
Abstract
Objectives:
This article compares national standards for area measurements of healthcare facilities in four countries and examines the risks and differences that can arise when comparing building areas of healthcare facilities internationally.
Background:
In the planning and management of healthcare facilities, the utilization and comparison of building floor areas plays a major role. Differences in terminology, classification, and methodology help to reduce planning and cost risks when applied on a local and national level. The proper allocation of building floor space is vital in the design of room programs, determination of floor space, construction costs, and operating costs.
Methods:
Each of the four hospital area measurement standards is compared to discern similarities and differences.
Results:
Most countries use a three-tier system of hospital area measurement: building gross area, department gross area, and department net area. Few differences were found between country standards for department area, though the German standards do not fully address this tier. Variation is found in whether a country includes certain functions in the hospital area—such as research space, shell space, or central energy plants—which can have a significant impact on the overall hospital area.
Conclusions:
This article informs further development of individual country standards and highlights principles to consider for international hospital area comparison.
Keywords
Hospital buildings are expensive, highly complex, and have a significant impact on patients and care providers. Efficient space planning is important especially due to high personnel and operating costs (Holzhausen et al., 2015). Decisions made regarding types and quantities of spaces can impact patient experience and patient safety (Brambilla et al., 2019). Some decisions related to hospital planning and management are informed by the area of the hospital in square meters (or square feet). The proper allocation of building floor areas is imperative for the economic consideration of healthcare buildings. Area allocations affect the design of room programs, area quantity determinations, construction costs, and operating costs (Zeitner et al., 2019). It is important that this information be accurate and consistent to provide confidence and reliability in cost estimating, design benchmarking, and facility management. “However, two architects, planners or facility managers measuring the same building will almost never arrive at the same…numbers unless they agree on the method of measurement and a clear definition of what is included and excluded” (Hayward, 2017, p. 8). “Casual benchmarking” and “apples-to-oranges” comparisons are common and the resulting data can lack credibility (Kahn, 2009). In response to these challenges, several countries have created hospital area measurement standards. These standards enable organizations to facilitate accurate and reliable benchmarking to support their hospital planning and management endeavors (Kelly & Pingel, 2021; Lavy et al., 2019; Pingel, 2021). However, many organizations work in international contexts and lack clarity in how to measure and analyze hospital areas across countries. Like other industries, healthcare organizations and design-related organizations are gradually becoming more internationally minded. There is opportunity for continued collaboration across countries to learn best practices in hospital planning, space programming, and operations. For example, principles of evidence-based design such as single-patient bedrooms that became prominent in the United States in the 1990s and 2000s have gradually been adopted in some other countries. European hospital designs that feature daylight in all occupied spaces have strongly influenced many recent US hospital designs. In cases like these, the adopted design strategy’s impact on hospital area may be unclear due to different international norms in area measurement. As international hospital area comparisons become more common, we hope that more insights can be identified on topics such as operations, staffing, flows, and space usage.
Despite cultural and geographic differences, hospitals around the world face many similar challenges. For example, rapid developments in medical technology, novel patient therapies, and pandemic responses are not only changing operational procedures and processes but are also demanding flexible space and a redesign of existing hospital structures. Another challenge is the increasing average age of patients in the course of demographic change (Matusiewicz et al., 2019). This is accompanied by the associated increase in chronic diseases and multi-morbid conditions (Schelhase, 2019). Future challenges in the hospital sector will extend beyond the consequences for individual facilities. Supporting international exchange could spur strategies and proposals for design and implementation from a broad community of stakeholders, including planners, architects and facility managers. International collaboration will provide an opportunity to share strategies for dealing with such challenges and opportunities in the future. Design or construction firms frequently work in multiple countries, and in some cases, the cross-border work is fluid and concurrent, such as for teams in the United States and Canada or in the Scandinavian countries. It is common for a team to compile project information from all countries worked in to inform future work in any one of the countries. Similarly, a hospital organization with locations in multiple countries may manage their hospital area information centrally, for example, to evaluate energy usage or to plan maintenance and repairs (Li et al., 2020).
In these cases, an approach may be to use the common practice area measurement standard of one country and apply that to the project sites of other countries. This may facilitate accuracy and consistency in measurements, which is important, but it may not allow the data to be used effectively by persons in other countries with different standards. Not being familiar with the measurement standard of the country used as the baseline, confusion and misinterpretations may result (whether knowingly or unknowingly).
Though not specific to hospitals, some international standards do exist. For example, international standards exist for property measurement in office buildings, residential buildings, industrial buildings, and retail buildings: “International Property Measurement Standards: Office Buildings November 2014; IPMS for Residential Buildings September 2016; IPMS for Industrial Buildings January 2018; IPMS for Retail Buildings September 2019” (International Property Measurement Standards Coalition [IPMC], 2014). Secondly, a standard was developed to achieve consistency in comparing building areas across European countries: DIN EN 15221-6:2011-12 “Facility Management—Part 6: Area and Space Measurement in Facility Management.” This standard states that “different national standards result in [area] variations up to 30% [and] clearly highlights the need for a harmonized European approach to area and space management” (Beuth Verlag GmbH, n.d.).
These international standards contribute to transparency and consistency in calculating and standardizing building floor areas, as there is a wide range of different national standards. However, a comparable standardized international document for hospital buildings is not yet available. National standards and guidelines for the measurement of hospital building areas exist in some countries. The individual standards define terms for certain hospital building floor areas and provide consistency nationally for the measurement of hospital areas. However, there are no guidelines developed (to date) that describe the similarities, differences, or comparability of international definitions. One difficulty in an international comparison of areas in hospitals is that in some countries, there is not a defined method of area measurement specific to hospitals. For example in Germany, standards exist in the building sector on areas and room volumes as well as on partial areas (net area) of functional areas in hospitals, however, these do not specify a comprehensive measurement method specifically for hospital areas.
