
Abstract
Osteochondral explants can serve as valuable ex vivo models for investigating joint development and testing therapeutic interventions in osteoarthritis (OA). The incorporation of synovial tissue in coculture settings more closely reproduces the inflammatory milieu characteristic of OA joints; however, no report exists regarding the culture media that can support such ex vivo systems. We investigated the reactivity of osteochondral explants using two media types: Dulbecco’s modified essential medium (DMEM) and chondrogenic medium (CHONDRO). Additionally, we tested the potential therapeutic effect of serum-free conditioned media (CM) derived from allogeneic adipose-derived stem cells (ADSCs) in the context of OA. Osteochondral fragments with or without homologous synovium were cultured in DMEM and CHONDRO for up to 30 days. A subset of explants received treatment with CM. Explant reactivity was assessed by cytokine release, synovial cellularity, and osteochondral protein content using Western blot and immunohistochemistry. Explants kept in DMEM displayed diminished levels of interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNFα), together with increased Collagen II (Col II) expression. Notably, consistent suppression of TNFα was observed following CM treatment. Conversely, the CHONDRO-kept samples exhibited an increased prevalence of chondrocyte clusters; heightened Perlecan presence as well as IL-1β levels in response to CM treatment and synovial tissue-dependent fluctuations in Col II levels. Remarkably, significantly increased β-galactosidase levels could be detected in osteochondral tissues treated with CM, regardless of the culture media type. In the experimental conditions created, DMEM provided a neutral milieu and was less prone to confounding experimental outcomes, rendering it suitable for evaluating potential therapies. CHONDRO apparently increased chondrocyte clusters and facilitated extracellular matrix synthesis; however, its usage requires caution due to potential interference with experimental readouts. CM could exert an antisenescence effect, an effect that warrants further investigation.
Impact Statement
This study provides a clinically relevant ex vivo human joint model, enabling evaluation of novel osteoarthritis therapies and advancing personalized medicine.
Keywords
Introduction
Osteoarthritis (OA) is a multifactorial degenerative disease that progressively affects all joint compartments, leading to the destruction of articular surfaces and loss of function. 1 Due to population aging, the burden of OA is increasing worldwide, affecting individuals, families, and community-level quality of life. The increasing burden of disease is impacting healthcare expenditures worldwide. 2 Despite decades-long efforts dedicated to developing novel therapies, treatments are limited to symptom relief with nonsteroidal antiinflammatory drugs and corticosteroids as major components of recommended interventions. 3 To date, there is no available drug or surgery proven to modify the natural history of the disease. 4 Limitations in the development of innovative therapeutics are mainly related to the complexity of the underlying pathogenic mechanisms, as well as the unmet need for relevant disease models. Models that closely reproduce complex intracellular and cell–extracellular matrix (ECM) interactions within joint compartments and could allow for patient stratification are necessary for testing such therapies in preclinical stages. Moreover, the imperative to comply with the guiding principles of reduction, refinement, and replacement of animal experiments 5 requires models of disease that can retain the complexity of in vivo situations while avoiding inutile animal sacrifice.6,7 Aside from concerns regarding animal exploitation, animal models of disease often fail to reproduce the particularities of naturally aging joints as well as the immune and metabolic crosstalk that influence joint tissue responses to trauma, degeneration, and repair. Organ-on-chip (OoC) systems that can accommodate multiple human cell-derived tissues under physiological culture conditions are emerging platforms that potentially overcome the limitations of current models. Joint OoC models have been proposed for testing OA drugs as well as regenerative interventions; however, major shortcomings, such as costs and limited modeling of ECM interactions, still need to be addressed. 8
Explanted cartilage tissue has been proposed as a modality for studying cartilage ontogeny and understanding cartilage repair. 9 Human osteochondral explants reportedly react to immune, hormonal, and biomechanical insults. 5 Osteochondral explants from horse cocultured with synovial tissue more closely approximated the OA phenotype ex vivo. 10
Adipose-derived stem-cell conditioned media (ADSC-CM) has emerged as a promising cell-free therapeutic approach due to its rich content of growth factors, cytokines, and extracellular vesicles that could act in modulating inflammation, promoting angiogenesis, while supporting tissue regeneration. 11 Osteoarthritic chondrocytes treated with ADSC-CM significantly decreased inflammatory cytokine expression. 12 A similar therapeutic approach in a rat model of OA was demonstrated to modulate expression of inflammatory markers, 13 reducing joint-related pain and neuroinflammation, 14 demonstrating ADSC-CM’s potential as a scalable alternative to cell-based therapies.
Human osteoarthritic osteochondral explants were cocultured with homologous synovium to validate an ex vivo model for evaluating novel OA therapies. Explants were maintained in either Dulbecco’s modified essential medium (DMEM) or chondrogenic medium (CHONDRO), and their responsiveness to conditioned media (CM) from ADSCs was assessed. Tissue reactivity, cytokine release, cellularity, and ECM composition were analyzed using Western blotting (WB) and immunohistochemistry (IHC).
Materials and Methods
Procurement of human osteochondral tissue
Human osteochondral tissue was obtained from patients undergoing elective total knee arthroplasty (TKR) after ethical committee approval (Ethical Committee Approval County Emergency Hospital Saint Spiridon Iasi Nr 29/11.03.2022), and informed consent was obtained from the patients. Tissues were collected during surgery in sterile recipients and transported to the laboratory at least 2 h after collection. After thorough washing with PBS supplemented with 2% antibiotics, cartilage and underlying osteochondral bone were cut using a sterile scalpel and scissors into square fragments of approximately 2 cm, placed in sterile Petri dishes (35 mm diameter), and immersed in serum-free culture media. Pieces of synovial tissue were carefully washed and placed on top of the osteochondral pieces, further cultivated in incomplete chondrogenic media (ICM) composed of DMEM (high glucose [HG]), 1 mM dexamethasone, 5 mg/mL ascorbic acid 2-P, 4 mg/mL proline, 1 mg/mL ITS + 1 supplement, and 11 mg/mL sodium pyruvate, or in serum-free DMEM. Explants were placed within an incubator and cultivated for up to 30 days, and the media was changed every 3 days.
Adipose-derived mesenchymal cell-conditioned media
Human adipose-derived mesenchymal cells from donors undergoing elective liposuction procedures after ethical committee approval and informed donor consent were isolated as described. 11 Cell passages 2–3 were washed with PBS and cultured in serum-free DMEM with 1% antibiotic. Media was harvested, centrifuged at 300× g for 3 min to obtain CM.
