
Abstract
Communication during patient transitions is difficult in a fragmented health care system. eHealth technologies are often seen as a panacea, but a large proportion of eHealth projects fail, primarily because of human, not technological, elements. To combat this tendency, concepts derived from institutional ethnography were applied to create an electronic communications solution, which enabled careful mapping of communications gaps; their consequences; and the diverse needs of multiple health care providers. Institutional ethnography allowed researchers to trace social relations across locations in the health system and determine how action could be coordinated to ensure that family physicians were informed of patients’ acute care encounters, while simultaneously strengthening relations between clinicians and information technology workers. As a result, an automated electronic notification system was piloted, evaluated, and spread to more than 92 percent of community physicians in one region of British Columbia, Canada, improving communication between providers and enhancing patient care.
Introduction
Health care delivery depends on the flow of information between many providers and sites. Without this, care provision is uncoordinated and patient safety is at risk. However, in the Canadian health system, different aspects of care delivery are regulated by different jurisdictions, and policy differences can make information transfer between them difficult. To address deficiencies that contribute to patient risk, the uniquely Canadian health care environment can benefit from a Canadian-made method of tracing social relations. Here, principles derived from institutional ethnography (IE), developed by Canadian sociologist Dr. Dorothy Smith, are applied to health care delivery in British Columbia (BC) to identify improvements to continuity between primary and acute care.
IE begins by taking a standpoint: imagine that you are a family physician (FP) whose practice includes an elderly patient whom you have treated for most of your career. You know your patient well; you’ve met her family and know her goals for the remainder of her life. Then, one day, her adult child books an urgent appointment and demands to know “what happened to mom.” You discover that this person for whose care you have been responsible for decades has experienced a sudden illness, been hospitalized, and died. How could you not know she was sick? Why didn’t you tell us what was going on? These are things the family wants to know. But you can’t answer them—no one in the hospital informed you your patient was there. The funeral home found out before you did.
This was the problem in an urban community in BC where I was hired as a nonclinical project manager to support FPs seeking improvements to the quality of patient transitions through a local nonprofit. My initial consultation with the FPs who had secured project funding revealed there was no process or policy that required the health authority responsible for hospital care to notify FPs of admissions or deaths; and no impetus to ensure that discharge notifications—while mandated by policy—were timely. This created gaps in care when patients transitioned. Investigations into the problem quickly revealed that a change in policy would not be sufficient because even if there was a mandate to notify FPs, there was no process to do so. It was clear that a new system-level solution was needed—including policies, but also technologies and individual work habits across numerous sites governed by different rules.
Crucial to this solution was an investigative strategy that could articulate the complexities of the system while remaining grounded in the practical need to solve a problem experienced by individual clinicians—an applied approach that could enable decision-makers “to see relatively autonomous human experiences. . . as social” and coordinated, or capable of coordinating (Deener 2018:296). As an applied sociologist, I knew that one promising approach was IE. This is an account of how using an applied IE approach can improve the success of what are traditionally understood to be technology projects, such as developing systems of notification.
After reviewing the relevant literature, I provide a description of methods. Findings related to articulating the root cause of the problem; its consequences; and the results of process and social mapping are presented, along with a description of the automated electronic notification system (eNotification) that was developed. Evaluation results from a pilot study are provided. The article concludes by defining the value of IE principles for health systems and technology research.
Literature Review
Communication During Transitions in Care
Transitions in care occur when a patient moves from one health setting to another, such as an admission to hospital from the community or discharge after an inpatient stay. Transitions create risks of harm to patients due to the fact that new practitioners, working under different governance structures with different protocols and procedures, and often steeped in a different work culture, are taking over care (Lee 2008; Solet et al. 2005). Provider workloads and scheduling make “warm” hand-offs—where providers speak in-person about a patient’s needs—difficult, if not impossible; transitions rely on the transfer of information to stand in for these conversations (Barr et al. 2017; Solet et al. 2005). As care between systems has fragmented, communication between providers has become increasingly complex (Coleman 2003; Jeffs et al. 2013). Individual practitioners must also account for institutional requirements, oriented to legal liability and regulatory accountability, exacerbating the logistical issues and time constraints that already threaten to break down communication (Dalmer 2018; Dixon-Woods et al. 2014).
