
Abstract
Aim:
To investigate how product design can be used to improve parent–infant bonding in a neonatal intensive care unit.
Background:
Impaired parent–infant bonding is an inevitable consequence of premature birth, which negatively influences development. Products, systems, or services that support the bonding process might counter these negative influences.
Method:
The first step was to trace existing products by performing a literature search in PubMed, the university library, and Google. The identified existing designs were then used in semistructured interviews with nurses and parents to get insights into their desires and recommendations for product design to enhance bonding. Interviews contained open questions and a multiple-choice questionnaire based on the literature search.
Results:
In total, 17 existing design types were used in interviews with 11 parents and 23 nurses. All nurses explicitly stated that practicality was the first criterion designs aimed at enhancing bonding definitely had to meet. All parents indicated that they would like to use a design to enhance bonding if that would contribute to their child’s health and development. For both parents and nurses, the most valuable way to enhance bonding seemed to be products to improve Kangaroo care; however, their specific desires varied substantially. Therefore, seven recurring themes were defined, resulting in nine general recommendations and six opportunities intended to enhance parent–infant bonding.
Conclusion:
This study provides design recommendations and opportunities based on parents’ and nurses’ expert opinions. Designing to enhance bonding is considered valuable; however, designs should match the stakeholders’ desires and conditions.
Worldwide, an estimated 15 million babies are born prematurely every year and this is still increasing (World Health Organization, 2015). Babies born before 37 weeks of gestation are considered premature infants, and babies born before 32 weeks of gestation are considered very preterm. Very preterm and critically ill babies are admitted to a neonatal intensive care unit (NICU), where neonatologists and specialized NICU nurses can provide the necessary medical care to those infants 24 hr a day. Nonetheless, the many unnatural stimuli that babies are exposed to in an NICU, such as tubes, patches, noise, bright lights, and painful procedures negatively influence development. Moreover, the impaired parent–infant bonding caused by those unnatural stimuli and separation from the parents also significantly affects hormonal, epigenetic, and neuronal development (Kommers, Oei, Chen, Feijs, & Bambang Oetomo, 2016).
According to neuropsychologists and psychobiologists, bonding is a process of coregulation: when an individual uses his or her capacity to regulate the internal environment of others as well as themselves. In order to do so, organisms sense cues that reflect the other’s internal environment and respond to those cues. Cues are for instance facial expression and voice, but also heart rate, temperature, skin color, and scent (Kommers et al., 2016; Kommers, Oei, et al., 2016). Every organism has appropriate sensitivities to send and perceive cues (Fleming, O’Day, & Kraemer, 1999), but in preterm infants, cues are scarce and difficult to recognize. Due to their physical immaturity, they are less capable of expressing their internal state. Parent–infant bonding is thus disturbed in a period of time when this is actually needed the most (Kommers, Oei, et al., 2016). Currently, awareness of the problem is growing, and therefore, hospitals are more inclined to increase family participation. In other words, daily caregiving becomes more and more centered around the entire family, a philosophy called family-centered care (Altimier & Phillips, 2013).
This philosophy acknowledges that, over time, the family has the greatest influence over an infant’s health and well-being (Altimier & Phillips, 2013). Medical staff is therefore encouraged to partner with parents, teach them how to understand their baby’s behavioral cues, and provide information about developmentally appropriate positioning and handling. Family-centered care is now recognized as an essential attribute of high-quality neonatal care, and it is intended to improve quality of life for high-risk preterm infants and their families (McGrath, Samra, & Kenner, 2011). One of the most important features of family-centered care is promoting and facilitating Kangaroo care.
Kangaroo care is when a diaper-clad infant is placed on the naked parental chest, enabling optimal parent–infant coregulation or bonding (Kommers et al., 2017). In addition to reducing infant crying and fussiness, it has shown to significantly reduce mortality and morbidity, to increase weight gain, and to improve temperature regulation, breast feeding, and parent–infant bonding (Cho et al., 2016; Conde-Agudelo, Belizán, & Diaz-Rossello, 2012; Kommers, Oei, et al., 2016). In spite of these well-known beneficial effects, the time that parents spend kangarooing is often limited due to several reasons, such as older siblings at home that need attendance and restricted parental leave for fathers and in some countries both parents (Feeley, Genest, Niela-Vilén, Charbonneau, & Axelin, 2016). Complementary approaches that could benefit bonding and hence improve the development of preterm infants have therefore been described.
