
Abstract
Background
Traditional medicine remains a vital component of primary healthcare, especially in regions with limited access to modern pharmaceuticals. Ethnomedicine explores how different cultures manage health and disease through traditional practices. Despite urbanization, many Kenyans rely on herbal remedies, yet comprehensive documentation is lacking. This study aimed to identify and analyze medicinal plants used in Westlands Subcounty, Nairobi, to preserve indigenous knowledge and support pharmacological research.
Methods
An exploratory qualitative study was conducted using semi-structured interviews, focus group discussions, market surveys, and field observations. A purposive and snowball sampling approach recruited key informants, including traditional healers, CAM practitioners, and community leaders. Data on medicinal plants, usage, and preparation methods were analyzed using ethnobotanical indices such as ICF, UV, RFC, RI, and JI.
Results
A total of 35 medicinal plant species from 22 families were documented for over 40 health conditions. The dominant families were Zingiberaceae, Lamiaceae, and Apiaceae. Leaves (43.8%) and seeds (21.9%) were the most used plant parts, with oral (74.4%) and topical (15.4%) routes of administration prevailing. Decoctions, raw consumption, and infusions were common formulations. High ICF values for immune support (26%), gastrointestinal disorders (23%), and respiratory ailments (15%) indicated strong informant consensus.
Conclusion
This study highlights the rich ethnobotanical knowledge in urban Kenya, emphasizing the need for scientific validation and conservation of medicinal plants. Findings support the integration of traditional medicine into modern healthcare. Future research should focus on clinical validation, safety assessments, and policy frameworks to enhance the sustainable use of medicinal plants.
Keywords
Introduction
Ethnomedicine is a specialized sub-discipline of anthropology that investigates how diverse ethnic societies conceptualize health, diseases, and therapeutic practices. 1 The utilization of plants for disease prevention and treatment has been a cornerstone of traditional medicine systems for centuries. Complementary and Alternative Medicine (CAM) is one of the fields that extensively leverages the medicinal properties of plants. CAM encompasses a broad spectrum of healthcare products, therapies, and treatment modalities that fall outside the scope of conventional medical practice. 2 Well-established traditional medical systems such as Ayurveda, Homeopathy, and Naturopathy have extensively explored the therapeutic potential of medicinal plants, contributing to the growing body of ethnopharmacological knowledge.
The integration of plant-based remedies in disease management has been deeply embedded in the cultural traditions of various ethnic groups worldwide. The medicinal properties of these plants are largely derived from ancestral knowledge passed down through generations through trial-and-error practices. Ethnomedicine not only examines the biomedical effects of plant-based treatments but also explores the ways in which individuals perceive and respond to illnesses, alongside their culturally defined healing methodologies. 3
Ethnomedicine serves two primary objectives. The first is to document and analyze the medical theories and empirical knowledge developed and refined by specific communities over time. The second is to facilitate medical translation, which enables cross-cultural comparisons of ethnomedical knowledge. This translation process is instrumental in integrating traditional healthcare insights into contemporary medical systems, enhancing healthcare delivery in culturally diverse populations. Furthermore, it provides an avenue for the scientific evaluation of plant-based therapies, potentially leading to the discovery of novel pharmaceutical agents or complementary treatment options. 4
Historically, plant-derived compounds have played a foundational role in the advancement of modern pharmaceuticals. The extraction of bioactive compounds from medicinal plants in the nineteenth century catalyzed the synthesis of early pharmaceutical drugs, marking the transition toward contemporary medical practices. Given this historical precedent, there is increasing advocacy for the scientific validation of traditional medicine. Within CAM, complementary medicine refers to therapies that are employed alongside conventional pharmaceutical interventions. As modern healthcare continues to evolve, an in-depth understanding of drug-herb interactions has become a critical component of pharmacology, underscoring the importance of ethnobotanical research in ensuring the safe and efficacious use of traditional remedies.
Across the globe, numerous traditional medicine systems have been practiced for centuries, including Chinese herbal medicine, African traditional medicine (ATM), Ayurveda, Shamanism, Siddha, Unani, and Vietnamese medicine. Each of these systems has evolved in response to regional biodiversity and accumulated cultural knowledge, collectively shaping the diverse ethnobotanical landscape observed today.
Traditional Medicine in Africa and Kenya
Despite significant advancements in Western medicine, traditional healing practices remain deeply embedded in African societies. ATM is one of the oldest and most diverse traditional healing systems, characterized by an extensive repository of medicinal plants utilized by various communities. Kenya, for instance, harbors over 7000 indigenous plant species, of which approximately 1200 have been identified for their medicinal properties. 5
While Western medical practices continue to gain prominence, certain Kenyan communities, such as the Samburu and Maasai people, continue to rely on traditional healing methods. However, despite their widespread use, many herbal practices remain undocumented, posing a risk of irreversible loss of valuable ethnobotanical knowledge. Over the years, ethnomedical surveys in Kenya have largely focused on rural and semi-nomadic populations, particularly the Maasai community. Research efforts have documented the extensive utilization of herbal medicine among the Maasai people in Narok County, reinforcing the continued reliance on medicinal plants for primary healthcare needs.6-10
The erosion of ethnobotanical knowledge in urban areas is an emerging concern. Several factors contribute to this decline, including the absence of systematic documentation, the aging of traditional knowledge custodians, rapid modernization, lifestyle transitions, and increased formal education. With younger generations gravitating toward modern lifestyles, traditional healing practices are being progressively marginalized. To counteract this trend, it is imperative to conduct ethnobotanical studies in urban settings, ensuring that traditional medicine remains a viable and recognized component of national healthcare systems.