International comparability of hospital areas is but one factor informing the planning and management of hospitals, but there is some overlap and interplay with other relevant factors. For example, normalization of hospital cost has been studied to reliably compare hospitals in different regions (Sharma et al., 2015). Other factors such as hospital energy usage or proportion of single-bed patient rooms have also been compared internationally and would benefit from an internationally compatible method of hospital area measurement.
Objective
As part of a broader study to achieve international hospital area benchmarking, as outlined in Figure 1, the objective of this study is to compare the similarities and differences in four national hospital area measurement standards. An adaptive framework and consistent form of presentation are outlined for better comparability. Differences in the designation, definition, and allocation of different hospital building floor areas can thus be simplified and made more transparent. We then suggest potential adaptations to accommodate international hospital area measurement, which we plan to test in case study projects in a future study.
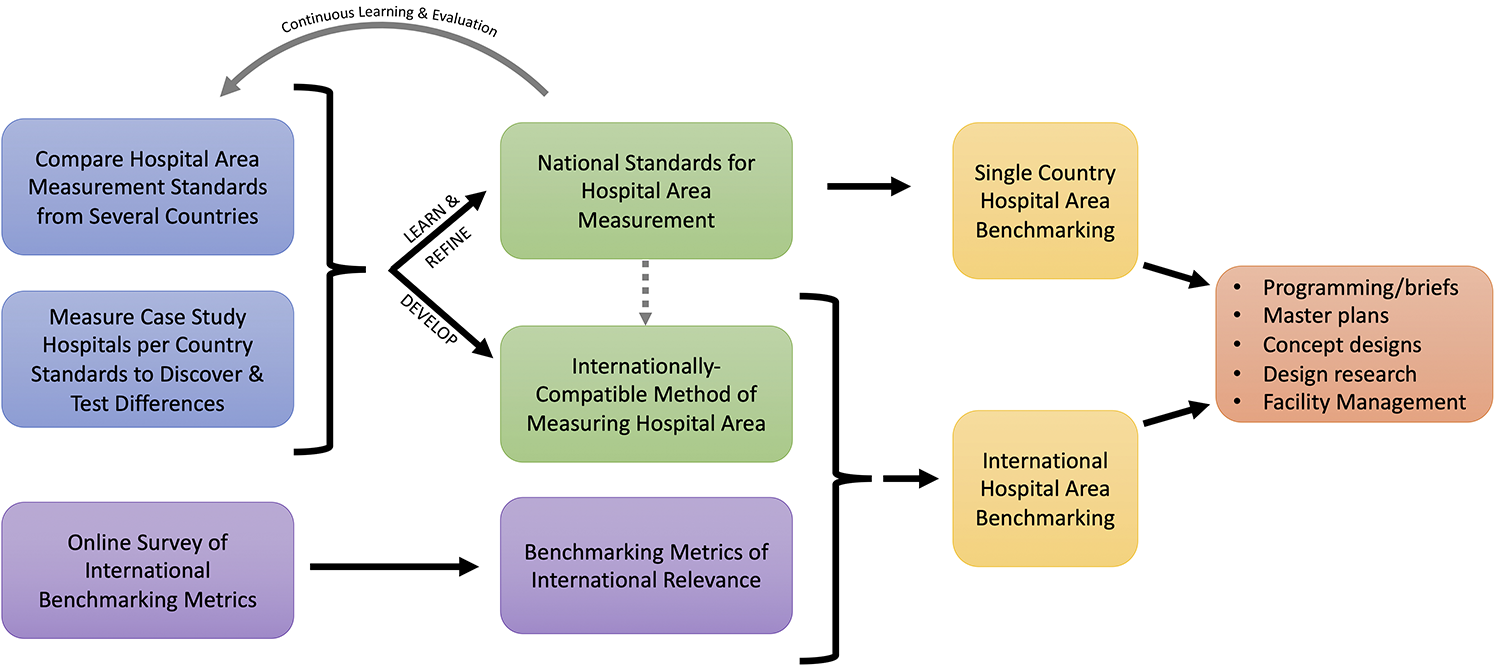
Process to achieve international hospital benchmarking.
Context and Background
For this study, we selected four countries that we were familiar with from our organizations’ work and where the country’s area measurement standard was thoroughly developed. Here, we provide a summary of the national standards for hospital area measurement for the four countries. Each standard is unique in terms of development process, stakeholder involvement, and areas of focus. For these four countries, the standards are more like “guidelines” in the sense that they are not on their own legally mandatory; however, they are generally seen to be the authoritative document on the topic and are sometimes adopted by local laws or contracts.
Canada
The CSA (Canadian Standards Association) Group is comprised of two organizations: a nonprofit standards development group and a commercial testing, inspection, and certification group. The CSA Group develops standards in a wide variety of sectors such as construction, environment, healthcare, petroleum, and more. In 1982, the CSA Group published the document “Z317.11 Area Measurement for Healthcare Facilities” (CSA Group, 2017). Significant updates occurred in 2002 and again in 2017, which is the current version and totals 46 pages. The standard was created by the Subcommittee on Area Measurement for Health Care Facilities which consisted of 17 members from the public and private sectors. Funding from several provincial governments contributed to the development of the standard. According to the area measurement standard, there are two main aims for its scope and purpose: Firstly, support healthcare facility planning and design activities that require such measurements (e.g., functional programming, building and room design, administration, cost estimating, and funding of capital programs). Secondly, facilitate meaningful comparisons between healthcare facilities throughout Canada.
The standards define area measurement as a three-tier system: The standards define area measurement as athree-tier system: building gross square meters, component gross square meters, and net area. The Canadian term “component” can be used interchangeably with the American term “department” and serves as “the basic building block for organizing health care facility projects” (CSA Group, 2017, p. 11). The standard includes descriptions (and some diagrams) to make clear which hospital areas should be assigned to building gross, department gross, or net area (CSA Group, 2017).