Explant exposure to CM was performed five times during 30 days: samples denominated: osteochondral tissue in DMEM = DMEM osteochondral tissue in DMEM with ADSC supernatant = DMEM-CM; osteochondral tissue and synovium in DMEM = DMEM-SYN; osteochondral tissue in coculture with synovium in DMEM with ADSC supernatant = DMEM-SYN-CM; osteochondral tissue in chondrogenic medium, ICM = CHONDRO; osteochondral tissue in ICM with ADSC supernatant = CHONDRO-CM; osteochondral tissue and synovium in ICM = CHONDRO-SYN; and osteochondral tissue and synovium in ICM with ADSC supernatant = CHONDRO-SYN-CM.
Histology
After 30 days, the explant tissue was fixed in a 2% paraformaldehyde solution, decalcified (20% EDTA at 4°C for 5 days), stained with hematoxylin and eosin (HE), and Masson’s trichrome. OA was scored using the HE and Masson’s trichrome staining. A board-certified pathologist (P.P.) scored all sections. Images were captured using an automated inverted fluorescent scanning microscope (Tissue Gnostic) equipped with TissueFax cell analysis software 6.0. Clustering and cell counting were performed using ImageJ for a minimum of 5 fields of view (FOVs)/sample.
Assessment of explant-released cytokines
The ELISA human tumor necrosis factor-α (TNFα) and interleukin-6 (IL-6) ELISA kit was used to assess the cytokines in the supernatant of the culture medium at different time points (0, 5, 10, 15, 25, and 30 days) according to the manufacturer’s instructions. The absorbance was measured at 450 nm with a microplate reader (BioTek Synergy HTX).
Quantitative polymerase chain reaction (qPCR)-based immunoassay: Human IL-17A and human IL-1β were quantified with commercially available immunoassay kits (ProQuantum™ immunoassay kit from Invitrogen), read with a qPCR instrument, and interpreted using ProQuantum software according to the manufacturer’s instructions. Initially, calibration standards were prepared in ProQuantum Assay Dilution Buffer via a 1:5 serial dilution. The standards and 10-fold diluted samples were transferred to 96-well plates. During the second stage, 5 µL of each diluted sample was added to 5 µL of the antibody-conjugate mixture, which was subsequently centrifuged at 3000× g (1 min) and incubated for 1 h at room temperature (RT). Finally, quantitative reverse transcription-PCR was performed by adding 40 µL of the qPCR mixture (Master Mix and Ligase), centrifuging for 1 min at 3000× g (RT), and incubating at RT for 1 min. Standard curves and numerical results regarding cytokine levels within samples were generated using ProQuantum software.
Western blot
Bone, cartilage, and synovial tissue pieces, stored in liquid nitrogen, were ground into powder. Protein was extracted using RIPA buffer, followed by the determination of the total protein concentration using a commercially available Bradford kit (Cat. #1610375; Bio-Rad, USA). SDS-PAGE was employed to separate proteins using Mini-PROTEAN TGX Precast Gels 4–20% gradient (Cat. #4561093; Bio-Rad Laboratories, USA) in running buffer. The separation process was run at 100V for a duration of 60 min. Subsequently, the proteins were transferred to Immun-Blot PVDF membranes (#1620177; Bio-Rad Laboratories, USA) using Mini Trans-Blot Cells for 75 min at 130V. The PVDF membranes were treated with EveryBlot Blocking Buffer (Cat. #12010020, Bio-Rad) for 5 min. Primary antibodies were applied: MMP-1 (Thermo Fisher Scientific, PA5-27210), MMP-13 (Thermo Fisher Scientific, 710311), Collagen II (Col II; Thermo Fisher Scientific, PA1-26206), Beta Galactosidase (Thermo Fisher Scientific, PA5-102503), and Perlecan (Thermo Fisher Scientific, MA1-06821); diluted to 1:1000 in EveryBlot Blocking Buffer and left to incubate for 1 h at RT or overnight at 4°C; washed with TBS-T; incubated with peroxidase-conjugated antirabbit IgG and goat antimouse IgG secondary antibodies diluted to 1:500 in EveryBlot Blocking Buffer for 1 h at RT; exposed to Clarity Western ECL Substrate (Bio-Rad) for 5 min RT; and visualized using an IBright FL 1500 (Invitrogen) Imaging System.
Immunohistochemistry
The synovial tissue was fixed in 10% formalin for 24 h and embedded in paraffin. After 24 h, paraffin blocks, including bone, cartilage, and synovial tissue, were cut into 5 µm sections using a microtome, and the slides were incubated at 37°C overnight. For osteochondral tissue, the decalcification step was performed as described. The IHC protocol included manual and automated steps. Deparaffinization and rehydration were conducted on a Leica Autostainer XL; epitope retrieval, blocking, and primary antibody incubation were performed manually; detection was performed with a horseradish peroxidase kit (UltraView Universal DAB Detection Kit (760-500) Ventana, Roche) on the Ventana GX Benchmark (Roche); counterstaining, dehydrating, clarifying, and mounting were done manually. Digital imaging was performed using an Easy Scan Motic Scanner. Quantitative analysis of IHC images was performed using ImageJ software, with at least 5–30 images at 10× magnification. The regions of interest were quantified at the same threshold as the area fraction (%) of the image.
Statistical analysis
All experiments were conducted in triplicate. One-way analysis of variance followed by Bonferroni post hoc analysis was performed using OriginLab PRO version 8.0. Significance levels were set at p ≤ 0.05 for both between-group and within-group differences (n = 3).
Experiment
Osteochondral explant morphology and gross aspect
The explants were kept in culture for up to 30 days. No changes in tissue gross appearance (volume, color, or consistency) were detected. Explant tissues were observed daily with a media exchange twice a week (unless otherwise mentioned for experimental purposes-exposure to CM). The gross appearance photos of the explant culture, as well as demographic details regarding donors, are available in Supplementary Data (Fig. 1 and Table 1). Notably, explant cultures containing synovial tissue rapidly turned yellowish, demonstrating media acidification, probably indicating a greater metabolic rate in these samples. This observation was consistent for both DMEM and CHONDRO culture media.
Microscopic evaluation of OA grading on HE osteochondral explanted samples:
Summary of the Impact of Culture Media on Osteochondral Tissue Explants
CHONDRO, chondrogenic medium; CM, conditioned media; Col II, collagen II; DMEM, Dulbecco’s modified essential medium; IL-6, interleukin-6; TNFα, tumor necrosis factor-alpha.