Research suggests that the use of parental odors can reduce stress and provide comfort to babies in the NICU (Croes, Chen, Feijs, & Bambang Oetomo, 2012). Furthermore, exposure to maternal sounds within the incubator resulted in promising effects (McMahon, Wintermark, & Lahav, 2012). However, such strategies are still not implemented or used routinely within NICUs. A reason for this might be that stakeholders’ desires are not described clearly in literature.
The purpose of this research was to investigate the opinions of parents and nurses on product design to enhance parent–infant bonding and to thereby discover design opportunities. We wanted to answer the question: “How can design be used to improve bonding between parents and their premature babies admitted to the NICU?” In this study, design refers to product design and design features of products. In order to do this, we first performed a literature search to identify both existing designs and items for a questionnaire to evaluate designs. Consecutively, the existing designs were shown to stakeholders in interviews in which they also completed the newly developed questionnaire. Finally, design recommendations and opportunities were derived from their expert opinions.
Method
Literature Search and Questionnaire Development
The electronic databases of PubMed, the university library, and Google were searched for the search terms “premature infant OR preterm infant OR neonate OR NICU OR parents, AND senses OR interventions OR bonding OR design” in the title or abstract. All abstracts found in PubMed and the university library and the abstracts on the first 10 Google pages of each of the 20 search term combinations were screened. Articles were considered relevant when the main topic was related to bonding, effects of an NICU stay on parents, and the influence of different senses on bonding: hearing, touching, tasting, scenting, seeing, or designing to enhance bonding. These criteria resulted in 34 articles and 17 Internet hits to be read full text, including their reference lists to search for additional relevant papers. In the end, 16 articles were included that described a design, system, or service to enhance parent–infant bonding at an NICU. An image and description of each design, system, or service was then printed and laminated to use in a semistructured interview with the stakeholders (Figure 1). Designs or services that turned out to have similar concepts were grouped.
Laminated cards.
Finally, the purposes of the designs (e.g., improving comfort or enhancing communication) were used to form items for a questionnaire to evaluate bonding-enhancing interventions in the interview. Nine items were defined, all containing a positive statement with respect to a design. Every statement could be ranked 1–5, with 1 indicating totally disagree and 5 indicating totally agree (Appendix). The medical ethical committee of the Máxima Medical Center has approved this study.
Study Setup
All nurses working in an NICU and all parents having one or more preterm babies admitted to our NICU were suitable for the interview. Families were recruited with help from the nurses, they indicated which families were eligible and asked them whether they wanted to participate. Each interview with parents took place in their single NICU room, to ensure privacy and to not unnecessarily separate parent and child. Interviews with nurses took place in an NICU office to ensure privacy. In the first phase of the interview, the researcher asked the participant to look at the laminated cards and to pick out those which the participant considered interesting. Each participant was allowed to choose their own laminated cards, to not bias them toward specific products. Thereafter, semistructured open-ended questions relating to advantages and disadvantages of each chosen design were asked. These open-ended questions were used to help each participant to openly share their personal opinions. In the second phase, the participant was requested to fill in one questionnaire per chosen design, resulting in a total interview duration of 20–30 min. To warrant privacy, interviews were not audio taped, but the interviewer took extensive notes during every interview. All notes were transcribed into a digital, anonymous document immediately after finishing.
Data Analysis
To become familiar with the data, all interview transcripts were read twice. During the second read, data pieces were coded to identify recurring themes. The themes could help answering the question how to use design to enhance parent–infant bonding in NICUs. Additionally, the questionnaires were analyzed, and every design was given a score depending on how the participants ranked the interventions. The outcomes of the questionnaires were summarized in tables. Finally, by combining the results from the literature search, the recurring themes, and the questionnaires, design recommendations and opportunities based on the stakeholders’ opinions were described.
Results
Existing Designs and Concepts
Throughout the literature search, 17 design types intended to enhance bonding between parents and premature babies were found (Table 1). The interventions were divided into three categories: (1) interventions facilitating or simulating aspects of Kangaroo care, (2) interventions exposing infants to parental stimuli or vice versa, and (3) interventions facilitating the communication between parent and infant while they are physically separated.