United States
In the United States, the American Institute of Architects (AIA) is a professional membership organization consisting of approximately 95,000 member architects and allied associates. In 1995, the AIA published the standard “D101 Methods of Calculating Areas and Volumes of Buildings” (AIA, 1995). The two-page standard describes a high-level methodology for calculating architectural area (gross area) and net assignable area for office, retail, and residential. Additional nonhealthcare-specific standards are published by: the Building Owners and Managers Association (BOMA, n.d.), the International Facility Management Association (IFMA, n.d.), and the International Building Code (ICC, n.d.).
Each of these standards has slight distinctions in how building areas are calculated, but they are not the focus of this article since a distinct healthcare-specific standard is available. In 2008, the healthcare architecture programs at Clemson University and Texas A&M University collaborated to publish “Analysis of Departmental Area in Contemporary Hospitals: Calculation Methodologies & Design Factors in Major Patient Care Departments” (Allison & Hamilton, 2008). The study developed a preliminary methodology for area calculation and provided analysis of benchmarking examples from several clinical departments such as Surgery and Inpatient Care. A main finding of the study was that the industry lacked and very much needed a standardized method for area calculation. The American Society of Healthcare Engineering (ASHE) is an association with approximately 12,500 members who work with design, building, maintaining, and operating healthcare facilities. In 2017, ASHE collaborated with the AIA Academy of Architecture for Health and the Academy of Architecture for Health Foundation to publish a 64-page monograph entitled “Area Calculation Method for Health Care” (Hamilton et al., 2017). The ASHE monograph aimed to build further on the 2008 work by Allison and Hamilton to create a thorough and standardized approach that did not conflict with the more basic requirements in the 1995 AIA standard and the 2002 Canadian standard. The three-tier area measurement methodology is nearly the same as the Canadian standard: building gross area, department gross area, and net area.
The ASHE monograph goes into more detail regarding the process for calculating areas, such as steps one may take and notes on specific software tools including AutoCAD and Revit. The ASHE monograph also goes into great detail on specific examples of areas that should be included as either Building Gross, Department Gross, or Net. For example, diagrams cover topics such as wall fur-outs around columns, nondepartmental corridors, exterior covered areas, and central utility plants (CUP). The overall goal of the method is to provide accurate and consistent area calculations (AIA, 1995). Projecting the net and gross space requirements for a new or renovated health care facility plays a key role in assessing facility configuration options and estimating the cost of the project at various stages of the planning process. Calculating and documenting existing spaces within health care facilities is also necessary for facility management, capital budgeting, financial reimbursement, and post-occupancy evaluation. However, two architects, planners, or facility managers measuring the same building will almost never arrive at the same department net and gross space numbers unless they agree on the method of measurement and a clear definition of what is included and exclude. (Hayward, 2017, p. 8)
Germany
The German Institute for Standardization (DIN) was founded in 1917 and is an “independent platform for standardization in Germany and worldwide” (DIN e.V., 2014). In 1975, DIN concluded a public–private partnership agreement with the Federal Republic of Germany, recognizing DIN as the only national standards organization. DIN contributors include over 36,000 experts from industry and research, from the consumer side and the public sector, contributing their expertise to the standardization process, which DIN manages as a privately organized project manager. The results are market-driven standards that promote global trade and serve economic productivity, quality assurance, the protection of society and the environment, and security and communication (DIN e.V., 2014).
The standard DIN 277:2021 “Areas and volumes in building construction” applies to the determination of floor areas and room volumes generally, not for a specific building type. It creates the basis for a comparison of buildings and properties as well as for the determination of costs according to DIN 276-1 and utilization costs according to DIN 18960 (DIN 277:2021-08, 2021). DIN 13080 is a hospital-specific standard with two additional supplements: DIN 13080:2016-06 “Division of hospitals into functional areas and functional sections,” DIN 13080 supplement 3:2016-06 “Division of hospitals into functional areas and functional sections—Form for the determination of areas in hospitals,” and DIN 13080 supplement 4:2016-06 “Division of hospitals into functional areas and functional sections—Master planning for general hospitals.” DIN 13080:2016-06 specifies the division of the hospital into eight functional areas (such as diagnostics and therapy, care, general services, etc.) and functional sections (such as emergency room, clinical outpatient clinics, rescue service) that are subordinate to the functional areas. DIN 13080 divides the areas according to function, regardless of cost allocation criteria, and refers to DIN 277. Both standards should therefore be considered together as a basis. DIN 277 is authoritative for determining the areas (DIN 277:2021-08, 2021; DIN 13080 supplement 3:2016-06, 2016; DIN 13080 supplement 4:2016-06, 2016; DIN 13080:2016-06, 2016). DIN EN 15221 Part 6 is a European standard that provides a common basis for planning and design for area management and financial evaluation. It also provides a basis for benchmarking in the field of facility management and for the measurement of floor areas in buildings and areas outside buildings (DIN EN 15221-6:2011-12, 2011). Furthermore, DIN EN 15221-6 addresses the inconsistent situation in Europe regarding the measurement of floor areas in buildings and creates a new standard with this norm. The aim is to measure data from area measurements standardized to provide consistent comparability of European floor areas (Beuth Verlag GmbH, n.d.).