Histology
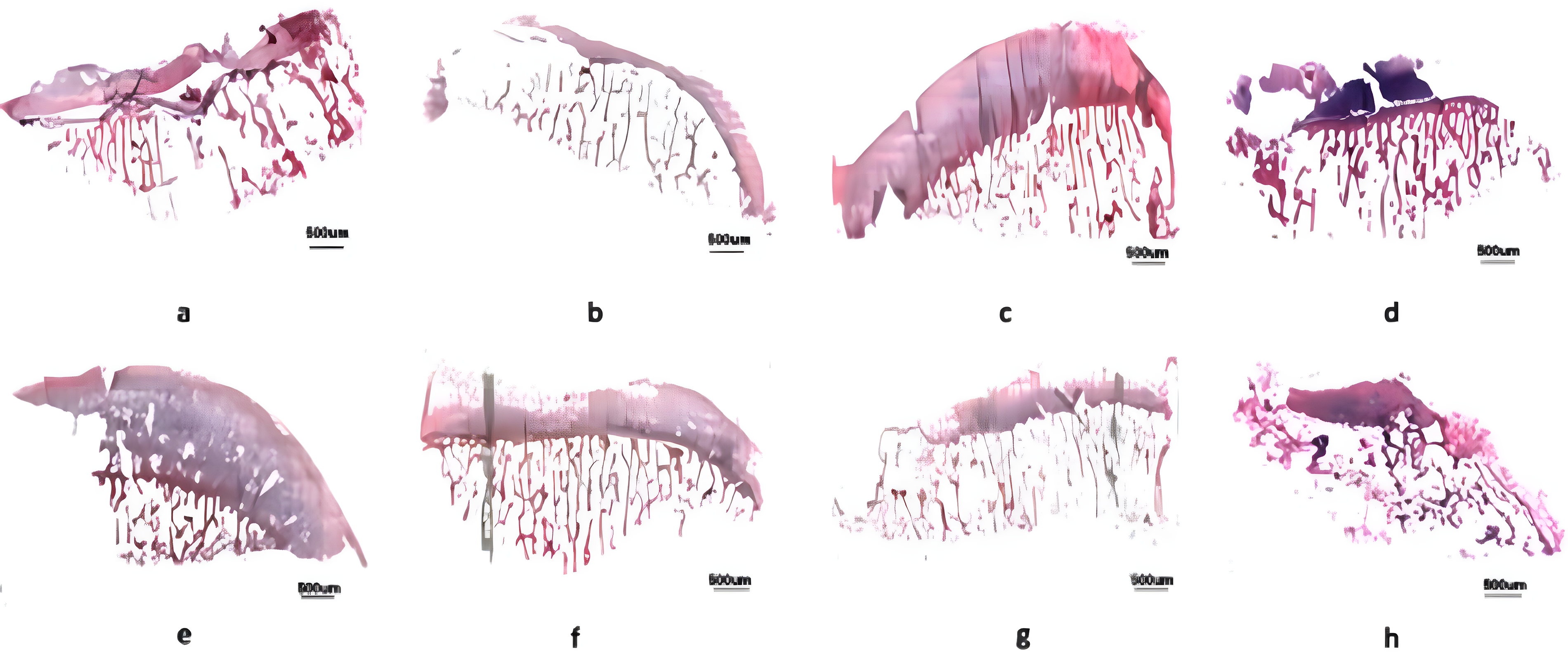
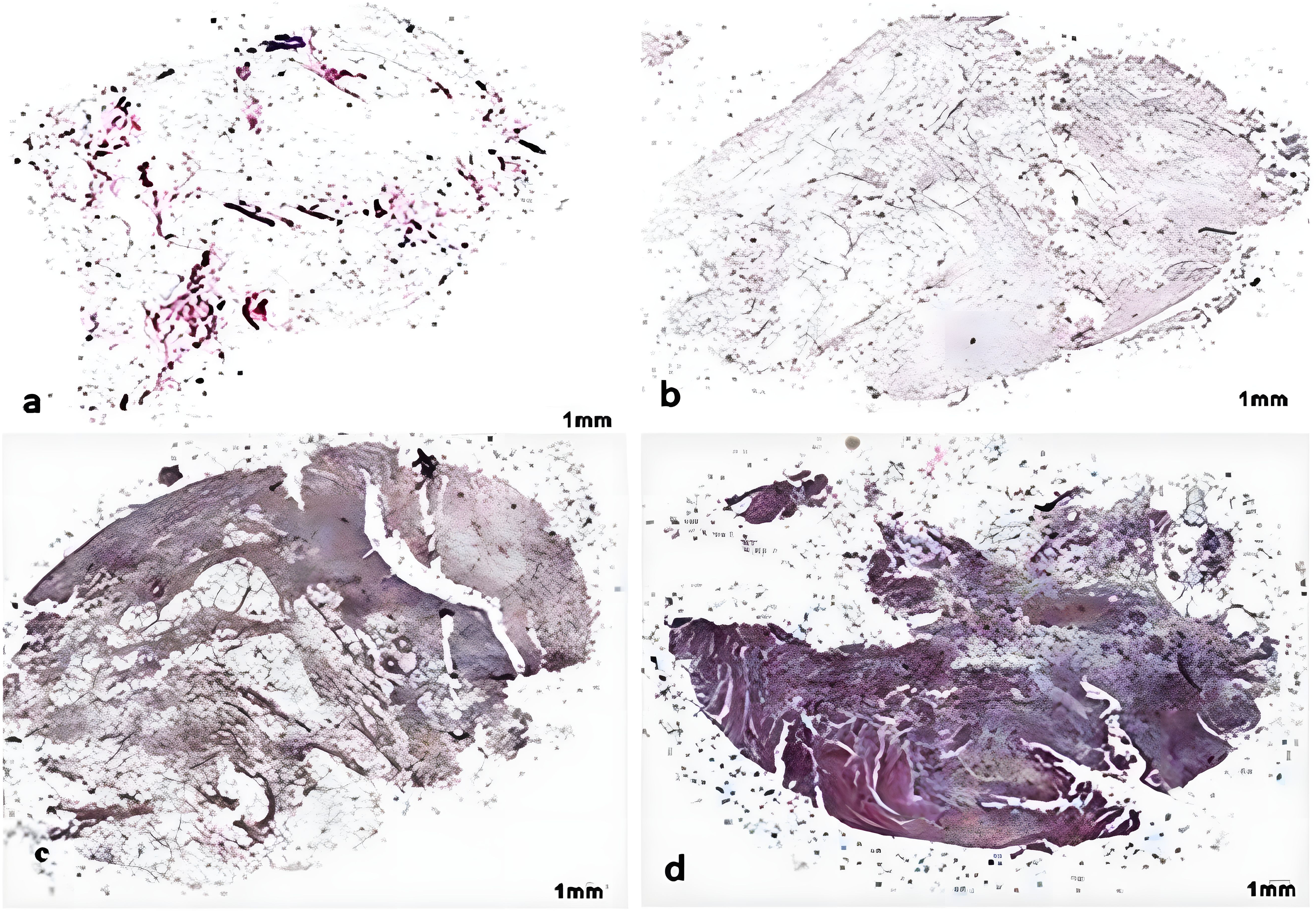
Histological evaluation was used to classify OA stages (OARSI recommendations), 12 and the template described by Pritzker was used. 13 OARSI Grade 6 (describing joint deformation and osteophyte formation) was not included in the assessment. Qualitatively, OARSI scoring of the slides stained with HE and Masson trichrome (5× magnification) revealed osteochondral changes in all the samples, ranging from Grade 3: vertical fissures (clefts); Grade 4: erosion; and to Grade 5: denudation (Fig. 1 and 2; Supplementary Data). Explanted synovial tissue revealed hyperplasia of the synovial lining cell layer and activation of resident stromal elements with inflammatory infiltration corresponding to moderate inflammatory synovitis (Fig. 2 and 3; Supplementary Data). 14
Microscopic evaluation of OA grading on HE-stained explanted synovial tissue samples:
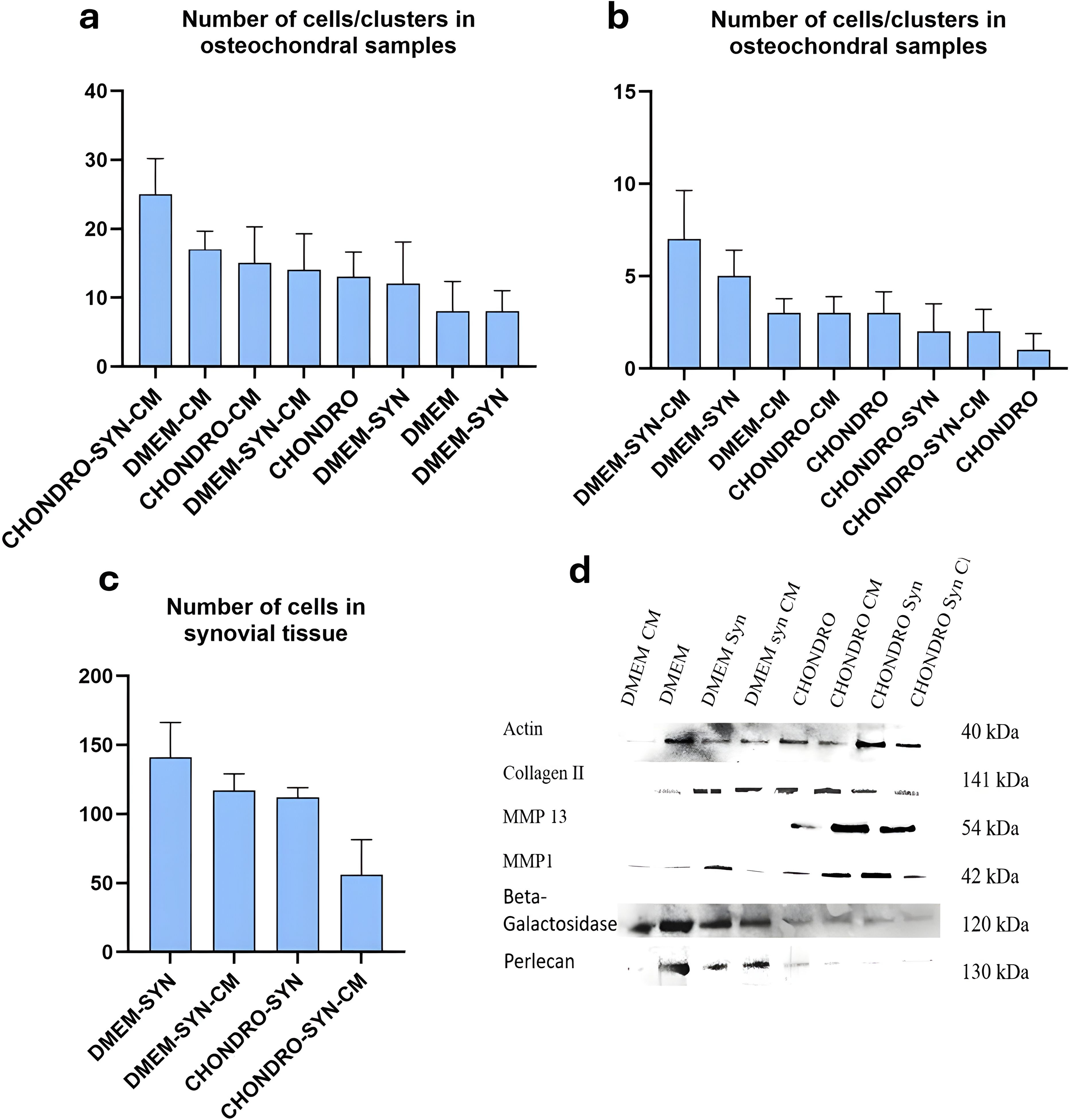
Cell clusters, the number of cellular elements per cluster within cartilage tissue, as well as the cellular elements in HE stained synovial samples, were counted in randomly selected FOVs using a grid by a member of the team (AM), blinded to sample identification. Compared with DMEM, CHONDRO explants contained more chondrocyte clusters. DMEM- and CHONDRO-treated explants treated with CM were found to have a significantly higher number of clusters than their nontreated counterparts (Fig. 3). However, the cell number per cluster was higher in DMEM explants, with a maximum for the CM-treated explants (Fig. 3a, b). Synovial samples cultured in CHONDRO media displayed significantly less cellularity than did those cultured in DMEM with or without CM. The CHONDRO and DMEM samples in coculture with synovium reacted to CM by displaying increased cellularity as well as an increased number of cells per cluster within the cartilaginous layer compared with the nontreated samples. The number of cells in synovial samples was higher in DMEM than in CHONDRO medium. Both explant types responded to CM by displaying significantly less cellularity (Fig. 3c), a possible indicator of a tendency to decrease the inflammatory response.
Number of cells detectable in H&E-stained osteochondral tissue.