Existing Designs to Enhance Bonding.
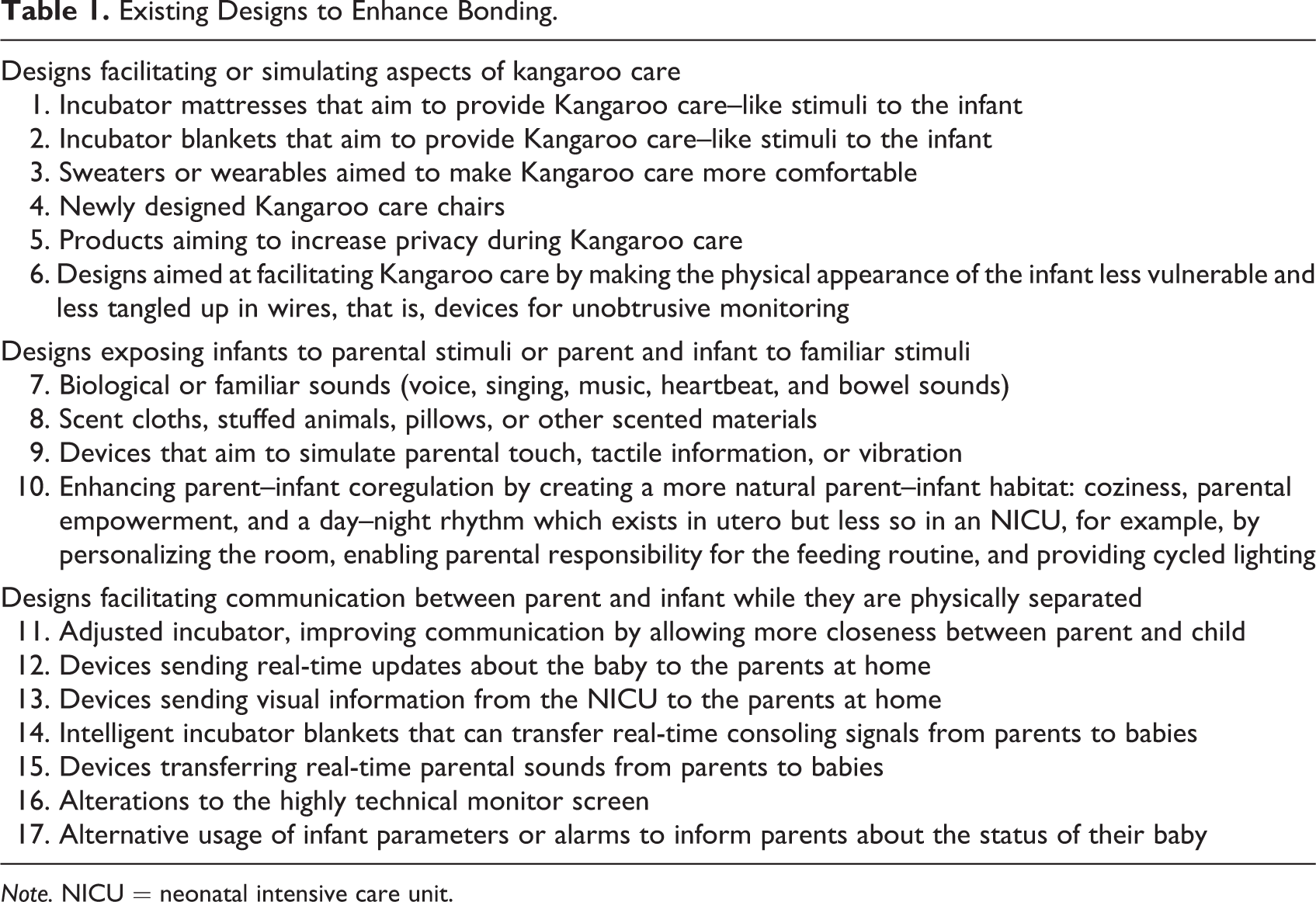
Note. NICU = neonatal intensive care unit.