This study aimed to identify and document medicinal plants utilized by residents and traditional healers in Westlands, Nairobi. By compiling and preserving this ethnobotanical knowledge, the study contributes to future drug discovery research, including the validation of pharmacological activity, phytochemical profiling, and toxicity assessments. While many prior studies have focused on rural and semi-nomadic communities, such as the Maasai and Samburu populations, there remains a significant gap in the documentation of ethnomedicinal knowledge in urban environments.
To bridge this gap, our study provides a comprehensive ethnobotanical survey in Westlands Subcounty, Nairobi, an urban area where traditional medicine coexists with modern healthcare systems. Westlands was chosen due to its unique demographic composition, representing a diverse socioeconomic landscape where traditional medicine coexists with modern healthcare systems. Westlands comprises high-income residential areas, informal settlements (such as Kangemi), and a significant Kenyan-Asian population, making it an ideal location to study how different socioeconomic groups access and utilize medicinal plants. The area also has a dynamic cultural mix, which allows us to explore variations in traditional knowledge retention and adaptation in an urban setting. Furthermore, Westlands has easy access to both formal healthcare facilities and informal herbal medicine markets, making it an important location for studying the integration of traditional medicine into urban healthcare systems. The findings from this study will help compare urban and rural medicinal plant use, offering insights into how urbanization and socioeconomic diversity impact ethnobotanical practices.
Our research investigates how medicinal plants are still being used, their cultural significance, and their role in urban healthcare settings. By examining medicinal plant use in an urbanized setting, this study provides new insights into the adaptation, preservation, and potential loss of traditional knowledge in urban communities. Furthermore, the findings from this study contribute to conservation efforts, pharmacological validation, and the integration of traditional medicine into formal healthcare systems. This documentation is essential for policy development, ensuring that traditional medicine remains a recognized and well-documented healthcare option for urban populations. The findings may also inform policy decisions on the integration of traditional medicine into national healthcare frameworks. Additionally, the documented medicinal plants hold the potential to support local economic development by fostering revenue-generating opportunities for communities engaged in herbal medicine trade and conservation initiatives.
Results
Socio-Demographical Data Analysis
A total of thirty-five participants were interviewed in this study, consisting of 13 men (37%) and 22 women (63%). While this gender distribution does not represent the overall demographic structure of the study region, it reflects the greater involvement of women in traditional medicine practices at the household level, positioning them as key informants. According to the 2019 Kenyan census, the male-to-female ratio in Westlands Subcounty was 99.2:100, indicating a relatively balanced population distribution. The majority of participants (48%) were aged between 31–50 years, followed by 26% in the 51–65 years category, 17% between 18–30 years, and 9% aged 65 years and above. The study findings suggest that traditional medicinal knowledge is predominantly preserved among older individuals (51 years and above) (75%), highlighting their critical role in maintaining and transmitting ethnomedicinal practices within the community. This aligns with the findings of Kigen et al, (2019), who reported that urbanization is accelerating the decline of indigenous knowledge by disrupting the intergenerational transmission of traditional medicinal practices, thereby distancing younger generations from their cultural heritage (Figure 1).

Age Distribution of Study Participants.
Educational Background
Educational attainment among participants was notably high, with 73% having attained tertiary education, 17.3% completing secondary education, 7.8% primary education, and 3.8% lacking formal education (Figure 2). The high level of education observed can be attributed to the urbanized nature of Westlands, which hosts numerous primary and secondary schools and emphasizes the importance of education. As a result, over 70% of the respondents have pursued higher education as a means to navigate the challenges of urban living and the high cost of living.

Education Level Distribution Among Study Participants.
Employment and Income Levels
Employment status among participants revealed that 74.3% were employed, 20% were unemployed, while 5.7% were self-employed as business owners. The average number of medicinal plants used was highest among individuals with an income below 5000 KSH, followed by those earning 81,000–100,000 KSH. Across all income groups, most participants preferred using traditional medicine before seeking conventional medical treatment. The primary reasons for this preference included greater accessibility, lower cost, and fewer side effects associated with herbal medicine compared to conventional pharmaceutical treatments. 8
Medicinal Plants Used in Westlands Subcounty
Diversity and Therapeutic Applications
The study documented 35 medicinal plant species classified under 22 botanical families, each exhibiting a broad range of therapeutic applications. These plants have been traditionally utilized in Westlands Subcounty for the treatment and management of infectious and non-infectious diseases, including respiratory conditions, gastrointestinal disorders, metabolic ailments, dermatological issues, immune modulation, and stress-related conditions. The widespread use of these species highlights the rich ethnobotanical knowledge within the community and underscores their significance in traditional medicine practices.
Among the documented plant families, Zingiberaceae (Ginger Family), Lamiaceae (Mint Family), and Apiaceae (Carrot Family) were the most dominant. The Zingiberaceae family, represented by species such as Zingiber officinale (Ginger), Curcuma longa (Turmeric), and Elettaria cardamomum (Cardamom), is well known for its anti-inflammatory, digestive, and decongestant properties. Plants from the Lamiaceae family, including Ocimum tenuiflorum (Holy Basil), Origanum vulgare (Oregano), and Salvia hispanica (Chia seeds), are widely used for respiratory conditions, immune support, metabolic regulation, and cardiovascular health. The Apiaceae family, containing species such as Cuminum cyminum (Cumin), Coriandrum sativum (Coriander), and Trachyspermum ammi (Ajwain), plays a significant role in digestive health, managing bloating, indigestion, and enhancing immune response (Table 1).
