
Abstract
Mass panics can arise in response to a variety of situations, such as the spread of pathogens, bank failures, or insecurities about economic supplies. Such panics can produce contagious behaviors such as fleeing social contacts, bank withdrawals, and panic buying. In such situations, the processing of external stimuli, mediated by the perceptions and biases of the individual, can reach a threshold point at which panic behaviors are triggered. Due to the human propensity to imitate the behavior of others in uncertain crisis situations, one individual’s panic behavior can spread contagiously. This paper looks at the similarities among case studies of mass panic around the world and from these cases synthesizes a conceptual model to aid our understanding. Decision-makers can use this model to strengthen national resilience against panic-generated behaviors and ensure an orderly and successful public response to future biological, financial, or economic crises.
Introduction
In certain conditions, crises can generate panic within a population. Mass panics can manifest in multiple ways, from the considerable population movements associated with the Black Death in the 1300s to the panic buying and widespread financial system disruptions experienced during recent decades. Previous studies and models of mass panic have tended to be specific to one or another kind of mass panic—either in response to a biological, financial, or economic crisis—that is, in response to a pandemic (Arnot et al. 2020; Khan and Huremović 2019; Perini 2018; Taylor 2022; Wheaton, Prikhidko, and Messner 2021), bank run (Calomiris 1999; Diamond 2007; Kaufman 1987; Weihong and Qiao 2016), or consumer panic (Billore and Anisimova 2021; Cham et al. 2023; Li et al. 2021). Investigations conducted here show that a set of conditions can be identified which consistently produce a mass panic response during historical crises of all these kinds across the centuries.
We define mass panic as an episode of contagious disgust or fear responses in a large group of people to an uncertain but significant and ongoing threat such as infectious disease, financial ruin, or significant economic constraint (i.e., a conspicuous threat to life or livelihood). Research on fear contagion explores how individuals in a group amplify each other’s fear responses, leading to a rapid escalation of panic. Studies have demonstrated that the perception of fear in one individual can trigger a cascade of fear responses in others, leading to a collective and heightened state of arousal (de Gelder et al. 2004; Perini 2018; Wheaton et al. 2021).
Additionally, the literature on disgust contagion emphasizes how the perception of an ongoing threat can trigger a shared sense of repulsion, contributing to collective panic (Taylor 2021; Walby and Spencer 2012).
Sociological factors such as social identity, group cohesion, and shared norms can also contribute to mass panic (Drury 2018; Levine and Manning 2017; Savage 2019). Sociological research also explores the concept of community resilience as a mitigating factor against mass panic. Communities with strong social networks, effective communication channels, and shared resources may exhibit greater resilience in the face of ongoing threats (Drury et al. 2019; Elcheroth and Drury 2020; Norris et al. 2008).
While we will recognize the role of these various kinds of factors in the dynamics underlying mass panic, we will follow here the central thread in the literature that mass panic is in the first instance triggered by the fight/flight/freeze response to a dangerous situation (Quarantelli 1954). It involves a sudden switch from behaviors that favor the group to those focused on helping oneself (Lang and Lang 1961). The classic example of mass panic is to “fly” from a contagious disease sweeping through an area. As might be expected if the threat is perceived to be other people (as disease vectors), the direction of flight tends to be away from that chosen by the majority of other fleeing individuals, especially when this majority is a higher proportion of all individuals or when the threat is perceived to be greater (Haghani and Sarvi 2019).
“Fight” responses arise when there is social competition for a scarce resource, as in financial crises, such as bank or stock market panics in which there is contagious withdrawal of funds such that people become afraid they will not be able to get access to their bank investments. Similarly, panic buying is a crisis in the goods-and-services sector of the economy that shares many features with the other two kinds of panic.
The third instinctual reaction, “freeze,” is the individual’s propensity to isolate themselves when in a state of uncertainty about the nature and location of a threat, or when the threat is so imminent and constraining that other options are not possible (i.e., one “succumbs” to the threat). Flight requires a sense that one can escape the threat effectively. If the threat is perceived as being everywhere—for example, due to a vague belief, such as the existence of unknown people poisoning Tylenol capsules—then there is no safe place to go to; an avoidance strategy is not clear, and flight is not an option. Also, if a dire outcome is obvious, with no escape, then acquiescence is the only proper response. A freeze, rather than flight, response is triggered in such cases (Perkins and Corr 2006). Furthermore, when a population is dense, and economic opportunities are tied to location, fleeing is not often possible. In such cases, people will take the second-best option, “freezing,” by isolating themselves, physically (e.g., by staying in their homes, as during COVID “lockdowns”), or epidemiologically (e.g., by wearing a mask when in public). Which reaction becomes dominant thus depends on the individual’s psychological traits, the nature of the threat, and its physical and social context (Dias, Coelho, and Zsido 2023; Zsido et al. 2020). Mass panic can therefore be considered a group-level manifestation of the “fight/flight/freeze” syndrome (Gray 1982).
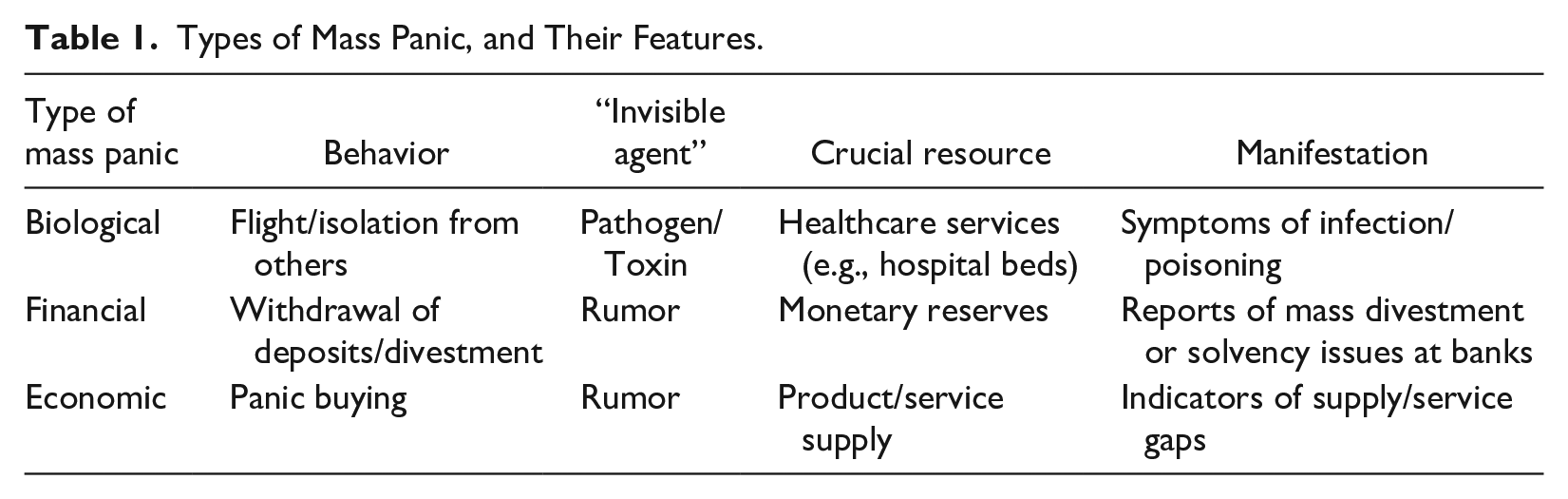
We further argue that there are three main categories of mass panic—biological, financial, and economic. In each case, there is a characteristic panic-induced behavior (e.g., flee populous areas), an “invisible agent” that causes observable “manifestations” on which others base their judgments about the nature of the situation facing them (such as a pathogen that infects people) and a resource on which the mass panic puts pressure (e.g., care services, such as hospital beds) (see Table 1).