In contrast to other countries´ standards, no standard in Germany defines the methodology of area measurements specifically for hospitals. The three-tier area measurement methodology found in the United States, Canada, and Australia is not specified in any German standard work but can be transferred by extrapolation as described in section Methodology Comparison (DIN 277:2021-08, 2021; DIN 13080:2016-06, 2016; DIN EN 15221-6:2011-12, 2011):
Australia
The Australasian Health Infrastructure Alliance (AHIA), formerly known as the Health Capital Asset Managers’ Consortium (HCAMC), consists of public sector collaboration in Australia and New Zealand. The alliance consists of senior asset managers from the public health authorities of the Australian and New Zealand states and territories. The AHIA was established in 2004. The AHIA assists industry organizations and member jurisdictions to “better plan, procure and manage” (AHIA, 2018) their health capital investments and assets. Research, information, and experience on developments in health facilities and infrastructure are collected and processed by the AHIA throughout Australia and New Zealand. A publication of acquired knowledge is the Australasian Health Facility Guidelines (AusHFG), first published in 2007 in collaboration with the Centre of Health Assets Australasia and Health Planning International. Since then, the guidelines have been updated regularly and consist of six parts with different focuses. Research findings generate best practice solutions for optimization potential in capital and facilities management. The AHIA continues to support and develop public health progress by updating the AusHFG, considering that accessible, functional, and cost-effective healthcare facilities are an important component of public health. Facility planning guidance and recommendations are based on knowledge research results and industry and consumer exchanges. The AusHFG Guidelines generally divide hospital areas into the following categories. (Bold: Corresponds to similar measures in other countries):
Methodology Comparison
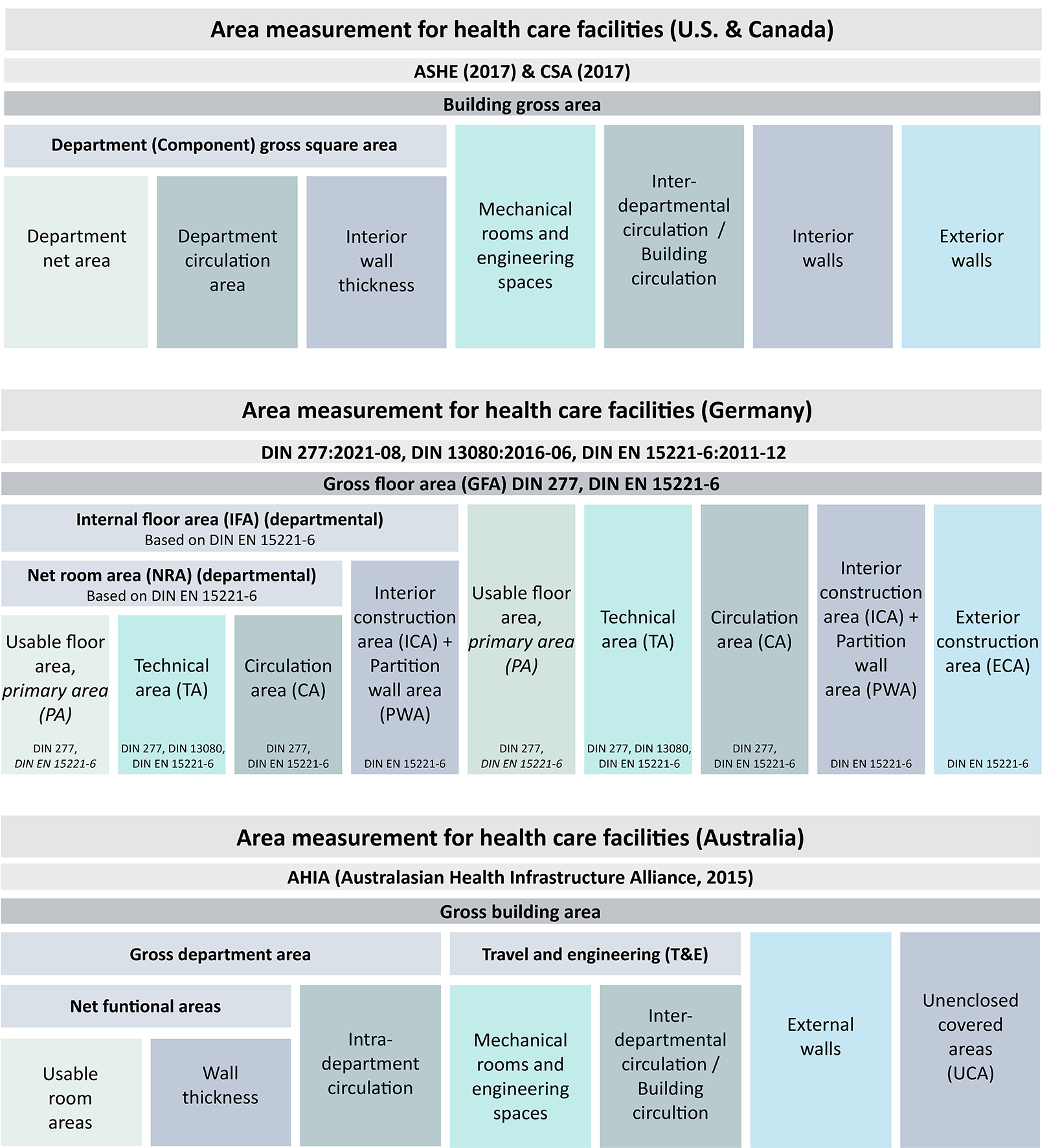
As shown in Figure 2, the four country standards are relatively compatible in use of the three-tier area hierarchy system, with some differences in terminology.

Overview of area terminology for each country.
Figure 3 shows more detail regarding the definitions of terms used to describe and categorize areas in healthcare facilities for the four different countries. Since in Germany no terminologies exist for department gross areas in hospitals, based on the German standards, DIN 277, DIN 13080, and DIN EN 15221-6 terminologies are defined according to American, Canadian, and Australian guidelines. This provides an adaptive framework allowing a comparison of the four standards.
Overview comparison of area measurement standards.
The four country standards were also compared on a detailed level regarding which specific types of hospital areas are included or excluded from each of the three area tiers. This gives further insights into what may cause area calculations to differ between countries. An excerpt of the detailed comparison is shown in Figure 4 and a full version is available in the Online Appendix.
