
Abstract
The Healthy Families Healthy Kids Initiative (HFHKI) is a community-based initiative developed based on the socio-ecological model to address preventive health care needs in El Paso County, Texas, one of the most economically and health-challenged border communities in the United States. HFHKI’s three main goals are to increase access to experiential learning and health education, service delivery, and sustainable systems/linkages of care. These were accomplished through seven critical activities. We present the rationale, background, setting, and conceptual framework for the initiative, followed by the methods used to develop and assess the success of the activities and results of our project outcomes. We end with a discussion of lessons learned and future directions. We also share insights gained from our community health promotion intervention during the COVID-19 pandemic, which will enrich current conversations among applied social scientists. Overall, our project served 2,347 participants of all age ranges during our first year of project implementation across all 7 activities. We recommend the use of the socio-ecological model in designing, implementing, and improving health interventions aimed at enhancing family and community health, with each intervention tailored to the needs of different segments of the community. While the need to contain the COVID-19 virus amid the pandemic has created challenges in health promotion efforts, the need to help affected communities regain control of their health cannot be stressed enough. Our project can serve as an implementation framework for community-based projects on the U.S.-Mexico border.
Introduction
Health disparities are a persistent concern in the United States, with ethnic-racial minorities disproportionately affected by striking health inequalities, their associated social inequities, and compounded health risks (Office of Disease Prevention and Health Promotion 2022). Compelling evidence suggests that structural disparities can hinder social mobility and access to health care, which can create a disproportionate burden of preventable diseases, chronic diseases, premature death, and other adverse outcomes that interfere with daily functioning and the ability to achieve optimal health among ethnic-racial minorities (Centers for Disease Control and Prevention [CDC] 2022a, 2022b). The Pew Research Institute noted that Hispanics continue to be the largest minority group in the U. S., constituting 19% of the nation’s population, with 62.6 million individuals in the U. S. identifying as Hispanic in 2021 (Lopez, Krogstad, and Passel 2022), and this number is expected to reach 111 million by 2060 (U.S. Census Bureau 2018). Counties in states located along the U.S.-Mexico border and Northeast and Midwest states with historically large Hispanic populations continue to drive the growth of the Hispanic population (Passel, Lopez, and Cohn 2022). Culturally and linguistically competent community-based interventions that promote healthy ecology can lead to positive outcomes and meet the needs of all Hispanics, especially those along the U.S.-Mexico border region.
In this paper, we address the research question: How can health promotion projects engage border communities to promote health and well-being while navigating the challenges faced by the COVID-19 pandemic? We describe in detail the establishment of the Healthy Families Healthy Kids Initiative (HFHKI), a community-based initiative developed based on the socio-ecological model and housed in The University of Texas at El Paso (UTEP) to address preventive health care needs in the community (HFHKI N.d.).
El Paso County shares many of the economic challenges of the poorest Texas counties, in addition to a multitude of health concerns faced by border communities. As one of the largest binational communities distinct from major metropolitan cities in the U. S., the health circumstances faced by the residents of El Paso County are unique. These include its proximity to Mexico, high poverty rates, the prevalence of communicable/chronic diseases, stark health disparities, shortages of health providers, and limited health care access (Office of Border Public Health 2019; Reyes et al. 2008; United States–Mexico Border Health Commission [USMBHC] 2010). This article sheds light on the challenges faced and lessons learned during the first year of our project implementation. We hope that the insights gained from our community health promotion intervention can help enrich current conversations among other applied social scientists and serve as a framework for practitioners starting new health initiatives in similar communities. We start with a review of the literature and the theoretical framework driving our research design, followed by a description of our project setting, study design, and data collection and analyses. We end with findings, lessons learned, and conclusions.
Literature Review
Background
Past research indicates that Hispanic children are more likely to live in poverty compared with non-Hispanic White children and those from other racial groups (Murphey et al. 2018). Economically disadvantaged families have less access to adequate, safe, and nutritious food (Feeding America N.d.) and are less likely to have health insurance and use preventive health care services (Tolbert, Drake, and Damico 2019). Structural disadvantages and lack of health care insurance can lead to delays in medical treatment and diagnoses at more advanced stages. Moreover, students living in poverty are less likely to do well in school, to perform at a level comparable with students from higher socioeconomic status backgrounds, and to attend college or graduate from college (National Center for Education Statistics 2015). Students from low-income families must also confront a number of bio-psycho-social health risks such as exposure to acute or chronic stressors and environmental safety hazards (Evans and Kantrowitz 2002; Schreier and Chen 2013). Inability to afford health care coverage, lack of knowledge of available services, poor care coordination, and shortages of health care providers can impact the receipt of treatment and service continuity (Texas Department of State Health Services 2018). Socioeconomic marginalization not only widens health disparities but may lead to the perpetuation of structural disadvantages and an intergenerational cycle of poverty that can be difficult to break without strategic interventions.