Types of Mass Panic, and Their Features.
Mass panic occurs in response to rapidly evolving crises where there is a feeling that time is running out to evade unwanted consequences. The time pressure can limit people’s ability to think critically and instead make them amenable to “following the crowd,” imitating the safety-seeking behaviors of others (Mawson 2007). The terror and alarm generated by a crisis can lead to extreme self-protective behavioral measures (Clarke 2002), such as avoiding all social contacts. The perceived danger of the situation is met with a weakening of self-control in which individuals resort to self-preservation (Osadchenko et al. 2020), even to the point of family relationships breaking down due to suspicion of each other’s infective status or perceived risky behaviors (Hossain, Ferdous, and Siddiqee 2020).
Mass panic can cause rapid and widespread social disruption. It is a contagious behavior, meaning that it spreads from person to person like a transmissible virus. Social norms can be violated very suddenly, eliminating a group’s reference points for how to live and behave as citizens in a society (Lagadec 1993).
Mass panic, where it occurs, can also prevent a government from effectively responding to an ongoing crisis. The uncooperative, antisocial behaviors arising from mass panic make populations more vulnerable to the impacts of a crisis such as the inability to safely store financial value, supply chain shortages from panic buying, or the impacts of using unsafe home cures against a disease.
For conceptual clarity, mass panic should be distinguished from a number of other phenomena with which it shares some features (see Table 2). These phenomena are distinguished by the perceptibility of the threat, the nature of onset (surprise and immediacy), the duration of the threat, and the degree of contagion or social imitation responsible for causing the behavior. 1 For example, mass hysteria is an episode of contagious behavior sparked in a group by significant, shared financial or emotional stress, often without the ability to express or release this stress in normal ways, but in the absence of a specific threat. This can include the belief that the individuals are subject to a disease and can manifest in afflictions such as dizziness and vomiting. It can also be mediated by shared institutional identity (e.g., to a school, factory, nunnery, or village) (Balaratnasingam and Janca 2006). 2 Examples include manifestations of dancing mania in medieval Europe wherein numerous people took to dancing for days (Waller 2009), the famous Salem witch trials, and the “Pokémon panic” of 1997, in which thousands of Japanese children exhibited seizures while watching an episode of a popular TV show (Baloh and Bartholomew 2020). When there is no obvious manifestation of the threat, as in the case of witchcraft, then “freeze” is the appropriate response, as an “attack” can come from any direction at any time. Remaining in a state of continual defensiveness can lead to heightened anxiety (Gray and McNaughton 2000; Miceli and Castelfranchi 2005).
Characteristics of Threat-Related Social Phenomena.
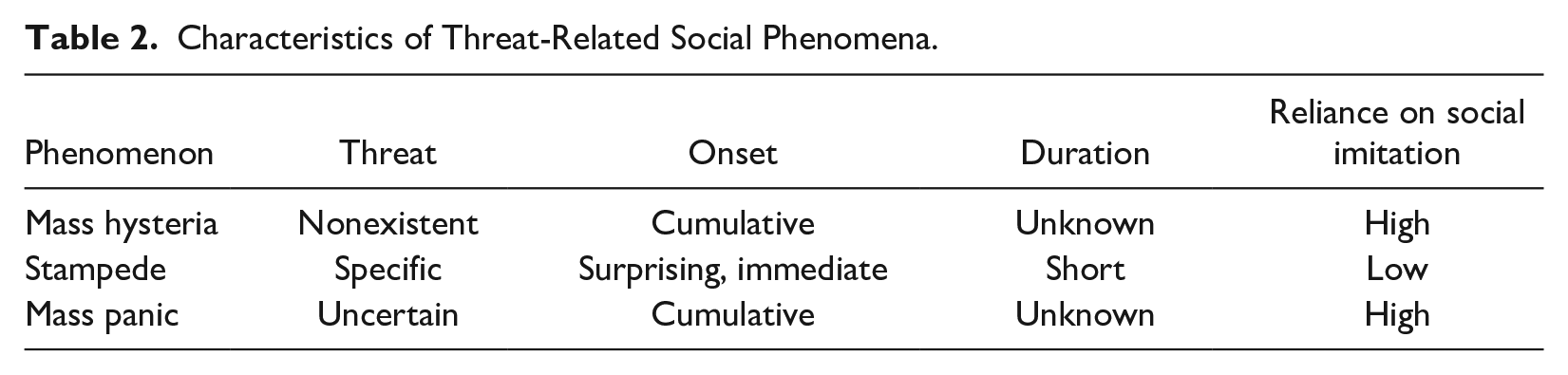
A stampede is an event involving panic behaviors in an often-enclosed group instigated by a clear and present danger when the means of flight or escape are constrained (Rogsch et al. 2010). It need not be contagious, as often everyone can directly perceive the threat, in which case it becomes a largely individual response in the presence of others (although the presence of other stampeding individuals can increase the sense of panic). Examples include a fire or bomb in a building, a school shooter, a terrorist attack, or collapsing sports stadium stands.
By contrast, mass panic arises when the threat is real, but not well-understood by the general populace, but also not characterized by a quick onset and cessation.
