
Abstract
Objective:
The aim of this study was to explore patients’ experiences of the physical environment at a newly built stroke unit.
Background:
For a person who survives a stroke, life can change dramatically. The physical environment is essential for patients’ health and well-being. To reduce infections, a majority of new healthcare facilities mainly have a single-room design. However, in the context of stroke care, knowledge of how patients experience the physical environment, particularly their experience of a single-room design, is scarce.
Method:
This study used a qualitative design. Patients (n = 16) participated in semistructured individual interviews. Data were collected in December 2015 and February 2017 in Sweden; interviews were transcribed verbatim and analyzed using content analysis.
Results:
Two main themes were identified: (i) incongruence exists between community and privacy and (ii) connectedness with the outside world provides distraction and a sense of normality. In single rooms, social support was absent and a sense of loneliness was expressed. Patients were positively distracted when they looked at nature or activities that went on outside their windows.
Conclusions:
The physical environment is significant for patients with stroke. This study highlights potential areas for architectural improvements in stroke units, primarily around designing communal areas with meeting places and providing opportunities to participate in the world outside the unit. A future challenge is to design stroke units that support both community and privacy. Exploring patients’ experiences could be a starting point when designing new healthcare environments and inform evidence-based design.
Stroke affects a large number of people, and the subsequent rehabilitation and care are challenging. In Sweden, as in most high-income countries, almost all people with stroke are cared for at special stroke units (Riksstroke, 2015). There are evidence-based guidelines for the care provided at stroke units, such as early and individual-based mobilization, frequent and accurate assessment of health status, and well-developed teamwork (Ringelstein et al., 2013; Stroke Unit Trialists’ Collaboration [SUTC], 2013). However, despite the fact that studies in other fields show that the physical environment is important and can influence the patient’s health outcomes and how care is provided (Ulrich et al., 2008), little is known about the physical environment’s contribution to the quality of care at stroke units. In this study, we describe how patients experience the physical environment at a stroke unit that has been rebuilt according to a new single-room design. Such an investigation is important because the majority of new healthcare facilities are built with a predominantly single-room design (Joint Commission, 2018). Recently, a study showed that patients in a newly built stroke unit with a single-room design spend more time being inactive and alone compared to patients in an older multibed room design (Anåker, von Koch, Sjöstrand, Bernhardt, & Elf, 2017). However, how patients experience being cared for in single-room units remains unexplored.
As an important part of the rehabilitation process at stroke units, the physical environment has recently been highlighted as an important factor in stimulating both cognitive and social activities among patients (Janssen et al., 2014; White, Bartley, Janssen, Jordan, & Spratt, 2015). According to Harris, McBride, Ross, and Curtis (2002), the physical environment can be described as the ambient environment (e.g., lighting, noise levels, and air quality); architectural features (e.g., layout of hospital); the size and shape of rooms and placement of windows; and interior design features (e.g., furnishing and artwork). All dimensions are important for supporting care and helping patients return to health and well-being. In nursing, the concept of the environment has traditionally been referred to as all that surrounds the patient; there is constant interaction between the patient and the environment (Meleis, 2017).
Ulrich (1991) argued that to promote well-being, the physical environment should be designed to support patient care by providing a sense of control, access to social support, and access to positive distraction. Researchers have examined several areas in which the physical environment can impact patients’ health outcomes; it has been found that sound and light (Huisman, Morales, van Hoof, & Kort, 2012) as well as the ability to experience nature (Ulrich et al., 2008) can affect health and well-being. Research has also shown that high levels of attractiveness, in the form of colorful contemporary furnishings and artwork, for example, may reduce patients’ anxiety (Becker & Douglass, 2008). The physical environment can also provide opportunities for activities and social interactions, for example, by providing access to communal areas with books, games, and computers; having access to these opportunities for interaction can be an important prerequisite for recovery after a stroke (Janssen et al., 2014; White et al., 2015).
Based on the knowledge that the physical environment can contribute to health and well-being, the concept of evidence-based design has been established and is increasingly attracting attention. Evidence-based design incorporates research to achieve the best possible health outcomes for patients, staff, and visitors (Hamilton & Watkins, 2009; Ulrich, Berry, Quan, & Parish, 2010). To gain a better understanding of the importance of the physical environment, individual experiences of the environment need to be studied further. This need for research applies especially when the trend is to go exclusively to single rooms.