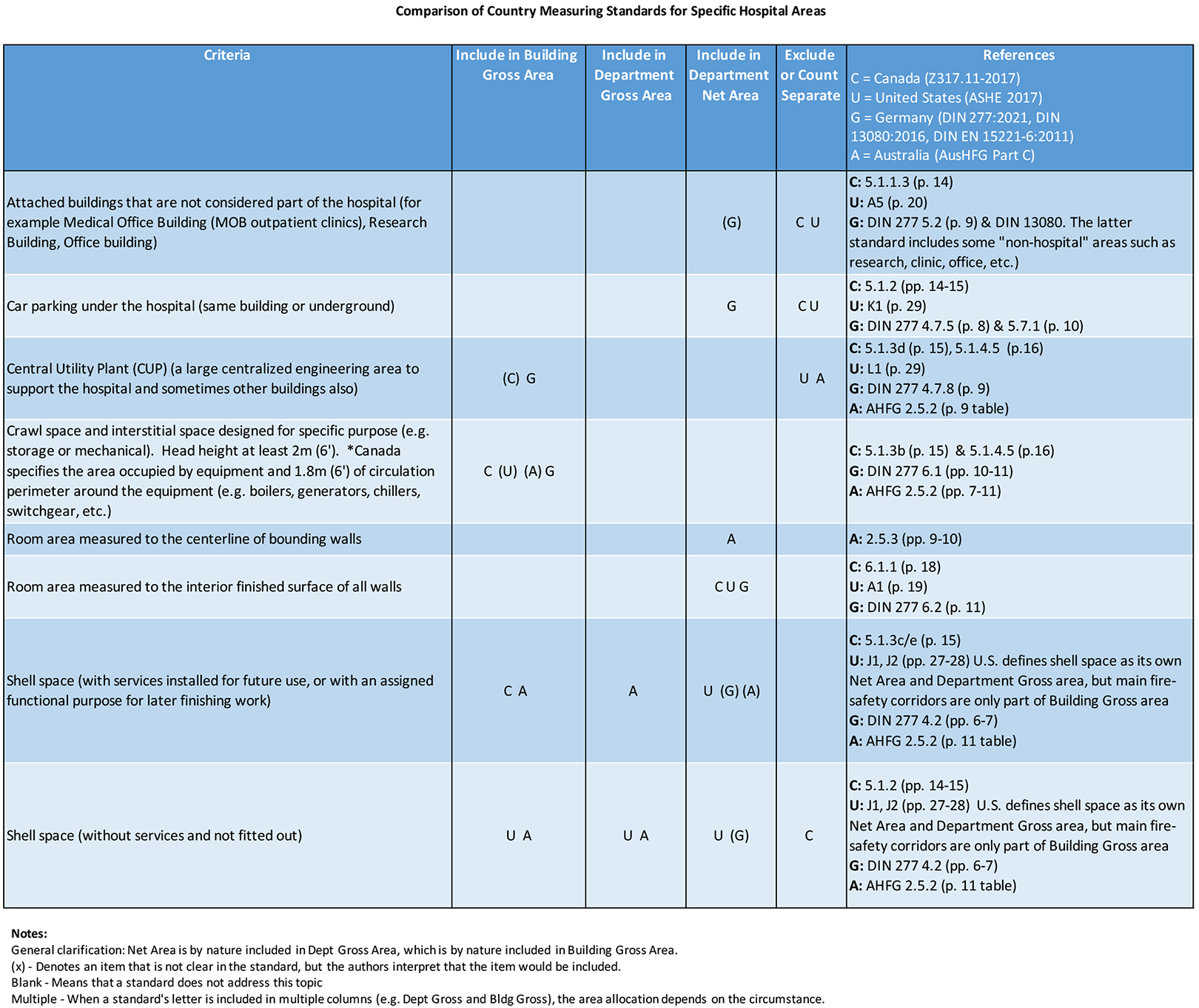
A detailed comparison of how area measurement categories vary in standards from the United States, Canada, Germany, and Australia (excerpt of full version available in the Online Appendix). Note. A letter in parenthesis (x) denotes a category not explicitly clear in the standard.
Findings—Applicable to Multiple Area Tiers
Several differences were detected between the standards that could affect multiple area tiers: building gross, department gross, and/or net area.
Shell space
All standards denote to include shell space that is fitted out for a specific purpose. However, the Canadian standard excludes shell space that is without services and not fitted out.
Research space
The US standard specifically excludes faculty offices or research spaces in order to maintain a “core hospital” of clinical space and support areas and to allow hospital areas to be more comparable between academic hospitals and community hospitals. The German standard includes faculty and research space, and though the Australian and Canadian standards do not address it directly, it may be included by implication as it is a functional space within the hospital.
Central plant
The American and Australian standards exclude CUPs (energy plants) from building gross area, stating that the area should be counted separately. In contrast, the German and Canadian standards include central plants in building gross area. DIN 277 states that if the purpose of a building is the supply by technical installations of another building, the areas are to be allocated to the net area (DIN 277:2021-08, 2021, p. 9).
Emergency vestibule
The US standard specifically states that emergency department vestibules count as net area and department area. Other country standards do not address this, and a person measuring may tend to count such a vestibule as building gross area.
Car parking
The American and Canadian standards indicate that parking areas are to be counted separate from building gross area. However, the German standard indicates that parking area is counted as building gross area and parking spaces counted as part of the net area. The Australian standard does not appear to address car parks.
Ambulance parking
Ambulance parking and receiving and shipping areas. The Canadian standard (CSA) specifically indicates that enclosed loading docks and enclosed ambulance bays are to be excluded from building gross area and counted separately. This unique category may be due to colder weather and more common enclosure of these spaces compared to other countries. In Germany, ambulance parking is included in the net area.
