
Abstract
In an effort to reduce food access issues for older adults, the United States Department of Agriculture’s (USDA) Commodity Supplemental Food Program (CSFP) provides monthly food assistance specifically for low-income older adults through local food banks. The purpose of this study was to explore factors that influence an older adult’s performance in food-related activities. Older adults eligible to receive a monthly senior food box from community food distribution sites were recruited to complete a survey. The survey included home information, Patient-Reported Outcomes Measurement Information Systems (PROMIS®) v1.1 Global Health measure, individualized supplemental food utilization profile (FP), and a kitchen inventory. Descriptive and statistical analyses were performed. From December 2021 until March 2023, n = 200 participants were recruited and n = 36 took the survey for an 18% completion rate with a mean age of 71 years old; 61% were female and 36% were male. Of the participants who took the survey, 64% (n = 23) acknowledged having at least one chronic disease and 89% (n = 32) indicated they prepared meals for themselves. The OPMF revealed grocery shopping, cooking, and eating as “extremely important” and directly related to their performance and satisfaction. The FP rate revealed that 61% (n = 22) of participants always use 100% of their food box by the end of each month. While the participants in this study report having at least one chronic disease, most are functional and independent when it comes to food-related activities, and most report that they have the tools to manage and use their food resources.
Introduction
According to the World Health Organization (2020), healthy aging is not necessarily the absence of disease but the process of developing and maintaining the functional ability that enables well-being in older age. One key determinant for healthy aging includes accessing and consuming nutritious foods (Abud et al. 2022). A number of food-related activities must occur in order to access and consume well-balanced meals such as preparing shopping lists, transporting grocery items, planning, preparing, serving, and cleaning (American Occupational Therapy Association [AOTA], 2020). Participation in food-related activities contributes positively to older adult identity maintenance and supports healthy aging (Plastow, Atwal, and Gilhooly 2015). Occupational therapy practitioners (OTPs) therapeutically use everyday occupations, like meal preparation and grocery shopping, to enhance and enable productive aging (AOTA 2020). Unfortunately, many older adults who experience chronic disease, impacting their cognitive, psychosocial, and physical health, find that their chronic conditions and associated functional impairments negatively impact participation in these important food-related activities.
While many older adults live with the effects of chronic disease, many also live in poverty (10.3%), according to the United States Census Bureau (Creamer et al. 2022). Older adults who are economically insecure struggle with rising housing and health care bills, inadequate nutrition, lack of access to transportation, diminished savings, and job loss (National Council on Aging 2022). Food insecurity is a potential consequence of economic insecurity and has traditionally been defined and measured as an inability to acquire adequate food due to a lack of money and other resources (Coleman-Jensen et al. 2022). Even though access to food resources for economically insecure older adults is available to many for pick up at local food banks and pantries, and in some cases, food bank home delivery, older adult food insecurity persists.
According to the 2021 State of Senior Hunger report, adults over 60 years of age, those who are from racial and/or ethnic minorities (specifically Black or Hispanic), those with disability, and those with incomes below the poverty level, were most at risk for food insecurity in the United States (Ziliak and Gundersen 2023). This report defines food insecurity based on the number of affirmative household responses to the 18-item United States Department of Agriculture (USDA) Food Security Supplement, which focuses specifically on access to food (Ziliak and Gundersen 2023). Ziliak and Gundersen (2023) estimate that 7.1% or 5.5 million older Americans are food insecure.
The top five states with the lowest percentage of food-insecure seniors are North Dakota (2.8%), Nebraska (2.9%), South Dakota (3.4%), Hawaii (3.7%), and Washington (3.7%) (Ziliak and Gundersen 2023). The top 5 states and territories with the highest percentage of food-insecure seniors are all located in the South and include Louisiana (13.4%), Mississippi (12.6%), the District of Columbia (11.2%), South Carolina (10.4%), and West Virginia (10.2%) (Ziliak and Gundersen 2023). Texas, where this study was completed, is one of the most populous states in America and, according to the State of Senior Hunger report, is one of the top 10 states with the highest percentage of food-insecure seniors (8.5%) (Ziliak and Gundersen 2023). According to a Meals on Wheels America (2022) Texas Fact Sheet, 18% of the state’s population are adults over the age of 60, approximately 40% of the population identifies as a minority, 30% report living with a disability, and 10% of older adults live in poverty, all risk factors for older adult food insecurity.
In an effort to reduce food access issues for older adults, the USDA Commodity Supplemental Food Program (CSFP) provides all 50 states monthly food assistance specifically for low-income older adults, 60 years and older, through local community food banks (U.S. Department of Agriculture [USDA], 2019). Despite federal funding for food access programs, older adult food insecurity remains a complex, multidimensional issue (Schmelzer and Leto 2018). In defining and finding solutions to this problem, researchers suggest including measures of physical food insecurity when assessing risk in the older adult population, which includes measures of functional limitation and social support (Lee 2022; Tucher et al. 2021; Vaudin, Moshfegh, and Sahyoun 2022).