Interview Outcomes
In total, eight mothers, three fathers, and 23 nurses were asked to give their opinion about the designs presented in the cards. When rereading the transcripts of their interviews, seven specific themes were identified, three of those themes were mentioned by parents and four by nurses. Recurring themes in the interviews with parents were enhancing bonding by the use of a design, receiving their child’s information at a distance (communication technology), and improving the appearance of the NICU environment. Recurring themes in the interviews with nurses were practical issues, empowering parents within the bonding process, communication technology, and improving the appearance of the NICU environment for parents and infants admitted to the NICU.
Parents: Enhancing Bonding by the Use of a Design
All parents indicated that they would like to use a design to enhance bonding if that would contribute to their child’s health and development. Parents considered it valuable to have their heartbeat or voice recorded, their scent absorbed, their temperature used, or other features transferred to their baby. “During Kangaroo care she can hear my heartbeat, so transferring my heartbeat to her is probably a good thing.” There were specific benefits to the parents as well, “Having my child listen to my heartbeat when I am not performing Kangaroo care would make me feel empowered.”
Parents: Communication Technology (Communication at a Distance)
In total, 7 of the 11 participating parents mentioned that communication devices could make them feel stressed. “Even at home everything already revolves around the fact that our baby needs to be in the NICU. We do not need to be reminded of that all the time.” Another mom stated: “Knowing that my baby is not doing well and not being able to physically be with him makes me feel sad.”
Nonetheless, 9 of the 11 parents expressed their desire to know how their child is doing when they are not around. One parent stated the desire to see his baby, “It would be nice if you can log on to a system before bedtime to see that she is sleeping peacefully.” In addition, another parent would like to respond to her baby as well, “Being able to respond to my child at a distance would definitely be valuable for me.” Two of the 11 parents indicated that they would definitely not like to use communication devices since this would cause stress and obsessive behaviors. One of them mentioned the importance of being physically present, which might be discouraged by implementing a communication device. Seven of the 11 parents were afraid to use communication devices at the wrong time, for instance, when their infant is sleeping, which is disturbing for the child’s development. Furthermore, some parents feared that their child would receive too many stimuli or that their child would associate their communication at a distance with stress when communication occurred in a stressful situation. Nine of the 11 parents indicated that they would like to have a visual image of their baby additionally to other communication technology.
Parents: Improving the NICU Environment
All parents were open to designs aimed at improving their own as well as their baby’s NICU environment to enhance comfort in the NICU, for instance, products that facilitate Kangaroo care or products that make the appearance of the room or incubator friendlier. Seven of the 11 participants were interested in products that improve comfort during Kangaroo care. Parents mentioned that they would like to have more privacy, less cold stress for their babies during transfers, more stability for the baby, and to see their baby’s face better while performing Kangaroo care. “Using a mirror while performing Kangaroo care benefits bonding since you can see your child and even make eye contact, and that is a very special moment.”
Three of the 11 participants mentioned that they are distracted by or obsessed with the monitor.
Nurses: Practical Issues
All nurses came up with practical issues regarding designs to enhance bonding, including hygiene, washing, and ease of use. They explicitly stated that practicality was the one and only criterion these designs definitely had to meet.
Nurses: Empowering Parents
Almost all nurses (20 of the 23) emphasized the importance of empowering parents within the bonding process. The nurses mentioned that parents can actively contribute to their baby’s health by being there to comfort and soothe their baby as much as possible, for instance, by performing Kangaroo care. “Parents are the best at soothing their own baby.” All nurses mentioned the latter as a scientific fact; they all feel that babies can benefit from being exposed to parental stimuli in their incubator. “It is scientifically proven that parents’ scent, sound, heartbeat, and warmth have a positive influence on the baby’s development.”
Nurses: Communication Technology (Communication at a Distance)
Eight of the 23 nurses thought communication devices contradict the philosophy of family-centered care. Some nurses explicitly stated they were afraid that communication devices might create more distance because parents could tend to stay away more often. Ten of the 23 nurses were afraid that parents would communicate to their baby at the wrong time. According to nurses, communication from parent to child at a distance should only be possible at the right time, for instance, communication should not take place during sleep and nursing care. Additionally, 14 of the 23 nurses believed that communication devices might cause stress for some parents, and 11 of the 23 nurses thought communication devices would interrupt their workflow. “When parents receive information about their child, but do not see what is happening, they are likely to call the NICU. These camera-calls are not our priority.” Another nurse added: “Imagine a mother talking to her baby all the time, that would drive me crazy!” Furthermore, nurses underlined the importance of ease of use. “Using a device should be easy, we are no technicians!” On the other hand, 11 of the 23 nurses considered visual information from babies to parents both joyful and educational; parents would learn about the child’s mimicry and body language.