All of these phenomena are underpinned by panic, an individual’s fear-based fight, flight, or freeze response to a perceived threat requiring a quick reaction, such as the presence of a predator, which can overwhelm normal cognitive processes. When the threat appears in a social situation or is of large scale, some contagion of response can occur (e.g., flood, earthquake, tsunami, nuclear power plant accident, and witchcraft accusations). The need for quick response can lead to “irrational” behaviors such as refusing to evacuate dangerous areas, refusing medical treatment, stigmatizing those trying to help (such as healthcare workers), or fleeing with a known case of the disease (making it more likely one infects multiple others) (Shultz et al. 2016).
It is important to clear up such definitional issues around mass panic, as they can have substantive bearing on arguments about the nature of such a phenomenon. For example, a number of scholars deny the very existence of mass panic (Clarke 2002; Gantt and Gantt 2012; Keating 1982; Norwood 2005). However, they are typically referring to what we have called stampedes (e.g., building fires and sinking ships) or physical disasters from which one can individually panic by fleeing or freezing (i.e., floods, earthquakes, and tornadoes).
This paper aims to produce a conceptual model of mass panic based on evidence from multiple case studies, taken from historical records and contemporary analyses, to better understand the phenomenon, and ultimately to aid the ability of policymakers to make effective panic-reduction policies. Subsequent sections describe the methods used to identify case studies of mass panic, identify the key features shared by those studies, and use these features, as well as variables from existing models of specific forms of mass panics to generate a generic conceptual model of mass panic, which enable us to reduce these complex psycho-social phenomena to a concise form. We believe we present here the first model that generalizes across these three kinds of preconditions for what appears to be a similar response, mass panic: biological, financial, and economic.
Methods
The conceptual model developed in this paper derives from a comparison of case studies of mass panic. Case studies were selected from a thorough library and journal search based on the terms “mass panic” or “mass hysteria,” eliminating those cases that did not involve a biological, financial, or economic crisis in which large-scale contagious panic was observed, leading to a protracted period of danger to the public’s health or social order (Enriquez-Sarano et al. 2019). The case should also be well-documented to allow for comparative analysis. In addition, because a detailed discussion of all the identified cases is beyond the scope of a single paper, the selected sample was designed to reflect variation in the size of the population affected (single regions in one country to global), and the level of actual damage done to social order or public health caused (from very low to very high). For biological crises, variety in the agent of infection was also sought: prion, virus, bacterium, or toxin.
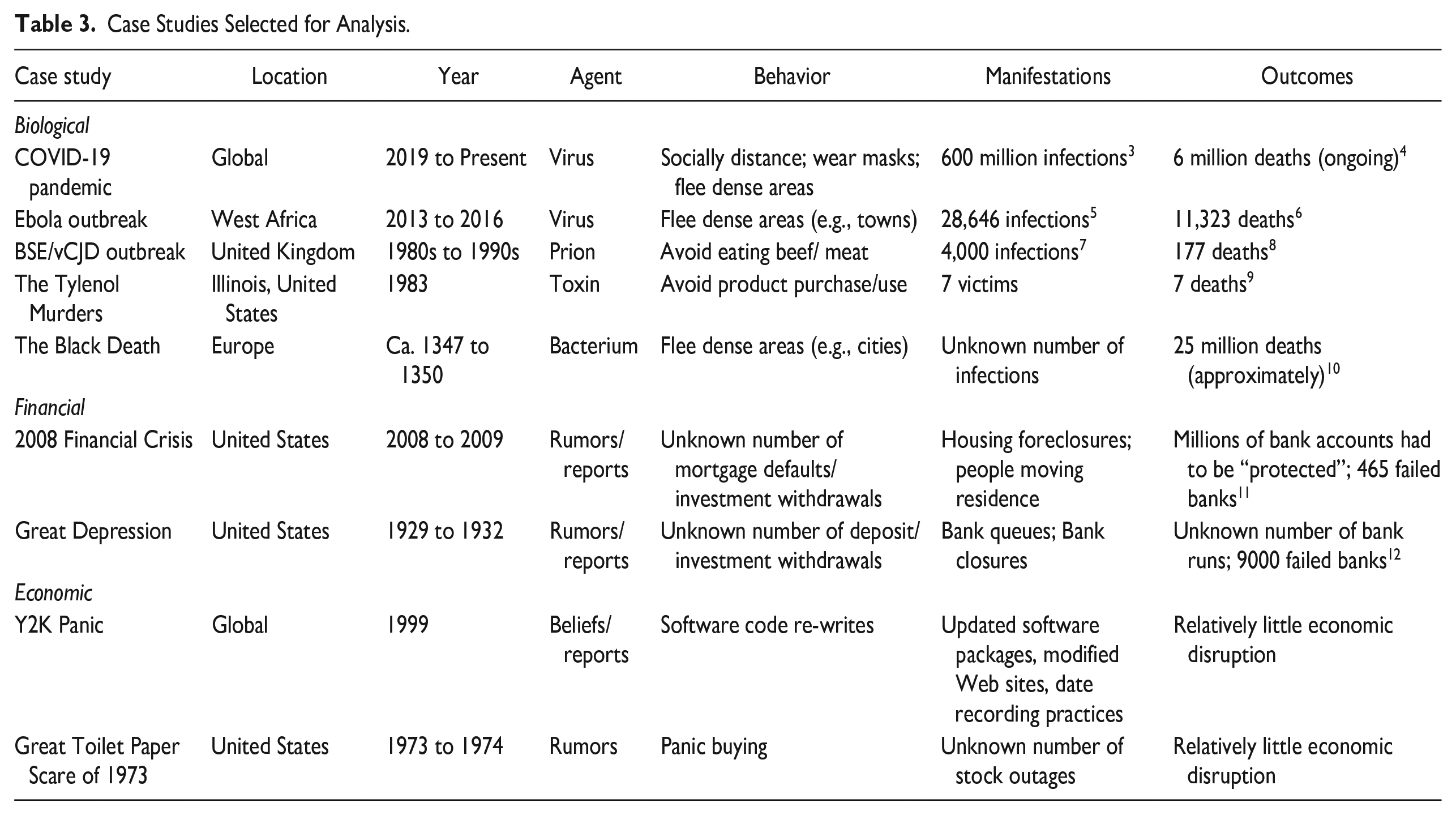
The case studies examined are listed in Table 3 and described in Appendix 1. Each case study’s key features were compared to find commonalities, utilizing a comparative case studies approach. This means that case studies are taken from different contexts and time periods and studied to reveal similarities and differences between them (Goodwick 2014). These commonalities were then combined, together with variables from existing theories of mass panics, to form a conceptual model. The outcome of this comparative case study analysis will thus be a conceptual model which details the common features between them. It will help to answer the question of what conditions need to be present in a society for a crisis to develop into a mass panic.