The original definition of food insecurity, from the Food and Agriculture Organization (FAO) of the United Nations (UN), is broader than the definition used by government organizations in the United States (Food and Agriculture Organization [FAO], 2008). The FAO (2008) states that food insecurity is a food access issue and the ability or inability to utilize and manage food resources. This definition, while from 2008, expands our current view of food insecurity from not just an economic access issue but one that includes evaluating the physical and cognitive utilization and management of food resources. Using this expanded definition in our understanding of this complex issue may help researchers, healthcare practitioners, and community workers develop holistic programming to reduce older adult food insecurity.
The purpose of this study was to explore the factors that influence an older adult’s performance of food-related activity including not just accessing but also managing food resources from a convenience sample in North Texas. The study participants were low-income older adults, living in North Texas, who receive monthly food supplements distributed regionally by the North Texas Food Bank and locally from community food banks. Since food insecurity is an emerging area in occupational therapy practice, the results of the survey will help inform those practitioners who work with older adults on the impact of food insecurity and functional health. We hope that this study will also inform future occupational therapy studies and programs that may help remediate and/or modify the factors that impact the performance of food-related activities for older adults.
Theoretical Framework
The Person-Environment-Occupation Model of occupational performance was used to design this study (Law et al. 1996). Occupational performance is the outcome of the transaction of the person, environment, and occupation (Law et al. 1996). In this study, occupational performance is the performance of food-related activities; the older adult is the person who qualifies for and participates in the CSFP monthly food box program, the environments are the contexts in which these activities take place, and the occupations are all of the activities that encompass accessing and managing food resources. The model assumes that these three components interact continually across time and space in ways that increase or decrease their congruence (Law et al. 1996). The survey instruments were designed and chosen to look at each aspect of the occupational performance of food-related activities (preparing, shopping, cooking, cleaning up, the home environment, self-reported chronic diseases, etc.). One of the goals of the study was to determine if there were any major components lacking that might benefit from a holistic occupational therapy approach in the future.
Methods
A cross-sectional descriptive study design, using quantitative methods was used for this study. Approval for this study was obtained from the Texas Woman’s University (TWU) Institutional Review Board (IRB) (approval number: IRB-FY2022-73).
Research Setting
This study was conducted at a variety of North Texas food distribution sites. At the time of this study, the North Texas Food Bank used two types of food distribution sites. One was a drive-thru model where food box participants drove their own vehicles to pick up their box and the other was a pick up site within a local community center.
Recruitment and Data Collection
Two hundred (n=200) older adults who picked up a monthly senior food box called CSFP from community food distribution sites were recruited to participate in this study, via convenience sampling between December 2021 and March 2023. The CSFP is a pre-packaged 35-pound box of non-perishables provided by the USDA and managed by the North Texas Food Bank (NTFB) and the Texas Department of Agriculture (North Texas Food Bank, N.d.). Older adults were eligible to receive the food box if they were 60 years or older, were a resident of North Texas, and met governmental income guidelines (North Texas Food Bank, N.d.). Data for this study was collected using an electronic survey via REDCap, which assessed older adults’ personal and contextual factors regarding food-related activity performance and utilization of their monthly supplemental food box (Harris et al. 2009). The survey consisted of six instruments:
The investigators recruited participants by distributing survey fliers to those interested at the North Texas distribution sites. Participants were eligible to complete the study’s survey if they were between 60 and 98 years old. The bottom age range is aligned with CSFP participation requirements which are set by the USDA. Additional study inclusion criteria included being a participant in the CSFP program, the ability to read English or Spanish at a 5th-grade level or higher, and access to a device capable of accessing the internet for 10 minutes uninterrupted. The study flier described directions for accessing the survey online. Interested participants could take the study flier and complete the survey at home by accessing the website link and/or QR code on the flier with their own device at their own discretion. Alternatively, interested participants could complete the survey onsite using a device provided by the study team. Participants who chose to take the survey onsite did so in a private office or in a separate parking area to ensure their privacy. The survey took 15–20 minutes to complete.
Data Analysis
All data were downloaded from the REDCap survey (Harris et al. 2009) into a Microsoft Excel (Microsoft Corporation 2023) spreadsheet to generate descriptive statistics. Means, standard deviations, and frequencies were reported for the sample variables. Data from the PROMIS® were analyzed by the HealthMeasures Scoring Service (HealthMeasures 2023).
Results
Demographic Characteristics
A total of 200 older adults were recruited, and 36 completed the survey for an 18% completion rate. Demographic characteristics of the 36 survey participants are listed in Table 1. Participants’ mean age was 71 years old, with a range from 60 to 85 years. More participants reported their gender as female (61%) than male (36%). Most participants (44%) indicated their race was “other” or “unknown/not reported.” The second most frequently indicated race was Black or African American (39%), followed by White (17%). Participants (61%) most frequently described their ethnicity as Hispanic or Latino.
Participant’s Demographic Information.