List of Medicinal Plants Used in the Westlands Subcounty.

A total of 35 medicinal plant species classified in 22 families were inventoried and reportedly used to treat more than 40 different infectious and non-infectious diseases.
Commonly Used Plant Parts and Routes of Administration
The most frequently utilized plant parts included leaves (43.8%), seeds (21.9%), fruits (9.4%), and roots (9.4%). Leaves were predominantly used due to their easy availability, cost-effectiveness, and high bioactive compound concentration. The increasing utilization of seeds in herbal medicine is attributed to their nutritional value and endorsement by certified nutritionists and traditional healers. Fruits and roots were less frequently used but were still significant in treating specific conditions such as respiratory infections, metabolic disorders, and inflammatory conditions. The routes of administration varied depending on the condition being treated, with the oral route (74.4%) being the most preferred due to its ease of preparation and efficient systemic absorption. The topical route (15.4%) was primarily used for skin conditions, wound healing, and localized pain relief. Other administration methods included steam inhalation for respiratory conditions, chewing raw plant parts, and applying plant extracts directly to affected areas.
Herbal Formulations and Methods of Preparation
The formulation of herbal remedies depended on the plant part used and the intended therapeutic effect. The most common methods of preparation included drinking decoctions (24.4%), consuming raw plant parts (19.5%), crushing and mixing plant material in water (14.6%), and incorporating plant parts into food preparations (14.6%). Decoctions were widely preferred for treating respiratory conditions, digestive disorders, and immune support, while raw consumption was favored for plants known to contain heat-sensitive bioactive compounds. Herbal remedies were also prepared as infusions, topical applications, or steam inhalations, depending on the targeted ailment.
The findings indicate that many of the documented medicinal plants have cross-cultural relevance and are also widely used in Ayurvedic, Traditional Chinese, and African Herbal Medicine systems. Their continued use in Westlands Subcounty highlights the importance of traditional knowledge in healthcare, particularly in communities with limited access to conventional medicine. The preference for herbal remedies was attributed to their availability, affordability, and lower risk of side effects compared to pharmaceutical drugs.
Given their widespread use and therapeutic potential, these medicinal plants warrant further phytochemical and pharmacological validation to confirm their efficacy, safety, and potential integration into modern healthcare systems. Additionally, conservation efforts are necessary to protect these valuable plant species from overharvesting and ensure sustainable utilization for future generations.
Quantitative Ethnobotanical Indices Analysis
Informant Consensus Factor (ICF) Values Analysis
The Informant Consensus Factor (ICF) is a crucial ethnobotanical index that helps evaluate the consistency of knowledge among informants regarding the use of medicinal plants for specific disease categories. Higher ICF values indicate greater agreement among informants, suggesting that a few highly effective species are used repeatedly for treating certain ailments, whereas lower ICF values suggest greater variation in plant use for a particular condition. The analysis of the ICF values in the present study provides insights into the most culturally significant medicinal plants and their importance in traditional healthcare systems (Table 2).
Informant Consensus Factor (ICF).
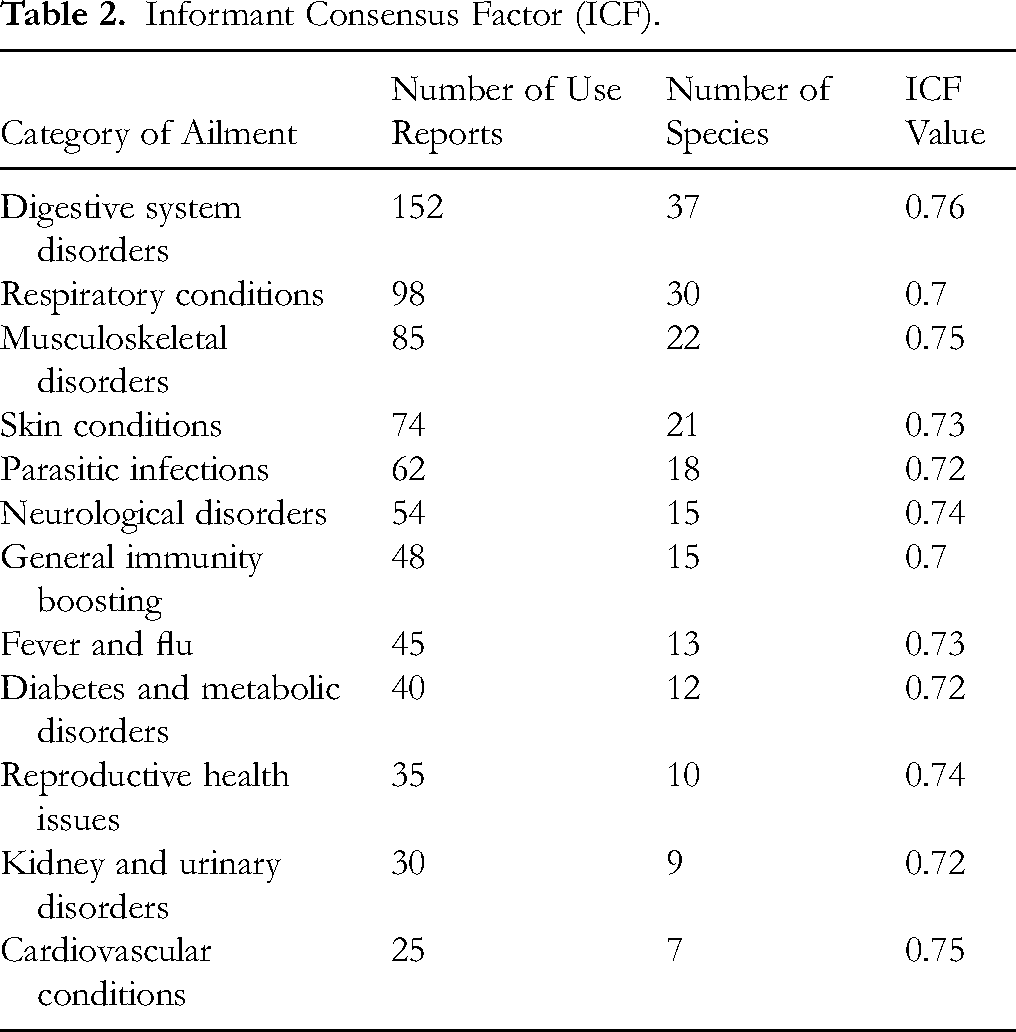
Digestive System Disorders: High ICF Value (0.76)
The ICF value (0.76) for digestive system disorders remains one of the highest, indicating strong consensus on the use of medicinal plants for conditions such as gastritis, diarrhea, ulcers, constipation, flatulence, and indigestion. Similar studies in Ethiopia 11 and Bangladesh 12 reported comparable values, demonstrating the universal reliance on plant-based remedies for digestive ailments.
