
Abstract
Rosemary (Rosmarinus officinalis L.) and its essential oil offers a wide range of therapeutic benefits, supported by both in vitro experiments and clinical research. Its key compounds, 1,8-cineole, camphor, and α-pinene, along with other minor constituents, contribute to its unique scent and are responsible for bioactivity. Aromatherapy with rosemary essential oil, documented in 39 scientific references available in scientific databases Scopus, WoS, Google Scholar, has been shown to enhance cognitive function, sleep quality, mood, and pain management, while also showing potential for addressing conditions such as androgenetic alopecia and various types of pain. In practice, rosemary oil is commonly used pure, occasionally diluted in some carrier oil, and less frequently in combination with other essential oils, for massage or inhalation therapies. Despite its beneficial effects, rosemary oil is not without risks. Case reports have documented allergic reactions, including contact dermatitis and, in rare instances, anaphylaxis. These observations underscore the need for caution, particularly in individuals with known sensitivities to specific compounds of the essential oil. Overall, rosemary essential oil represents a valuable modality within aromatherapy and integrative health approaches. However, its safe application requires careful consideration of both therapeutic benefits and potential adverse effects, emphasizing the importance of informed use in clinical and home settings. This review systematically compiles and evaluates current scientific evidence on rosemary essential oil in aromatherapy, highlighting its therapeutic potential, practical applications, and safety considerations, thereby providing a comprehensive resource for researchers and practitioners.
Keywords
Introduction
Rosemary (Rosmarinus officinalis L.) is an aromatic member of Lamiaceae family originated from the Mediterranean region, and cultivated worldwide due to its decorative, aromatic, and medicinal properties. 1 Its common name comes from the Latin words ros (meaning “dew”) and marinus (meaning “sea”), translating to “dew of the sea”. 2 Rosemary is an evergreen perennial shrub with a well-developed fibrous root system that is tolerant to drought. 3 Aboveground, it grows into a shrub 1–1.5 meters tall with multiple branches. The perennial branches have dark grey, layered bark, while the annual ones are covered in light grey hairs. 4 The leaves are needle-shaped, arranged in opposite pairs, and are highly aromatic. Rosemary is almost always in bloom, producing small, two-lipped flowers that can be white, pink, purple, or blue. The seeds are small and brown.
Rosemary is recognized as a traditional spice and medicinal plant as well as a promising plant in modern pharmaceutical, cosmetic, and food industries. Today, rosemary is an important essential oil-bearing crop, especially for Morocco and Tunisia, where it is cultivated but also collected from wild shrubs, while in Spain, France, and Italy it is predominantly cultivated for raw material. 5 Rosemary oil is a clear, mobile, colourless or pale-yellow liquid with a characteristic odour, obtained by steam distillation from the aerial parts of the plant. Rosemary essential oil (Rosmarini aetheroleum) is utilized in the cosmetic industry for various products, including soaps, shampoos, gels, rosemary alcohol, rosemary water, cleansing milk, deodorants, anti-wrinkle creams, aftershave lotions, hydrating facial creams, as well as massage and aromatherapy formulations. 6 Alongside lavender, 7 and rose essential oils, 8 rosemary essential oil is frequently used in aromatherapy practices, as evidenced by a significant number of publications summarized in the following text.
Considering the growing popularity of aromatherapy as a complementary and alternative therapeutic approach, it is essential to establish a solid scientific basis for the use of essential oils. Numerous studies have demonstrated a strong connection between aromatherapy and both physiological and psychological responses. Therefore, it is important to use essential oils of standardized quality in accordance with ISO standards, as their bioactivity is directly determined by their chemical composition. Moreover, certain essential oils or specific chemical constituents within them can cause adverse reactions, including skin irritation, allergic responses, and in rare cases systemic toxicity. Balancing therapeutic efficacy with potential clinical risks requires careful evaluation of both pharmacological and toxicological data. Particular attention should be given to the appropriate route of administration, optimal dosage, and duration of exposure. Establishing evidence-based guidelines for the safe and effective use of essential oils is crucial for integrating aromatherapy into mainstream healthcare practices and ensuring patient safety. All of these aspects are addressed in the present review.