Cytokine release
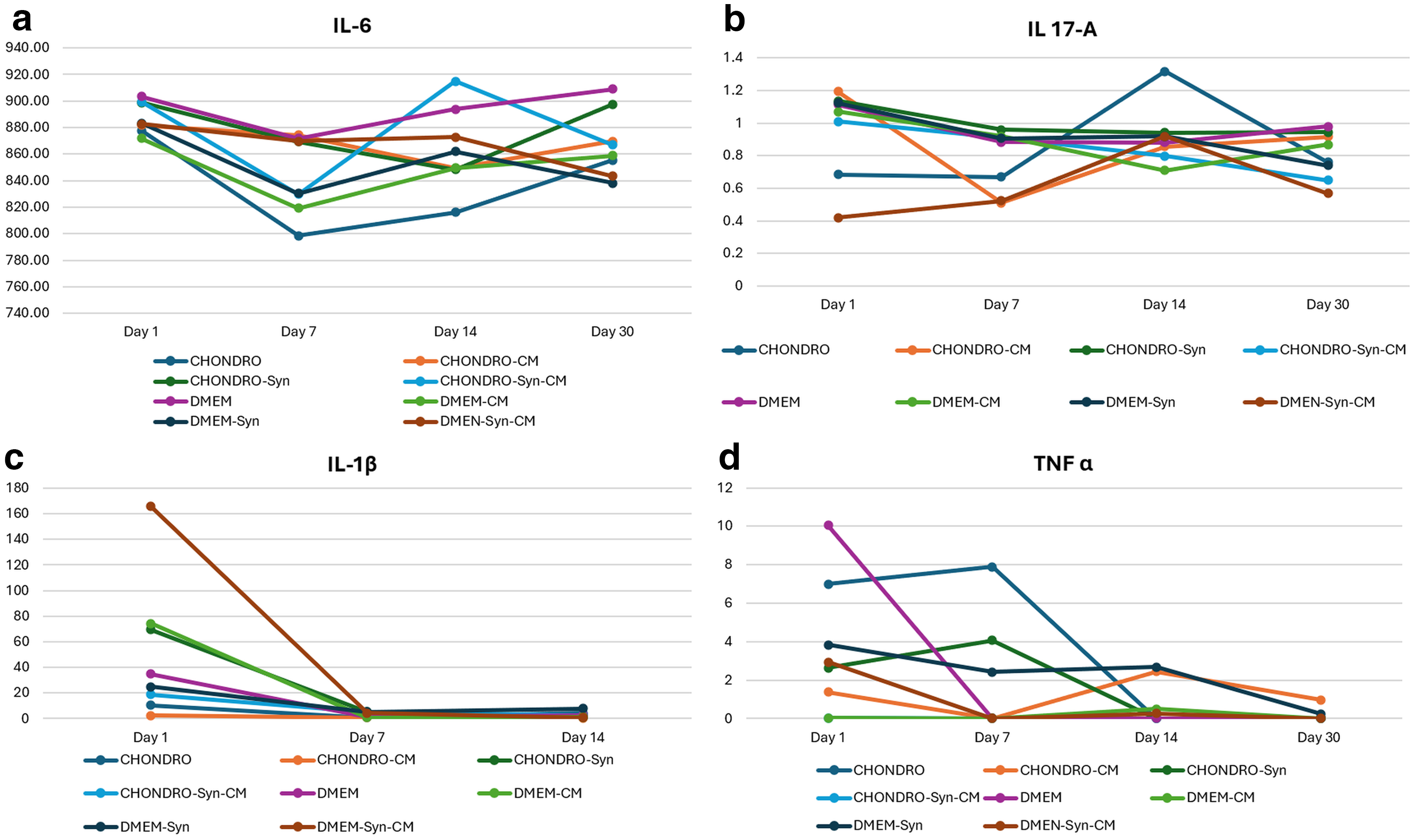
We used two methods for the detection of cytokines within culture media based on predictable concentrations of the corresponding proteins correlated with method sensitivity. Sandwich ELISA was used to detect IL-6 and TNFα, as their detection limits ranged from 10.24 to 400 pg/mL with <0.1 pg/mL sensitivity. Lowest IL-6 levels were detected in CHONDRO-treated explants without synovium. However, in the presence of synovial tissue, DMEM explants displayed lower values of IL-6 at all experimental time points than CHONDRO. CM treatment decreased IL-6, reaching a minimum after 30 days, while non-CM explants continued to display high IL-6 levels (Fig. 4a). TNFα was found to be time-dependent and significantly decreased to nondetectable values after 7 days in culture in all explant types. A significantly higher concentration of TNFα was detected in samples containing synovium for both CHONDRO and DMEM explants, while CM treatment significantly decreased the level of TNFα (Fig. 4b).
Time-resolved dynamics of cytokines released by osteochondral tissue samples over 35 days;
Commercially available qPCR-based immunodetection allows the detection of cytokine levels ranging from 0.064 to 10,000 pg/mL with a sensitivity of <0.05 pg/mL. We found that IL-17A was present in both CHONDRO and DMEM explants. Interestingly, immediately after treatment, CM treatment did not seem to affect the IL-17A level. After 7 days, the explants reacted to the CM by displaying a decreased level of IL-17A in both synovium-free and -containing explants. IL-1β, on the contrary, was detectable only in the initial stages. On day 1 after CM treatment, the IL-1β level was significantly increased compared with nontreated conditions for both DMEM and CHONDRO. A significantly higher amount of IL-1β was detected in explants containing synovial tissue in both culture media types (Fig. 4c, d).