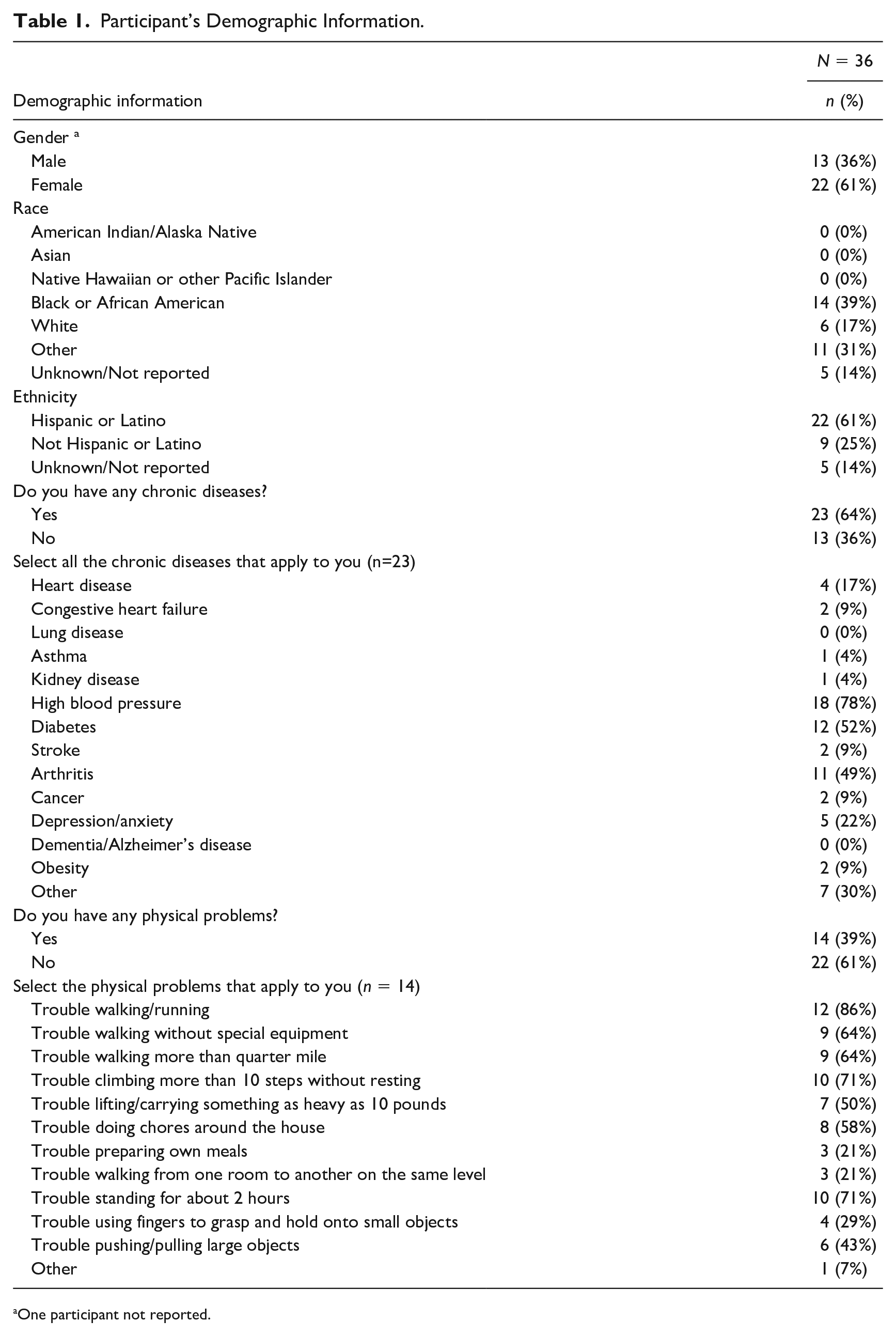
One participant not reported.
The majority of participants (64%) acknowledged having at least one chronic disease. Of the participants who responded affirmatively, 78% reported having high blood pressure, followed by arthritis and diabetes at 49 and 52%, respectively. Only 39% of all participants confirmed having a physical problem. Of those participants, “trouble walking/running” was the most common (86%), followed by “trouble climbing more than 10 steps without resting” (71%), difficulty “lifting/carrying something as heavy as 10 pounds” (50%), “trouble using fingers to grasp and hold onto small objects” (29%) and “trouble preparing own meals” (21%).