This breakdown is not insignificant; communication errors are often implicated in adverse events during patient transitions (Patel and Landrigan 2019). For example, a cohort study of 400 transitioning patients discharged from a tertiary Canadian hospital found that two-thirds of adverse postdischarge events could have been mitigated and that systemic issues, particularly lack of communications systems, were implicated in 60 percent of harms (Forster et al. 2003). In the absence of formalized processes, communication is variable and unreliable (Solet et al. 2005). Since it affects the quality of care transitions and poor transitions are linked to worsened patient outcomes (van Walraven et al. 2008), researchers have for decades been calling for systematic improvements to address barriers to the flow of information across health care settings in Canada as in elsewhere in the world (Hampson, Roberts, and Morgan 1996; Jeffs et al. 2013).
eHealth Implementation
Communication technologies are often proposed to solve poor patient transitions (Graetz et al. 2014). These are part of a suite of digital health technologies referred to as eHealth (Boogerd et al. 2015). eHealth is not simply an electronic way of doing things that were once done with paper. It fundamentally changes the way in which tasks are carried out (Green, Harvey, and Knox 2005). Zamora et al.’s (2012) extended example of prescription orders illustrates this very well. On paper, a physician may identify medication doses in the measurements they prefer. An order may be combined with a note about allergies on the same piece of paper. A nurse who receives the order may add their own instructions to the pharmacist, to assist with interpretation. Paper allows information to be clustered together; recognizes the contributions of multiple clinicians who can be separated through different handwriting; and allows for individual quirks.
Electronic prescribing, on the contrary, is not just a typed medication order. It is an interface that is connected to a prescription database, which can transmit directly to the pharmacy. The physician must choose the medication from a list, along with predetermined dosages. Allergies are entered elsewhere, requiring physicians to navigate away from the prescription order screen. If nurses review prescriptions, they may not be able to add interpretive notes. The physician’s method of giving an order, the nurse’s contribution, and the pharmacist’s response are changed (Zamora et al. 2012).
Staff must learn new ways of interacting with health information and with each other (Zamora et al. 2012). They must orient to eHealth interfaces that did not previously exist, which diverts their time and attention, interrupting their workflow (Ash and Bates 2005; T. F. Bishop et al. 2013). Providers often struggle to learn not only what information to enter where but also how to include eHealth in their practice of medicine (T. F. Bishop et al. 2013). Furthermore, they must take on these new tasks in a context where they are typically already over-burdened with work (Aveling, Parker, and Dixon-Woods 2016).
The reality is that most eHealth projects ultimately fail (Adler-Milstein, Bates, and Jha 2013; Leviss and Charney 2013). Poor design, disorganized implementation, and inadequate attention to training and change management can cause quality improvement (QI) projects such as eHealth to make health care delivery more difficult instead of less (Dixon-Woods et al. 2014). As Grenier and Bigdoli (2015) discovered in their evaluation of health reform in Quebec, users will resist if the learning curve is too steep, eHealth creates too much work burden, or there are setbacks in implementation (see also Barr et al. 2017; T. F. Bishop et al. 2013). This is especially true when front-line workers feel they have little input into system design (S. Bishop and Waring 2016; Grenier and Bidgoli 2015).
The result is poor uptake and information that may be partial or of poor quality (Adler-Milstein et al. 2013). Such information is less reliable for other users, who will in turn resist because they worry about increased risk to patients (Ash and Bates 2005). When eHealth does proceed, implementation is often uneven, fracturing along lines of health access inequity, such as between government and nongovernment sites or between urban and rural settings (DesRoches et al. 2013).
How, then, does an eHealth project avoid failure? Factors that contribute to the success of projects include that they engage multidisciplinary users; consider both intended outcomes and the workflows that achieve those outcomes; identify how changes will affect nontechnological aspects of work; provide incentives for use; and are supported by training (Graetz et al. 2014; Zamora et al. 2012). A key commonality is that these factors attend to human, not just technological elements (Tummons et al. 2018).
However, there is little concrete information about how to ensure these elements are incorporated. Indeed, as Quinlan (2009:626) points out, the way in which “knowledge processes are conceptualized as technical, cognitive processes” without regard to social components is a deficit of much of the literature on health systems change. Aveling et al. (2016) add that broad institutional and workplace cultural contexts are often absent in the analyses of eHealth projects, even though they significantly affect the work processes of practitioners (Barr et al. 2017).
IE
To address these deficits, IE offers a useful approach. IE was developed by Canadian sociologist Dorothy Smith, who argued that the coordination of people creates the social relations that comprise institutions (D. Smith 1999). These social relations are beyond our immediate reckoning; IE provides ways of explicating the processes that coordinate individual activities to produce similar practices across settings (McCoy 2008). A key area of focus in IE is the use of tools that enable information to move from site to site, referred to as texts (Deveau 2009). The points at which texts are taken up from one local setting to be acted upon in another can be understood as processing interchanges (Pence 2001). Texts as used in IE include print documents but also technologies that sort, store, and retrieve information, such as electronic health records (EHRs). Such technologies act as both archives of information and processes for transmitting that information (Akemu and Abdelnour 2020). They mediate existing or potential social relations, and it is through the interaction of people with technologies that work is accomplished (Tummons et al. 2018).