Musculoskeletal Disorders: Strong Agreement (ICF = 0.75)
The ICF analysis shows 0.75 for musculoskeletal disorders, reflecting strong agreement among informants regarding plants used to treat arthritis, joint pain, and muscle cramps. Similar agreement levels were observed in South Africa. 13
The ICF analysis demonstrates an improved understanding of ethnobotanical knowledge consensus in Westlands Subcounty. The higher ICF values (>0.70) indicate strong agreement on the use of medicinal plants for digestive issues, respiratory conditions, musculoskeletal pain, and immunity boosting. The increase in ICF for diabetes and neurological disorders suggests growing recognition of specific medicinal plants for these conditions. Future research should focus on pharmacological validation, phytochemical analysis, and conservation strategies for the most frequently cited medicinal plants.
Use Value (UV) Analysis in Ethnomedical Research
The Use Value (UV) index was employed to assess the relative importance of medicinal plants based on their frequency of citation by informants. A higher UV score indicates that a plant is more frequently used and considered highly significant in traditional medicine.14,15 Table 3 presents the results of the UV analysis for the most frequently cited medicinal plants.
Most Frequently Cited Medicinal Plants by Their use Value (UV).

Among the medicinal plants documented, Zingiber officinale (Ginger) had the highest UV value (0.64), indicating its widespread use in treating digestive disorders, inflammation, and respiratory conditions. This was followed by Ocimum tenuiflorum (Holy Basil) with a UV of 0.58, highlighting its frequent application for respiratory ailments, immunity boosting, and stress relief. Allium sativum (Garlic) (UV = 0.55) was also highly cited for its antimicrobial and cardiovascular benefits, reflecting its traditional role in preventing infections and improving circulatory health. 16
Curcuma longa (Turmeric) (UV = 0.50) and Eucalyptus globulus (Eucalyptus) (UV = 0.48) were commonly used for anti-inflammatory, wound-healing, detoxification, and respiratory therapies. Similarly, Aloe vera (UV = 0.46) and Azadirachta indica (Neem) (UV = 0.45) were widely recognized for their dermatological applications, particularly in treating wounds, burns, and skin infections.
Further, Moringa oleifera (UV = 0.42) was frequently mentioned for its immune-boosting and nutritional benefits, supporting its increasing integration into modern herbal medicine. Trigonella foenum-graecum (Fenugreek) (UV = 0.40) and Withania somnifera (Ashwagandha) (UV = 0.38) were noted for their role in metabolic regulation, stress management, and hormonal balance, making them important medicinal plants in traditional healing systems.
The Use Value (UV) analysis highlights the most culturally and therapeutically significant plants in Westlands Subcounty, with high UV values indicating strong traditional consensus on their effectiveness. Plants with UV values greater than 0.50 demonstrate strong cultural importance and should be prioritized for pharmacological validation, conservation efforts, and clinical research to assess their efficacy in modern medicine. These findings reinforce the necessity of integrating traditional knowledge with scientific research to enhance the development of natural therapeutic agents.14,15
Relative Frequency of Citation (RFC) Analysis
The Relative Frequency of Citation (RFC) index was calculated to determine the prominence of each medicinal plant species in traditional healthcare practices. A higher RFC value indicates that a plant is more widely recognized and frequently cited by informants, signifying its ethnobotanical importance.16-18
Among the documented species, Zingiber officinale (Ginger) had the highest RFC value (0.85), demonstrating its widespread use in treating digestive disorders, inflammation, and respiratory ailments. This was closely followed by Ocimum tenuiflorum (Holy Basil) (RFC = 0.78), which was frequently cited for its role in respiratory infections, immunity enhancement, and stress relief. Allium sativum (Garlic) (RFC = 0.75) was another highly cited plant, reflecting its antimicrobial, cardiovascular, and immune-boosting properties (Table 4).
Relative Frequency of Citation (RFC) Analysis.