Home Information
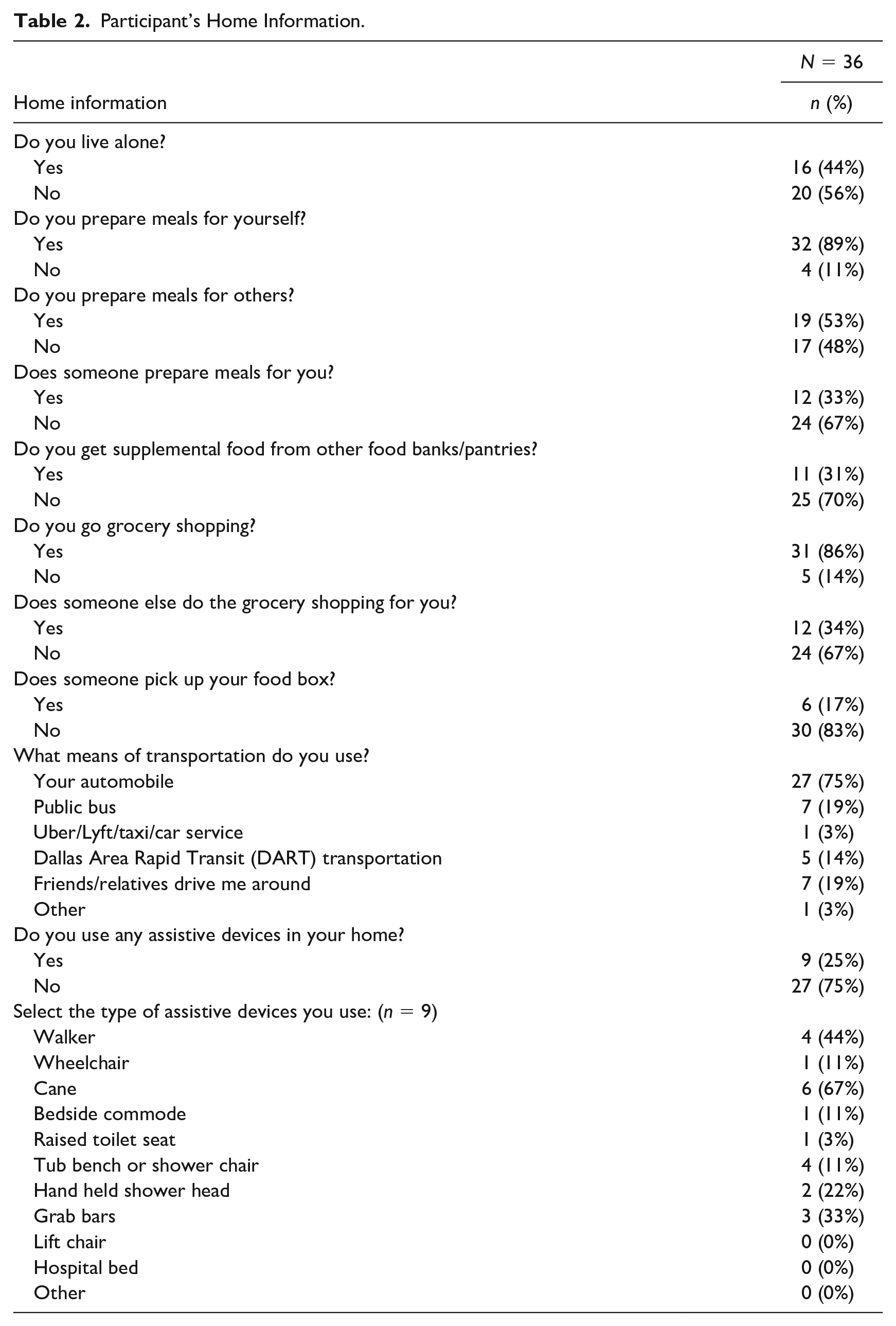
Less than half of participants (44%) reported living alone (Table 2). A majority of participants (89%) indicated they prepare meals for themselves. About half of the participants (53%) also indicated they prepare meals for others. Most participants (86%) go grocery shopping. A personal-automobile was identified as the most common means of transportation (75%). Most participants reported not using an assistive device in their home (75%). However, the most frequently reported devices by those who did indicate using a device were cane (67%), walker (44%), and grab bars (33%).
Participant’s Home Information.
PROMIS®
The participants’ PROMIS® SF v1.1—Global Physical Health average T score was 44.4 (Table 3). Their average T score on the PROMIS®—Global Mental Health was 49.9. Both of these T score averages were near the average T score for the general population (Hays et al. 2009). For both instruments, the majority of participants (53% physical health and 56% mental health) received a score below the average for the general population, while 47% (physical health) and 44% (mental health) of participants scored above the general population average for each instrument.
Participant’s Patient Reported Outcomes Measurement Information System (PROMIS) Short Form (SF) v1.1 - Global Health Mean Scores.