Health disparities along the U.S.-Mexico border region are a long-standing public health concern given the extremely high number of people without health insurance, particularly in rural and semi-rural communities (USMBHC 2010). Lack of health insurance is linked to a lack of quality health care coverage, low or no access to preventive health care services, and minimal health care treatment (Sommers, Gawande, and Baicker 2017; Woolhandler and Himmelstein 2017). Hispanics comprise the largest group of uninsured adults and the smallest group of individuals with private insurance coverage, compared with non-Hispanic Whites, non-Hispanic Blacks, and non-Hispanic Asians (U.S. Census Bureau 2022; U.S. Department of Health and Human Services [DHHS] 2018). In terms of health, obesity has been a widespread health concern among Hispanics for the past two decades (Salinas et al. 2020), with Hispanic children being almost twice (1.8 times) more likely to develop obesity than non-Hispanic White children (DHHS 2020). Obesity is a risk factor for an array of chronic diseases such as cardiovascular diseases, diabetes, hypertension, cancer, and sleep apnea (National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK] N.d.; Pi-Sunyer 2009). Physical activity is a key component in preventing and managing many health conditions, as participation in physical activities can help reduce the risk of obesity and many other health conditions such as cardiovascular diseases, type 2 diabetes, high blood pressure, cancer, and stroke (CDC 2022c; NIDDK N.d.). Physical activity also helps regulate emotional and mental health by reducing the risk of depression and anxiety (CDC 2022c). However, parks and other publicly accessible recreational facilities that help promote engagement in physical activities are not equally distributed in racial minority (Hispanics and Blacks) neighborhoods and low-income neighborhoods facing financial strain (Moore et al. 2008).
Conceptual Framework of This Health Promotion Intervention
The conceptual framework and underpinning theory for this intervention were adapted from the socio-ecological model. The origins of the socio-ecological model can be traced back to the ecological systems theory developed by the American psychologist Urie Bronfenbrenner in the 1970s to understand and describe the context of human development, where he depicted a conceptual model as nesting circles that place individuals in the center. Specifically, Bronfenbrenner used five different systems within which children have close connections to illustrate the dynamic and complex systems of their surrounding environment, namely, the microsystem that encompasses the individuals’ immediate surroundings (e.g., parents, siblings, and teachers); the mesosystem comprising networks of microsystems and interactions between microsystems; the exosystem referred to as remote social settings that indirectly impact individuals (e.g., neighborhood and workplaces); the macrosystem that entails the overarching norms, values, customs, and laws that shape the structures and exchanges between the other systems; and the chronosystem, which involves life events, transitions, and changes across the life span (Bronfenbrenner 1974, 1977, 1979, 1986). Bronfenbrenner’s work helps establish the foundation for understanding the multifaceted nature of human relationships with their environment. Over the years, the socio-ecological model has evolved, been refined, expanded, and prevalently adopted to advance different fields including biology, psychology, education, social work, and public health (Paat 2013; Richard, Gauvin, and Raine 2011). Furthermore, the use of this holistic model in health promotion programs to improve well-being is becoming more evident in health research central to closing the gap in disparities and increasing the strength and effectiveness of community-based interventions (Caperon, Saville, and Ahern 2022; Kennedy et al. 2021; Zhang and Warner 2023).
The CDC (2007) introduced a four-level framework of the factors informed by the social-ecological model to illustrate the importance of the interplay between individuals, relationships, community, and societal factors, as well as the central role that the larger contextual determinants of health play in prevention strategies. In examining community engagement, Caperon et al. (2022) proposed the use of the socio-ecological model to develop multilevel solutions and identify systematic roadblocks to tackle barriers to engagement in health initiatives. To date, the socio-ecological model has been widely applied or recommended in studies focusing on violence prevention, health promotion, substance abuse treatment, obesity prevention, and cancer prevention, among others (e.g., Akinyemiju et al. 2022; Manuel et al. 2017; Quick et al. 2017; Sabri et al. 2022). The model remains ideal for understanding frameworks for the practice of community engagement through acknowledging the complex relationships between different systems and recognizing that divergent life outcomes are impacted by multiple interconnected factors (e.g., individual or group effects can create ripple or “spillover” effects), which allows practitioners to identify factors that contribute to poor life outcomes, pinpoint leverage points for change, and promote equitable outcomes (CDC 2015). It is imperative for applied social science practitioners serving disadvantaged communities to develop approaches to circumvent barriers posed by socioeconomic deprivation and health inequities to help their communities attain their highest level of health.