Search Strategy
We conducted a comprehensive literature search across four main databases: Web of Science, PubMed, Scopus, and Google Scholar. The search strategy included combination of following keywords: rosemary, Rosmarinus officinalis, essential oil, aromatherapy, inhalation, massage, and ingestion. To ensure the relevance and quality of the included studies, review papers were excluded. Furthermore, duplicates, publications without full-text access, studies that did not present controlled clinical trials, randomized or crossover designs, quasi-experimental pre-test/post-test approaches, or animal experiments were removed. In total, 39 studies meet the inclusion criteria and provided scientific evidence regarding the inhalation, massage, and oral application of rosemary essential oil in aromatherapy practice, including three studies conducted on experimental animal models. The data extracted from all included studies were summarized in Table 1. To aid an interpreting the results, additional discussion focuses on the key chemical compounds of rosemary essential oil responsible for its fragrance, biological activity, and aromatherapeutic effects. To provide a comprehensive overview, this review also addresses the report adverse effects of rosemary essential oil and summarizes selected blending formulations used in aromatherapy practice.
Review of Research Studies on the Effects of Rosemary Aromatherapy (the results are Listed According to the Year of Publication, from Newest to the Oldest, and Within One Year in Alphabetical Order).

N/A – not applicable.
Aromatherapy Application
Aromatherapy is a branch of phytotherapy that uses essential oils to support health by promoting relaxation and stress relief, enhancing mood, restoring balance and well-being, relieving minor discomforts, and supporting the immune, respiratory, and circulatory systems. The term derives from “aroma”, meaning fragrance or smell, and “therapy”, meaning treatment. Although it does not cure major illnesses, it is considered an effective complementary therapy, mainly applied through inhalation (via the respiratory tract and olfactory pathways), topical absorption (massage and cosmetic aromatherapy involving essential oils for the skin, body, face, and hair), or ingestion (oral administration). 48
Based on a review of 39 papers that include animal studies, controlled clinical trials, and quasi-experiments, it is evident that rosemary essential oil has significant potential for use in aromatherapy (Table 1). It may improve cognitive function and sleep quality, reduce stress and anxiety, relieve depression and pain, stimulate mood, and be effective in the treatment of androgenetic alopecia. However, three studies reported no significant effects of rosemary essential oil in aromatherapy applications.
As shown in the available studies listed in Table 1, rosemary essential oil applied via inhalation ortopically has been found to improve cognitive function,9,15,16,2328–30,33,34,43,47 enhance sleep quality,9,12,13 and reduce stress and anxiety.9–11,13,19,25,26,38,42,44–46 Additionally, it may help relieve depression,13,19 reduce pain, 18 20–22,24,32,35,37,39 and improve mood state. 31 40–42,47 Rosemary aromatherapy has also been reported to be effective in the treatment of androgenetic alopecia. 36 However, three studies found no significant effects of rosemary essential oil aromatherapy.14,17,27 A visual representation of these activities is shown in Figure 1.