Immune cell population in explanted synovial tissue
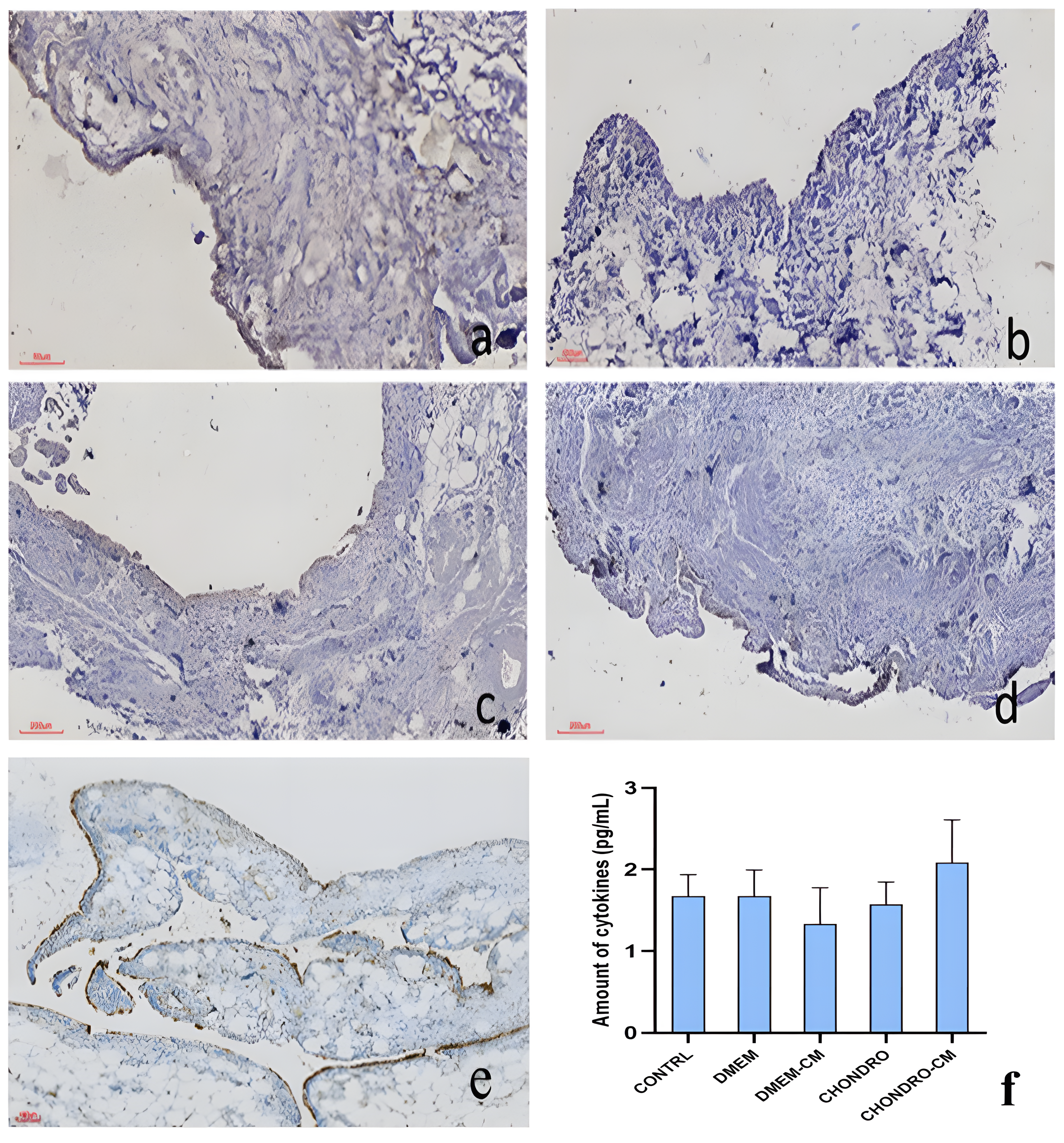
To detect cellular immune reactivity in the explanted synovium, we performed IHC staining for CD68 followed by a quantitative assessment of CD-positive elements via semiautomated image analysis. Compared with control tissue (synovial sample from an age-matched OA-free donor undergoing knee surgery for a traumatic event), CD-positive elements (calculated as the percentage of CD68-positive cells relative to the total image area) did not significantly differ upon the addition of CM or other culture media. Notably, however, explants kept in CHONDRO media exposed to CM were found to contain greater amounts of CD68-positive cells (Fig. 5a–f).
Immunohistochemistry for CD68 in explanted synovial samples:
Osteochondral tissue protein content: WB and IHC
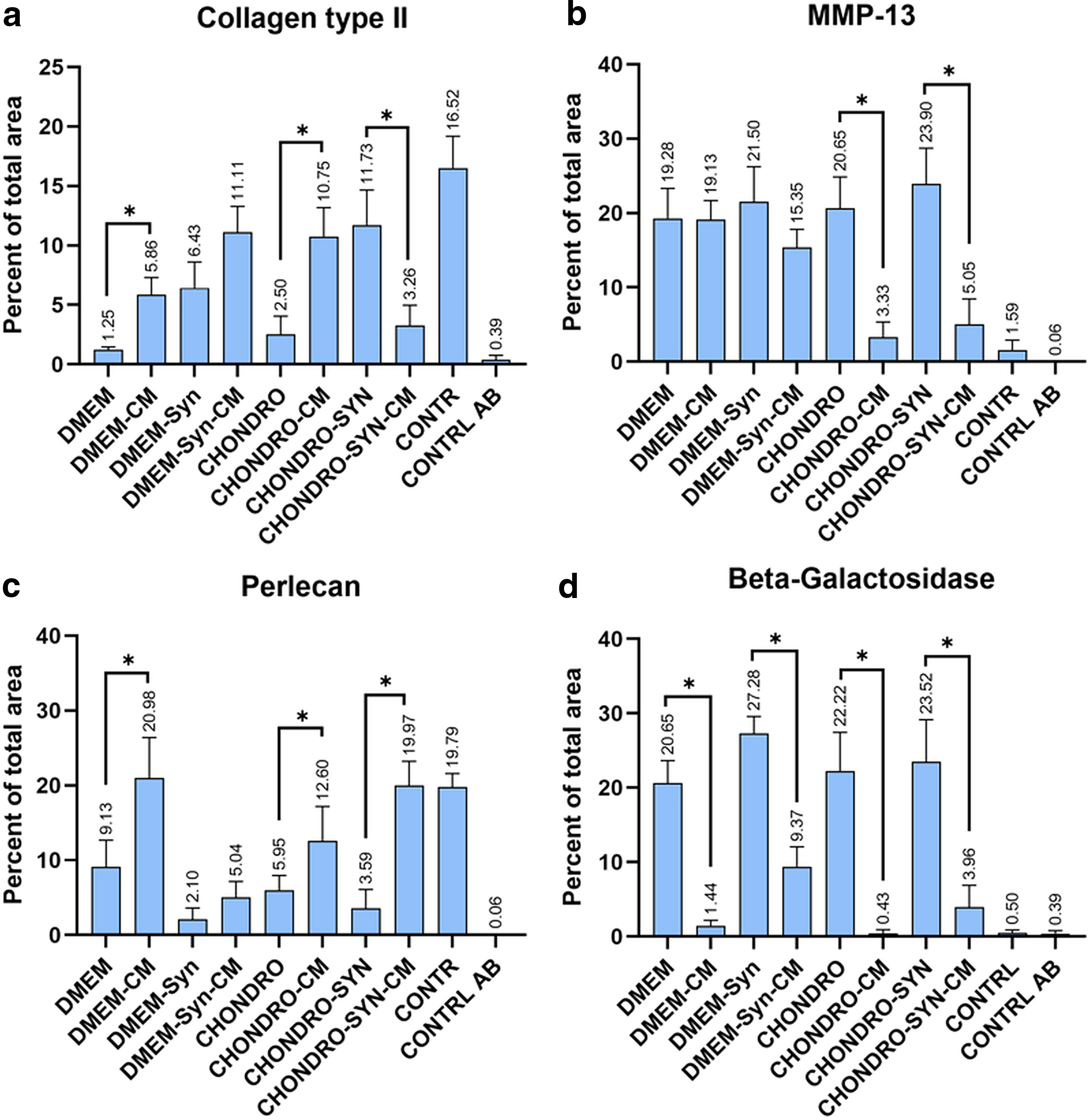
Protein content was assessed using WB and IHC, followed by quantitation of the amount of positive staining detected on the IHC slides. Both WB and IHC were performed to detect two catabolic enzymes, matrix metalloproteinase isoforms 1 and 13, as well as two cartilage ECM proteins. In addition, the presence of beta-galactosidase was tested as a marker of cellular senescence. 14 MMP-1 and MMP-13, Collagen Type II, and Perlecan, as well as beta galactosidase, were detectable in all the samples (Fig. 3d) and IHC (Fig. 5). Collagen type II was significantly increased in samples cultured in DMEM supplemented with CM. This was not consistent in CHONDRO explants, where Collagen Type II was decreased in the CM-treated samples containing synovium but not in the synovium-free samples (Fig. 2a and 6a; Supplementary Data). All explants treated with CM displayed significantly lower levels of beta galactosidase as assessed by IHC, irrespective of culture media, and the presence of synovium (Fig. 6d). There was a significant increase in the percentage of cells in the synovium-free DMEM sample treated with CM, as well as in the CHONDRO sample with or without synovial coculture (Fig. 5 and 6c; Supplementary Data).