Nurses: Improving the NICU Environment
Ten of the 23 nurses indicated that stress could be reduced by optimal positioning and support of a baby’s movement. “If children are supported in their posture, they experience less stress.” More than half of the nurses (12 of the 23) believed that product design could help to improve Kangaroo care. According to them, it should be investigated how more privacy, security, warmth, or a longer duration of Kangaroo care with optimal skin-to-skin and eye contact could be enabled by design. “There is nothing like real human contact.” One nurse even opted for continuous Kangaroo care. “I think it would be best for the baby when parents perform Kangaroo care longer and more frequently, preferably 24 hours a day.”
Outcomes of the Questionnaires
The frequency with which stakeholders chose a certain design differed. Tables 2 and 3 represent how frequently a particular design type was chosen, and what the mean score and the specific scores for that design type were. In summary, designs from all three categories (facilitating Kangaroo care, designs using parental stimuli, and communication devices) were selected during the interviews for various reasons. Designs that aimed to facilitate Kangaroo care were considered interesting and advantageous by both parents and nurses. Communication devices were also chosen frequently, but they scored high scores (desired) as well as low scores (undesired).
Results Questionnaires, Parents.
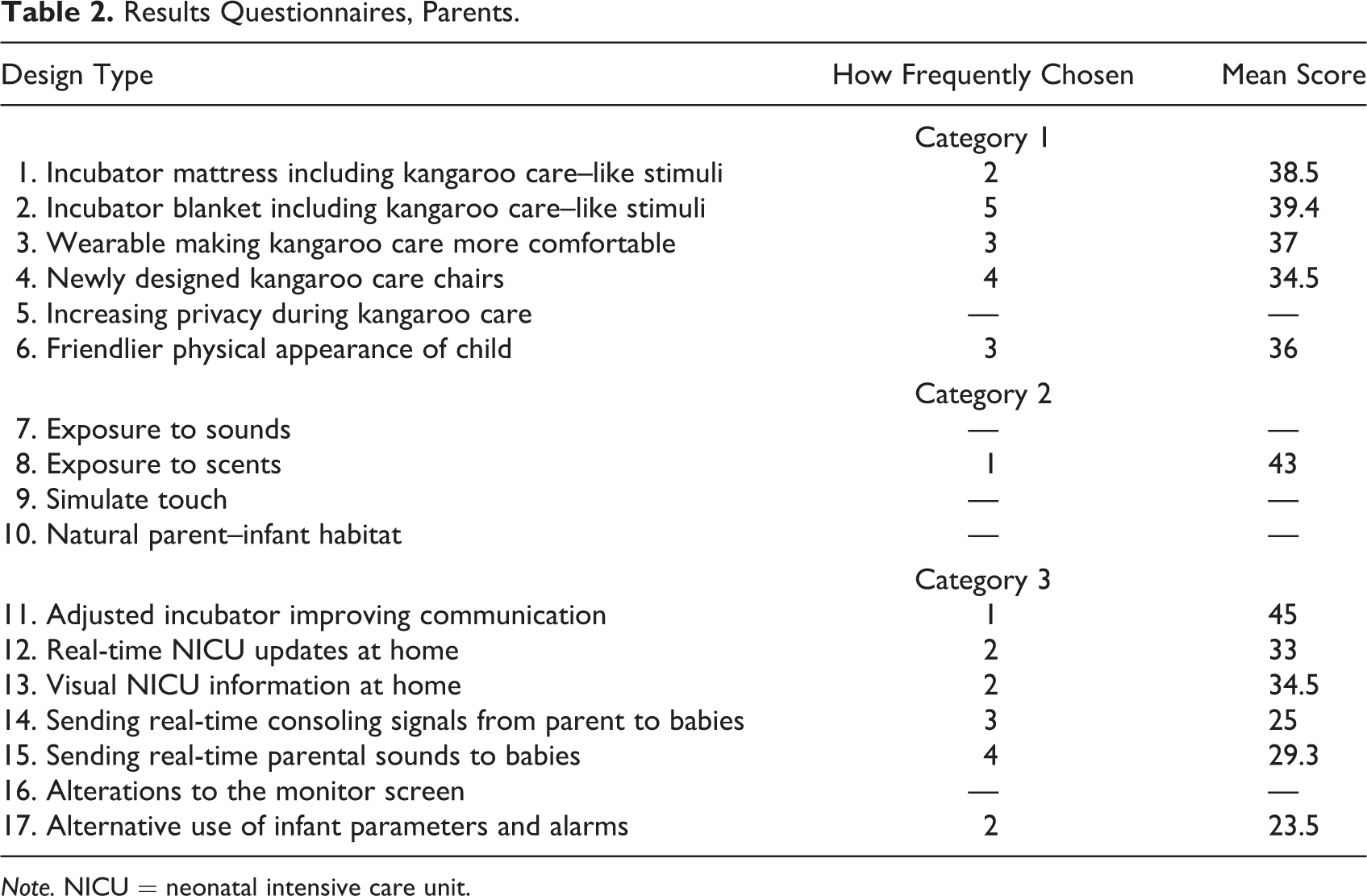
Note. NICU = neonatal intensive care unit.
Results Questionnaires, Nurses.
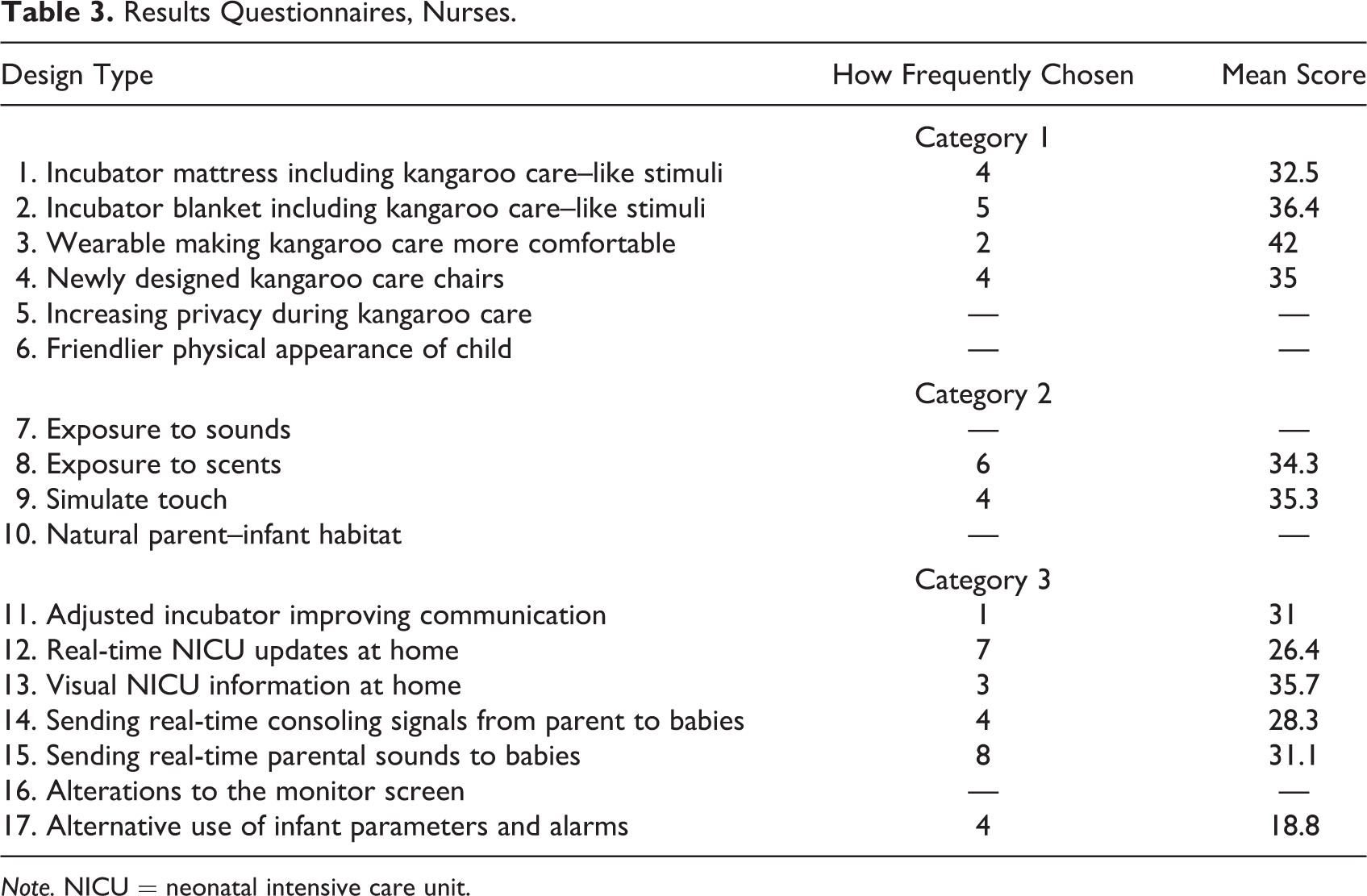
Note. NICU = neonatal intensive care unit.
Design Recommendations and Design Opportunities
The literature search and interview analyses resulted in the following design recommendations and opportunities.
Design Recommendations
The design should directly or indirectly support parent–infant bonding.