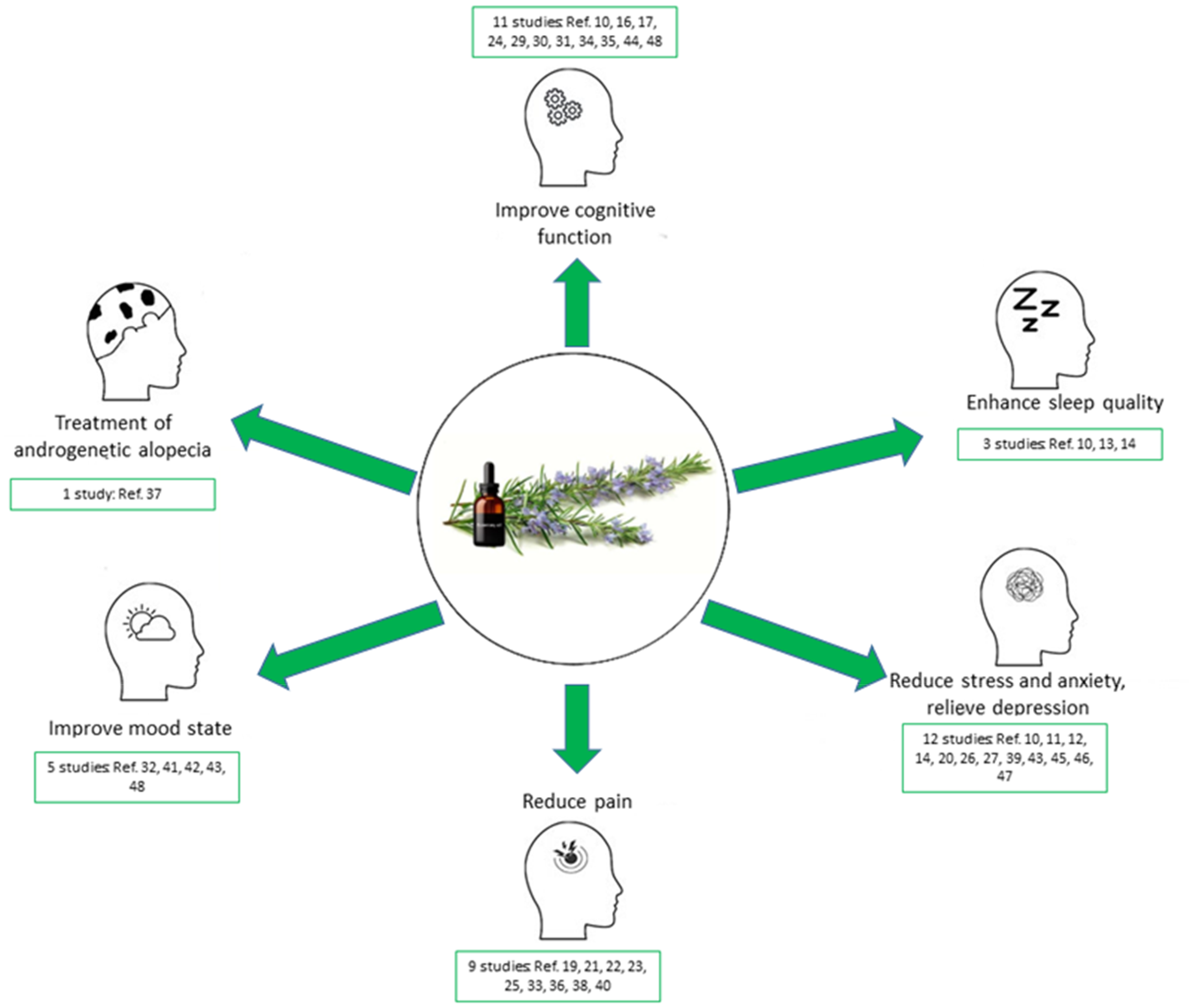
Health-related effects of rosemary essential oil via inhalation or massage. Each panel displays an icon and outcome label, with representative citations below. Outcomes with overlapping psychological effects are consolidated for clarity.
Chemical Composition
At the market, according to ISO 1342 standard, 49 two main types of rosemary essential oil are available: the 1,8-cineole (eucalyptol) chemotype, known as the Tunisian or Moroccan type, and the camphor chemotype from Spain. Quantification of the representative compounds is shown in Table 2. These two types differ in aroma: the Tunisian or Moroccan type has a fresh herbal aroma, with camphoraceous scent, while the Spanish type has a strong camphoraceous aroma with minty and medicinal notes.