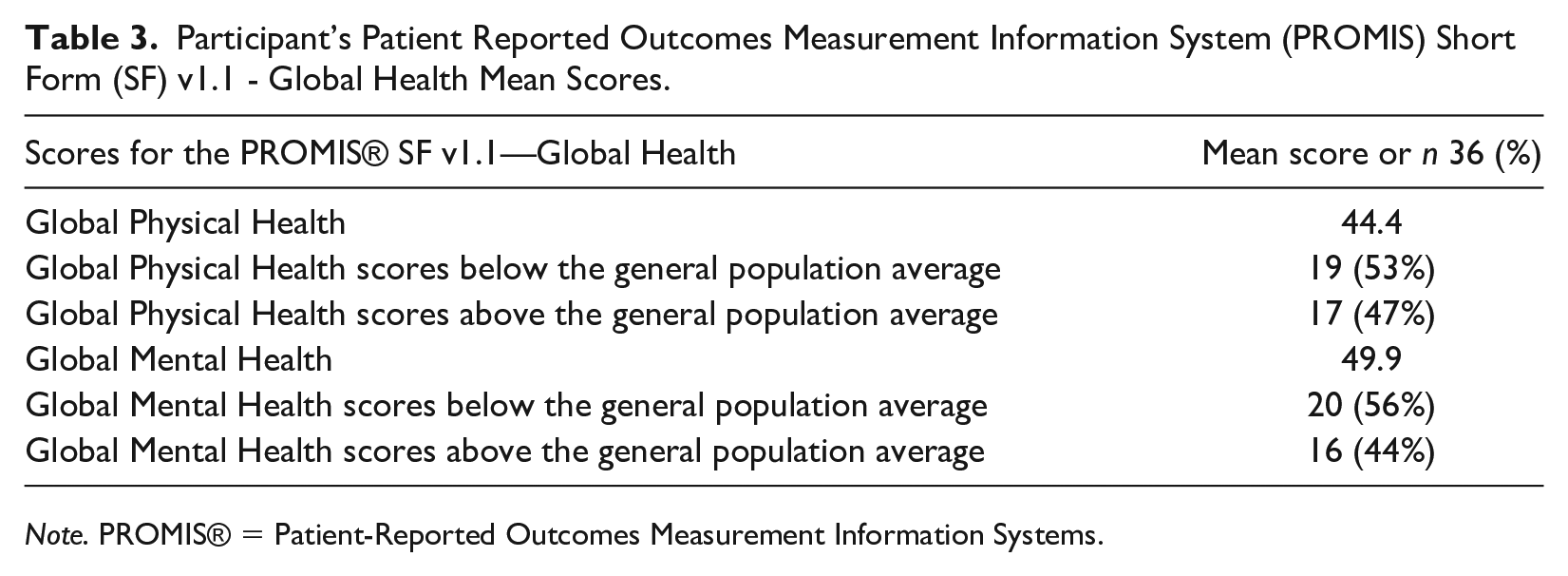
Note. PROMIS® = Patient-Reported Outcomes Measurement Information Systems.
Occupational Performance Measure of Food Activities
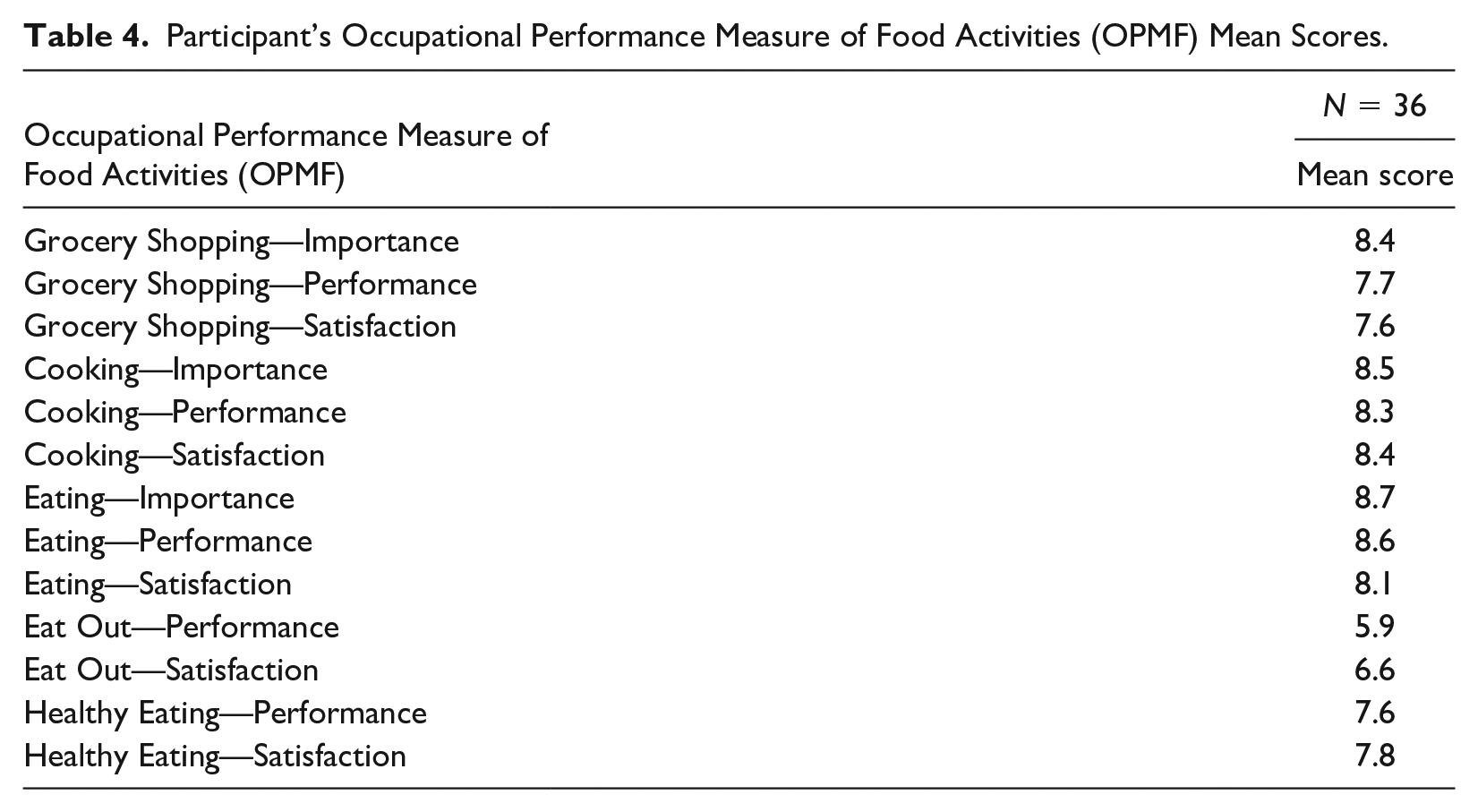
A majority of participants reported grocery shopping, cooking, and eating as “extremely important” (55%, 61%, and 66%, respectively). Table 4 shows the mean performance and satisfaction scores for the various food activities. None of the mean scores for performance and satisfaction fell below 5.0 for any of the food activity items. Participants rated their performance and satisfaction with eating out lowest, with mean scores of 5.9 and 6.6, respectively. The highest rated mean score for performance was for eating at 8.6. Eating also had the highest satisfaction score, with an average of 8.1.