Case Studies Selected for Analysis.
Results: A Conceptual Model of Mass Panic
First, we describe the results from the case study comparison and then the conceptual model derived from those results.
Case Study Comparison
A close reading of the available literature on mass panics (see Appendix 1 for a descriptive account of the selected cases) suggests a variety of features are characteristic of the majority of social crises. This investigation suggests that the behaviors characteristic of mass panics include:
Mass flight or exodus from population centers (in biological cases) (Clarke 2002);
Dangerous health-seeking practices including using harmful home remedies (in biological cases) (Knoblock and Malkin 2022);
Hoarding of resources (e.g., through panic buying) (Chua et al. 2021), including money, which can produce bank runs (Calomiris 1999);
Violence against health or aid workers and/or government officials (Mawson 2005);
Ignoring government-mandated directives and government advice (Corbu et al. 2021; Demirtaş-Madran 2021; Richards, Briggs, and Axe 2020);
Rioting and looting (Friedgut 1987);
The spread of conspiracy theories and rumors (Jedwab, Johnson, and Koyama 2019).
Our review also suggests that factors such as the following are associated with these behaviors:
A perceived high, but uncertain, risk of personal harm or suffering (physical or financial);
No means of escaping the threat and uncertain prospects of threat reduction in the near future;
A generalized distrust of others as they may be a source of the threat (e.g., an asymptomatic carrier of disease);
The institutions responsible for maintaining public safety (e.g., the government or health service) are primarily working with incomplete information and making judgments which many disagree with, thus limiting their credibility;
Rumors freely circulate amongst the population.
The fact that certain conditions consistently appear in these cases points to the existence of a mass panic causal pathway. If we can identify how these common elements combine to cause a mass panic, this would form the foundation of a causal model of mass panics.
Model Development
Understanding the behaviors exhibited by populations in social crises is best achieved using a behavior-centered approach, grounded in behavioral science. Therefore, this conceptual model takes the classic form of a causal model in which individuals process information to make decisions about how to respond to a particular kind of situation: a social crisis. However, as it is also a population-level model of mass behavior, it incorporates a feedback loop between the individual level and that of the group, in which individuals imitate each other’s response to create a large segment of society engaging in similar responses to the preconditions. We thus posit that a threshold exists during a crisis in which, if sufficient stimuli are present, and transformed by sufficient individuals into individual panic behaviors, the population at large will, through imitative behavior, start to exhibit those same behaviors, leading to a mass panic. (Bissell 2015; Granovetter 1978; Porcellacchia 2020; Qiao 2019) Moreover, a tipping point being reached in one kind of panic (e.g., biological) can trigger a panic in another (e.g., financial) (Chahuán-Jiménez et al. 2021; Gunay and Can 2022).
Figure 1 shows the conceptual model through which we can understand how the discovered set of factors might facilitate mass panic arising from a biological, financial, or economic crisis. The model suggests that various external factors influence an individual’s decision-making, categorized here as financial, economic, biological, and social. The factors in the dotted bubble are only relevant during instances of a crisis of that kind—to wit, when the panic is in response to a disease outbreak, the biological factor applies (represented here in green). Similarly, if it is a financial or economic crisis, then the financial or economic factors apply.
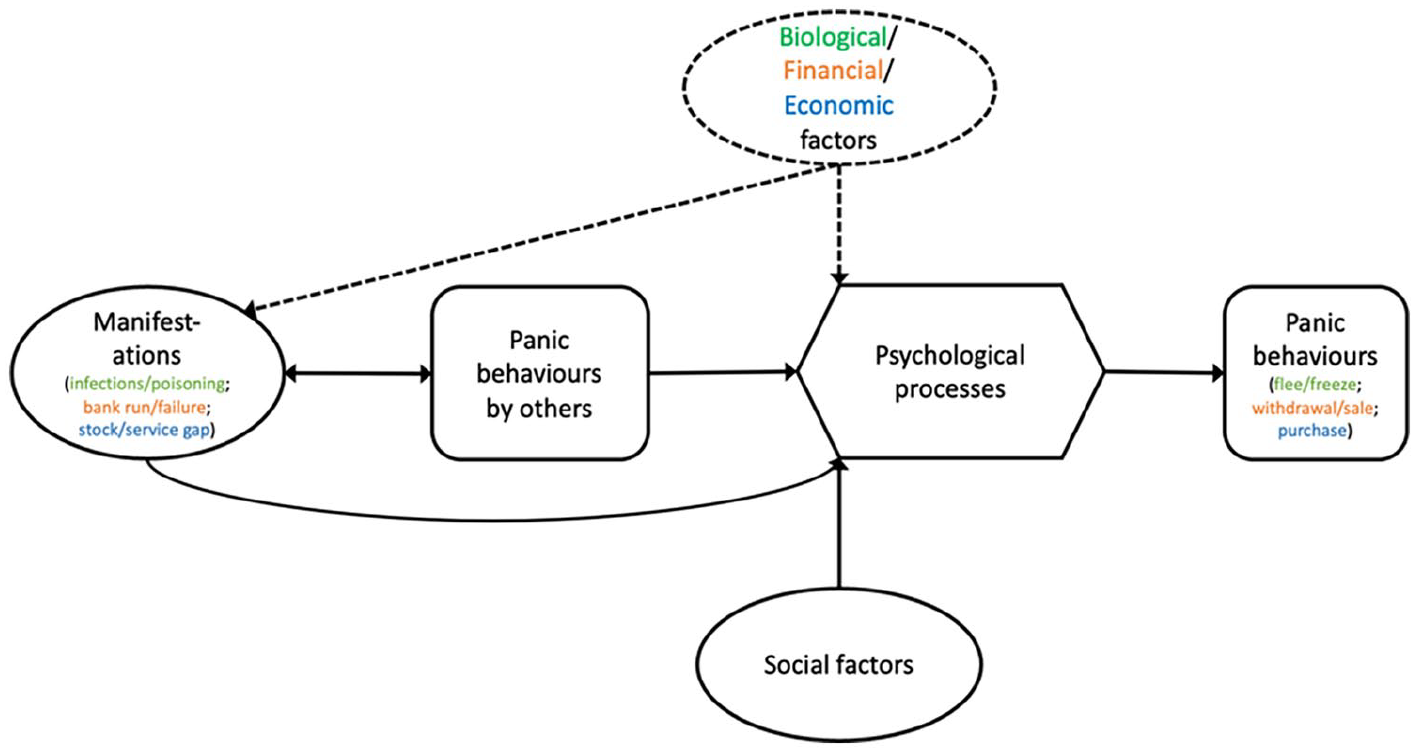
The model of mass panic.