Quantification of IHC signal (percent of total area) for
MMP13 slightly decreased in DMEM explants exposed to CM, while a significant decrease was detected in CHONDRO explants treated with CM compared with nontreated for both synovium-containing and synovium-free samples (Fig. 6b).
Discussion
Relevant biomimetic models that simultaneously reproduce the articular joint complexity and the large phenotypic diversity of OA are needed for testing therapies with disease-modifying potential that are both effective and potentially personalized.15,16
An increasing number of total joint replacements are performed globally. 17 TKR involves surgical removal of the whole joint cartilage layer, including the subchondral bone. Removal of the synovial layer is optionally performed as a modality to avoid postoperative joint effusion, as well as the surgeon’s preference. Synovectomy during TKR for inflamed joints is associated with improved postsurgery recovery in terms of pain and range of motion. 18 As a consequence, with appropriate informed consent and ethical approval, osteochondral cutoffs and homologous synovial pieces could be obtained.
Here, we investigated the responsiveness of human osteochondral explants in coculture with homologous synovial tissue to be used as ex vivo OA models. Given the conflicting data in the literature regarding explant conditioning and maintenance, we compared the use of two different media, DMEM and CHONDRO. As proof of concept for explant model reactivity, we used CM media from allogeneic ADSCs as a possible therapeutic intervention for treating OA. Explant reactivity in terms of cytokine release and changes in ECM composition were assessed quantitatively at the protein level using immunoassays, WB, and IHC.
Osteochondral tissue fragment collection was performed after macroscopic mapping of the OA lesions, following the recommendations of the International Cartilage Repair and Joint Preservation Cartilage Injury evaluation package 19 with the purpose of collecting explant samples from zones displaying similar degrees of macroscopic OA damage.
Osteochondral fragments and synovium kept in both culture media types displayed no macroscopic signs of tissue deterioration. As previously reported, no cells were observed to migrate from the explants. 20 Explant-released IL-6 was detected in both media types in samples cultured with and without synovial tissue for up to 30 days. CM addition did not significantly influence IL-6, except for in the case of synovial-free samples kept in DMEM for 30 days, which contained lower amounts of IL-6 than the nontreated samples. IL-6 levels are known to increase in joints with symptomatic cartilage defects or OA. Previous findings suggested that IL-6 can stimulate anabolic metabolism within resident chondrocytes, thereby fostering a favorable milieu for neocartilage formation during in vitro regeneration. IL-6 targeting has been proposed as a potential strategy to enhance cartilage matrix production in the context of autologous chondrocyte implantation or microfracture for symptomatic cartilage defects or OA. 21 Here, as expected, the highest amount of explant IL-6 was found in synovial cocultured samples with a maximum at 14 days. The significantly lower amount of IL-6 in DMEM-cultured synovial-free samples treated with CM could imply that the level of IL-6 of nonsynovial origin can be decreased by CM treatment, but this effect is not maintained in CHONDRO. It is possible that the dexamethasone concentration in CHONDRO-treated cells influences IL-6 expression in explant chondrocytes but not in synovial tissue. However, further mechanistic studies are needed to elucidate the role of specific media compounds in implant reactivity, especially given the known chondrotoxic effect of intra-articular delivered corticosteroids. 22 TNFα rapidly became undetectable except in synovium-containing samples at 7 days, probably indicating its synovial origin as well as the rapid response to joint milieu changes. 23 Remarkably, CM treatment induced a decrease in the TNFα concentration to undetectable levels in both DMEM and CHONDRO explants. Existing data strongly support inhibition of TNFα as a potent modality for preventing and treating OA. 24 CM from various mesenchymal stem cells (MSCs) exert chondroprotective effects in vitro and in animal models, inhibiting inflammatory cytokines, including TNFα. 25 This was confirmed in our study by the comparative cytokine dynamics, in which CM-treated samples consistently displayed lower TNFα levels. IL-1β was found to be consistently increased in all the samples treated with CM; however, values were detectable for only 7 days, with the highest amounts in synovial explants. IL-1 has been classically considered a target for treating OA 26 ; however, recent data question the validity of this approach. IL-1α and IL-1β were not found to be involved in the occurrence of posttraumatic OA in a murine model. 27 Moreover, IL-1β pretreatment increased synovial MSC chondrogenesis 28 and could be a mediator of synovial-induced cartilage regeneration. 29 IL-17A decreased with CM treatment, especially in synovial explants. These findings are consistent with the synovial origin of IL-17A 30 and reflect synovial tissue reactivity to CM, confirmed by the present study.