Curcuma longa (Turmeric) (RFC = 0.70) also exhibited significant citation frequency, particularly for its anti-inflammatory, antioxidant, and wound-healing capabilities. Eucalyptus globulus (Eucalyptus) (RFC = 0.65) was well recognized for its decongestant and expectorant properties, making it a widely used remedy for respiratory conditions.
Other commonly cited plants included Aloe vera (RFC = 0.60) and Azadirachta indica (Neem) (RFC = 0.58), both of which are extensively used for dermatological applications, wound healing, and antimicrobial treatments. Moringa oleifera (Moringa) (RFC = 0.55) was acknowledged for its immune-boosting and nutritional benefits, while Trigonella foenum-graecum (Fenugreek) (RFC = 0.50) and Withania somnifera (Ashwagandha) (RFC = 0.48) were frequently cited for their role in metabolic regulation, stress relief, and hormonal balance.
The RFC analysis highlights the most culturally significant medicinal plants in Westlands Subcounty, with higher RFC values (>0.70) indicating strong agreement on their traditional use. The findings suggest that these plants are widely recognized and relied upon for their medicinal properties, emphasizing the need for further phytochemical research, pharmacological validation, and conservation efforts to ensure their continued availability and use in traditional medicine systems. The results also reinforce the critical role of traditional knowledge in identifying potent medicinal plants for further scientific exploration and integration into modern healthcare practices.
Relative Importance Index (RI) Analysis
The Relative Importance Index (RI) was calculated to assess the overall medicinal significance of plant species by integrating both the RFC and the Relative Number of Use Categories (RNUs). Higher RI values indicate that a plant is not only widely cited but is also used for multiple therapeutic purposes, making it an essential part of traditional medicine. 18
Among the documented species, Zingiber officinale (Ginger) had the highest RI value (0.86), reflecting its extensive use in managing digestive disorders, respiratory conditions, inflammation, and immune system support. Ocimum tenuiflorum (Holy Basil) (RI = 0.79) was also highly ranked due to its broad application in respiratory ailments, stress relief, and immune modulation. Allium sativum (Garlic) (RI = 0.76) exhibited similar importance, being frequently used for cardiovascular health, antimicrobial properties, and metabolic regulation (Table 5).
Relative Importance Index (RI) Analysis.

Curcuma longa (Turmeric) (RI = 0.71) ranked high due to its well-known anti-inflammatory, antioxidant, and wound-healing properties, while Eucalyptus globulus (Eucalyptus) (RI = 0.67) was recognized for its effectiveness in treating respiratory conditions, particularly colds, flu, and congestion relief. Aloe vera (RI = 0.62) and Azadirachta indica (Neem) (RI = 0.59) were highly valued for their extensive use in dermatological treatments, wound healing, and antimicrobial applications.
Moringa oleifera (RI = 0.57) demonstrated significant ethnobotanical importance due to its immune-boosting, nutritional, and antioxidant benefits. Meanwhile, Trigonella foenum-graecum (Fenugreek) (RI = 0.53) and Withania somnifera (Ashwagandha) (RI = 0.49) were valued for their role in metabolic regulation, stress adaptation, and hormonal balance.
The RI analysis highlights the most culturally and therapeutically significant medicinal plants in Westlands Subcounty. Plants with higher RI values (>0.70) demonstrate strong traditional significance and should be prioritized for scientific validation, conservation efforts, and pharmacological research. The findings further reinforce the importance of integrating traditional knowledge with modern medicine to explore potential therapeutic applications and ensure sustainable utilization of these valuable medicinal plants.
Jaccard Index (JI) Analysis
The Jaccard Index (JI) was calculated to assess the similarity between the medicinal plant species documented in this study and those reported in previous ethnobotanical studies from various regions. Higher JI values indicate greater similarity, meaning that a significant number of plants are commonly used in multiple locations, while lower JI values suggest distinct ethnobotanical practices. 16
The highest Jaccard Index (7.04%) was observed for Narok County, Kenya (Kigen et al, 2019), reflecting a relatively strong overlap in medicinal plant use between the two study areas. This suggests a shared traditional knowledge system likely influenced by similar cultural and environmental conditions. Likewise, Kajiado County, Kenya (Kiringe, 2006) exhibited a JI of 5.97%, indicating some level of medicinal plant use continuity within Kenyan regions (Table 6).
Jaccard Index (JI) Comparison Table.

Comparatively, Tanzania 20 and Uganda 21 had moderate JI values of 5.69% and 5.31%, respectively, showing that certain medicinal plant species are shared across East Africa. The JI for Ethiopia 11 was slightly lower at 4.90%, suggesting some degree of variation in ethnomedicinal plant use, possibly due to regional differences in flora and cultural practices.
Outside of Africa, India 22 and China 23 exhibited JI values of 4.92% and 4.73%, respectively, indicating a modest overlap in medicinal plant selection, likely influenced by Ayurvedic and Traditional Chinese Medicine systems. South Africa 13 and Brazil 24 recorded JI values of 4.52% and 4.58%, respectively, reflecting some degree of global convergence in herbal medicine practices. The lowest JI was observed for Turkey 25 at 4.27%, indicating that medicinal plant use in this study area differs significantly from the ethnobotanical traditions of Turkey.
The JI analysis highlights the influence of geography, cultural exchange, and ecological diversity in shaping medicinal plant knowledge across different regions. While some plants have cross-regional medicinal significance, others are used in region-specific ethnomedical practices. This underscores the importance of documenting and preserving traditional knowledge systems while integrating scientific validation to enhance the global acceptance and application of medicinal plants in healthcare. Future research should explore the pharmacological properties of common species to support their broader medicinal applications and conservation.