Around the world, new healthcare environments are built primarily using a single-room design (Joint Commission, 2018). Studies have shown that patients treated in single rooms have a lower incidence of both airborne and contact-related infections (Simon, Maben, Murrells, & Griffiths, 2016; Ulrich et al., 2008) and confusions (Caruso, Guardian, Tiengo, dos Santos, & Junior, 2014) than patients in multibed rooms. Reduced noise levels in single rooms improve communication between patients and staff (Ulrich et al., 2008). Studies have also shown that patients appreciate being cared for in single rooms because these rooms provide a personal sphere without disturbing elements (Maben et al., 2015; Persson, Anderberg, & Ekwall, 2015). However, the sense of loneliness and isolation that patients experience as a result of a single-room design compared with multibedded units is receiving more attention (Persson et al., 2015: Singh, Subhan, Krishnan, Edwards, & Okeke, 2016).
The present study focuses on patients who have suffered a stroke. Stroke can affect any neurological function, for example, it can cause visual impairment and memory loss, and it can impact a person’s daily life (Elf, Eriksson, Johansson, von Koch, & Ytterberg, 2016; Langhorne, Bernhardt, & Kwakkel, 2011). Shortly after a stroke, increased engagement in physical activities targeting mobility may result in reduced impairment (Veerbeek et al., 2014).
To live independently and manage their daily lives at home, all stroke patients should be treated in stroke units. A stroke unit is an organized and highly specialized unit that provides complete care for stroke patients and constitutes a geographically defined unit in the hospital (SUTC, 2013). A person who receives care in a stroke unit is less likely to have complications caused by immobility, such as venous thromboembolism or chest infections, compared to a patient who receives care in a general ward (Govan, Langhorne, & Weir, 2007). The care at stroke units focuses on acute medical interventions and early rehabilitation, which are provided by a multiprofessional team (Riksstroke, 2015). Stroke guidelines recommend starting rehabilitation early to regain functions such as the abilities to walk, talk, and read (Ringelstein et al., 2013; SUTC, 2013).
Research on patients at stroke units has focused mainly on aspects such as where patients spend their days as well as the types of activities and interactions they engage in (Bernhardt, Dewey, Thrift, & Donnan, 2004; West & Bernhardt, 2012). Recently, we had the opportunity to compare patients’ behavior in a stroke unit before and after the unit underwent reconstruction. The comparison showed that patients’ activities and interactions varied between the old and the new units and that these variations could be related to the difference in design. In the new stroke unit, the patients spent more time alone in their rooms, were less active, and had fewer interactions compared with the patients in the old unit. One explanation could be the transformation from mainly multibed rooms to single rooms (Anåker et al., 2017). Nevertheless, we need a deeper understanding of how the physical environment affects patients and the quality of care at stroke units (Campbell, Roland, & Buetow, 2000). A well-designed physical environment can be defined as an environment that can contribute to social, psychological, spiritual, physical, and behavioral care (Jonas & Chez, 2004). However, the physical environment’s design and its impact on health and care are rarely the focus of the studies conducted at stroke units.
In summary, a well-designed, stimulating, and attractive healthcare environment is a key factor in patient care. Observations of patients’ activities and interactions during stroke care are important; however, such studies do not reveal how patients experience an environment and what meaning they give to that environment. How patients experience the physical environment in stroke units in general, and stroke units with single-room designs in particular, remains unknown. The aim of this study was to explore patients’ experiences of the physical environment at a newly built stroke unit, and the knowledge generated by this investigation can inform the design of new stroke units.
Method
Design
The study used a qualitative design with an inductive analytic approach (Elo & Kyngäs, 2008; Krippendorff, 2004) that was applied to transcripts of semistructured individual interviews. This study is part of a larger study, where we explore different factors in the physical environment that may influence patients and staff at a stroke unit.
Setting—The Physical Environment
The criterion for a stroke unit to be included in the study was that the unit should have been newly built and subject to a more fundamental change than merely refurnishing the patient rooms and making slight surface improvements. The selected stroke unit was located in a university hospital in Sweden and was completely renovated in 2014, when it underwent several major changes in design, including the transition from a multibedroom to mainly single-room design (Figure 1).

Scheme of the selected stroke unit.
Ambient environment
All patient rooms had daylight opportunities, artificial light in the corridors, dimmer switches in bathrooms, and infrequent loud noise from the helipad on the roof of the building.