Method
Setting
El Paso County is located at the intersection of three states (Texas and New Mexico in the U.S., and Chihuahua in Mexico). The county shares a border with Ciudad Juárez (also known as Juárez), one of the largest cities in Mexico. Both Juárez and El Paso (City and County) maintain close cultural connections in addition to geographical proximity. The border has historically been fluid, with residents from both cities frequently crossing the border to visit family and relatives, shop, or attend school or university. The El Paso-Ciudad Juárez region remains one of the most dynamic areas along the U.S.-Mexico border that is heavily shaped and enriched by multiple cultures (U.S., Mexico, and indigenous), where residents living on the border are bound by strong family ties and socioeconomic linkages. Mobility among the binational residents through border crossings has led to the creation of binational communities with multiple bridges connecting the two countries and facilitating the residents’ interaction. The border is characterized by rapid population growth compared with the growth of the U.S. population (USMBHC 2010).
El Paso County is predominantly Hispanic, with individuals of Mexican and Mexican American heritage constituting the highest proportion of the county’s population. With a population of over 800,000 people, El Paso County is ranked as one of the most populous and one of the poorest counties in Texas. According to the latest available census data, the county’s estimated median household income of $50,919 is well below the statewide and national median household incomes ($67,321 for Texas and $69,021 for the U.S.). El Paso County also has lower educational attainment, with 79.8% of adults 25 years or older having a high school diploma or higher, compared with 84.8% in Texas and 88.9% in the country (U.S. Census Bureau N.d.). Many residents come from non-English speaking families who are learning English for the first time. The population residing on the U.S.-Mexico border is largely medically underserved. A vast majority of these geographical areas encompass economically marginalized and/or rural neighborhoods. Economic disparities and inequalities are deeply embedded in the rural and semi-rural farming communities located across the county. Access to structured physical activities, nutritious food, preventive health care, and reliable health information is lacking for families and children residing in this region, yet it is imperative for optimal growth in the early childhood developmental life stages (see CDC 2022c, 2022d). Being diagnosed as overweight or obese can impact the quality of life and increase the risk of other chronic diseases (CDC 2022e). Additionally, information highlighting the importance of nutrition and health education needs to be shared broadly with families, so they can develop long-standing healthy eating habits that will be passed down to future generations and spread within the community.
Study Design
The HFHKI began in the Fall of 2021, 18 months following the declaration of COVID-19 pandemic as a global public health emergency by the World Health Organization (WHO N.d.a.). HFHKI was launched with the mission to raise awareness of health risks, promote access to health care, reduce health inequities/disparities, and increase access to information, instructions, communications, and interventions for school-age children, their families, and communities. The initiative has three main goals: to increase access to (1) experiential learning and health education, (2) service delivery, and (3) sustainable systems/linkages of care. With an emphasis placed on cultural and linguistic competence, our initiative, supported by a small working group of UTEP faculty members and students, in partnership with different community partners, was created based on the premise that every community is entitled to good health and no child should be left behind. This initiative is unique in the sense that all activities are “mobile.” That is, services are brought to underserved communities rather than expecting community members to travel to a fixed location. This helps maximize the project impact, build community capacity, and spread awareness.
Owing to a number of issues related to the COVID-19 pandemic that began a year prior and the additional time required to develop fruitful community partnerships, our first year of project implementation encountered a delayed start date, and the implementation period was cut short by seven months. Like many communities throughout the nation, El Paso County experienced different surges of infection and death rates, and multiple waves of rising COVID infections during that time. While the COVID-19 pandemic guidelines had relaxed and less emphasis was placed on home quarantine and social distancing at the time, mask-wearing continued to be encouraged (and sometimes required) to minimize disease transmission in different community locations.
To address health disparities and inequalities, HFHKI integrates seven critical components (e.g., structured physical enrichment activities, a healthy eating curriculum, and preventive health care services) aimed at helping families and children in El Paso County thrive and build a healthy tomorrow, based on the understanding that a child’s health is a shared family and community responsibility. The project aligns with the integrated socio-ecological model (Bronfenbrenner 1986) and acknowledges that a child’s health encompasses their physical, mental, and social well-being, and is not solely based on the absence of disease (Texas Education Agency N.d.; WHO N.d.a.). It also helps raise awareness and empower families with knowledge and skills that can help them become active “health promoters” to create sustainable changes in their communities. This project intervention focuses on four aspects of school-age children’s ecologies: intrapersonal (i.e., holistic child: biological, psycho-emotional, and social processes), interpersonal (e.g., families and schools), communities, and culture, by drawing on available resources, developing capacity, sharing information, and building sustainable community partnerships. Figure 1 shows that children’s health is intimately related to the well-being of their families, schools, and communities and is shaped by the cultural context of their living environment.