The design must be safe.
The design must be hygienic and easily cleanable.
The design should not interfere with the workflow of the nurses and therefore should not require complex knowledge of technology.
It should be minimally stressful to apply or implement the intervention for nurses, infants, and parents.
The intervention should empower parents, allowing and motivating them to contribute actively to the well-being of their child.
It should be optional to use (certain features of) the device, instead of required, that is, it should be possible to switch off (certain features of) the device at any time.
Communication devices must not interfere with infant development.
Communication devices should be adjustable to the individual needs of infants and parents.
Design Opportunities
Improve interaction between parent and infant, preferably develop designs that are tailor-made, that is, suitable for the individual preferences for each parent–infant interaction (e.g., during Kangaroo care).
Facilitate appropriately timed communication at a distance.
Use design to minimize infant stress and empower parents, for instance, an unobtrusive monitoring design which reduces stress and number of wires enabling parents to perform transfers from the incubator to their chest independently.
Improve the parent–infant interaction using the monitor, instead of having the monitor cause distraction.
Find ways to provide more privacy, security, or warmth during Kangaroo care or enable a longer duration of Kangaroo care with optimal skin-to-skin and eye contact.
Use design to increase parental involvement in the bonding process, in line with the philosophy of family-centered care, for example, an app to capture and emphasize joyful moments during an NICU stay.
Discussion