Discussion
The findings of this ethnobotanical study highlight the rich diversity of medicinal plants used by the residents of Westlands Subcounty, Nairobi, and their continued reliance on traditional medicine despite urbanization and the widespread availability of modern pharmaceuticals. A total of 35 medicinal plant species belonging to 22 botanical families were documented, with a broad range of therapeutic applications. These findings align with previous ethnobotanical studies in Kenya, Ethiopia, and other parts of Africa, emphasizing the persistence of indigenous knowledge in urban communities and the need for its systematic documentation and conservation.
Diversity and Therapeutic Applications of Medicinal Plants
The study identified Zingiberaceae, Lamiaceae, and Apiaceae as the dominant plant families, supporting their widespread use in traditional medicine worldwide. The Zingiberaceae family, represented by species such as Zingiber officinale (Ginger) and Curcuma longa (Turmeric), was frequently cited for anti-inflammatory, digestive, and respiratory treatments. Similar findings have been reported in other studies, where the Zingiberaceae family has been recognized for its bioactive compounds with strong pharmacological properties. 11 The Lamiaceae family, which includes Ocimum tenuiflorum (Holy Basil) and Origanum vulgare (Oregano), was primarily used for immune-boosting, metabolic, and cardiovascular applications, consistent with findings from previous ethnobotanical studies. 24
An emerging concern highlighted by this study is the potential overexploitation of frequently used medicinal plants, especially those with high use values and cultural significance. As demand for traditional remedies grows—both locally and globally—unsustainable harvesting practices may become an indirect driver of biodiversity loss, particularly in urban fringe areas where natural habitats are already under pressure. Balancing the therapeutic use of medicinal plants with their conservation requires integrated strategies, such as promoting community-based sustainable harvesting, encouraging domestication and cultivation of high-demand species like Zingiber officinale and Ocimum tenuiflorum, and implementing local biodiversity monitoring systems. These efforts can help mitigate the risk of plant population decline while preserving cultural heritage and supporting public health needs.
Patterns in Plant Part Utilization and Routes of Administration
The most commonly used plant parts in this study were leaves (43.8%), seeds (21.9%), fruits (9.4%), and roots (9.4%). The dominance of leaf-based remedies aligns with existing literature, where leaves are preferred due to their ease of harvesting, high bioactive compound concentration, and environmental sustainability. 12 Seeds have also gained prominence, particularly due to their high concentrations of essential oils, fatty acids, and bioactive phytochemicals that contribute to therapeutic effects. 26
In terms of routes of administration, oral ingestion was the predominant method (74.4%), with topical application (15.4%) used for dermatological and inflammatory conditions. The preference for oral decoctions, herbal teas, and raw plant consumption aligns with reports from other African ethnobotanical studies, 13 where decoctions were found to enhance bioavailability and medicinal efficacy.
ICF and Consensus on Disease Categories
Quantitative ethnobotanical indices, particularly ICF, revealed high agreement among informants on the use of medicinal plants for digestive disorders (ICF = 0.76), musculoskeletal conditions (ICF = 0.75), and respiratory ailments (ICF = 0.70). These findings indicate that local communities share extensive knowledge on the effectiveness of specific plants for treating common ailments, reinforcing their potential for scientific validation and pharmaceutical development.
The high ICF for digestive system disorders (0.76) suggests that medicinal plants such as Cuminum cyminum (Cumin), Coriandrum sativum (Coriander), and Zingiber officinale (Ginger) are widely recognized for their antispasmodic, anti-inflammatory, and digestive properties. This strong agreement is consistent with studies conducted in Ethiopia 11 and Bangladesh, 12 which reported similar reliance on plant-based treatments for gastrointestinal disorders.
Similarly, musculoskeletal disorders (ICF = 0.75) showed a strong consensus on the use of anti-inflammatory and analgesic plants, including Curcuma longa (Turmeric) and Brassica juncea (Mustard). Previous research in South Africa 13 supports this finding, highlighting the widespread use of turmeric in managing joint pain, arthritis, and muscle cramps.
The ICF for respiratory conditions (0.70) remained moderately high, reflecting the popularity of plants such as Eucalyptus globulus (Eucalyptus), Ocimum tenuiflorum (Holy Basil), and Allium sativum (Garlic) for treating colds, flu, and bronchial infections. Similar results were observed in Brazil, 24 where an ICF of 0.71 was recorded for respiratory ailments.
Use Value (UV) and Cultural Significance of Key Medicinal Plants
The Use Value (UV) index highlights the cultural embeddedness and therapeutic relevance of medicinal plants within the Westlands community. Zingiber officinale (UV = 0.64), Ocimum tenuiflorum (UV = 0.58), and Allium sativum (UV = 0.55) emerged as the most frequently cited species, reflecting both their accessibility and versatility in treating multiple ailments such as digestive disorders, respiratory infections, and inflammation. These findings mirror those from Bencheikh et al 14 in Morocco and Jin et al 15 in China, where high UV values were also reported for these species in urban and semi-urban ethnobotanical settings. The repeated citation of these plants underscores their perceived effectiveness and cultural familiarity, which may facilitate community acceptance in future integrative health interventions. Furthermore, these species have demonstrated pharmacologically active compounds in prior studies, supporting their potential as candidates for further clinical validation and drug discovery research.