IE is well suited to identifying gaps in the way in which individuals across settings “link up” (Pence 2001). Deveau (2009:3) refers to the resulting analysis as “social cartography” that renders visible connections that enable work processes, or lack thereof. This is particularly useful for health research, where patients (and their information) move frequently. For example, Waters and Rankin (2019) used IE to understand how scientific evidence was embedded into policies governing the practices of Canadian registered nurses undertaking wound care; while Kearney et al. (2018) employed it to examine the use of the Objective Structured Clinical Examination (OSCE) in determining clinical competence. Numerous other examples can be cited (e.g. Dalmer 2018; Grenier and Bidgoli 2015; Mykhalovskiy and McCoy 2002; Quinlan 2009).
Tracing social processes is especially important in the Canadian health care system where legislation, regulation, and service provision is undertaken at multiple levels (federal, provincial, and regional) and where there are numerous organizations and individuals with different accountabilities who need to manage patients (Vedel et al. 2011). When there is a lack of information, there may be an important role for new “texts” play. However, IE emphasizes the fact that texts stand in for social relations; they do not stand on their own. To build solutions that can coordinate action across jurisdictions, work must begin with the social, not technical, which is what this project aimed to do.
Methods
The project was conducted through a Division of Family Practice (DFP). DFPs are nonprofit organizations funded through the BC Ministry of Health and Doctors of BC (the BC Medical Association) to provide FPs with a venue through which they can participate in health systems change. From most stakeholders’ perspectives, it was a QI project. 1 QI is a form of rapid testing intended to leverage small-scale innovations at the front line of service delivery, using ongoing monitoring to make incremental changes (Dixon-Woods et al. 2014). QI is the method endorsed by DFP and by the funder, the Shared Care Committee, a provincial organization funded through the same Master Agreement as are DFPs. The general precepts of QI, such as starting small and testing changes iteratively, are familiar to many who work in information management and information technology (IMIT), 2 where responsibility for most eHealth projects typically lies. As such, the regional health authority with whom the DFP partnered had institutional mechanisms for managing such work; the authority does not require ethics reviews for QI work, and there was no formal Research Ethics Board approval. For survey data, an informed consent statement was placed in the introduction, informing participants that they were consenting by completing the survey. Consent for interviews was collected verbally prior to the interviews commencing.
The alignment between QI and IE is not straightforward; the former tends to focus narrowly on concrete changes without attending to power or to the way in which specific processes do not “exist” on their own, but are accomplished through the linking up of individual actors. For this reason, I believe IE was an invaluable addition to the project’s methods, and one which ultimately made it more successful. However, it is important to recognize that, starting as it did from a QI lens, the project carried out was not IE in its pure form, and many aspects of IE were not fully addressed through the work. The methods described in this section should therefore be understood as drawing on concepts from IE in a fashion similar to previous work (e.g. see Webster et al. 2015), rather than being read as a claim that this study “was” IE in its most comprehensive form.
Problematic, Standpoint, and Multisite Engagement with Participants
IE begins with a point of inquiry called a problematic that arises from a specific group’s standpoint (D. Smith 1999). From this, researchers branch out to explore the way in which individuals are connected. The problematic identified by the FPs who initiated the project was that FPs did not know about their patients’ interactions with acute care, which they knew represented a risk to their patients’ health. The work originated in their standpoint. Their concerns stemmed from their everyday experience of trying to provide care in a system where the complexity of health needs is increasing and the population is aging, two features of the Canadian context that lead to an increasing number of patient transitions between settings (British Columbia Ministry of Health 2015; Vedel et al. 2011).
Communicating the FP standpoint was done through patient scenarios that detailed typical acute care transitions (see Supplemental Materials). The fictional patients had names and backgrounds, and the scenarios described the consequences of communications gaps for both the patient’s and the FP’s experience. Scenarios were shared with the committee that oversaw the project, which included representation from both the health authority and the community. Health authority administrators were not used to thinking about the end-point of a patient’s transition; their orientation was toward how care was accomplished within the boundaries of the authority’s jurisdiction—including both those of physical space and of legal liability. The scenarios were necessary to help administrators understand FPs’ standpoint, which was grounded in personal relationships with patients as opposed to the need to attend to policy or procedure.
The project also needed to engage with the IMIT Department. Personnel who would build the solution were more amenable to the FP standpoint because they understood the concept of designing for “end-users” and could extend that frame to FPs in the context of hospital transitions. IMIT partners also brought their own perspective, which emphasized technological enablers and limitations; requirements for standardizing and automating processes; and scalability. Moving out from the initial standpoint thus identified new elements that became important components of the project work.