Architectural features
There were two parallel corridors with four nursing stations, two on each side. There were separate rooms for physicians and therapists. Patient rooms were mainly single, except for one room with three beds, which was reserved for acute patients in need of medical monitoring. Bathrooms were located in the patient rooms. All patients’ rooms had windows facing outside. The patient lounge was located at the end of the corridor without a visible entrance from the corridor; the lounge had windows with daylight.
Interior details
Patient rooms had white walls and gray floors. Contrasting colors (dark gray) were used around the doors and toilets in patient bathrooms. All doors to patient rooms had a window (with blinds) facing the corridors. All patient rooms had a bed and a bedside table as well as a chair and table by the window; there were no TV screens in patient rooms. There were handrails along the walls in the corridors. The patient lounge had tables with chairs and a TV screen.
Participants
Participants in the study were recruited from the selected stroke unit. Patients who met the following inclusion criteria were asked by the first author to participate in the study: a confirmed stroke diagnosis, admitted to the stroke unit for at least 24 hours, and able to give informed consent and answer questions. Patients who met the inclusion criteria were recruited consecutively. Interviews were conducted with a total of 16 patients (7 women/9 men). Two of the participants were wheelchair users. All included patients were able to visit all areas of the ward.
Data Collection
The data collection was conducted in December 2015, and in order to gain more comprehensive data, we returned to the stroke unit in February 2017. Data were collected through interviews in each patient room. The patients were either lying in bed or sitting on a chair or in a wheelchair next to a table by the window. The interviews were conducted by the first author, who sat on a chair beside the patient. To minimize the risk of excessive preunderstanding, the interviews were performed using a preprepared interview guide. According to Kvale, Brinkmann, and Torhell (2009), the use of a preprepared interview guide can reduce the risk of preconceptions that can result in incorrect analyses.
The patients were asked to describe their experience of the physical environment of their room and of the stroke unit as a whole. The following are examples of questions asked: “Could you please describe the physical environment in your room? What do you consider important factors in the physical environment in general at this unit? Could you please describe your experiences in a single room at this stroke unit?” Follow-up questions were asked in order to explore different aspects of the physical environment. The interviews were audiotaped and transcribed verbatim to text. The interviews lasted 10–37 min.
Data Analysis
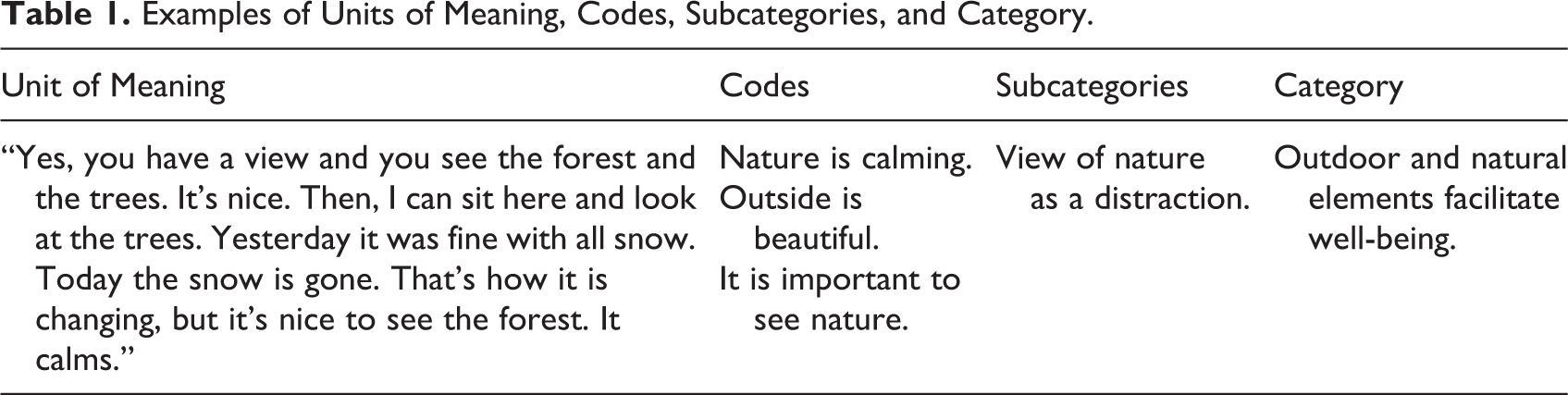
Inductive content analysis was performed according to the methods of Elo and Kyngäs (2008) and Krippendorff (2004). The transcribed text was read individually by the first and last authors several times, allowing them to immerse themselves in the data and to obtain an overall impression of the text as a whole and to identify its fundamental meaning. In the next step, a unit of meaning essential to the purpose of the study was chosen for the subsequent analysis. A unit of meaning can be either one or several sentences from the transcribed text. Focusing on the manifest content and on organizing the data, the first author coded the units of meaning. After this step, the codes were listed in higher order headings and grouped under categories and themes (Elo & Kyngäs, 2008; Table 1). To achieve trustworthiness (Shenton, 2004) in the present study, the analysis moved back and forth among the interviews, codes, subcategories, and categories to validate the results. The researchers discussed each step of the analysis until consensus was achieved. Furthermore, clarifying representative quotations from the interviews were added to the results to strengthen the credibility of the analysis. During the analysis, the authors critically reviewed, thoughtfully considered, and reflected on the findings in light of their preunderstandings.