Other inputs to this decision-making model are the behaviors of others and the observable “manifestations” associated with the crisis. “Manifestations” are those phenomena perceived by the individual as worrisome evidence of that particular kind of crisis; they serve as stimuli for panic behaviors by others as well as requiring consideration by the focal individual. Each kind of panic produces manifestations of some kind, but they have different ontological statuses, depending on the type of panic. However, they are always indicative of the kind of crisis, and otherwise not usually observed, such as people exhibiting characteristic signs of illness, forming long queues at banks or shops, or large numbers of people selling or moving house.
So manifestations are quite heterogeneous between types of crises. What unites them is that they are observable indicators of a (potential) crisis occurring in the vicinity. Biological manifestations can be symptoms of infections generated by pathogens coming into contact with hosts, with the symptoms becoming noticeable on the body or in the behavior of those infected. Financial manifestations are queues at banks or rumors of a bank run. 13 Economic manifestations can be shelves in retail outlets empty of a certain product, or an inability to access or purchase a service, or rumors of panic buying by others (Rajkumar and Yasir Arafat 2021). In all cases, social reports of these manifestations (e.g., in news feeds) can also function as manifestations, on which people can, and will, act. Note that for both financial and economic crises, panic behaviors can be manifestations (i.e., people lined up in bank queues are both). Biological manifestations, on the contrary, are produced through infection by pathogens, an invisible process. The number and speed of increase in the number of manifestations can be a significant factor in determining that one is in the middle of a crisis, and therefore that a panic response might be the best option available in such a situation.
These inputs on the left of the diagram are perceptual, translated cognitively by the individual through a variety of psychological processes (described in detail below) into behavior. If the external factors are of sufficient magnitude for that individual, then a threshold will be reached, at which point they will start to engage in the panic behaviors characteristic of that type of crisis.
Finally, in all kinds of crises, people will tend to mirror the actions of others. A central prerequisite for mass panic is psychological contagion through imitation (Billore and Anisimova 2021; Le Bon 2002). Given that in ambiguous situations people tend to imitate the behavior of others (Haghani and Sarvi 2017), one person’s panic behavior can prompt another person to mimic that behavior, should it be observed or learned about (e.g., through gossip). So while the model is couched at the level of an individual (and their psychological processes), since panic behavior serves both as an input and output of the model, there is feedback from one person’s behavior to others’, which is how one person’s fight/flight/freeze response can become mass panic, by being imitated many times by others. For example, large numbers of individuals will panic buy if they observe others panic buying, especially if they do not understand why (Marshall 1947; Ntontis et al. 2022). Panic buying of toilet paper was widespread during COVID-19. This behavior was performed firstly on a small scale and observed by others; these others often copied the behavior despite being unaware of the cause of the behavior they were observing, and felt compelled to act similarly due to the intensity of the panic-buying behavior that they perceived. One reason for this was that the perceived scarcity of certain items generated a competitive mindset (Kirk and Rifkin 2020). The imitative behavior produced the supply shortage that it sought to protect individuals against. No shortage had initially existed.
This feedback loop is more likely to occur when the speed of progression is fast (Huis in ‘t Veld and de Gelder 2015). With a rapidly spreading disease, for example, and an ambiguous social environment, individuals will look to the behavior of the crowd to gain information on how to behave. Observing panic buying on social media or via traditional media publications acted as a strong peer influence that compelled others to imitate the behavior (Prentice, Quach, and Thaichon 2022). With the advent of social media, the contagious spread of panic behaviors can now happen much faster and does not depend on the proximity of the viewer to the individual being recorded acting out the behavior.
Such panics can have a variety of consequences for the population involved—again depending on the kind of crisis—such as public health problems (excess deaths), financial system defaults, or economic downturns (not pictured in Figure 1).
Such a conceptual model allows us to reduce the chaos and complexity of mass panic cases into a concise tool. We next discuss the mechanics of this causal model in greater detail, beginning with a description of the elements that apply no matter what kind of crisis is occurring; these will be considered separately as social and psychological processes. The factors that are specific to a particular kind of crisis—biological, financial, or economic—largely derive from existing theory. Being less novel, the discussion of these elements is relegated to Appendix 2.
Social factors
We begin with a discussion of the influences on decision-making that come from the social world.
Speed and degree of spread of misinformation/rumors/conspiracy theories
For every crisis that leads to mass panic, there tends to be a parallel crisis of spreading rumors and disinformation (Brunning 2012). Rumors are produced when people need to rationalize information in an ambiguous context where there are large gaps in public knowledge (Stieglitz and Dang-Xuan 2013). Where detailed information is not forthcoming from trustworthy sources, people will fill the knowledge gap with the explanations available from elsewhere or their own imaginations. A lack of information particularly affects those with existing mental health conditions, including anxiety, which is likely to be exacerbated (McKay et al. 2020). Conspiracy theories and rumors are appealing during crises as the explanations they offer provide instant gratification in an otherwise extremely chaotic situation (van Prooijen 2022). Rumors may emerge about ways to avoid the danger (e.g., home remedies). For example, during COVID-19, Chinese social media were awash with supposed confirmation from a respectable virological institute that a traditional herbal medicine, Shuang huanglian, was effective in preventing the COVID-19 virus from replicating inside the human body (Zou and Tang 2021). This led to panic buying of the product throughout the country. Being in possession of a “remedy” may also increase an individual’s readiness to engage in behaviors that increase their risk of infection.
In historical mass panic events, the information that might cause panic (such as visible signs of disease, or rumors about some impending disaster) could spread only as quickly as word-of-mouth could travel. In societies with modern communication technologies, such contagion need not require geographic proximity or crowding, and depend only on virtual contact. In contemporary crises, images and messages can spread globally in a matter of minutes thanks to the advent of social media. During crises, social media posts that convey negative information appear to spread faster (Barbagallo et al. 2012); during COVID-19, sensationalist claims and shocking images including empty shelves at grocery shops spread quickly due to the attention that they could grab (Naeem 2021). This contributed to mass panic by amplifying and exaggerating rumors of panic buying and convincing individuals to imitate this behavior. Unfortunately, the spread of disinformation, fake news, and rumors via social media tends to outpace the spread of reliable official information (Radwan and Radwan 2020), making mass panic mitigation more difficult. Even emotions can be transmitted contagiously via social media, and during health crises, this contagion appears to speed up (Hariharan et al. 2017).