Participant’s Occupational Performance Measure of Food Activities (OPMF) Mean Scores.
Individualized Supplemental Food Utilization Profile
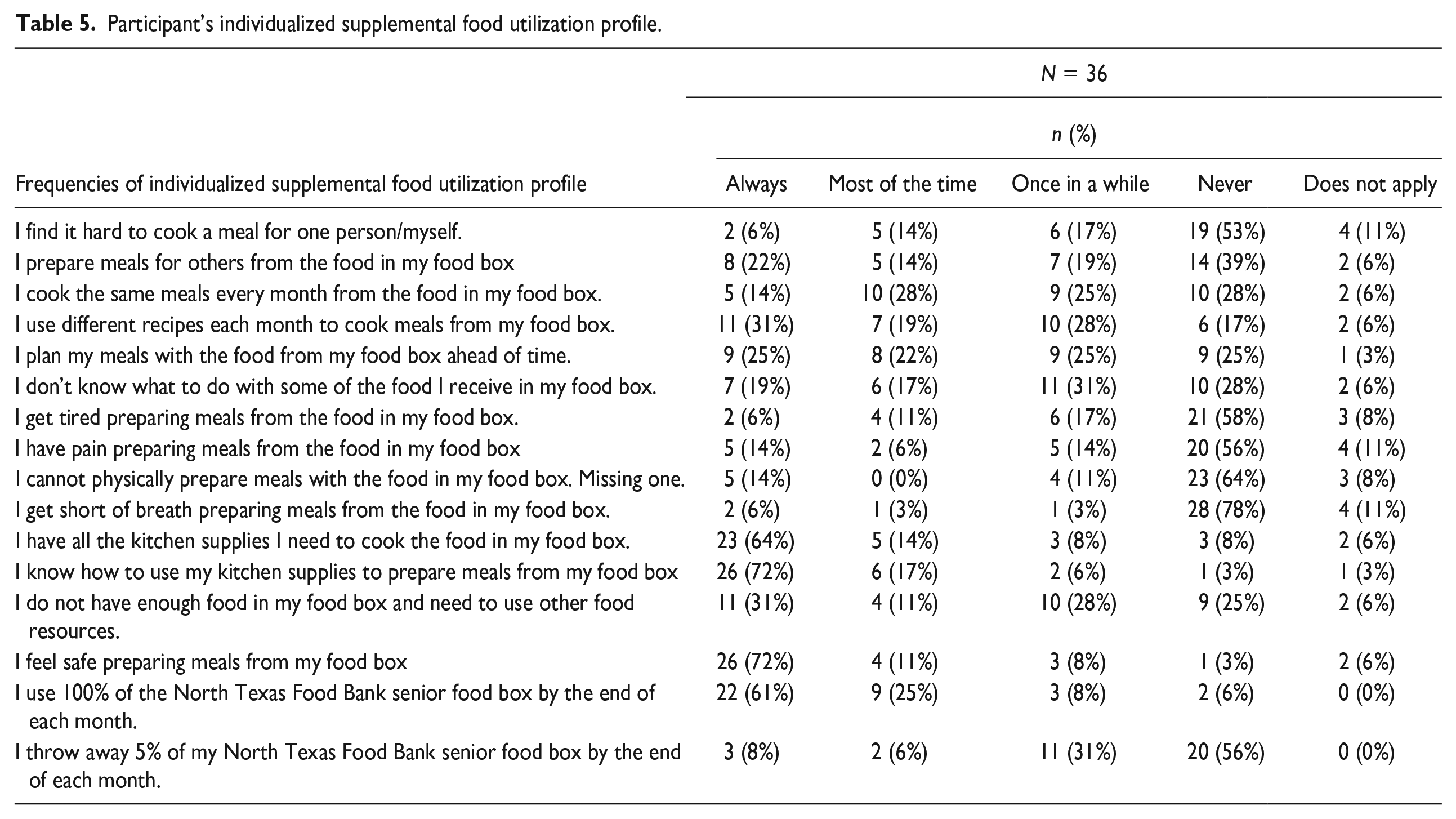
A majority of participants indicated they always “use 100% of their NTFB senior food box by the end of each month” (61%) (Table 5). Few participants (8%) reported always “throw[ing] away 5% of [their] NTFB senior food by the end of each month.” The most frequent response reported for the need to use other food resources in addition to the food box was always and never (31% each), followed by once in a while (28%), most of the time (11%), and does not apply (6%). Only a few participants (14%) reported they always “cannot physically prepare meals with the food in [their] food box” while 17% reported “get tired preparing meals from food in [their] food box” once in a while. Some participants (14%) also indicated once in a while for the frequency of having pain preparing meals from food in their food box. About 31% responded once in a while to not knowing “what to do with some of the food [they] receive in their food box.”