A typical strategy in IE is to follow a document as it moves across locations to determine other standpoints to examine, but I did not have a document to follow. My strategy was instead to follow a chain of potential responsibility, in line with methods employed in past ethnographic research on health work practices (e.g. see S. Bishop and Waring 2016). For instance, identifying the need for an electronic solution necessitated engaging the Privacy Office, because a Privacy Impact Assessment is a procedural step in IMIT projects. This in turn led to Medical Affairs since part of their role in credentialing physicians is assigning role-based access to patient information.
Continuing to follow IE procedures wherein access to participants is negotiated outward from the original standpoint (G. Smith 1990), the committee engaged with hospitalists, 3 which led to a reconceptualization to include processing interchanges within the hospital. An interdisciplinary meeting resulted that included registration clerks; unit clerks; ward managers; liaison nurses; emergency (ED) nurses; ED physicians; hospitalists; FPs; and administrators in Seniors Care and Patient Access and Transitions. 4
Finally, the committee engaged with vendors who provide infrastructure to health care information systems. These included the vendor that provided the health authority’s EHR; a company contracted to provide reports distribution services; and multiple different electronic medical record (EMR) vendors who supplied FPs. Consultations occurred informally through meetings and email; consistent with what other applied IE researchers have done (e.g. see Pence 2001; G. Smith 1990).
D. Smith (1999) has described using interviews with concrete questions that elicit clear descriptions of the steps each person takes to move a process to the next location. The activities described above were structured similarly in that patient scenarios and follow-up questions stayed grounded in the everyday. However, these engagements were not conducted as formal interviews. Rather, they took place as part of committee meetings; at events where participants from many different health care locations were invited to review issues together; and informally through one-on-one discussions and emails. In fact, many of the insights that led us to engage with a new group or add questions to our investigation came from these “grassroots” conversations.
Mapping Procedures
The consultations described above solicited information about constraints to and enablers of individual action; from whom or where they received the information; how they used it; and to whom or where they in turn shared it. This information was mapped by documenting local accounts; identifying coordination points to other accounts through common texts (policies, alerts, etc.) or processes (e.g. medical rounds, patient hand-offs); and noting gaps where locally produced patient information did not travel. From this, I produced an ethnographic account of the information system, including points of fragmentation. It contained the origin, course, and consequences of the problem and delineated social relations by documenting who was affected and how. Similar processes were employed to articulate how an eHealth solution could potentially affect information transfer across sites, as well as how it would affect individuals.
In determining who would be affected, I followed an auditing process recommended by Pence (2001), wherein individuals who would be located at a potential processing interchange had an opportunity to suggest how their piece of the process could be improved. Information accumulated through mapping was continually returned to the oversight committee to discuss findings to date, which helped solidify decisions about which interchanges were the most important to attend to and which should be considered “out of scope,” similar to how ethnographers move back and forth between field study and institutional engagement (Deener 2018). In the Findings section, results of the mapping are discussed along with how they were mobilized to produce improvements.
Pilot Participants and Evaluation Procedures
While the focus of this manuscript is on assessing the utility of apply IE concepts to eHealth projects, the solution developed during the pilot was itself the subject of evaluation. A total of 50 FPs enrolled in a pilot study and received eNotifications for every patient admitted to acute care in one geographical region over a 4-month period. Postpilot, participants received an online survey asking them to rate their satisfaction with the system and its value to clinical practice; with a response rate of 46 percent. Physicians were then invited to participate in interviews to gather narrative data that illustrated changes to patient care. A private evaluation company was contracted to collect survey and interview data, which were provided in summary form so participants could not be identified. No individual patient information was collected, but aggregate data on the volume of notifications were provided by the health authority.
Evaluation results are provided in the Findings section with the caveat that it was not designed as a “mixed-methods” study. The intention is not to have quantitative data make a “cameo appearance” to add validity to ethnographic findings (Hancock, Sykes, and Verma 2018:314), but to demonstrate that the project evaluated whether the solution arrived at through the use of IE concepts addressed the problem originally identified.
Findings
Mapping resulted in a rich description of the problem and its consequences, akin to in-depth field notes. Through ongoing dialogue about findings “in the field” at the oversight committee, chronological and jurisdictional boundaries around what was “relevant” were developed (Deener 2018). The resulting account informed the creation of the eHealth solution. In this section, the results of mapping are presented followed by a description of the eHealth solution and findings from the QI evaluation.