Limited Values (in %) for Representative Compounds in Rosemary Essential Oil According to ISO 1342 Standard. 49
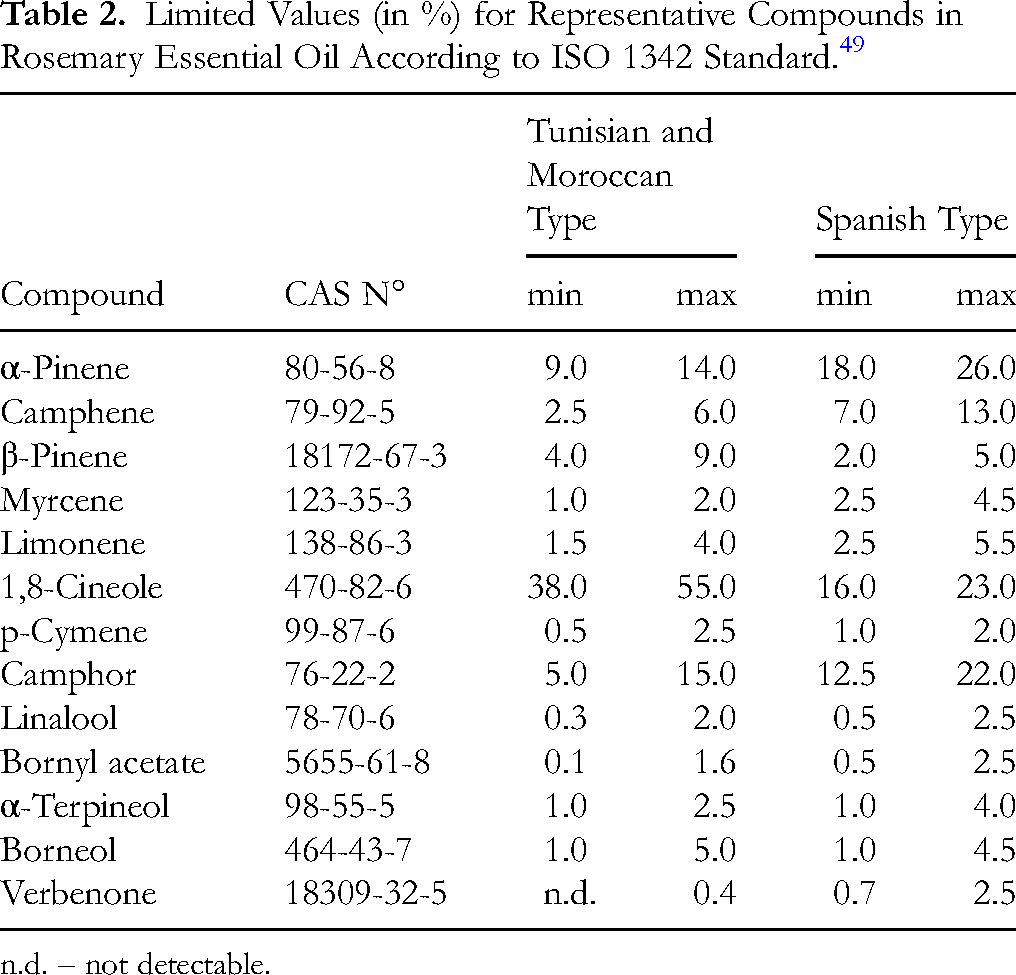
n.d. – not detectable.
The three most abundant compounds in rosemary essential oil that contribute to its aroma and biological activity are: 1,8-cineole, camphor, and α-pinene (Figure 2), along with numerous other minor constituents such as camphene, β-pinene, myrcene, limonene, p-cymene, linalool, bornyl acetate, α-terpineol, borneol, verbenone and others. These compounds exhibit significant biological activity, giving rosemary essential oil a strong therapeutic potential. Consequently, it is widely used in the pharmaceutical industry, as well as in cosmetics, the food industry, and aromatherapy.

Structural formulas of the main compounds in rosemary essential oil.