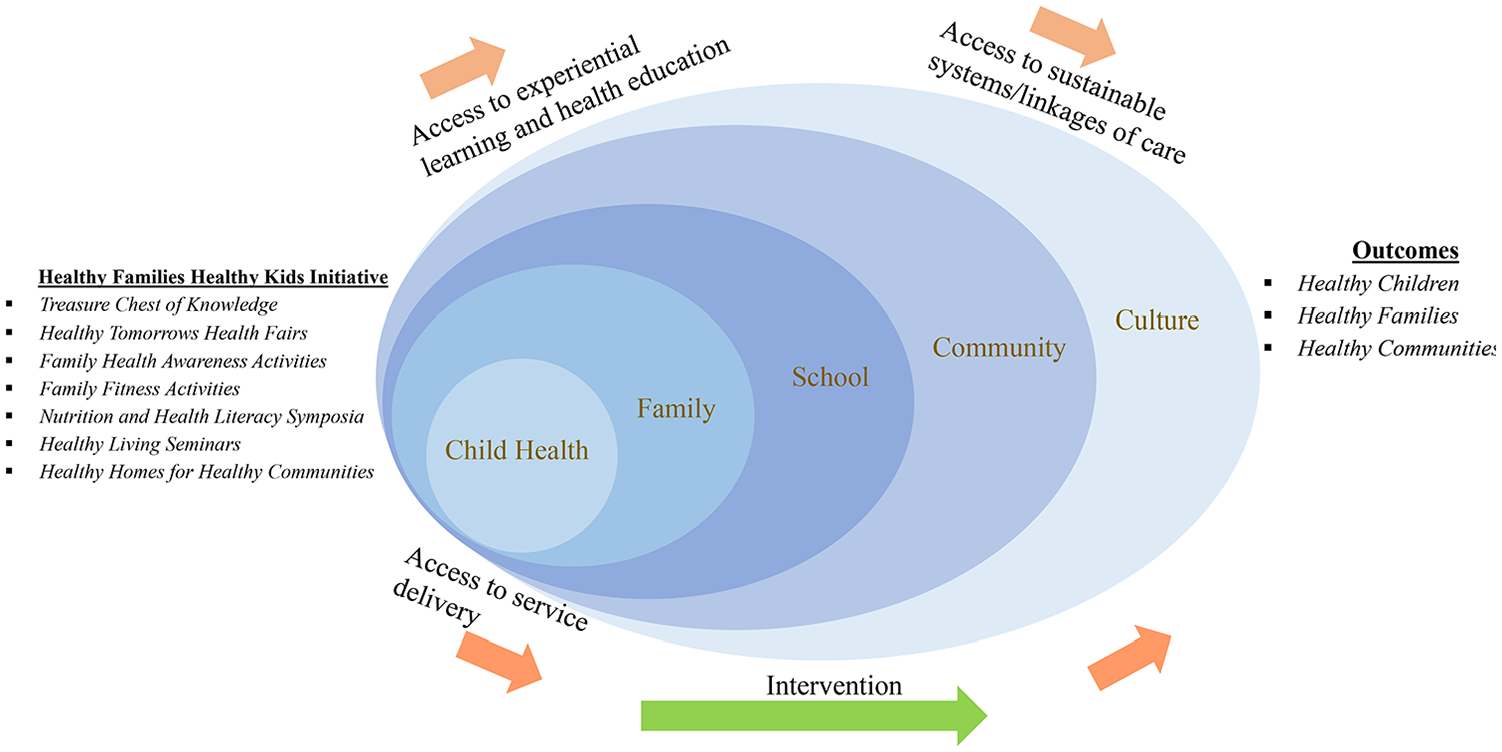
Healthy Families Healthy Kids Initiative (HFHKI)’s model of practice.
To ensure that our project attained the aforementioned goals we set up to accomplish, our project followed the S.M.A.R.T. (Specific, Measurable, Achievable, Relevant, and Time-bound) objectives established for each goal (Health Resource and Service Administration N.d.), which correspond to seven critical activities that we developed to target the needs of families and school-age children, taking into consideration the interrelatedness of their ecologies at varied levels (family, school, community, and culture). Furthermore, for each activity, we developed performance measures and expected outcomes/deliverables (e.g., the number of participants we intended to reach via our outreach and project events/activities, educational materials/products created, and percentage of health literacy gained).
