and information provided before the actual procedure was felt to reduce anxiety and distress. Spaces can be designed to incorporate evidence-based pain-reduction and distraction methods. Many nonpharmacological options exist, such as comfort positioning of the patient (Wente, 2013) and technology as a digital distraction (Gates et al., 2020). Control over the environment can even influence patients’ perception of pain (Malenbaum et al., 2008).
There is significant evidence supporting the impact of the built environment on patient health outcomes and experience in hospital settings (Jamshidi et al., 2020; MacAllister et al., 2016). Children experiencing procedural pain have better outcomes and experiences if their environment is suited to their unique needs (Malenbaum et al., 2008). Furthermore, patients are aware of the physical environment and should be involved in the design of it (Trochelman et al., 2012). Yet there is paucity of human-centered design research to help us understand how to design pediatric procedural spaces to support comfort and minimize pain. With the current unprecedented surge in hospital construction, it is imperative that environmental characteristics influencing the well-being of patients, caregivers, and HCPs be identified and incorporated in future hospital designs. We expect that our methods, which involve insights from many key stakeholders, will result in a design that is durable and ideally suited to those who will use it.
The next step is to build one ideal procedure room prototype based on the design recommendations. Then, we will test the space with simulated and real patients and iterate on the design prior to scaling to create additional procedural spaces. Lessons learned can be adapted to other patient care spaces in the hospital.
Limitations
Our center is a large, tertiary care pediatric hospital. Although the findings are consistent with other research in this field, the project was conducted at one site, so our results and implications are center specific. Solutions suggested from our center may not be possible to implement or relevant to smaller or less resourced centers. However, we note that our findings can be implemented without major resources. All the patients involved in the project were part of patient-advocacy groups, which means that they have knowledge of the hospital and have previous experience with procedures. Not every patient who will be treated in the procedure room has this experience. While we gathered insights from HCPs and parents, we did not interview children under 12 years old, so may not have captured the experience of younger children. Finally, all participants involved spoke English. By not including participants who don’t speak English, we missed the perspective of the patients and family members who experience language barriers.
Recommendations for Future Research
Human-centered design should continue to be explored as a structured methodology of co-designing healthcare spaces. Future research should continue to develop methods where patients, caregivers, and HCPs co-design healthcare spaces with designers and architects. Further research is needed to build an evidentiary base for a rigorous approach to translating themes from qualitative data to design criteria and prototypes of healthcare spaces. Specifically in healthcare, it will be important to demonstrate how human-centered design methods can be used to augment evidence-based facility design and other improvement methodologies, such as quality improvement, lean, and six-sigma. Research is needed to show how simulation can be effective to prototyping healthcare spaces. Finally, more research is needed to differentiate between the unique needs of the patient, caregiver, and HCP and to understand when to prioritize each user’s needs when designing a space.
Implications for Practice
Human-centered design methods can be used to inform the design of clinical spaces.
Involving patients, caregivers, and HCPs in co-designing spaces can result in more efficient, safer, and intentionally designed care environments.
Patients and HCPs want more control over features in their clinical spaces, including light, sound, and temperature.
It is feasible to design clinical spaces that promote evidence-based psychological, physical, and pharmacological interventions known to minimize pain in children.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867231161097 - Designing a Child-, Family-, and Healthcare Provider–Centered Procedure Room in a Tertiary Care Children’s Hospital
Supplemental Material, sj-pdf-1-her-10.1177_19375867231161097 for Designing a Child-, Family-, and Healthcare Provider–Centered Procedure Room in a Tertiary Care Children’s Hospital by Sasha Litwin, Lindsay Clarke, Jocelyne Copeland, Jennifer Tyrrell, Caleb Tait, Vina Mohabir and Fiona Campbell in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.