Findings—Building Gross Area
In the detailed comparison matrix, we found general consistency among the four standards in measuring the building gross area of the main portion of the hospital. The area is defined as the total area within the boundary line of the exterior cladding material. However, in the Australian case, there is a lack of clarity—in common practice, the facade thickness is often counted separately (e.g., 2%–3% of total area) and included in building gross area, but the standard implies that the facade thickness is to be completely excluded. For cantilevered building overhangs or exterior niches for swing-out doors, the US standard counts as “half area.” The other standards exclude this space. Similarly, the US standard includes the area of structural columns supporting cantilevered building above, while the Canadian and German standards exclude this space. The Canadian standard specifically states to include mechanical space whether it is enclosed or unenclosed, such as a rooftop air handler. In addition, service access routes around the equipment are to be included in gross floor area. This is distinct from the other country standards which exclude unenclosed spaces. Finally, the standards are in agreement that circulation not dedicated to a specific department is to be counted as building gross area. For example, public corridors or corridors serving more than one department.
Findings—Department Gross Area
The theoretical definition of department gross area is nearly equivalent across the standards in the United States, Canada, and Australia: the space associated with a clinical or functional unit within the hospital, generally including room net area plus wall thicknesses and departmental circulation. The German standards do not specifically define department gross area as a term, but extrapolations can be made from the various German and European standards together with best practice. The three countries' methodologies vary in how the department area boundary line is located in specific situations, for example when the boundary is adjacent to building support areas, nondepartment corridors, and out-swinging doors. The degree of impact from these differences will be investigated further in future paper testing case study projects.
Findings—Net Area
The Australian standard is unique in measuring room net area to the centerline of walls rather than to the face of walls. Specific direction is given on how to handle unique conditions such as walls of varying thickness. The four standards are consistent in measuring public lobbies and waiting areas but vary somewhat regarding how to handle enlarged public circulation spaces. The Canadian, German, and Australian standards do not count public circulation corridors as net area—even when the corridor is “open” to adjacent spaces the approximate boundary can be determined by estimating circulation routes. In contrast, the US standard includes circulation space as net area when designed as a public concourse/gallery/“main street.”
For open circulation in front of open-bay patient stations, such as PACU cubicles, the standards are consistent in counting the circulation as department gross area rather than net area, though for the Australian and German standards this is only implied indirectly. For circulation within a room (e.g., aisle between workstations) or circulation within an open workspace (e.g., circulation area for seating behind a nurse station counter), the standards are consistent to count this as net area, though again it is only implied indirectly in the Australian and German standards.
Discussion
Overall Similarities and Differences in Approach
In this article, we have identified differences in hospital measurement area standards that will need to be reconciled in order to facilitate comparison of international hospital areas.
The American, Australian, and Canadian hospital area calculation methodologies are built upon a three-tier structure of building gross area, department (component) gross area, and net area. In Germany, this approach is often used in practice but there is not a defined standard for how to measure department gross area. In this article, we have extrapolated how that could be defined based on the existing German standards. The four different countries' standards vary in their level of detail, their areas of focus, and the types of supporting diagrams included. For example, the Canadian standard gives a clear outline of each type of area to include or exclude, while the US standard gives more focus to situations that may arise when actually performing the area calculation. The Australian standard, in contrast, is less comprehensive in content topics but includes helpful suggestions for percentages of circulation and engineering space that can be used during programming (briefing). The German standard precisely divides the net area of the hospital into functions and assigns a color code to the resulting functional areas. Depending on the relevant national standard, there are differences in the terminology of building floor areas in healthcare facilities, although the terms are by definition referring to the same floor area. One example is the term net floor area: Canada: Net component area United States: Department net area Germany: Usable floor area (Nutzungsfläche)
Australia: Usable area
A slightly different term is used in each of the countries to refer to the same concept of the area within a single room. More significant, however, is when the terms appear to be referring to the same area type but in fact are different. For example, in Australia, the term net functional area (NFA) is calculated up to the centerline of the wall thickness, which may be confusing for someone in another country accustomed to “net area” not including any wall thickness. A more complex example can be found with department gross area. The United States, Canada, and Australia use nearly equivalent terms and definitions. However, the closest term in the German standard is “department net room area” (Netto-Raumfläche), which excludes wall thicknesses, structural columns, or chases (voids)—which results in a significantly smaller area calculation than department gross area in the other three countries. In the European standard DIN EN 15221 Part 6, the “internal floor area” in relation to a department corresponds to the department gross area.
Inclusion and Exclusion of Certain Areas
Research and faculty space
The German standard according to DIN 13080 explicitly mentions that research and faculty space should be considered as net area. The Canadian and Australian methods do not address this specifically, but it is implied that these spaces are included along with other occupied hospital spaces. In contrast, the American standard specifically states that research and faculty areas are not included. For a community hospital, this difference may be negligible, but it could be a significant area for an academic medical center.
Multiple buildings
The American and Canadian standards indicate that attached buildings with nonhospital functions are to be excluded. For example, this could include an outpatient clinic or research building attached to the hospital. However, the German standard DIN 13080 includes functional areas such as general services and research, teaching, and training which implies that they would be included as part of the hospital area even when not part of the main building(s). Nevertheless, the area calculation is made per building. This challenge is more clearly illustrated by a hospital consisting of multiple buildings and connecting corridors. Each building may have a distinct function and would need to be determined if it is part of the “hospital.” In addition, the enclosed walkways to nonhospital buildings would be completely excluded from the hospital area per the American and Canadian standards, but the German standard implies that areas that are structurally connected to the building are included in the area calculation. However, this topic is not explicitly addressed in the German standard. The Australian standard also does not appear to address this topic.