In this context, “conspiracy theories” encompass contagious ideas that claim events are being influenced by powerful actors against the public’s interest (Goertzel 2010). Such theories make mass panic more likely as they represent at least one sector of society breaking away from the official version of events during the crisis. Believing that the threat comes not from a pathogen or toxic agent (e.g.) but from an out-group, government, or other external threat can lead to noncompliance with official health-seeking or panic-control guidance, prejudice against the population that they perceive to be behind the risk, or widespread dissemination of potentially harmful disinformation—all of which undermine policymakers’ abilities to prevent mass panic behaviors from occurring (Douglas et al. 2019).
People have a deep psychological need to have explanations during a crisis, as well as a need for more existential reassurance of their safety (Barreto et al. 2020). In an ambiguous environment where governmental or other official sources are not forthcoming as to why populations are experiencing unusual phenomena (e.g., bodies are appearing on the streets in various stages of decay, as in the Black Plague Case), uncertainty and hence anxiety abounds. Conspiracy theories can fulfill the need for certainty by offering a framework of explanation where the ambiguity and chaos of the unfolding crisis can be re-ordered to the individual’s satisfaction.
Misinformation has contributed to mass panic for far longer than the internet has existed. The spread of conspiracy rumors in London, placing the blame for the Plague on Jews and/or witches, during the Black Plague via conversations in the streets was highly influential on the population’s panic behavior (Madsen 2021). Conspiratorial rumors were advanced. Official printed information regarding the Plague also promulgated conspiracy theories (McDowell 2006), giving them authority, causing deep distrust of the out-groups being blamed, and exacerbating the generalized distrust and fear within the population (Madsen 2021).
Bank runs can also be started or influenced by misinformation. Even if depositors know the rumors to be false, they have an incentive to withdraw funds if they suspect other depositors will believe the rumor (Diamond 2007).
Public level of trust in relevant institutions
In a crisis, the public’s faith is drawn to institutions for their ability to reduce the perceived risk for each individual (Cheung and Tse 2008). In this way, they feel reassured that they will not have to take matters into their own hands to ensure their survival. When a crisis is building, with rumors in general circulation and a rising number of manifestations, a population will tend to rely on their leaders, institutions, and government to present a solution. If there is strong trust in the ability of the government or other relevant institutions to handle the situation, mass panic is unlikely. There can be a “rally round the flag” effect (B. Johansson, Hopmann, and Shehata 2021) that galvanizes the population and prevents panic. For example, during financial downturns, when the public has confidence in institutions such as central banks and deposit insurance agencies, they are more likely to believe that the government and financial regulators will take appropriate actions to stabilize the financial system and protect their deposits during times of financial stress. This trust can help to prevent runs on banks by reassuring depositors that their funds are safe, even in the event of a bank failure. This trust additionally translates into a higher adherence to crisis management policies and emergency legislation introduced by governments during a crisis (Bargain and Aminjonov 2020).
On the contrary, during the BSE/vCJD crisis, governmental sources claimed that beef was safe to eat. However, the public’s awareness that different authorities presented conflicting information and advice led to outrage and the devastation of the beef market regardless of governmental statements. In the Black Plague case, looting and robbery became widespread in urban areas as there was no effective institution able to maintain public order.
Psychological processes
Our conceptual model relies on certain assumptions about factors that mediate the point at which panic behaviors occur. These conditions can modify the expected output of the conceptual model in various ways.
Personal factors
First, a variety of personal factors can influence decision-making about the need to panic.
Perceived vulnerability to the threat
One factor that varies from individual to individual is how vulnerable an individual feels to the negative effects associated with a particular kind of threat. This can manifest in beliefs about their ability to resist infection or the effects of infection (illness) by a specific pathogen (Stangier, Kananian, and Schüller 2022), or their degree of exposure to financial ruin should a bank fail (Calomiris and Gorton 1991). This can be at least partly based on the individual’s own history of episodes in which a similar kind of crisis arose. The effectiveness of their response to past situation(s) can significantly influence their processing of stimuli associated with the current crisis, giving them a degree of resilience and hence reducing the likelihood of panicking (Sherman, Arthur, and Thomas 2021).
Level of uncertainty about the nature of the threat
A potentially dominant variable is the individual’s level of uncertainty about the nature of the threat, which we have noted can determine the likelihood of the “fight-flight-freeze” system being activated, and which of these three responses will be produced (Pickering and Corr 2008). Uncertainty can arise from both a lack of information and personal experience, as well as mis- or disinformation.
Loss of control
Finally, in a crisis, individuals can perceive a loss in their ability to control the consequences of that situation through their own actions—a sense that what others are doing dominates what will eventually come out of that situation (Holsti 1989; Usher, Durkin, and Bhullar 2020). This can lead to a sense of helplessness and anxiety (Lifshin and Mikulincer 2021).
Biases
There are also a number of biases, or tendencies to weigh certain kinds of information more heavily than others, when judging the nature of a situation and potential responses to it, which impact on decision-making in a crisis.
Negativity bias
First, there is a general tendency to pay greater attention to threats than opportunities, called a “negativity bias” (Cacioppo, Cacioppo, and Gollan 2014; Rozin and Royzman 2001). Throughout our evolutionary history, there has tended to be an imbalance in the severity of outcomes or consequences: ignoring threats can be deadly, whereas ignoring opportunities is hardly ever lethal. Thus, those who were more attuned to dangerous circumstances and who made the right responses to them were more likely to survive. This selective bias meant careful individuals were also more likely to hand down the genes that made them more attentive to danger to subsequent generations (Cacioppo et al. 2014). A particular example relevant to biological panics is the asymmetrical selection pressures on predators and prey: failure at one role means death, but for the other just a missed meal (Thompson 1994). So, there is a selective advantage for prey (like people in pandemics) to over-detect threats.
The manifestations experienced in biological crises likely trigger social disgust: an anxiety that those around you could be vectors of disease. This makes individuals more vigilant in scanning their environments for potential threats (M. Johansson 2007). This heightened awareness leads individuals to make false-positive assessments of threat, for example, seeing Tylenol pills in their medicine cabinets as menacing or witnessing someone coughing during COVID-19 when that person was merely clearing their throat. Everyday nonthreatening stimuli become threatening in these conditions, pushing individuals toward the trigger threshold for panic.