Comparative Ethnobotanical Analysis Using Jaccard Index (JI)
The Jaccard Index (JI) was employed to compare the medicinal plant knowledge in Westlands Subcounty with other regions. The highest JI (7.04%) was observed for Narok County, Kenya, 7 indicating a strong overlap in plant use. This suggests that traditional knowledge transcends regional boundaries, with shared plant utilization between urban and semi-rural communities. Comparisons with Tanzania (JI = 5.69%) and Uganda (JI = 5.31%) revealed moderate ethnobotanical similarity, while the JI for Ethiopia (4.90%) was slightly lower, likely due to regional variations in flora and cultural practices. Notably, international comparisons with India (JI = 4.92%), China (JI = 4.73%), and South Africa (JI = 4.52%) suggest that some medicinal plants have cross-cultural therapeutic applications.
Implications for Conservation and Future Research
The study underscores the urgent need for conservation efforts to protect medicinal plants from overharvesting and habitat destruction. Urbanization and land-use changes threaten the availability of these species, necessitating sustainable harvesting strategies and conservation policies. Furthermore, as traditional knowledge is predominantly held by older generations, initiatives should be introduced to document, preserve, and integrate ethnobotanical knowledge into modern healthcare and education systems. Additionally, the findings highlight the potential for pharmacological studies to validate the efficacy of highly cited medicinal plants. Future research should focus on phytochemical screening, clinical trials, and toxicity assessments to ensure the safe and effective integration of traditional medicine into modern pharmacotherapy.
Limitations of the Study
This ethnobotanical study was conducted within a specific urban context—Westlands Subcounty, Nairobi—which, while diverse, may not fully represent the broader range of traditional medicinal practices across other urban or rural settings in Kenya. The use of purposive and snowball sampling, while appropriate for identifying knowledgeable informants, may have limited the inclusion of less connected community members or those from minority cultural backgrounds. Additionally, the reliance on self-reported data from interviews and discussions introduces the possibility of recall bias, where participants may unintentionally omit or misremember details regarding plant use, preparation, or efficacy.
One limitation of this study is the use of non-probability sampling techniques, such as purposive and snowball sampling. While these methods are appropriate for ethnobotanical research that requires the selection of knowledgeable informants, they may lead to potential overrepresentation of frequently cited individuals or commonly known plant species, thereby limiting the generalizability of the findings. Future studies could consider complementary probabilistic methods to ensure broader community representation.
Moreover, the study primarily focused on documenting traditional knowledge and applying quantitative ethnobotanical indices without conducting laboratory-based phytochemical or pharmacological analyses. As such, the therapeutic claims made by informants have not yet been scientifically validated. While the findings provide a strong foundation for future research, they should be interpreted as indicative rather than conclusive. The cross-sectional nature of the study also limits the ability to assess how knowledge and usage patterns may evolve over time, particularly among younger generations. Nonetheless, these limitations do not detract from the significance of the insights gained, which highlight the continued relevance and richness of traditional medicine in an urban Kenyan setting.
Conclusions and Recommendations
Conclusion
This study highlights the enduring value of ethnobotanical knowledge in an urban setting, documenting a rich diversity of medicinal plant species used in Westlands Subcounty, Nairobi. The range of plants identified, and the breadth of ailments they are used to treat—particularly digestive, musculoskeletal, and respiratory conditions—reflect a deep-rooted reliance on traditional medicine, even amid urbanization.
These findings not only underscore the cultural and therapeutic significance of traditional healing practices but also provide a vital record of indigenous knowledge that is at risk of being lost. The documentation serves as a foundation for future scientific investigations and offers promising leads for the discovery of bioactive compounds with potential for drug development.
Moreover, the results emphasize the need for conservation of medicinal plant species and support integrating traditional medicine into modern healthcare systems through policy, research, and education. Future work should build on this baseline by conducting phytochemical analyses, pharmacological evaluations, and toxicity studies to validate the safety and efficacy of the most commonly cited medicinal plants.
Recommendations
Pharmacological Validation and Clinical Research: The study recommends prioritizing the phytochemical screening, toxicity testing, and pharmacological evaluation of the most frequently cited medicinal plants—such as Zingiber officinale, Ocimum tenuiflorum, and Curcuma longa—to scientifically validate their safety and therapeutic efficacy. These findings offer a valuable starting point for the development of evidence-based herbal therapies.
Digital Documentation and Knowledge Preservation: In response to the ongoing erosion of traditional knowledge, urgent efforts should be made to document and digitally preserve ethnobotanical information. Such databases would serve as a critical resource for researchers, healthcare practitioners, and future generations.
Integration into National Healthcare and Conservation Efforts: Policymakers and stakeholders should consider integrating validated traditional medicine into national healthcare frameworks, particularly for chronic and lifestyle-related diseases. Simultaneously, conservation strategies must be implemented to ensure the sustainable use of medicinal plant resources and the protection of biodiversity.
Methods and Materials
Study Area
This study was conducted in Westlands Constituency, Nairobi, Kenya (Figure 3). Westlands is situated approximately 3.2 km northwest of Nairobi's Central Business District (CBD) and falls within the geographic coordinates 01°16'01.0"S, 36°48'42.0"E (Latitude: −1.266944; Longitude: 36.811667). The area covers a total of 72.4 km² and is characterized by an elevation of 1800–1850 meters above sea level. The constituency is intersected by Nairobi River and Mathare River and contains sections of the native Karura Forest. The region hosts a diverse population, including a significant proportion of Kenyan Asians. Additionally, Westlands comprises high-income residential zones as well as informal settlements such as Kangemi. The area is also renowned for its commercial hubs, entertainment centers, shopping plazas, restaurants, and nightclubs, contributing to its vibrant social and economic landscape.