Building Services/Engineering Space
As shown in Figure 5, there is inconsistency in how these space types are handled among the four standards and in common practice. Hospital designs sometimes include air handler units (ventilation fans) that are installed on the roof and open to the air. This design decision is based on factors that may include climate zone, esthetics, service access, and cost. In some projects, the design may fluctuate back and forth between having an enclosed room for air handlers versus having the same air handlers exposed to the outdoors. According to the United States and Australian standards (which exclude counting rooftop air handlers), this would cause a lower building gross area than an equivalent building with enclosed air handlers. The Canadian standard accounts for this situation by including rooftop air handlers and their circulation space as building gross area. The German standard (DIN 13080) includes the area of rooftop air handlers as building gross area. DIN 277, on the other hand, indicates that rooftop air handler systems that are not fully enclosed and roofed are not considered as technical area. Consequently, this area is also not included in the building gross area. In common practice, reference is made to DIN 277, so that rooftop air handlers are not considered for the area calculation. The American and Australian standards exclude CUPs (Energy Plants) from building gross area, stating that the area should be counted separately. In contrast, the German and Canadian standards include central plants in building gross area. Often, the central plant is a stand-alone building, and in some cases, it may serve other nonhospital buildings on the campus. This variation in design could create difficulty in knowing how much of the central plant area to assign to the hospital.

Comparison of mechanical areas in each standard. Note. Listing both Yes and No denotes that two standards have differing approaches on the topic.
Building Gross Areas
Figure 6 outlines a preliminary framework to accommodate variation in country standards by allowing customization to add or remove “supplemental areas” as needed in the context. Variation was found in methods of measuring shell space, outdoor mechanical areas, CUPs, and area under cantilevered building above. When summed together, this variation may be significant between methods. Several variations may be of less significant impact such as canopies and structural columns outside the building envelope. Several area categories are listed specific to one country’s area method but not addressed by other methods. For example, the US standard (ASHE) recommends that building gross area include a specific line item for “miscellaneous structure.” This unique area category was probably added to account for earthquake seismic bracing for projects on the west coast of the United States. Several of the standards are clear to require separate calculations for areas excluded from the building gross area, such as central energy plants, rooftop air handlers, or canopies. These areas may require different treatment when used for cost estimating as compared to use for space benchmarking. Finally, the Australian standard differs in that the facade (exterior envelope wall thickness) is not clearly stated in the standard to be included in building gross area. Instead, the standard’s focus is placed on travel (circulation) and engineering areas making up the building grossing factor.
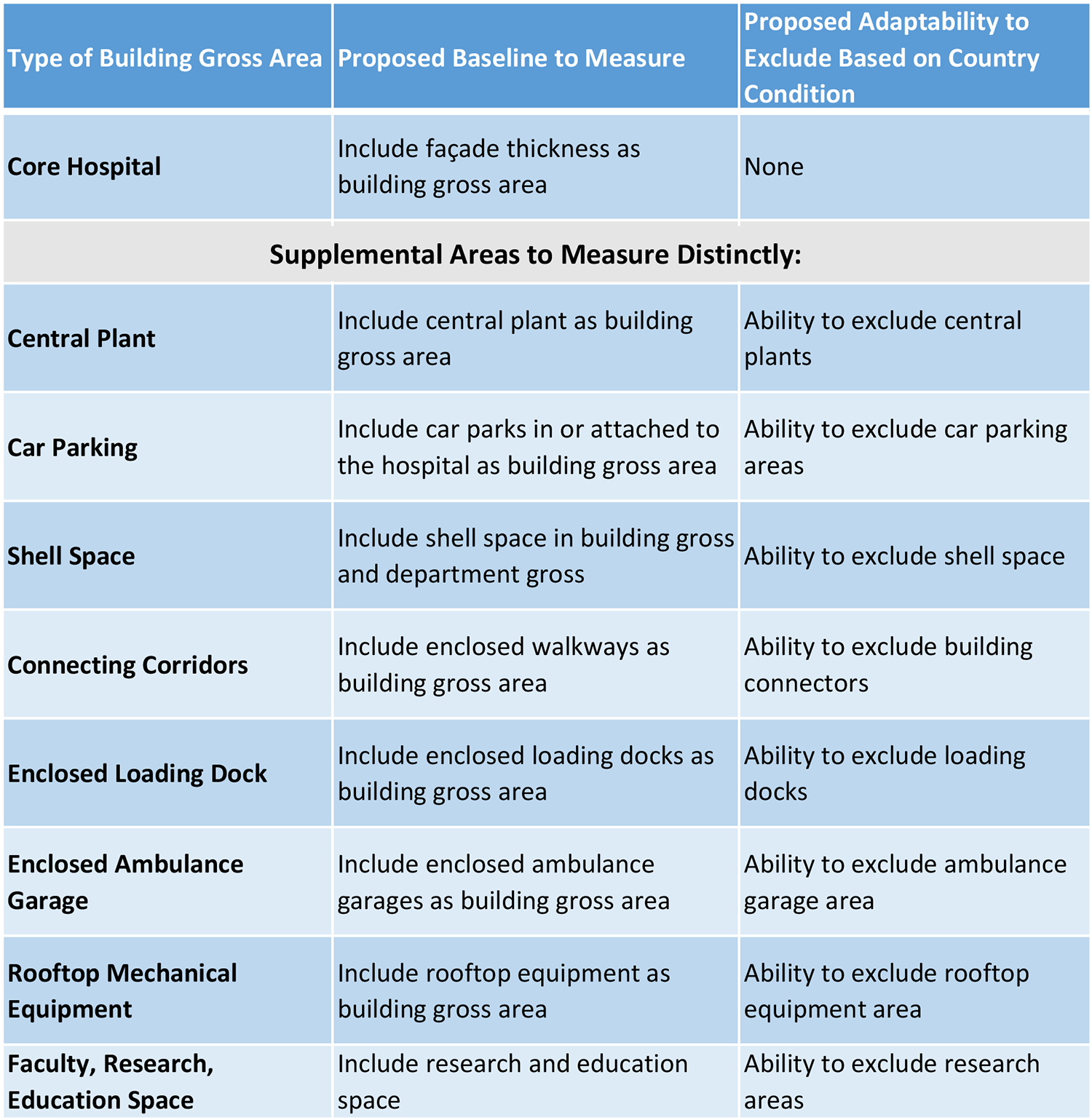
Preliminary framework to allow customization in hospital measurement to accommodate country-specific needs.