Treasure Chest of Knowledge is designed to increase health literacy and foster a sustainable culture that supports active living and healthy eating and reduces the risks of childhood chronic diseases (e.g., obesity). The project team developed culturally and linguistically competent electronic and hard copy materials about health promotion education (e.g., healthy eating, healthy living, and health literacy) for dissemination. The materials were developed based on the needs of the target population and the characteristics of the communities (e.g., linguistic ability, comprehension level). Examples of published materials consisted of but were not limited to posters, flyers, pamphlets, and infographics.
Healthy Tomorrows Health Fairs aim to raise awareness of chronic illnesses and prevention strategies/services/health care and detect health problems as early as possible to facilitate timely treatment among adults. Preventive health care screenings were offered to check the levels of blood glucose, cholesterol, hematocrit, and hemoglobin A1C. In addition to checking blood pressure, height, weight, body mass index, and blood type, urinalyses were also performed to assess kidney function. The health fairs also aim to bring awareness of existing services and facilitate the development of sustainable community partnerships aimed at decreasing gaps in health disparities and increasing access to care.
Family Health Awareness Activities consist of a series of family-friendly health promotion activities, aimed at promoting families and school-age children’s inclusivity and creativity. Some examples of activities consisted of health promotion contests in the form of coloring, drawing, and poem-writing, and family-friendly activities such as healthy Christmas snacks (Figure 2) and healthy gingerbread house building (Figure 3) to encourage the incorporation of fruits and vegetables in the diet.
Family Fitness Activities provide structured enrichment and physical activities that promote varied ways to reap the benefits of active living (i.e., reduce stress, improve sleep, strengthen the cardiovascular system, and decrease the risk of obesity). Some examples were Zumba and exercise classes.
Nutrition and Health Literacy Symposia assist participants in translating their health literacy into tangible actions to care for their dietary needs and improve health outcomes. The symposia consisted of a series of podium presentations delivered by guest speakers with varied health expertise and credentials (e.g., a licensed counselor, a registered dietitian, and a medical doctor).
Healthy Living Seminars aim at promoting healthy lifestyles using public presentations on varied topics related to healthy and active living, led by health professionals and community members specialized in different health domains (e.g., social work, nutrition, and health) who engaged the audience in meaningful conversations to provide guidance and instructions on how to lead a healthy life. Examples of topics included stress management, diet and nutrition, and weight management.
Healthy Homes for Healthy Communities consist of child development and parenting workshops aimed at bridging health care gaps and increasing access to care using a comprehensive curriculum developed based on a compilation of evidence-based practices in the field, resources from Bright Futures (American Academy of Pediatrics N.d.) and the Rural Community Health Toolkit (RHIhub) (Rural Health Information Hub 2017), as well as health and nutrition curricula from the American Academy of Pediatrics. The culturally and linguistically competent curriculum consisted of modules that focused on holistic health, health literacy, and a parenting guide.

Christmas snacks.

Healthy gingerbread house.
Data Collection and Analyses
Prior to the project implementation, our project protocol was reviewed and approved by the University’s Institutional Review Board (IRBNet ID:1796970). HFHKI activities were held in local schools, shelters, and community venues via collaborations and partnerships with different schools, agencies, and health experts. During its first year of implementation, the project team collected essential project data on all activities that took place and evaluation data on different educational activities (e.g., seminars, workshops, and symposia) to track the successful implementation of all activities. Because our child-focused activities were generally shorter in duration, our data collection focused only on adult participants. Our project serves everyone regardless of their age, sex, gender, race, disability status, and other demographic characteristics. Different methods and measures were used in process and outcome evaluations for continuous improvement of the project, including developing a database to track activities and events that were offered, as well as the number and basic demographic characteristics of participants (when feasible). A mixed-method survey (consisting of four structured quantitative measures and one qualitative measure) was developed to effectively assess changes (from pre-activity to post-activity) in the levels of awareness or knowledge (i.e., health literacy) of voluntary participants taking part in different activities, reached via convenience and purposive sampling, as well as their level of satisfaction with the activities and their likelihood of returning. Finally, periodic project leadership meetings allowed for continued feedback about unexpected issues and/or challenges that surfaced to provide timely solutions, improve service delivery, and document project impact. The project advisory committee, consisting of our community partners and content experts, also assisted in developing strategies for clear communication/information-sharing, service delivery, technical support, and resource management and provided feedback and observations to identify concerns or barriers, resolve challenges, and optimize project outcomes.