Results from Mapping: Explaining the Problem
Historical preconditions
A first step was to articulate the historical preconditions of the problem to understand why it existed and persisted. While most administrators involved had been in their positions for a decade or less, several FPs had been in practice for 20 or 30 years, and their longevity helped situate the issue. Historically, they explained, there had been no need for notification because as with most Canadian cities, FPs in this area were most responsible for patients’ admissions and care in hospital (Lee 2008). They did bedside visits, reviewed charts, spoke with specialists and nurses, and made treatment decisions. Most, if not all, had ordering privileges and could control the trajectory of patients’ care, including deciding when to discharge them. As they were present for day-to-day care, they were aware when patients died in hospital. However, over the last two decades, there has been an exodus of FPs from many urban hospitals in Canada, concurrent with the rise of hospitalists (Lee 2008; Neimanis et al. 2017). As a result, FPs have become removed from the everyday work of hospital care, and the community/acute divide has become one not just of location, but of medico-legal jurisdiction (Lee 2008).
What occurred must be distinguished from a formal change or a response to a sudden shock—new legislation or a catastrophic event such as the destruction of a hospital in an earthquake, for example—which likely would have been addressed using an explicit change management plan. The movement of FPs out of the hospital was gradual (in fact, the process is still ongoing; a small number of urban FPs hold on to their privileges, and FPs are still ubiquitous in smaller community hospitals). No solution for notification followed FPs as they left because there was no formal leaving.
The current state
Understanding historical preconditions helped contextualize the current state. Additional to the absence of a formal change management plan was the absence of any specific policy or protocol requiring admission notification to FPs. No documentation could be located wherein notifying FPs of admissions was specified in any position’s job description. If notification happened, it was because the ward-specific practice was to notify. Even then, notifications were not universal, but made only in cases where someone determined a special need for the FP’s involvement. There were similar disparities in death notification. For FPs, this was an experience of inconsistency and uncertainty: they did not know what information to expect and could not detect any pattern.
Discharge notification was different because there was a legal mandate for discharge summaries to be sent to FPs. This work was done by a centralized unit called Health Records. There is no legal mandate for immediate discharge notification, and there are many steps that introduce potential delays in the transmission of discharge summaries. First, the discharging physician often dictated the summary as or just after the patient was physically leaving the hospital; that is, the work did not commence until the patient was already transitioning. Second, the dictation went into a queue until a staff member became available to transcribe it. Third, the transcribed summary was sent in another queue to Health Records to be distributed, and fourth, staff at Health Records had to physically place the summary into an envelope with the FP’s office address on it. Finally, a courier had to pick the envelope up and deliver it to the FP. 5
Varying volume of patients entering and leaving the hospital at any time—along with staffing fluctuations—holidays, sick leave, and so on—combined to exacerbate these delays, such that when the project was initiated, FPs reported it could take anywhere from 72 hours to 3 weeks for a summary to arrive. In many cases, FPs reported that the patient presented for follow-up care prior to the FP receiving a discharge summary. Since admission notifications were rare, this meant that patients were seeking care from an FP who did not know they had been hospitalized in the first place.
Consequences of the absence of a coordinating text
The absence of a coordinating text—a notification—was not benign. Mapping revealed that there were both system inefficiencies and risks to patient safety. System inefficiencies arose at all points in the transition process. FPs who were unaware that their patients had been hospitalized could not know that those patients’ scheduled appointments would not be kept. Had they known, the appointments could have been canceled and other patients seen. Similarly, when FPs did not know their patients had been admitted, they could not send in recent laboratory results or information such as cognitive baselines for dementia patients. This resulted in duplication of testing because hospital providers did not know what had already been done. A lack of notification for deaths in hospital sometimes created duplicate work in completing death certificates as hospital providers undertook this work without informing Coroner’s offices, which then contacted the FP on record for the same paperwork. Patients were not always able to provide accurate accounts of the acute care they had received, so FPs would set up treatment plans and then receive the discharge information and realize that something different was required. This necessitated a return visit, affecting both doctor and patient.
A more significant consequence had to do with risks to patient health. One FP recounted a story of a patient with dementia who had been hospitalized without the FP’s knowledge. The patient developed a urinary tract infection which affected her cognition. Unaware of the hospitalization, the FP had no opportunity to send in the patient’s cognitive baseline data. Hospital providers assumed the patient’s cognitive deficits were part of the underlying dementia, when in fact they were symptoms of a developing acute condition. This delayed the diagnosis and treatment of the infection.
Another risk had to do with patients being discharged without the supports that FPs would have known they needed. FPs reported that some patients overestimate their ability to self-manage and hospital clinicians have insufficient knowledge about the patient to counteract these assumptions. Finally, there was a serious risk of medication errors. FPs who were unaware of a hospitalization did not know that medication reconciliation was needed. When patients presented to their FPs before discharge summaries arrived, they often did so without a list of current medications, making it even more difficult to determine the best course of action.