Department Gross Areas
In the detailed comparison matrix, we found consistency among the four standards in how to measure the department areas. The greatest variation was found in the allocation of shell space. The American, German, and Australian standards include shell space as department area. The Canadian standard includes shell space only as building gross space, and only if it has services installed for future use or has a clear assigned functional purpose for later finishing work.
Standardization and Comparability
The process of measuring hospital areas inevitably requires a person to make subjective decisions and interpretations throughout the process. The four standards attempt to provide guidance to clarify some of these situations, especially those that occur more commonly. For example, the US standard includes 15 pages of clarifications, definitions, and examples in an attempt to standardize the process and reduce variation among various projects being measured. The Canadian and Australian standards have similar content, though it is more integrated into the measurement process description. In Germany, there is no detailed method of how area measurements are performed in hospitals. This leads to inaccuracies in the individual procedure of area measurements. In a future paper, we plan to investigate the degree of impact for some of these areas open to interpretation, such as consistency in department naming and specific locations to draw area boundary lines.
To maximize international compatibility and make hospital areas comparable, it may be useful to have a “core hospital” as a baseline that includes the hospital areas that most country standards agree upon. Then, supplement areas could be added as needed for a certain country’s standard, such as research departments or central plants. However, this approach may require measurement of all supplemental areas applicable to all country standards. Additionally, this approach may deem that some elements of a country standard are inherently not compatible with the other area standards, such as the Australian method of measuring net area to the centerline of the wall.
It is important that a measuring standard provide information relevant to each of the countries it is intended for. It is also important to provide sufficient detail and clarity in a standard to ensure consistency in its use—ideally, different persons measuring the hospital area independently will achieve the same outcome. Otherwise, different persons will have a different interpretation on criteria that are not addressed sufficiently. On the other hand, if a measuring standard is too detailed, it may be onerous and cumbersome for the user and may reduce compliance with the standard. It is important that any standard be clear, concise, and effective. For hospital area measuring standards, this may include emphasis on criteria that have the most impact. In a subsequent paper, we plan to use case studies to help evaluate what portions of a hospital could be considered the core baseline and which may be supplemental areas as well as analysis of which measurement criteria have the greatest impact.
Conclusion
In this study, we have described the similarities and differences among four national standards for measuring hospital area. Unique observations can be made when comparing each of the three tiers: building gross area, department gross area, and net area. There are indeed differences in the standards that must be reconciled in order to facilitate comparison of international hospital areas. In some cases, a country may not have a defined standard for measuring hospital areas, creating significant opportunity to learn from standards that exist today. In other cases, such as Germany, further coordination is needed among national standards, especially in relation to the hospital context. Furthermore, by examining different national area measurement standards, a valid standard for area measurements in hospitals can be derived for Germany. For example, the German standard may wish to consider clarifying the category of department gross area which has been standardized in several other countries. In all cases, an awareness of hospital measurement practice is essential since architects and space programming consultants must decide “whether the projections made for projects and their budgets can rely on the information gathered” (Hamilton et al., 2012, p. 2). The understanding gained through an analysis of the four standards gives insights into methodology and approach that could inform the pursuit of an internationally applicable method for measuring hospital area. Such a standard would be useful for healthcare organizations operating facilities in multiple countries and for healthcare architects and contractors with projects in multiple countries.
Differences in methodology and terminology among the existing standards need to be evaluated and resolved, with each approach needing to flex to some extent in order to develop consensus on a hybrid standardized approach. An understanding of the methodology and terminology in each country is imperative to ensure that hospital areas measured across countries are accurate and reliable.
Limitations/Ideas for Further Research
We plan to test these ideas further in a second paper evaluating case study projects according to the four national area standards as a means of testing this adaptive framework, as well as evaluating the differences in the standards to determine the degree of impact on hospital area. Additional topics related to hospital area measurement could also be studied further. Our study was limited to review of hospital area standards from four countries. Additional country standards could be reviewed for new insights. Other topics of study may relate to how the hospital area information may be utilized and thus any related requirements for measuring or formatting the data. For example, cost estimating in the early stages of a project is often based on building gross area, while space benchmarking is often based on department gross area. It is possible that certain areas, such as rooftop air handlers and central energy plants, may need to be counted differently for costing as compared to benchmarking. Additionally, in contrast with traditional hospital space benchmarking, sustainability rating systems such as LEED and WELL focus more on measuring “regularly occupied areas”—for example, to develop metrics on daylight and outdoor views. This perspective could be studied further for potential alignment with the four country area standards in this article.
Implications for Practice
Inconsistencies in what types of spaces to include in the hospital area can have a significant impact in the resulting area measurement. This must be reconciled to allow for consistent comparison of hospital areas across countries.
To maximize international compatibility and make hospital areas comparable, it may be useful to have a “core hospital” as a baseline that includes the hospital areas that most country standards agree upon.
Then, supplement areas could be added as needed for a certain country’s standard, such as research departments or central plants.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_19375867221078838 - A Comparison of Hospital Area Measurement in Germany, Canada, Australia, and the United States: Part 1
Supplemental Material, sj-pdf-1-her-10.1177_19375867221078838 for A Comparison of Hospital Area Measurement in Germany, Canada, Australia, and the United States: Part 1 by Hannah-Kathrin Silja Viergutz and Michael Apple in HERD: Health Environments Research & Design Journal
Footnotes
Acknowledgments
The authors would like to thank HDR and Hajo Haller for the exchange of knowledge and further suggestions. The authors would also like to thank Dr. Jeri Brittin and Abigail Heithoff for their support by reviewing the paper and valuable feedback.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael Apple was employed by HDR, an architecture and engineering firm, during this research. HDR provided salary support for this author but did not have any additional role in the design, decision to publish, or preparation of this manuscript. Hannah-Kathrin Viergutz declares no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.