In the current study, design recommendations and design opportunities to enhance parent–infant bonding in NICUs were assessed by performing a literature search and semistructured interviews. Existing designs were identified with the literature search and used as the topic for the interviews. In total, 17 design types were identified, and 11 parents and 23 nurses were interviewed about these designs. Both stakeholder groups reported different recurring themes in the interviews.
All parents indicated that they would like to use a design to enhance bonding if that would contribute to their child’s health and development. All nurses mentioned practicality as a condition; designs should be hygienic, properly washable, and easy to use. Most nurses emphasized the importance of empowering parents within the bonding process, and for both parents and nurses, the most valuable way to enhance bonding seemed to be designs to improve Kangaroo care. Indeed, Kangaroo care has been described as one of the most effective interventions in the NICU for the care of both preterm infants and parents and the most natural intervention leading to improved regulation, that is, bonding (Carbasse et al., 2013; Cho et al., 2016; Conde-Agudelo, Belizán, & Diaz-Rossello, 2012; Kommers et al., 2017; Kommers, Oei, et al., 2016). Additionally, studies have shown that exposure to maternal sounds and music therapy improves the weight gain of preterm infants (Zimmerman, Keunen, Norton, & Lahav, 2013). Moreover, such stimuli have a favorable effect on respiratory rate (Bieleninik, Ghetti, & Gold, 2016) and they facilitate parent–infant attachment (Zimmerman, McMahon, Doheny, Levine, & Lahav, 2012). Also, the exposure of maternal or parental odors to preterm infants possibly has a positive effect on both stress reduction and the comfort of babies admitted to the NICU (Croes et al., 2012). Designs employing (some of) these features may thus be helpful for enhancing parent–infant bonding in NICUs, as was also demonstrated by our literature search and the conducted interviews.