Participant’s individualized supplemental food utilization profile.
Kitchen Inventory
Of the kitchen items, 31 of them were owned by at 50% of participants (Table 6). Almost all participants (94%) reported having a refrigerator. Other frequently selected items, stove/range, oven, and frying pans, were each selected by 89% of participants. The second most frequently selected items were a chef’s knife/utility knife, can opener, and sauce pans, which were indicated by 80%, 80%, and 78% of participants each. The two least frequently reported items were an Instapot (8%) and a food processor (22%).
Participant’s Kitchen Supply Inventory.
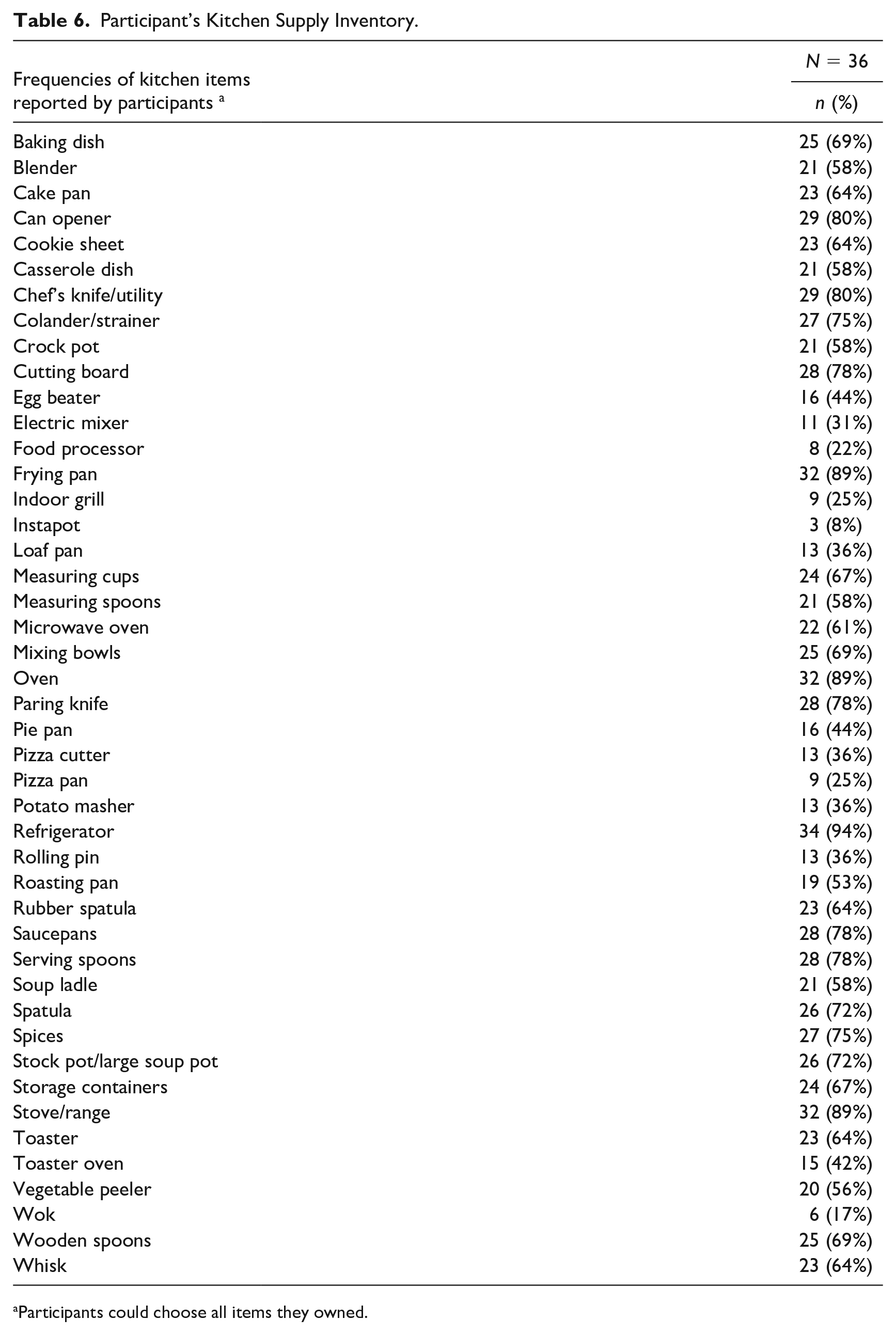
Participants could choose all items they owned.