Results from Mapping: Explaining Social Relations
Explicating a “phantom chain of communication.”
To document the social relations that would be required to create processing interchanges where none yet existed, I mapped a “phantom chain of communication,” gathering information from people in different locations that were lacking information just as a traditional IE project would follow an existing text from hand to hand.
I assumed that individuals at each “link” were acting intentionally. For example, when asking registration clerks how they confirmed the patient’s FP during admission, I assumed there were important reasons for not doing so—such as the need for expediency to trigger the process of locating a bed for the patient—and inquired about these reasons. This enabled the project to systematically identify not only the technological but also the social and workflow barriers to the processes required.
The oversight committee treated each stop along the way as equally important, from the clerks to the Chief Medical Information Officer who was overseeing a multiyear project to redesign the IMIT infrastructure for the entire health authority. The chain was considered “complete” once the committee had identified all the potential actors who would be affected by the creation of a new notification system, and the mapping data were used a reference to ensure that the design of that system had no unintended consequences for any processing interchange along the way.
Designing eNotification
The work of mapping led to a deceptively simple set of requirements: notifications had to be straightforward and quick to comprehend; be interoperable with many EMRs to reach as many FPs as possible; be sustainable; and could not increase anyone’s workload once it was built since, as with most Canadian hospitals, the hospitals in this community routinely operate over-capacity (e.g. see Crawley 2020; Olsen 2017). IMIT created an automated electronic notification of hospital admissions, deaths in hospital, and discharges from acute care facilities to any FP in the province.
The admission notification is triggered when the registration clerk completes an admission record for a patient. The system does not require the clerk to alter their work tasks but is automatically engaged when the admission submission is received by the EHR. The form auto-populates fields from the EHR including patient identifiers; date of admission; facility identifiers; and the name of the most responsible provider (MRP) at admission (often, an ED physician). Discharge notifications work in a similar fashion but are triggered by the submission of the discharge form (deaths are considered a form of discharge in the EHR).
The notification is sent electronically to FPs’ EMRs. How it arrives depends on the technological capabilities of individual FPs’ offices. Some EMRs can receive the information into their software and display it as an alert, so that it becomes one listing in a series visible on the computer screen when the FP logs in. For FPs whose EMRs do not have this capacity, the third-party vendor contracted by the health authority to transmit the data has a Web-based repository where notifications are stored as messages that can be downloaded once an FP has signed on with a user name and password.
Results of the Pilot Evaluation
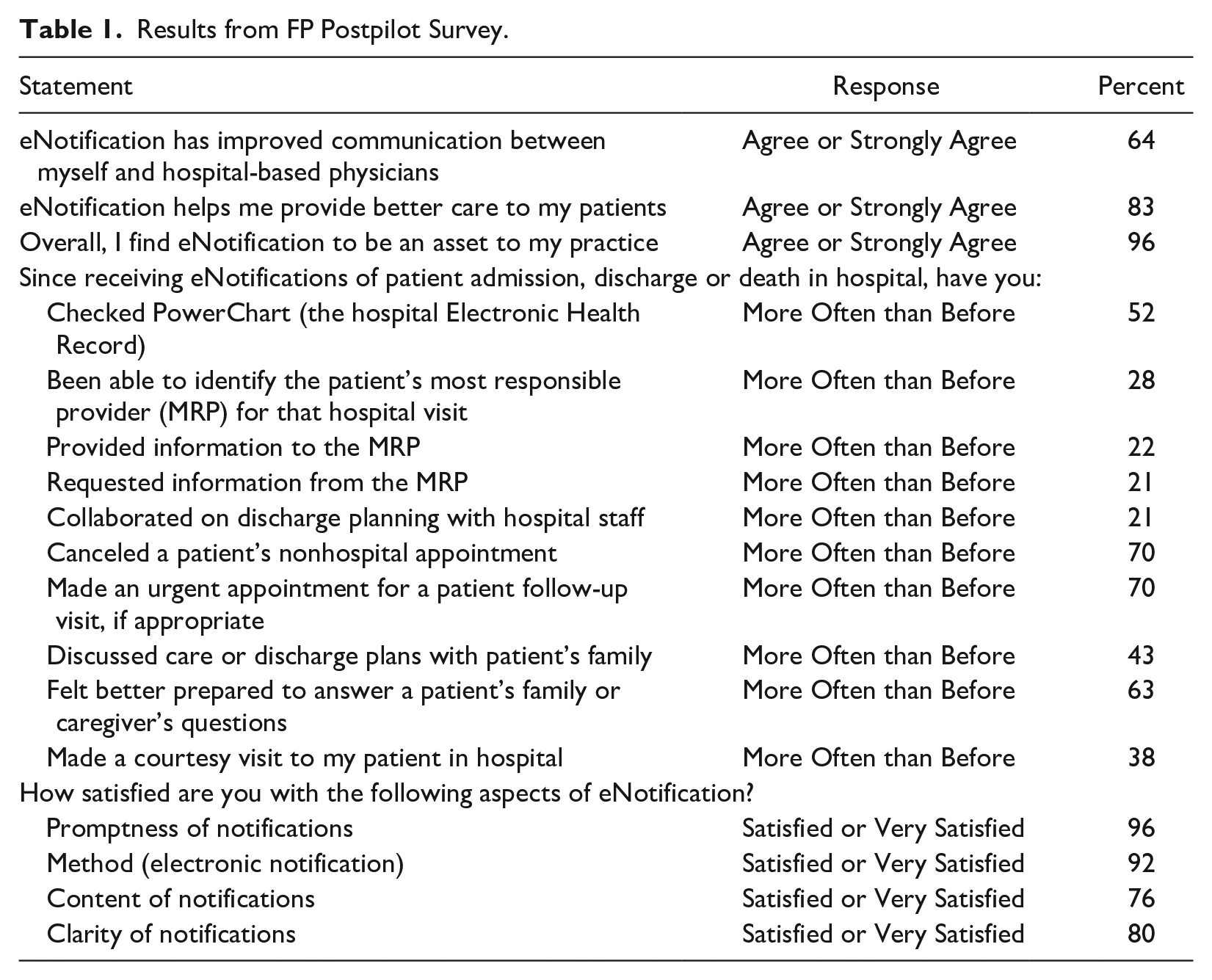
Pilot testing included technical testing to ensure the messages were delivered correctly and on time, and “real-world” testing of admissions, deaths, and discharges during the study period. A total of 943 notifications were sent during the 4 months. At the end of the pilot, FPs rated the value of the system: 96 percent agreed/strongly agreed that eNotification was an asset to their practice; 72 percent reported they scheduled or canceled an appointment as a result of the notification; 68 percent found that they were better prepared to discuss a patient’s care with them or their families; and 83 percent thought that the notification enabled them to provide better care. Complete results are presented in Table 1.