Descriptive analyses were performed to tabulate the total number of participants and summarize important characteristics of the participants. In the bilingual (English and Spanish) and voluntary evaluation surveys that generally took the participants less than five minutes to complete, online and in-person participants were asked to indicate their level of satisfaction or dissatisfaction with the activity and their likelihood of returning to the activity again in the future, using a 5-point Likert scale (from 1 “Very Unsatisfied” to 5 “Very Satisfied” and from 1 “Very unlikely” to 5 “Very likely”). For each activity, a mean score was obtained by summing all the scores and dividing them by the number of participants. To measure knowledge gained, participants were asked to rate their knowledge on the topic on a scale of 1 (“low”) to 10 (“high”) for pre-activity and post-activity. Knowledge gained was measured by calculating the value increase from pre-activity to post-activity, dividing it by the value measured at the pre-activity, and converting the decimal number obtained to a percentage. The percentage computed helps gauge the changes in health literacy knowledge. Lastly, the inclusion of an open-ended question allowed the participants to share any suggestions or concerns about the activities they participated in.
Results
Altogether, the project served a total of 2,347 participants during the first year of implementation (September 2021 through February 20221), exceeding the project’s expectations in an abbreviated implementation timeframe. Table 1 shows the tabulation of activities and numbers of participants based on available data.
Tabulation of Activities and Numbers of Participants in Year 1.
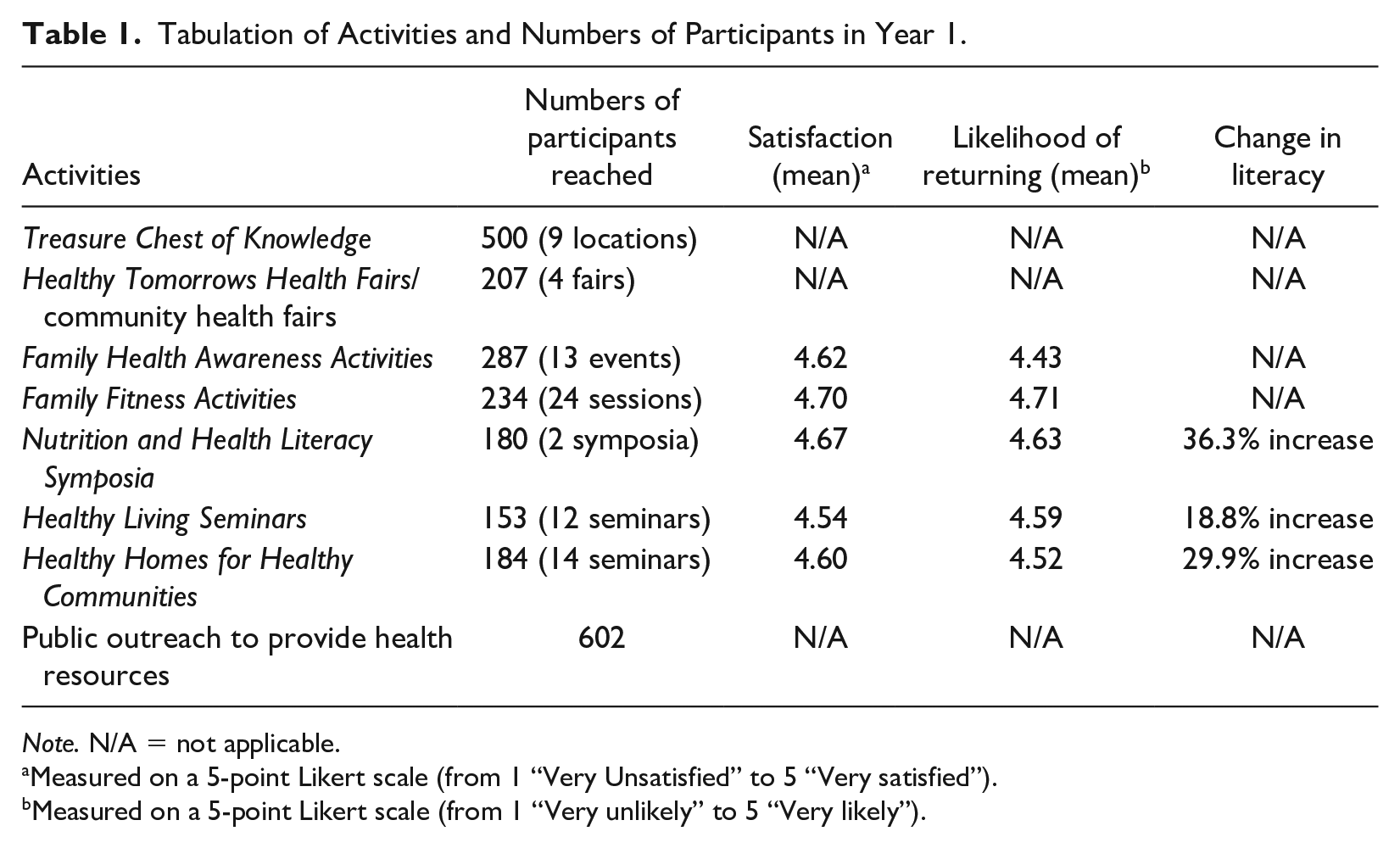
Note. N/A = not applicable.