Examples of Units of Meaning, Codes, Subcategories, and Category.
Ethical Approval
The study was approved by the regional ethical review board in Uppsala (permit numbers: EPN No. 2012/199). The patients received written and verbal information on the study and signed a written informed consent prior to each interview. The patients were informed that the interviews would be recorded. The researchers were not employed at the participating unit.
Results
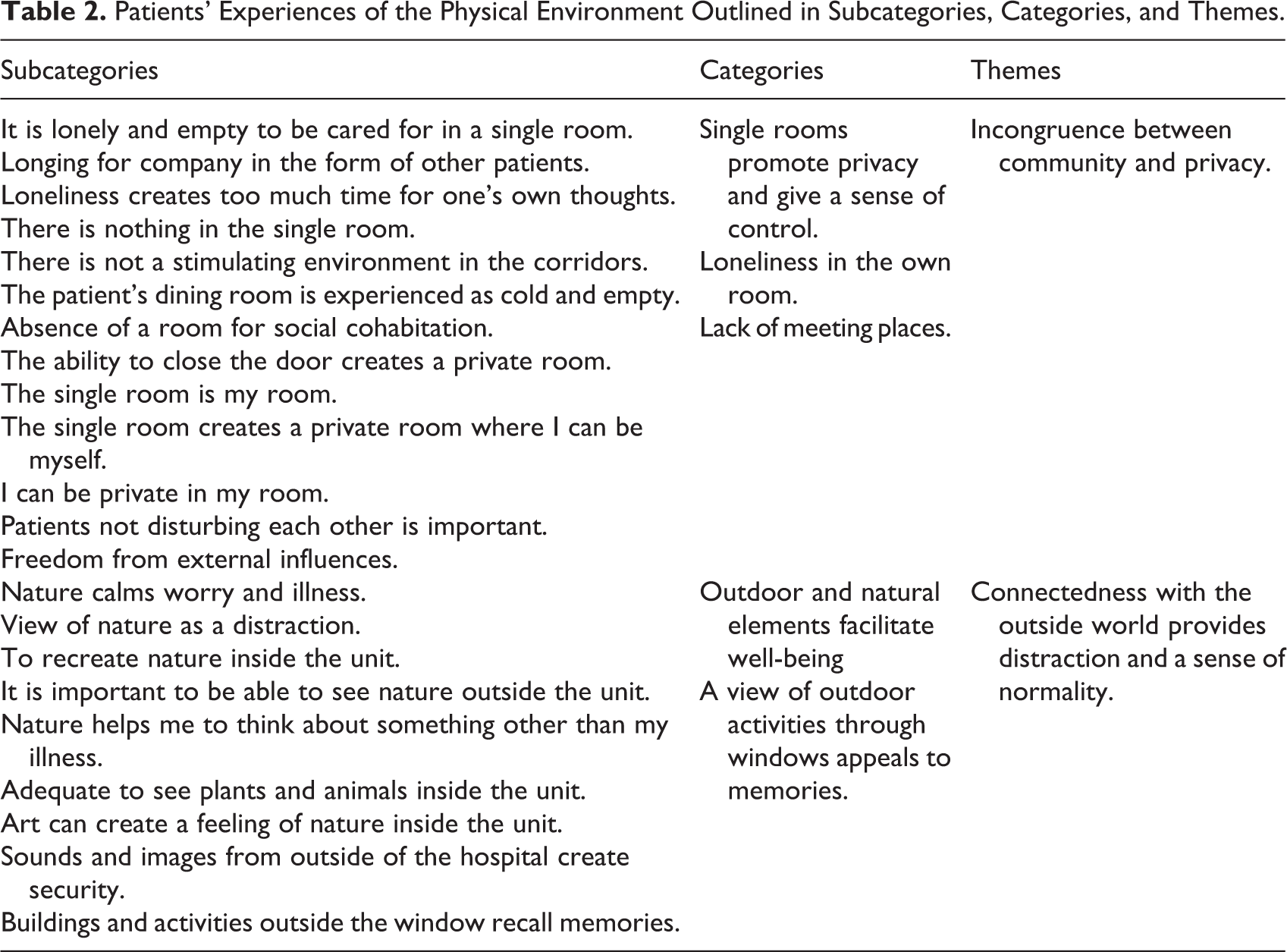
A total of five categories emerged in two themes and described how the patients at the stroke unit experienced the physical environment: (i) incongruence between community and privacy and (ii) connectedness with the outside world provides distraction and a sense of normality (Table 2). The categories are presented below and discussed using quotations from the interviews.