This study showed less consensus about communication devices. Parents as well as nurses expressed contrasting thoughts regarding those. Some considered these devices as promising and stated they would be willing to use them. Others merely saw hazards when using communication devices in NICUs, including increased stress, obsessive behaviors, and possible interference with the babies’ development and the nurses’ workflow. This is in agreement with literature; parents emphasize the importance of constant information and wanting to know what is going on, but information from within the noisy, crowded NICU environment with its monitors and alarms can also be a source of distress (Aagaard & Hall, 2008). The information gathered in both literature and interviews was used to provide an overview of design recommendations and opportunities as an inspirational tool for designers. However, the study does have limitations worth mentioning.
Each participant was allowed to choose their own preferences out of the literature-researched designs, but the use of these existing designs in the interviews may have imparted bias onto the study results. Another limitation might be the fact that the study captures broad recommendations instead of concrete or specific recommendations. The reason for this is that the variety in interview outcomes in our study clearly showed that the challenge for designers lies in creating a device that can be adjusted per individual and from moment to moment, to be able to satisfy all stakeholders. These heterogeneous outcomes were obtained in a fairly homogeneous group. All participants were habituated in the same region and admitted to, or working in, the same hospital, which already has a strong focus on parent–infant bonding. This potentially reduces generalizability of the results. However, participants did differ with regard to their family settings and whereabouts, for instance: for some parents, this was their first baby, whereas other parents already had children, and some parents were rooming in, whereas other parents stayed at the Ronald McDonalds house or at home. Despite that, it would be interesting to repeat the study in a more heterogeneous population, including multiethnic groups with widely diverse socioeconomic standings. Moreover, in the longer term, user tests including prototypes will be required in order to gain insights into the value and effectiveness of devices designed according to the design recommendations and opportunities.
Future Implications
This study demonstrates that designs could be used to improve parent–infant bonding in NICUs according to both nurses and parents. For instance, bonding might be improved by a design facilitating parents to leave something personal inside the incubator or a design changing the incubator from a barrier into a temperature regulating tool that additionally invites parents for well-timed interaction with their child. In addition, based on our results, enabling parents to easily see their baby’s face continuously during Kangaroo care would also enhance bonding. Also, some parents might want the opportunity to communicate with their child at a distance, which could be achieved by a telephone app. Such an app could allow parents to receive a visual image of their baby and send their voice and heartbeat live to the NICU at appropriate times. Finally, some broader steps could be taken, such as codifying recommendations for product design for NICUs via the Standards for Newborn ICU design (White, Smith, & Shepley, 2013). The Standards for Newborn ICU Design contains recommended standards with respect to family space, hand hygiene, lighting, and other aspects of NICU design. Implementing product design recommendations to enhance parent–infant bonding may therefore be relevant in the future.
Conclusion
Impaired parent–infant bonding is an inevitable consequence of premature birth, which negatively influences development. Research suggests that enhancing parent–infant bonding by, for instance, the use of parental stimuli can enhance development. However, such strategies are still not implemented or used routinely within NICUs. A reason for this might be that stakeholders’ desires are not described clearly in literature. We investigated the opinions of parents and nurses about existing designs aimed at enhancing bonding and their desires for future designs. Using a semistructured interview, we identified nine design recommendations and six design opportunities. Most importantly, designs should be adjustable per individual and from moment to moment, so that development is not disturbed but improved. If a design indeed contributes to their child’s health and development, all parents indicated that they would like to use a design to enhance bonding.
Implications for Practice
Every design intended for the NICU should be hygienic, easy to use, and safe for the user.
A good strategy to design for bonding is to aim for devices that facilitate or simulate Kangaroo care.
Designers should investigate the individual needs for the infants and parents they are designing for, to enable them to create a product that is adjustable to the individual needs of an infant and parent at any given time.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.