1,8-Cineole
1,8-Cineole, also known as eucalyptol, is a bicyclicmonoterpene with a strong herbal odor and a minty, camphoraceous, eucalyptus-like flavor. The main sources of this compound are eucalyptus, rosemary, and camphor laurel. 50 1,8-Cineole exhibits therapeutic properties in the treatment of various respiratory conditions, digestive disorders and cardiovascular diseases.51–54 Moreover, it shows potential in combating various types of cancer, including leukemia, as well as skin, oral, colon, breast, liver, and ovarian cancers.51,55 It also exhibits strong antioxidant, anti-inflammatory and antimicrobial properties. 56 Finally, studies have shown that 1,8-cineole, when applied by inhalation, can relieve anxiety, 57 prevent depression, 58 improve cognitive performance, physiological arousal, and well-being, 59 reduce inflammation, 60 and pain. 61 These biological activities of 1,8-cineole are directly related to the aromatherapeutic potential of rosemary essential oil, given the dominance of this compound in its composition.
Camphor
Camphor is a bicyclic monoterpene ketone with a strong, characteristic camphoraceous, penetrating, pungent, and aromatic odor resembling a mothball-like fragrance. The primary plant sources for industrial camphor extraction include camphor laurel, camphor tree, camphor basil, and others. Camphor is widely used in households as a fumigant and insect repellent, and in religious ceremonies.62,63 It is also commonly incorporated into cosmetics and pharmaceutical formulations due to its vasodilatory properties, which stimulate blood circulation, induce both cooling and warming sensations, and provide mild local anesthetic effects.64,65 At low doses, camphor exhibits anti-inflammatory activity, whereas higher doses may cause irritation. 66 Prolonged topical application (exceeding one month) may lead to contact dermatitis. 64 Additionally, camphor inhalation has been shown to induce significant changes in psychophysiological parameters, suggesting sedative effects. 67 However, prolonged inhalation or ingestion can lead to systemic toxicity, with seizures potentially being the first clinical sign. 68 Additionally, camphor is rapidly absorbed from the gastrointestinal tract, and within 5–15 min, initial symptoms such as nausea, vomiting, and abdominal pain may appear; in more severe cases, additional symptoms like headache, dizziness, confusion, agitation, anxiety, and hallucinations can develop. 69 Therefore, caution is advised when using rosemary essential oil, especially when taken orally, and its use should be under the supervision of a qualified healthcare practitioner. 70
α-Pinene
α-Pinene is a highly volatile monoterpene with a fresh pine scent and woody flavor, found in conifers, junipers, angelica, and many other plants. Investigations have indicated that α-pinene exhibits a wide range of biological activities, including antimicrobial, antiparasitic, anti-inflammatory, antioxidative, neuroprotective, gastroprotective, antiapoptotic, and antitumor potential. 71 α-Pinene is used as a food-flavoring ingredient, in pharmaceuticals, cosmetic formulations (such as products for oral and lip exposure, body lotions, and creams), household care products (including detergents and air fresheners), as well as in the agricultural sector for eco-friendly pest management due to its insecticidal and nematocidal effects.72,73 Additionally, α-pinene is considered a promising alternative biofuel, especially as a jet fuel replacement, due to its low moisture absorption, high energy density, and excellent flow properties at low temperatures. 74 Inhalation of α-pinene at therapeutic concentrations induces an anxiolytic-like effect, 75 alleviates depressive-like behavior, 76 and shows potential for the therapeutic treatment of mental health conditions such as schizophrenia. 72
In summary, the presence of camphor in rosemary essential oil induces vasodilation when applied to the skin, increasing local blood circulation and producing alternating cooling and warming sensations, while providing a mild local anesthetic effect. These properties support the clinical observations that rosemary aromatherapy massage can reduce pain and inflammation in osteoarthritis,18,21,24,39 decrease neuropathic pain severity, 32 relieve menstrual pain,20,37 and may be effective in treating androgenetic alopecia. 36 Furthermore, 1,8-cineole and α-pinene act via olfactory pathways, by inhalation reaching brain activity with thirty minutes. 77 They influence emotional centres and exert aromatherapeutic effects, including reducing anxiety and depression, enhancing cognitive performance, and improving overall well-being. This is indicated by a significant number of studies, which show that rosemary essential oil is very popular for inhalation (Table 1).