Results from FP Postpilot Survey.
Qualitative information collected through interviews emphasized the way in which the service enabled FPs to provide better patient care: It allowed me to touch base with the family of a pediatric patient. They were anxious to have more information and I was able to support the family because I could follow up on what was happening at the hospital. It was very timely, as I was then able to speak to my patient’s nurse case manager. She immediately phoned the family to make sure that my very frail elderly patient had enough home supports in place upon discharge.
Having timely notifications also improved FPs’ relationships with their patients: [It] allows me to have a better follow up appointment. . . it looks really bad when they show up at the office and you don’t know what happened. Patients know we might not be involved in hospital care, but they feel more comfortable when we know where they are. It helps build the relationship.
FPs also articulated unexpected benefits. For instance, the oversight committee was concerned that in smaller communities where patients are still admitted by their FPs, the notifications would be redundant. That turned out to not always be the case: [It] lets me know if any of my patients have been admitted to our local hospital under specialist only care. I do have hospital privileges but. . . I’m not psychic.
Physicians noted that the notification made them “feel more connected to the patient’s care” and “like part of the team.” One physician commented that “now. . . when families phone, I know what is going on.”
They also reported leveraging the notifications to make other tasks easier: There is now a clear dated medical record of admitting and discharge dates. This is very useful for Disability forms.
Benefits to the project team and to sustainability
Previously, fragmentation in the health care system had prevented differently located clinicians from learning from each other or from understanding why a potential solution that seemed straightforward from one standpoint was unworkable from another. Mapping not only articulated the problem through a variety of lenses (legal, technical, clinical, and administrative), but also engaged individuals in solutions-development in a way that transcended traditional siloes. For instance, IMIT workers valued the opportunity to hear how their “back-end” work would enable better patient care, while clinicians gained an appreciation of the technical complexities of health in the digital age. Thus, mapping had the secondary benefit of strengthening relationships between groups within the health authority, such as clinicians and IMIT personnel, and also between groups in different care settings. In a debriefing session with the oversight committee, one member explained, “having the initial meetings was so important. It really opened up a lot of information we hadn’t considered before.”
Mapping helped identify obstacles to implementation that could have caused the project to stagnate or fail. For instance, recognizing competing priorities within the health authority, which was in the midst of a large digital health transformation, enabled the committee to position the project as a successful eHealth implementation that was part of the overall transformation, not separate from the larger goal. Being able to take the standpoint of health authority leaders allowed the team to build a better case for the solution, which contributed to it becoming a part of the information management system. As Dixon-Woods and Martin (2016) point out, many QI efforts are abandoned after the pilot stage, whereas eNotification underwent formalized approvals and was both spread and sustained by the institution. After the pilot, eNotification was implemented across the region and within two years, 92 percent of FPs were able to receive alerts.