Patients’ Experiences of the Physical Environment Outlined in Subcategories, Categories, and Themes.
Incongruence Between Community and Privacy
Single rooms promote privacy and give a sense of control
The patients described their single rooms as a space of privacy. Controlling their own room was cited as central to the patients’ perception of their care. The patients described control as the opportunity to close the door and cut out all sounds from the corridor and other patients at the unit. Controlling their own room was described as an important part of patients’ experience of care at the stroke unit.
Furthermore, the single room was considered one’s own home. The patients compared their room to a home, and this created a sense of privacy that was highly valued: “It will be like my room. You close the door. It’s like my home. I feel better then, that’s fine. I don’t feel ill.”
Patients also described how it was easier to sleep at night without disturbing persons in the room, and thus, their sleep improved. One patient put it as follows: “It’ll be my own room and then it’s easier to sleep. You don’t have to hear the others when they sleep, snore and so on.”
Loneliness in the own room
Patients expressed that the time spent in their own rooms consisted of many long hours of loneliness, a loneliness that in itself created a feeling of emptiness. They were aware that if they wished, they could leave their own rooms and go to the patient lounge to find company and community. However, their choice was to stay in their own single rooms: “I have no company now. It’s clear that I can go to the lounge. But, many are ill there. Maybe it’s hard for them to talk so I stay here in my room. But, it’s lonely.”
Patients addressed the lack of color, art, television, and furniture. They described how difficult it was to make time pass when you have nothing to look at. Additionally, the patients expressed that the room could have been designed to be warmer and more welcoming, for example, by adding more color and art on the walls in the room; these changes would have reduced loneliness. Together, the lack of interior details and the lack of other patients created an empty room where it was difficult to make time go faster.
Patients expressed that they missed having someone to talk with. They described this situation as if there were no opportunity to share the day with another person, and there was too much time for their own thoughts. These thoughts often concerned their own bodies, both physical and mental: “I think it would be great to have meet-ups with someone else. Then, I’m happier and that’s good. Now there’s so much time for thought. I’m alone.”
Furthermore, patients described how during the day, very few people visited the patient rooms; visitors could have broken up the sense of loneliness.
Lack of meeting places
Patients described a longing for social places in the communal areas at the stroke unit. The existing communal environment, in the form of a patient lounge, was described as sterile and empty: “There’s a chair and table and a TV. Nothing more. There’s nothing. It’s quite sterile in there. It’s just the tables. And then you may not be able to watch TV, then some get disturbed.”
The patients described a desire for a communal room or meeting place that provided an opportunity to meet other patients; they believed that such a room—or a similar place in the corridors—could reduce loneliness. The patients talked about their wishes for social spaces that invited people to converse with other patients: “Should there be a sofa? Then, I could meet the other women. However, many people are very ill. Nevertheless, it would be nice to have a nice room to meet other people. Then, it would not be that lonely.”
Connectedness With the Outside World Provides Distraction and a Sense of Normality
Outdoor and natural elements facilitate well-being
The ability to sit by the window and look out to the forest and nature was described by the patients as creating a sense of serenity. A patient described nature as a distraction that allowed one to think of something other than hospitalization and illness itself. Being able to glance at the living trees and the weather’s changes during the day was experienced by the patients as calming. Yes, you have a view and you see the forest and the trees. It’s nice. Then, I can sit here and look at the trees. Yesterday it was fine with all snow. Today the snow is gone. That’s how it is changing, but it’s nice to see the forest. It calms.