Discussion
OTPs possess skills in analyzing an individual’s performance of food-related activities as well as evaluating the personal and environmental contexts in which these activities occur (AOTA 2020). OTPs are in a distinct position to address factors associated with food insecurity in older adults including the factors that occur within the environment and within the person, specifically those caused by physical, cognitive, and psychosocial conditions (Juckett and Robinson 2019). The purpose of this study was to explore the factors that influence an older adult’s performance of food-related activity including not just accessing but also managing food resources from a convenience sample in North Texas.
The majority of participants (64%) in this study reported having at least one chronic disease, which is consistent with the Center for Disease Control’s (CDC) National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP 2022), which states that 6 in 10 adults have at least one chronic disease. While the study recruited a small sample (n = 36), there was good representation from racial and ethnic minority groups (Hispanic 61% and African American 39%), which is consistent with the literature in that racial and ethnic minorities are at risk for food insecurity (Tucher et al. 2021). The participants’ self-reported chronic diseases were also consistent with some of the most common conditions experienced by older adults in the United States: hypertension, high cholesterol, arthritis, coronary heart disease, and diabetes (NCCDPHP 2022).
Tucher et al. (2021) established a novel summary indicator of food insecurity in a nationally representative cohort of older adults. Frailty status, being homebound, being socially isolated, experiencing community disability, being a racial minority, being female, and having a high number of comorbidities were highly associated with food insecurity. Overall, this study’s participants indicated good function and community mobility as only 39% reported a physical problem, 75% drove their own vehicles to pick up their food boxes, and most reported not using assistive devices. In addition, the respondents indicated satisfaction with their food boxes; most used all of the food resources each month, while very few reported difficulties managing these resources. It also appears that most participants have the kitchen tools needed to prepare their food resources at home. According to this study’s findings, having access to this monthly box of food is important and it may contribute to the participant’s overall functional independence.
Because this sample has more older adults who are independent and functional, it is unclear whether the North Texas older adults who participate in CSFP who have less independence and more functional limitations could potentially benefit from occupational therapy (such as those who have their food box delivered or picked up by proxy). Various studies have previously reported associations between food insecurity and functional limitations (Jackson et al. 2019; Lee and Frongillo 2001; Petersen et al. 2019). Another study found that having a disability, physical or mental, was related to food insecurity (Hadfield-Spoor, Avendano, and Loopstra 2022). Having both physical and mental disabilities increased the threat of food insecurity, and each subsequent disability raised a disabled individual’s chances for food insecurity. Feeding America surveyed older adults who participated in various food assistance programs to better understand their needs and found the majority of older adults reported problems with transporting heavy food items (Frongillo and Warren, N.d.). Older adults also reported difficulties with food preparation activities, mobility, and transportation.
Developing community programs to address food insecurity is an emerging practice area in occupational therapy. New approaches to addressing food insecurity and its base causes are important and necessary (Juckett and Robinson 2019; Martin et al. 2013). For example, a participant's choice of food pantry, motivational interviewing, and individualized service referrals resulted in improvements in participants’ food security and self-sufficiency scores (Martin et al. 2013). Adams et al. (2022) concluded that OTPs need to work with communities when seeking to address social issues, which include food insecurity. Schmelzer and Leto (2018) used an occupation-based program consisting of a group discussion of goals, an experiential activity, and group reflection, resulting in statistically and clinically significant improvements in perceived satisfaction and performance of food-related activities. OTPs have a role in providing interventions to maintain physical functioning and independence in older adults and to help prevent the development of functional limitations and disability in this population.
Conclusion and Recommendations
This study captured information regarding physical and functional histories and food-related activities in a mostly minority respondent group receiving government funded food assistance. While the participants in this study report having at least one chronic disease, most are functional and independent when it comes to food-related activity performance and most report that they have the tools to appropriately manage and use their food resources. Almost all report using all of the food received in their monthly food box, which indicates how important these resources are and that the supplemental food may contribute to their health and function. Future research should investigate the possible occupational therapy needs of those who receive their CSFP box via a proxy and who have less functional independence. Researchers should also explore potential difficulties regarding the functional transport of large or heavy food items, like the CSFP boxes.
Footnotes
Acknowledgements
The authors would like to thank the North Texas Food Bank.
Authors’ Contributions
The authors conceived the idea and reviewed the literature. All authors read, edited, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for research, authorship, and/or publication of this article: Funding provided by Texas Woman’s University for graduate assistant support.
Ethical Approval
The Texas Woman’s University (TWU) Institutional Review Board (IRB) reviewed and approved this study involving human participants (TWU IRB #: IRB-FY2022-73).