Measured on a 5-point Likert scale (from 1 “Very Unsatisfied” to 5 “Very satisfied”).
Measured on a 5-point Likert scale (from 1 “Very unlikely” to 5 “Very likely”).
In general, our survey data showed that participants were pleased with the activities offered (average ratings = >4.5 out of 5.0) and expressed the intention to return to the activities (average ratings = >4.4 out of 5.0). We also received many positive verbal and written comments from the participants which expressed appreciation, gratitude, and/or compliments on the activities (e.g., “Very informative presentation, I really learned a lot that I thought I already knew!” and “Very interesting, informative & fun presentation!”)
Discussion
This project can serve as an implementation framework for community-based projects along the U.S.-Mexico border. There are substantial benefits of investing in preventive health care efforts focusing on families and community members on the border, as improving family and community well-being can shape future health trajectories, and the benefits accrued at an early developmental stage have the potential to mitigate health risks/adversities in later life (CDC 2022b). Despite the fact that this project was implemented in El Paso County during spikes in the COVID-19 pandemic, the project model can be replicated in other rural and underserved communities in Texas or throughout the nation, particularly in Southwestern states. Overall, while our first-year health promotion efforts provided many opportunities and rewarding experiences for our local community, implementing health-oriented activities during the COVID-19 pandemic was particularly challenging. Below, we share constructive suggestions, insights, and lessons learned that may be fruitful for other interventions.
Cultural Relevance
Given that the cultural orientation of Hispanic communities emphasizes family-centeredness and multi-family/multigenerational living arrangements, future interventions can focus on nutritional and health knowledge that targets the entire family system. Although our initial design focused primarily on school-age children and their families, it is challenging to target only this subgroup as Hispanic communities are heavily family-oriented and family connections permeate all interactions, not just those with school-age children. We anticipate enriching our curricula with knowledge of pressing health issues relevant to the medically underserved community. In addition to encouraging healthy eating and promoting the use of preventive health care that identifies serious medical problems in advance and reduces medical costs in the long run, our project aims to bridge knowledge gaps in nutrition and health (e.g., encourage healthy eating while maintaining the intake of familiar and culturally appropriate food items), with an emphasis placed on linguistic competence. We recommend the integration of respect for self-determination and person-centricity in curriculum design (Robbins, Mattison, and Dorrance 2018). For instance, while our project encourages the use of different exercise modalities to engage the community (e.g., yoga, mindfulness meditation, martial arts, Zumba, dance, Tai Chi, and other forms of activities/exercises led by experienced/professional instructors), not all modalities are receptive to all subgroups in the Hispanic community. Community members should be encouraged to select the physical activities they are most comfortable with that drive personal empowerment and pique their interests. In our case, Zumba was the favored exercise modality.
Integration of Science, Knowledge, and Hands-On Experience
We recognize the value of hands-on activities in improving functional skills. In our healthy cooking seminars, our project works with a registered dietitian (i.e., Dr. Sarah L. Ruiz, one of the authors in this article) to provide homeless shelter residents with guidelines (e.g., Dietary Guidelines for Americans 2020–2025 [DietaryGuidelines.gov 2020]) and suggestions on how to prepare nutritional meals on an affordable budget. Specifically, residents were taught skills ranging from selecting affordable fruits and vegetables to preparing easy, balanced meals and making healthy choices. Through Healthy Living Seminars, residents were provided community health instructional support by health experts who reinforced critical health principles at home and in the communities (e.g., conflict resolution and mental health literacy). Healthy Homes for Healthy Communities, our parenting workshops, promote the delivery of culturally/linguistically competent health curriculum/lesson plans by building on existing services/resources (i.e., Bright Futures and Rural Community Health Toolkit) and integrating interdisciplinary evidence-based models of care to promote effective child development and parental care (e.g., coping with parenting stress, mindful communication, and child safety). These educational workshops also focused on holistic health enrichment instructions for parents/caregivers with school-age children of three different developmental phases (early childhood, middle childhood, and adolescence).