Patients talked about their longing for art with illustrations of nature in the patient rooms, in the corridors, and in the patient lounge. They thought the images should reflect landscapes, forests, or water: “I miss a painting. Morning sun or evening sun, the forest or water, a beautiful painting.”
A view through windows on outdoor activities appeals to memories
Patients expressed a desire to see and understand what was going on with regard to activities taking place outside their own windows. Patients described how looking at, for example, cars, people, and construction workers outside the window, offered distraction from what was happening inside the unit itself. Construction sites and traffic on roads outside the window recalled memories of previous occupations. The sound itself could recall memories of one’s work: “I hear them working out there. It reminds me of my work. When people work, that’s fine. The noise, the drilling resembles my old mining job. Then, you feel the action. I miss my job.”
Additionally, having a view of outdoor activities through the window was described as something that offered a different focus and could act as a distraction from one’s own illness. Real life was going on outside the unit, in contrast to life inside the walls of the hospital, which felt like it was not part of normal life.
Discussion
This study explored patients’ experiences of the physical environment focusing on the design of a newly built stroke unit with a single-room design. We sought to understand patients’ experiences of the physical environment from their perspective. The main findings primarily revealed how having a single room gave the patients a sense of control by offering privacy. However, social interaction was absent in the single rooms and instead the patients experienced loneliness. Another key finding was that patients experienced positive distraction when they looked at nature or at activities that went on outside their windows.
A prominent finding was that most participants felt that the single-room design could be both a facilitator of privacy and a barrier to reducing loneliness in the unit. Patients in our study highly valued the privacy that the single room provided, a privacy that gave them a sense of control. However, at the same time, the patients asked for communal areas where they could meet other patients, talk, and watch TV. Patients expressed the desire for both community and privacy to be included in the design of the same physical environment. This incongruence is a challenge for those involved in the planning and design processes of new stroke units (e.g., architects, other designers, and healthcare professionals). In light of Ulrich’s (1991) theory of supportive design, that is, designs that render a sense of control, possibilities for social support, and positive distraction, our findings suggest that both community and privacy to be included in the design of the same physical environment.
Patients reported being lonely in rooms of their own, and this issue was mentioned repeatedly by the majority of the patients interviewed. The patients said that being cared for in a single room was lonely and empty and that they had no one to talk with during the day. This is consistent with the findings of several studies (Maben et al., 2015; Persson et al., 2015; Singh et al., 2016), indicating that patients felt lonelier in single-room units compared to multibedroom units. Generally, older people felt lonely in the community, but loneliness increased following admission to single rooms—a loneliness that could be described in terms of reduced social interaction, lack of companionship, and less surveillance by nursing staff (Singh et al., 2016). This feeling of loneliness should not be ignored by healthcare. Negative health outcomes linked to loneliness include disability, cognitive decline, and depression (Gray & Worlledge, 2016; Lund, Nilsson, & Avlund, 2010). Even if the experiences and consequences of loneliness can vary greatly, it is worth considering whether there are design parameters in the physical environment itself that can reduce loneliness.
To reduce patient experiences of loneliness in individual rooms while maintaining the single-room’s unrivalled opportunity for integrity and privacy, new ways of designing the physical environment are required, as are new ways of developing the care process. Within the care process, staff need to consider carefully how they support patients in this new type of physical environment, that being single-room accommodation, and manage patients so that they are less lonely by enabling visits to other areas in the unit. In order for the healthcare professionals to make a good assessment by way of an analysis of patient status, the new single-room design requires more frequent visits on the part of healthcare staff to the patients.
The lack of social interaction in a single room can make the patient feel alienated from what is going on outside that room. Given the radical spatial shift in healthcare to a single-room design, which has been followed by a system of organization where staff actively work closer to the patient and conduct more staff–patient interactions bedside in the individual patient’s room, it is vital to consider ways to reduce loneliness. To encourage patients to visit communal areas and thus possibly reduce loneliness, architects and other designers can follow several design principles. According to International Health Facility Guidelines (2018), wayfinding principles include, for example, creating a unique identity at each location at the unit, using landmarks and sight lines in the corridors, and giving rooms in the unit different types of visual character. Furthermore, we suggest that to reduce the sense of loneliness and create more opportunities for social interactions, the design of the physical environment needs to include more variation. It could be valuable to create several small areas (instead of one large patient lounge) with groups of furniture where patients could sit and meet others. Reducing corridor lengths is another way of changing the environment, as is providing small areas for meetings and socialization around the unit.