Early response bias
Second, a “first come, first served” rule can come into effect in some situations of social dependence: a selective advantage accrues to those responding earlier than others when fleeing dangers like predators or avalanches (slower individuals get caught) (Diamond and Dybvig 1983; Stanford 2002), or when consumption or hoarding opportunities can be threatened by the resource stock running out (e.g., buying of foodstuffs and getting access to deposited funds) (Calomiris 1999; Chen 1999). 14 These contexts can apply to any of the emergencies relevant here and therefore can result in both mass panic and panic buying (Kirk and Rifkin 2020). So when a threat presents itself, especially if the nature and size of it is unknown, it is better to react quickly and perhaps automatically (e.g., by copying the responses of others), rather than taking time to cogitate, neutralize, or avoid the threat before others do.
Imitation bias
Third, if others are already panicking, a rational assumption is that they are likely to have better information (e.g., have seen/heard something with which you are not yet acquainted)—and so their response should be copied, especially if there are many of these other people. Even if normally these others would not be the most reliable source on which to base imitative behavior, one does so in this situation, because of the negativity bias to respond rather than not, as well as the bias to be an “early responder.” It is also beneficial to copy others when there are a number of options available in terms of behavioral response, coupled with uncertainty about the payoffs likely from each option (Turner et al. 2022). All of these factors thus reduce the level of information, time, and mental processing required to reach the trigger point.
Discussion
Physical disasters such as floods, earthquakes, tornadoes, and nuclear power plant failures tend to produce pro-social responses, as do social upheavals like terrorist attacks and emergency population displacements. This is because the danger is of known origin, briefly acute, and then gives way to a lengthy recovery period (Clarke 2002; Norwood 2005). In such cases, community cohesion is more likely to be the response (Clarke 2002; Gantt and Gantt 2012). In effect, people cooperate to address a common threat coming from the population’s shared environment (Drury, Novelli, and Stott 2013). However, in biological, financial, or economic disasters such as disease outbreaks, bank runs, and panic buying, other people become the proximate source of threat (of infection or crowding out access to resources). When this is the case, social cohesion can decrease, breaking down social bonds, and causing people to behave in an antisocial fashion. It can also mean that the crisis is not a sharp, short shock to the environment or social order, like physical disasters. Instead, the crisis can persist, getting worse or better, depending on conditions, some of which will remain unknown to the populace. This can produce significant uncertainty and, when it occurs at scale, can lead to mass panic.
In a crisis, mass panic as described in this paper is not inevitable. However, if the conditions detailed here and condensed into the conceptual model are met, the threshold can be passed, triggering a large-scale panic response. At this point, one person’s panic behavior becomes the population’s guidebook. Through imitation, panic behaviors spread throughout the community, at which point it can be considered a “mass” behavior.
A good model of mass panic should be able to make useful predictions. Prediction in specific circumstances will of course depend on the actual parameter values for the variables relevant to the kind of panic in question, which in turn depend on the on-the-ground conditions for those panic predictors. However, a general kind of prediction concerns whether one kind of panic might instigate another kind (a kind of prediction that most models of panic cannot make because they are domain-specific). For example, might a pandemic cause runs on banks? In general, our model suggests that links between different kinds of panics must occur through the factors common to both of them—which we classify as social factors (e.g., viral misinformation), psychological factors (biases and uncertainty), observation of manifestations, or the panic behaviors themselves (of the other kind). For example, our model should be able to explain why economic panics are often caused by biological ones, while the reverse type of causation rarely happens (Arafat, Kar, and Kabir 2022; Hobbs 2020). The model suggests that an economic panic can be triggered by a biological one directly by the panic response to the spreading pathogen: fleeing or freezing can result in loss of access to supplies and services, through two mechanisms: first, running off into the countryside (or isolating at home) can mean it becomes more difficult to avail oneself of product/service outlets; second, if those who own or manage economic institutions must also flee or freeze, then supply chains can be threatened and access points (such as shops) can become undermanned or closed. Both of these processes can lead to limited (access to) supplies and hence panic buying. This dynamic occurs via the following linkages: observed manifestations of new infections lead to panic behavior by others, such as fleeing. These reactions are observed by individuals who are also subject to rumors about a pandemic, and a perception of their susceptibility, causing them to flee into the country. Before leaving, those individuals think it advisable to stockpile essential supplies, so they buy unusually large amounts of various products. Word of this behavior then becomes part of the social information acquired by others still thinking about their response to rumors about a pandemic, who then decide to flee the disease, as well as to mimic the purchasing of medicines, food, and other supplies. So panic responses to both the biological and economic threats tend to proliferate through the population. In this way, biological factors can trigger economic panics. As these mechanisms are central to the model, and tied directly to panic behavior, they are likely to often be activated.
On the contrary, why do economic panics not always lead to biological ones? Economic disruptions can make a population more susceptible to the spread of disease. During times of panic buying, access points such as stores can become crowded with people, making it easier for disease to spread. Panic buying can also lead to shortages of essential items, such as hand sanitizer, soap, and tissues, which are important for preventing the spread of disease. Panic buying can also increase stress levels, which can have a negative impact on overall health. When people are stressed, they may be less likely to take proper precautions to prevent the spread of disease, such as washing their hands frequently and wearing masks. However, each of these mechanisms is weak, and all depend on the precondition of a pathogen with the right characteristics to initiate an outbreak (as defined by the biological factors in our model) being already in circulation. Therefore, the conjunction of the necessary processes is unlikely to arise, except under rare coincidences.
Pandemics could have an impact on the financial sector, including banks, through the same mechanisms that affect other service providers (as described above). However, bank closures known to occur due to under-manning, rather than a threat to the money supply, are unlikely to trigger panic withdrawals, as the cause of closure is known to be unrelated to bank reserves. On the contrary, pandemics can lead to reduced demand for money, through high levels of unemployment and a decrease in consumer spending, which can put pressure on banks to remain viable. However, the long exposure of banking systems to such economic disruptions has forced them to install mechanisms to reduce their susceptibility to panic. Primary among these is federal insurance. So, during pandemics, the involvement of most modern banks in a centralized risk-sharing system, guaranteed by the government, enables those banks to survive unusually large fund withdrawals caused by economic uncertainty. In the Spanish flu epidemic of 1918, for example, the U.S. Federal Reserve system (an early form of fund sharing) functioned quite well. By the 2020s, when COVID hit, the internationalization of this kind of insurance enabled the financial system to maintain even greater stability in the face of potential panic, resulting in very few bank runs or failures (Zhang, Hu, and Ji 2020). So, the modern financial system has become well buffered to disturbances from economic factors due to the factors included in our model: reserve requirements, and authority-based insurance schemes which distribute risk across the whole, potentially global, financial network. There is also no causal link between catching a disease or the panic buying of goods or services and the panic selling of financial instruments. As a result, financial panics are almost always caused by deficiencies in the financial sector itself, via excess speculation on financial derivatives, or lending practices such as high-risk mortgages, together with inadequate regulation and governance of the sector, and perverse incentives for those working within it (Llewellyn 2002).