Incentives to Boost Attendance and Encourage Active Participation
Bradley et al. (2018) postulated that carefully selected incentives can lead to behavioral change and the selection of healthier lifestyles, including the domains of fitness, nutrition, and preventive lifestyle. We learned that selecting meaningful incentives to encourage community attendance and active participation helps strengthen the goals of our project. Some suggestions include a giveaway or raffle of selected items (e.g., nutritional food, nutritional guide, healthy cookbooks, insulated lunch boxes, classic measuring cups for healthy cooking, family board games, children’s story books, basketballs, jump ropes, hula hoops, and stress balls) to promote the continuation of healthy living. Incentives may also be provided to encourage active living and promote the development of a healthy hobby.
Flexibility and Adaptation
Our attempts to reach the targeted number of participants and secure engagement from the community partners in our health promotion efforts during the pandemic were challenged by the need to adhere to COVID-19 guidelines (e.g., social distancing and mask-wearing) in the local context, especially since fighting COVID-19 transmission was the top priority to ensure community safety. Given the unpredictability of COVID-19 waves, we learned to adapt to event cancelations and postponements. We found residents in El Paso County were generally open to participating in fun and engaging activities, particularly as families had grown tired and weary of staying at home in isolation to avoid contagion. Fortunately, our project was able to meet the project objectives and exceeded expectations by increasing the frequency of our events/activities once the local guidelines on COVID-19 permitted.
Limitations
Although we encountered many challenges throughout the first year of our project implementation, we also experienced many successes and accumulated many valuable lessons. Several limitations are worth mentioning. Given that most of our events are one-time events and the transient nature of some of the economically disadvantaged populations our project serves (e.g., residents in homeless shelters), we were not able to keep track of the participants’ progress over time. Therefore, the number of our participants only reflects the total count of all participants who had attended our events, not accounting for the returning status of the participants. Just like any other surveys, our data were subjected to self-selection factors (e.g., participants who were pleased with the activities might be more likely to complete the survey) and social desirability bias (e.g., participants might select certain responses on the survey to present a pleasant front). We also had challenges collecting data from our online events and large events where participants tended to come and go in an unstructured, at-will manner. Additionally, our evaluation surveys were not linked to participants’ demographic information to safeguard our participants’ privacy, and this limited the type of data analyses our project was able to conduct. Nevertheless, the purpose of this article is not to report on an intensive, research-driven project. Rather, the purpose is to present a translational framework for learning and practical insights that may serve as a set of suggestions, guidelines, and input for other applied social scientists and health practitioners who encounter roadblocks in their community-engaged health promotion implementation, just as we did.
Conclusion
In sum, our project (n = 2,347) has provided some insights for considerations for current and future applied social scientists. We recommend the use of the socio-ecological model in designing, implementing, and improving health interventions aimed at enhancing family and community health, with each intervention tailored to the needs of different segments of the community. This may involve the use of a culturally and linguistically multidisciplinary approach to encompass a multitude of health expertise. During the first-year implementation of the HFHKI, we witnessed the importance of education and prevention in promoting community health. We anticipate that our project will continue to evolve to adapt to the “new normal” throughout the different stages of the COVID-19 pandemic. For instance, at the time of this writing, a new variant has emerged, EG-5, which scientists believe is more transmissible and severe than previous Omicron subvariants (Katella 2023). Because families residing in predominantly rural communities do not have access to many healthy activities, health promotion interventions can engage families in structured enrichment and physical activities to encourage varied ways to diversify active living, where families can receive instructions on enrichment activities to promote physical health. The CDC recommends the use of a “Whole Community” approach in working on community-based COVID-19 prevention and response efforts, where all parties (including individuals, families, organizations, schools, and governments) regard preparedness as a shared responsibility (CDC 2023). As echoed by Bradley et al. (2018), The changes required to create a healthier America and affect costs associated with lifestyle-related diseases need to happen on a personal level, coupled with a supportive infrastructure and public policies to promote and sustain them. This shift is critical to our transition from health care to a healthier way of living and of controlling avoidable costs (P. 198).
While the need to contain the COVID-19 virus amid the pandemic has created challenges in health promotion efforts, the need to help affected communities regain control of their health cannot be stressed enough (Van den Broucke 2020).
Footnotes
Authors’ Note
This manuscript has not been published elsewhere and it has not been submitted simultaneously for publication elsewhere. Paat is the first and senior author of this paper. The second and third authors contributed equally to this manuscript. Their names are arranged alphabetically based on last names. The project team thanks HRSA and all their community partners for their assistance/support in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for research, authorship, and/or publication of this article: The Healthy Families Healthy Kids Initiative is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $250,000. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.