The patients in our study commonly expressed that they wanted a more encouraging environment with art, television, and inviting furniture in corridors and patient lounges. In general, patients at a stroke unit need environments that motivate them to engage in activities, thereby reducing the risk of complications and impaired functioning. Today, the recommendation is that patients be active when undergoing rehabilitation (Dobkin & Dorsch, 2013). We know from previous research (Janssen et al., 2014; White et al., 2015) that access to communal spaces is important because it creates the possibility of social interaction, which is important for poststroke recovery. There is a need for places that draw the patient out of the single room toward activities in the unit. Rosbergen et al. (2017) have shown that an embedded enriched environment at stroke units, such as that created by communal areas with various types of stimulation equipment (games, iPads, music, and magazines), increased physical, social, and cognitive activity. Communal dinners were also shown to increase such activity. As we build more stroke units with only single rooms, it is essential to ensure that patients have access to other spaces such as communal areas, spaces that draw them out of their single room.
The findings of our study also revealed the importance of connecting the patient to the outside world. In line with Ulrich’s (1991) theory, nature provides a positive distraction from being a patient in a stroke unit. However, at the same time, our study indicates that positive distraction can be provided also by a view on activities (and in that sense extends Ulrich’s theory). The patients in our study described how sitting at the window and having a view of nature or of activities in the streets and buildings distracted them from their care at the unit. The world outside is a world of normality, in contrast to life inside the hospital, which is seen as not normal. For the patients in our study, connectedness with the outside world could include both viewing the outside world and also incorporating nature into design elements at the stroke unit. Both approaches are described as important for helping patients to think about something other than their illness.
Patients’ explicit request for visual exposure to nature needs to be taken into account when designing new stroke units. Viewing nature and having access to natural environments seems to result in lower blood pressure and lower heart rates (Fich et al., 2014; Tang & Brown, 2006) and ultimately has a restorative effect on patients (Ulrich, 1991; Ulrich et al., 2008). Designing a physical environment with access to nature and the outside world is therefore fundamental for achieving quality in care. Consequently, how patients experience the physical environment is important when designing new stroke units. In line with the concept of evidence-based design, patients’ experiences need to be part of the planning and design process (Hamilton & Watkins, 2009). Outdoor and natural elements in the physical environment as well as design elements that reduce loneliness need to be included when designing new stroke units. People and the environment are truly intertwined, making it even more important that further research is conducted from the perspective of all people—patients, staff, and visitors—who are part of the healthcare environment.
Limitations
The sample in this study was small (n = 16) and from only one stroke unit. However, small sample sizes are typical for qualitative research, where the focus is on richness rather than representativeness. While the small sample size may limit the transferability of the findings to other similar stroke unit contexts, the experiences of the patients in this study provide valuable insights that could deepen knowledge about the physical environment of stroke units in general. Further exploration of this topic is warranted and should include a larger sample of participants from several stroke units with different designs of the physical environment.
Another limitation (or challenge) of this type of research is that people could have difficulty verbally describing their experiences of space. To deepen and enrich the interviews, further research is needed that includes a variety of designs and methods.
Conclusion
Patients with stroke require a physical environment that supports care and rehabilitation. The physical environment should always be considered from the user’s perspective. This study highlights potential areas for architectural improvements at stroke units, primarily focusing on the design of communal areas with meeting places and on creating possibilities to be part of the world outside the unit. A future challenge is to design stroke units that include both community and privacy. Listening to patients’ experiences of the physical environment can be a starting point in the design process and a step toward ultimately improving care.
Implications for Practice
When improving the physical environment to achieve quality of care at stroke units, patients’ experiences of the physical environment (as explored by interviews) are central and could be valuable in the design process. To reduce loneliness, stroke units should be designed to enable patients to visit communal areas where they can experience social interactions and have access to a stimulating environment that includes, for example, books, games, and computers. Design components that both allow patients to view the outside world and include natural elements in the physical environment should be considered when designing new stroke units.
Footnotes
Acknowledgments
The authors would like to thank the Swedish Research Council Formas, the Swedish Stroke Association, the Doctoral School in Health Care Sciences at Karolinska Institutet, and Dalarna University research area Health and Welfare for supporting this study with research funds. The authors thank Asgeir Sigurjónsson for the illustration of the stroke unit.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.