Map of Study Area (Source: https://www.google.com/search).
Study Design, Population, and Sampling
This study employed an exploratory qualitative descriptive design to systematically document the use of medicinal plants within the community. The study population comprised residents of Westlands, Nairobi, with the findings intended to provide insights applicable to this region. The target population included traditional healers, CAM practitioners, family heads, religious leaders, community elders, and other individuals possessing specialized knowledge of medicinal plants.
To ensure the inclusion of individuals with relevant ethnobotanical expertise, a non-probability sampling approach was adopted, incorporating snowball and purposive sampling techniques. These methods were selected as random sampling would not have guaranteed the participation of individuals with the required knowledge of medicinal plant use. Purposive sampling is a well-established method in ethnobotanical research, particularly in preliminary studies, skill-specific participant selection, cultural comparisons, case studies, and studies involving small, specialized populations. Given that only key informants with extensive experience in traditional medicine were included, purposive sampling was deemed the most suitable technique. Data collection proceeded until saturation was reached, defined as the point at which no new information or themes emerged. Previous ethnobotanical research suggests that a minimum of twelve participants is generally sufficient for studies employing this design.27,28
The eligibility criteria required participants to be adults aged 18 years and above, including traditional healers, CAM practitioners, family heads, religious leaders, and community elders actively involved in or knowledgeable about traditional medicine within Westlands. Individuals residing outside Westlands or lacking expertise in medicinal plant use were excluded from participation to maintain the study's focus on relevant ethnobotanical knowledge.
Research Procedures
A pilot study was conducted to gain a preliminary understanding of the research area and refine data collection methodologies. This phase involved selecting study sites, administering questionnaires to a subset of participants for feedback, and fine-tuning the interview and discussion guides. The insights gained from the pilot study enhanced the efficiency and reliability of data collection instruments. Data collection was conducted between April and June 2021, through semi-structured interviews and focus group discussions (FGDs) with key informants. Participants were first introduced to the study through informal discussions to establish rapport, followed by a detailed explanation of the research objectives, data usage, and confidentiality measures. Participants retained the right to decline answering any questions at any stage of the study.
Plant Sample Collection and Identification
Plant specimens were collected and systematically examined to ensure accurate identification. Each specimen, including leaves, bark, stems, roots, and other plant parts, was carefully documented with key details such as local plant name, habitat, and morphological characteristics. The collected specimens were then analyzed by an experienced taxonomist, who conducted a detailed classification to verify their botanical identity. Following this examination, voucher specimens were prepared, assigned unique identification numbers, and deposited in the USIU-Africa herbarium for future reference and scientific study.
Study Registration
This study was an exploratory ethnobotanical field survey and was not prospectively registered on an open science platform such as the Open Science Framework (OSF).
Quantitative Ethnobotanical Methods
To systematically assess medicinal plant knowledge in Westlands Subcounty, Nairobi, the study employed various quantitative ethnobotanical indices as described by Du et al, (2022); Ghanimi et al, (2022) and Leonti, (2022), including:
Informant Consensus Factor (ICF): Measures agreement among informants regarding plant use for specific disease categories, calculated as: ICF = (Nur−Nt)/(Nur−1) where Nur is the total number of use reports for a particular category, and Nt is the number of species used for that category. Use Value (UV): This index evaluates the relative importance of plant species based on their frequency of citation by informants. The formula is: UV=∑U/N where U is the number of uses reported for a species, and N is the total number of informants. Relative Frequency of Citation (RFC): This measures the prominence of a plant in local knowledge, calculated as: RFC = FC/N where FC is the number of informants mentioning a species, and N is the total number of informants. Relative Importance Index (RI): This assesses the overall medicinal relevance of a plant species, integrating its frequency of citation and number of use categories. RI = (RFC + RNUs)/2 where RNUs is the relative number of use categories over the maximum. Jaccard Index (JI): This compares ethnomedicinal data between different studies to identify shared traditional knowledge. It is given by: JI = (c × 100)/(a + b−c) where a and b are the total species recorded in two studies, and c is the number of shared species.
Data Analysis Methods
All collected data were thoroughly reviewed for completeness, accuracy, and internal consistency.
Ethnobotanical data were analyzed using descriptive statistical methods articulated in Tardío and Pardo-De-Santayana 29 which included frequency distributions and percentages, to summarize participant responses and usage patterns. In addition, various quantitative ethnobotanical indices were applied to systematically assess and interpret the significance of medicinal plant knowledge within the study area, following established methodologies and analytical protocols.
Footnotes
Acknowledgements
The authors would like to extend their gratitude to the United States International University- Africa for their support toward the successful completion of the research work.
Ethical Considerations
Ethical approval for this study was obtained from the United States International University-Africa Institutional Review Board (USIU-A IRB), located in Nairobi, Kenya. The study was reviewed and approved under protocol number USIU-A/IRB/088-2021 on 25th March 2021.
Author Contributions
All authors participated equally in the conceptualization, investigation and write up of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available by request from the author.
Statement of Informed Consent
Written informed consent was obtained from the participants of the study for their anonymized information to be published in this article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the United States International University, Institutional Review Board (IRB), approval number USIU-A/IRB/088-2021 approved protocols.