Discussion
Using concepts that originate in IE rendered visible gaps in different locations throughout the health system. Starting from a particular standpoint and articulating a problematic through the use of realistic accounts helped stakeholders orient to the problem as one about relationships between providers, not just technology. Mapping enabled the identification of potential consequences, such as the danger that the project would stagnate due to conflicting priorities within the health authority, as well as new opportunities, such as the chance for FPs to send in patient information upon receipt of an admission notification so that their extensive knowledge of the patient could be shared. Pence’s (2001) concept of processing interchanges gave structure to the informal conversations and using auditing procedures enabled me to engage with all actors who could be affected by the solution. Thus, IE procedures enabled challenges and prospects to be explicitly managed in early stages of implementation, instead of becoming obstacles to uptake or lost opportunities in the future. This is an essential consideration in applied sociological endeavors, as implementing change within existing institutional contexts requires sensitivity to both organizational mandates and resource pressures.
As with all methods, IE has limitations. Although useful for mapping processes and understanding complex information exchanges, it does not quantify results in a way that could be easily generalized to another setting. The engagement of multiple health care professionals at each step of the process helps ensure validity, but it is possible that a different group of people beginning from a different point of inquiry may have identified different issues. To some, the method may seem to lack rigor as it does not emerge from pre-existing theory, but from grassroots conversations that are often informal in nature, although it should be noted that this limitation may be balanced by the benefits that such an approach have for creating collaborative relationships among stakeholders. Finally, the process by which the inquiry unfolded would be difficult to replicate.
In addition, an important limitation must be noted regarding the application of IE in this study. An explicit intent of IE is to understand how ruling relations are reproduced through the coordination of individuals through texts (Rankin 2017). From a sociological perspective, power is an essential consideration in any setting where individuals are navigating their everyday lives through the requirements imposed by institutions. However, there were both pragmatic and political considerations to attend to which made an explicit exploration of power difficult to accomplish. This is not to imply that power was “not a problem” for the individuals and groups who were affected by the creation and use of eNotification, and indeed other studies have demonstrated the complex power dynamics at play even between physician groups (e.g. see Lee 2008 for a description of some of the between-group dynamics of FPs and hospitalists).
Findings from this study can be applied in other health care settings. Practitioners wanting to improve the quality of patient transitions in their institution can benefit from an IE-inspired approach that engages interdisciplinary teams in an ongoing and collaborative fashion, examining the way in which individual work is coordinated with others’ through mapping processes, which can also identify important system gaps.
The project stands as evidence of the value of IE for developing robust partnerships and for the fact that practical applied solutions that last can emerge from such partnerships. The positive effect of the process has increased interest in cross-collaboration between the clinical, technical, and administrative staff who were involved, ensuring an ongoing sharing of world views that will undoubtedly be of continued value to the health system. As such, this project serves as an example of sustainable improvements that can be accomplished when a sociological approach is brought to issues that have traditionally been understood more narrowly as technological problems.
The success of eNotification is of course not solely due to an IE approach. The technological innovation is notable, and the commitment of health authority leadership was invaluable to ensuring that the project was properly resourced. What IE did was open up new avenues for exploration, which unearthed foundational problems related to the lack of a change management process when FPs began leaving acute care work. IE provided a mechanism through which the social relations that underpin “IMIT problems” could be brought to light, improving the likelihood of long-term success.
Health care delivery in Canada involves eHealth components that are essential to ensuring continuity across a patchwork of services administered at different jurisdictional levels. It is important that eHealth design attend to these social relations. The work of Canadian sociologist Dorothy Smith has great value in providing an approach for mapping the extra-local connections through which health work is accomplished, recognizing that the texts that “write the social” are increasingly electronic (D. Smith 1999).
Supplemental Material
sj-docx-1-jax-10.1177_19367244211000709 – Supplemental material for Using Institutional Ethnography to Bridge the Gap and Develop eHealth Communications for Patient Transitions in British Columbia
Supplemental material, sj-docx-1-jax-10.1177_19367244211000709 for Using Institutional Ethnography to Bridge the Gap and Develop eHealth Communications for Patient Transitions in British Columbia by Kristin Atwood in Journal of Applied Social Science
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author was employed by the organization that undertook the research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the project was provided to the organization by the Shared Care Commitee, a Joint Collaborative Committee of the BC Ministry of Health and Doctors of BC.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.