Theoretically, the financialization of modern economies could mean that a banking panic could lead to panic buying of goods and services, because money, as the medium of exchange, is required to make purchases. For example, when banks fail, people become anxious about their personal liquidity, which leads to economic depression and reduced consumer spending overall, but potentially increased spending, with a rush to buy “essential goods” (on expectation that others will feel the same needs). When people become concerned about the stability of the economy or their personal financial situation, they may start hoarding essentials such as food, water, medicine, and other supplies in case of a future shortage or disruption. This sudden increase in demand can result in empty store shelves and higher prices, creating a self-fulfilling cycle of fear and panic, even in the face of a general depression (Arafat et al. 2020). However, this is unlikely, as financial panics are typically initiated or accompanied by economic depression, which limits consumer demand, rather than spurring it, so shortages of goods do not arise (Gertler, Kiyotaki, and Prestipino 2020). As a consequence, banking panics are rarely accompanied by panic buying.
Finally, neither a financial nor economic panic is likely to lead to a biological one, because flight or freeze behaviors are only a response to a perceived threat of infectious disease, which only arises with the spread of a biological agent. Financial/economic and biological crises can happen simultaneously, in parallel, but for independent causes.
The recent COVID-19 pandemic, in particular, shows a typical pattern of causation between all three kinds of panics: once it was clear a pandemic was occurring, and people were beginning to engage in panic behaviors to avoid infection, toilet paper and other necessities were widely hoarded, as people feared they would be unable to access vital supplies during potential lockdowns of unknown duration (Baddeley 2020; Keane and Neal 2021; Naeem 2021). The lockdowns in turn had significant impacts on business interests and international financial flows (Albulescu 2021; Ali, Alam, and Rizvi 2020) but national governments engaged in strategies such as “quantitative easing” of the money supply to reduce the likelihood of significant bank panics (Zhang et al. 2020). 15 So, a biological panic induced an economic, but not financial, one, as suggested by this discussion of the expectations deriving from our model.
Limitations
Numerous limitations exist in the existing literature, which make this modeling effort weaker than it otherwise could be. There is currently a limited understanding of the specific neural mechanisms underlying the contagion of disgust and fear within large groups, and a lack of comprehensive exploration into the long-term (as opposed to short-term) psychological impacts on individuals and communities of mass panic events (e.g., COVID epidemic). A more comprehensive integration of sociological and neurobiological perspectives is also needed. While there is recognition of both social and neural factors, there is little in the way of systematic examinations into how these dimensions interact and influence each other during episodes of mass panic. The role of media and information dissemination in amplifying fear or disgust during ongoing threats is acknowledged, but there is a gap in understanding the specific dynamics of information spread. Research should explore how different types of information, communication channels, and media framing contribute to the contagion of panic within populations. Evaluations of intervention strategies designed to mitigate or prevent mass panic are also rare. Future research could explore how factors such as age, socioeconomic status, or preexisting mental health conditions may amplify or mitigate the impact of mass panic in different populations.
Conclusion
This paper has shown that crises in which mass panic is a behavioral outcome share common features, even though considerably different kinds of institutions (public health, financial, or economic) and underlying agents (pathogens, bank closures, stock supplies) are involved. These commonalities have been synthesized into a conceptual model of mass panic to aid the understanding of this behavioral response. That is, mass panic is produced by circumstances with consistent features throughout history—features that have withstood enormous changes in culture, behavior, language, technology, and ways of living. As a consequence, mass panic can be understood as a specific kind of problem that requires the attention of stakeholders in the social order.
Because the preconditions for mass panic arise fairly rarely, this might suggest that mass panic should not concern scientists, media, or governments. However, when it does occur, it can lead to incredibly costly consequences in the short and long term—the destruction of many lives and/or livelihoods. For this reason, providing a new way of thinking about these situations, and their common causes, can be not only instructive, but crucial to social welfare.
In future crises, this model could be used to assist policymakers under time pressure to respond effectively in ways that prevent the trigger threshold from being reached. Such offices need specific advice for how to forestall mass panics of each kind. The means of recognizing the initial stages of a crisis of any of these kinds are well-known to the relevant experts—epidemiologists and economists. Essentially, they monitor the values of the crisis-specific factors for each type (listed in Appendix 2) through surveillance strategies of various kinds, enabling them to identify “hotspots” where viral infections might be breaking out, or logistical problems at crucial junctures of supply chains that presage a stock-out.
Once a (potential) crisis has been identified, surveillance systems set up to monitor variables specific to that kind of mass panic should then rush into action, and begin conducting preplanned activities. These could include running social surveys to measure aspects of trust in the relevant social institutions or to monitor frequency-of-mention trends for terms identifying any conspiracy theories that spring up around it, circulating on social media networks. Levels of psychological traits such as perceived vulnerability to the relevant kind of threat, or increases in generalized anxiety, could also be measured. So, our model would suggest that it is also incumbent upon public officials to keep track of other factors—essentially the social and psychological factors in the model which are generic to all such panics—if they want to shut down the dynamics that lead from crisis to mass panic. In this way, governments and other institutions can become vigilant about the symptoms before the behaviors start to be widely imitated, as a means of forestalling the progression to a full-blown mass panic, with all of its costs. In this way, we hope that the modeling effort conducted here can help to limit the occurrence and severity of future mass panics.
Supplemental Material
sj-docx-1-jax-10.1177_19367244241245702 – Supplemental material for Understanding Mass Panic
Supplemental material, sj-docx-1-jax-10.1177_19367244241245702 for Understanding Mass Panic by Henry W. Fletcher and Robert Aunger in Journal of Applied Social Science
Footnotes
Acknowledgements
The authors thank Justin Aunger and Deborah Colson for commenting on previous versions of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
As the paper depends entirely on the analysis of secondary data, no ethical permissions were sought.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.