One of the hallmarks of synovial tissue changes within OA is the presence of inflammatory elements within the synovial lining, which parallel the degree of OA destruction. 31 The inclusion of synovial-like tissue is mandatory for obtaining relevant in vitro OA models. 32 Here, histological and IHC staining revealed that explanted synovial samples corresponded to OA grades 4–5, which was consistent with the histological OA grading of osteochondral tissue. CD68-positive cells were detectable in all the samples, while nonsignificant variation was observed between the samples treated or not treated with CM and between media types. Notably, CD68 staining in the explanted synovium and the control tissue did not significantly differ. This can be explained by the fact that the synovial tissue used as control was procured from a knee trauma patient, possibly displaying synovial tissue reactivity after injury. 33 CD68-positive synovial macrophages correlate with increased synovial fluid MSCs, being potentially associated with attempts at regenerating cartilage 34 or subchondral bone. 35
We next assessed the protein content in osteochondral tissues by investigating the presence of the normal cartilage tissue markers Collagen Type II and Perlecan. Matrix proteinase isoforms known to be definitive for the catabolic osteoarthritic milieu, as well as beta-galactosidase as a marker of cellular senescence, were also investigated. Both WB and IHC confirmed the presence of Col II, Perlecan, MMP-1, MMP-13, and beta-galactosidase within the explanted tissue in all the samples. We found that Col II was significantly higher in synovium-free samples treated with CM from both DMEM and CHONDRO than in control samples, but was not significantly different in synovium-containing explants. Col II has been previously shown to increase in chondrogenic ADSC sheets 36 as well as in OA joints treated with CM from various MSCs in animal models.37,38 This effect could not be reproduced in our study in synovium CHONDRO explants. Col II synthesis could be affected by the dexamethasone in CHONDRO media combined with the presence of synovial tissue; however, further investigations and mechanistic studies are needed. Type II collagen in mature cartilage is highly cross-linked by nonreducible hydroxylysyl–pyridinoline bonds, which makes the bulk fibrillar network poorly soluble in detergent-based buffers. Consequently, the use of RIPA buffer in this study captured only the RIPA-soluble fraction of COL2A1 (e.g., nascent or less cross-linked molecules), while the majority of the cross-linked collagen likely remained in the insoluble pellet. Therefore, our WB data should be interpreted as relative changes within this soluble pool, not as total Col II content. More aggressive chaotropic/enzymatic extraction protocols (e.g., guanidine-HCl followed by pepsin digestion) or hydroxyproline assays would be required to quantify total Col II. Perlecan was increased in all CM-treated samples regardless of the presence of synovial tissue or media type, demonstrating both explant reactivity and the potential effect of CM. However, further studies are needed to determine the exact molecular structure of the Perlecan domain in this context, given its ubiquitous role in promoting cartilage ECM synthesis as well as matrix mineralization. 39 MMP-13 was found to decrease upon CM treatment, but significantly only in CHONDRO, probably due to a synergistic effect with media components. Cytokine levels reported herein were quantified from longitudinal culture supernatants, independent of tissue extraction efficiency, while WB results reflect changes within the RIPA-soluble protein fraction, which may underestimate contributions from highly mineralized bone tissue.
Senescence and the senescence-associated phenotype (SASP) have been recently recognized as one of the factors involved in OA onset and progression. 40 CM treatment was found to significantly decrease beta galactosidase presence within osteochondral samples, regardless of the presence of synovial tissue or the media type. While this finding needs further extension on the full spectrum of SASP markers, our findings present evidence that seno modulation could be a possible mechanism of action of CM treatment.
A summary of the different explant behaviors in the two different culture media used in this study is provided in Table 1.
Here, we present evidence that osteochondral tissue from cocultured with a joint homologous synovium can serve as a model for studying the effect of possible intervention therapies in advanced stages of OA. Explants can be kept for extended periods in culture media, as organotypic cultures demonstrate reactivity to the added compounds that can be tested for therapeutic effect. We found that CHONDRO media interferes with explant readout; therefore, serum-free DMEM can act as a neutral milieu for testing potential therapies. A limitation of this study is the relatively uniform tissue donor population represented by age (40–50 years) and posttraumatic knee OA, which was inferred from the hospital unit profile (regional trauma center). The lack of age-matched OA-free controls is another limitation that we found problematic to overcome due to ethical issues in sample procurement. Another limitation is the restricted number of biological replicates (n = 3) dictated by the limited availability of eligible human surgical waste tissue; while multimodal readouts and blinded region-level quantification strengthen internal validity, larger donor cohorts will be essential to confirm and extend these findings. Although these results need to be validated in larger and more diverse donor sample populations, the findings could document the need for systematic collection of disposable biological samples during TJR. Statistical analysis of explant reactivity has been considered as a method to overcome donor variability. 41 We propose that systematic collection of osteochondral tissue, combined with the synovium whenever possible, could be performed within a preexisting ethical and logistical framework. Readouts from multiple donors with different demographics, geographical backgrounds, and comorbidities were collected and stored in appropriate databases. This approach could aid in artificial intelligence-based modeling of phenotype-based responses to a proposed novel therapy, furthering precision medicine in treating OA.
Conclusion
In this study, we present evidence supporting the utility of osteochondral tissue cocultured with synovium as a model for testing therapies for advanced OA. The choice of culture media significantly influences explant reactivity, with DMEM being a neutral milieu for testing potential therapies. CM from allogeneic ADSCs can promote cartilage matrix remodeling and counteract the inflammatory milieu in OA and could act as a seno modulator within the articular joint milieu. Systematic collection of osteochondral and synovial tissues can offer a valuable resource for overcoming donor variability and advancing precision medicine in OA treatment.
Ethical Approval
Donor tissue procurement for the extraction of adipose-derived mesenchymal cells was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the County Emergency Hospital Iasi Saint Spiridon Iasi Romania Nr 31567/1507/2015 and the Ethical Committee of the County Emergency Hospital Saint Spiridon Iasi Nr 23/01/08/2018 Ethical Committee Approval for Osteochondral and Synovium Tissue Samples from the County Emergency Hospital Saint Spiridon Iasi Nr 29/11.03.2022.
Authors’ Contributions
Conceptualization: C.-M.Z.-D. and L.L. Methodology: L.L., A.E.M., C.S., A.P., and C.-M.Z.-D. Software: A.E.M. Validation: L.L., D.A., and A.A. Formal analysis: C.S. Investigation: C.-M.Z.-D. and A.E.M. Resources: D.A., A.A., L.L., and N.L. Data curation: L.L. and F.Z.-E. Writing—original draft preparation: C.-M.Z.-D. and C.S. Writing—review and editing: L.L. and F.Z.-E. Visualization: A.E.M. and A.P. Supervision: L.L. Project administration: L.L., N.L., and A.A. Funding acquisition: L.L. All the authors have read and agreed to the published version of the article.
Footnotes
Acknowledgment
The authors thank Dr. Dan Cionca for support in collecting donor samples and disposable after TKR.
Funding Information
Financial support was provided by the Romanian Ministry of Research, Innovation and Digitization, CNCS/CCCDI-UEFISCDI, project number ERANET-EURONANOMED-3-OASIs, within PNCDI III (contract number 273/2022). The authors also acknowledge the financial support of the grant of the Ministry of Research, Innovation and Digitization under the Nucleu-program within the National Research Development and Innovation Plan 2022–2027, Project number PN 23 11 01 01.
Declaration of AI Use
AI was not used for generating results, text, figures, or any other item in this article.
Consent to Participate
Donors of adipose tissue from liposuction surgeries and donors of osteochondral and synovial tissue removed from knee joints as part of the procedure of total knee replacement have given their written consent for using data resulting from processing respective tissues in research on the condition of anonymization.
Availability of Data and Materials
The data are available from the authors.
Disclosure Statement
The authors declare no conflicts of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.