Side Effects of Rosemary Aromatherapy
Contact dermatitis from rosemary is uncommon but may be underdiagnosed, so it should be considered in the differential diagnosis of dermatitis. 78 It is advisable to properly dilute rosemary essential oil in carrier oil and perform a test on forearm before applying it to the skin, as its components can cause irritation in sensitive individuals. However, toxic side effects of rosemary essential oil may occur with components of the essential oil. 79 Several published case reports of rosemary-induced contact dermatitis were identified. These reports highlight the plant's potential to cause allergic reactions, including allergic contact dermatitis and, in rare cases, severe anaphylaxis. Clinical manifestations range from localized eczema and itching to systemic responses such as respiratory distress. Reactions have been triggered by various forms of exposure and were confirmed through patch or prick testing.
This review compiles documented case reports of rosemary-induced allergic responses, with a focus on the type of exposure and clinical presentation. The cases are grouped into the following categories based on the context and route of exposure: aromatherapy-related reactions, topical herbal preparations such as poultices, plasters, and alcohol, cosmetic and personal care products, plant contact through direct handling or environmental exposure, ingestion-related dermatitis, occupational exposure, and severe systemic reactions including anaphylaxis. This categorization helps illustrate the varied manifestations of rosemary allergy and emphasizes the importance of considering rosemary as a potential allergen in both clinical and occupational settings.
Aromatherapy-Related Reactions
A 45-year-old woman developed widespread dermatitis after using a mixture of essential oils for pain relief. 80 Patch tests revealed allergies to several oils, including rosemary.
Topical Herbal Preparations
A 45-year-old man developed blistering dermatitis on the thigh after using an herbal poultice containing rosemary and thyme. 81 Patch testing confirmed allergic contact dermatitis caused by both, rosemary and thyme in the poultice. A 56-year-old man developed itchy, vesicular dermatitis after using rosemary leaf plasters for knee pain. 82 Symptoms resolved after withdrawal. A 53-year-old man had recurring itchy eruptions with skin peeling on the chest after applying rosemary alcohol. Allergies confirmed to rosemary and other Lamiaceae species. 83
Cosmetic and Personal Care Products
A 23-year-old woman developed facial dermatitis linked to a cleansing gel containing rosemary leaf extract. 84 Patch test confirmed allergy to rosemary.
Plant Contact
A 48-year-old woman developed swelling and eczematous lesions on her hands, eyelids, and face after touching rosemary during a walk. 85 Patch and photopatch tests confirmed rosemary allergy. A 62-year-old woman had recurrent dermatitis on hands, forearms, and face after handling rosemary in sunlight. 86
Ingestion-Related Dermatitis
A 59-year-old man with chronic cheilitis linked to regular ingestion of rosemary-flavored food. 87 Symptoms resolved after dietary elimination of rosemary.
Occupational Exposure
A 56-year-old man developed occupational allergic contact dermatitis on his hands, forearms, and face after contact with rosemary leaf extract. 88 He reacted to carnosol, a naturally occurring compound found in rosemary.
Severe Systemic Reactions
A 16-year-old girl experienced multiple allergic reactions, including anaphylaxis, after exposure to rosemary via ingestion, skin contact, and airborne exposure. 89 Skin tests confirmed allergies to rosemary and lavender.
Balancing Therapeutic Benefits and Clinical Risks
Achieving this balance between therapeutic benefits and clinical risks requires careful consideration of individual patient and specific therapeutic goals, and the good knowledge of the chemical composition and biological potential of the oil used as a complementary therapeutic agent. Ultimately, a nuanced understanding of both benefits and risks allows practitioners and users to apply rosemary aromatherapy responsibly, integrating its therapeutic potential into holistic health approaches while safeguarding patient safety.
According to the reviewed studies, in inhalation aromatherapy, rosemary essential oil is typically applied at a dose of 2–5 drops, either pure or diluted in a carrier oil such as sweet almond or borage oil (at 25%), placed on a cotton pad, cotton balls, or gauze positioned approximately 5–10 cm from the nose, often attached to the collar, for 30–60 min. Shorter exposure times are generally reported as ineffective. The oil may also be administered using diffusers or sprays. In most studies, inhalation aromatherapy with rosemary essential oil was performed for periods ranging from one week to one month to enhance cognitive function, improve sleep quality, and reduce anxiety levels.
Topical application of rosemary essential oil has been reported in the form of ointments that significantly reduce pain scores in knee osteoarthritis and rheumatoid arthritis, or as massage therapy lasting 15–20 min. For massage, rosemary essential oil is usually diluted in jojoba or black seed oil and applied two to three times per week to alleviate pain, anxiety, and depressive symptoms. Additionally, daily massage of the frontoparietal and vertex regions of the scalp for six months has been shown to be effective in the treatment of androgenetic alopecia. Oral administration of rosemary essential oil has been reported only in animal studies.
Compared with other widely used essential oils in aromatherapy, such as lavender 7 and rose, 8 rosemary essential oil occupies a distinct position due to its pronounced stimulating and cognitive-enhancing properties. While lavender and rose oils are primarily associated with relaxation, anxiolytic, and mood-stabilizing effects, rosemary essential oil is known to promote alertness, improve memory and concentration, and enhance overall mental performance. These effects are largely attributed to its high content of 1,8-cineole, camphor, and α-pinene, compounds that modulate neurotransmission and cerebral blood flow. Consequently, rosemary essential oil serves as a complementary counterpart to sedative oils like lavender and rose, offering a more invigorating and performance-oriented profile within aromatherapy practice.
Blending
Rosemary essential oil (CAS No: 8000-25-7) has a distinctive flavor and aroma, primarily attributed to its high content of 1,8-cineole, camphor, and α-pinene. It is typically classified as a fresh, herbal-type of essential oil. A review of the literature revealed that only two articles addressed blending rosemary essential oil with other oils and the development of aromatherapy recipes containing rosemary.90,91 It can be mixed with lavender oil (floral scent), peppermint oil (menthol scent), eucalyptus oil (medicinal scent), pine oil (green scent), patchouli oil (woody scent), and lime oil (fruity scent) to enhance both the aroma and therapeutic properties (Figure 3).7,48,92–99

Suggested aromatherapy blends: Proportions of rosemary essential oil with complementary floral, menthol, medicinal, green, woody, and fruity scents.
Conclusion
This review provides the first comprehensive, evidence-based synthesis of the therapeutic effects, mechanisms, and safety of rosemary essential oil (Rosmarinus officinalis; Rosmarini aetheroleum) in aromatherapy. By integrating data from controlled clinical trials, randomized studies, and animal models, it evaluates inhalation, massage, and oral applications while emphasizing standardized essential oils and their chemical composition. Rosemary essential oil, when used in aromatherapy, has been shown to enhance cognitive function, sleep quality, mood, and pain management, while also showing potential in addressing conditions such as androgenetic alopecia and various types of pain. In addition, the review balances the documented health benefits with potential adverse effects, such as contact dermatitis resulting from prolonged topical application or hypersensitivity reaction to essential oil compounds. Finally, it provides practical insights into application methods and dosages (eg, dilution in carrier oils and blending with other essential oils), thereby bridging the gap between scientific evidence and real-world aromatherapy practice.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Ministry of Science, Technological Development and Innovation of the Republic of Serbia, grant number: 451-03-136/2025-03/200032.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.