
Abstract
Catha edulis, commonly known as “Khat,” is a large shrub that is native to the Arabian Peninsula (particularly Yemen) and some African countries, including Ethiopia, Kenya, and Somalia, and the plant is used traditionally for its psychostimulant, euphoric, and analgesic properties. C. edulis contains several pharmacologically active compounds, but cathinone is responsible for the vast majority of its pharmacological properties. Traditionally, Khat is known for the treatment of type 2 diabetes in Africa, particularly in Uganda. Numerous studies that explored this area yielded inconclusive findings. Some studies showed that chewing Khat lowers blood glucose levels (BGL) in non-diabetic patients, while others showed that ingesting Khat delays gastric emptying time, and this supported and explained the earlier claim of its benefit in Type 2 diabetes mellitus (DM). However, a recent meta-analysis gave a contradictory submission that Khat is associated with an insignificant reduction in BGLs in non-diabetic humans and animals with a significant increase in BGLs in patients with diabetes. Most importantly, reports suggested that Khat exacerbates common complications of diabetes, such as depression, sexual dysfunction, dyslipidemia, proteinuria, and hypertension. The current findings concluded that Khat does not have a beneficial effect on Type 2 DM. Chewing Khat is believed to be a risk factor for Type 2 DM for raising glucose levels and a possible determinant of its poor outcomes and prognosis.
Introduction
Catha edulis (Vahl) Endl., colloquially referred to as “Khat,” is a large shrub (Figure 1) native to the Arabian Peninsula (particularly Yemen) as well as some African countries, including Ethiopia, Kenya, and Somalia. People have traditionally used Khat for its psychostimulant, euphoric, and analgesic properties.1,2 Its young buds and tender leaves are chewed to attain a state of euphoria and stimulation. 3 Chewing sessions can last between three and seven hours, and approximately ten million people worldwide chew Khat leaves daily.

Catha edulis (Vahl) Endl. plant (https://powo.science.kew.org/taxon/urn:lsid:ipni.org:names:941530-1).
Khat comprises several pharmacologically active compounds such as phenylalkylamines, cathedulines, and alpha-aminopropiophenones which when chewed are released into the body together with other active components. 1 Despite the presence of several active compounds in Khat, cathinone (Figure 2a) is primarily responsible for its pharmacological properties. Cathinone is a relatively unstable alkaloid that is rapidly metabolized in the body into norpseudoephedrine (cathine [Figure 2b]), conferring on it an amphetamine-like effect. 4

Chemical structure of cathinone (a) and its derivative cathine (b) found in C. edulis (Vahl) Endl.
Cathinone is released within 15–45 min of chewing Khat, and the plasma peak level of cathinone is reached 1.5–3.5 h thereafter. This compound is bio-available in plasma for up to 24 h of Khat consumption and produces euphoric, psychostimulant, and analgesic effects. 5
Several studies across the globe have reported that Khat-chewing is detrimental to health. The main adverse effects of Khat include those on the gastrointestinal system and central nervous system, but it also affects the cardiovascular, respiratory, endocrine, and genito-urinary systems. The effects on the central nervous system resemble those of amphetamine, but the differences are quantitative. The main toxic effects include increased blood pressure, tachycardia, insomnia, anorexia, constipation, general malaise, irritability, migraines, and impaired sexual potency in men.2,6,7 The withdrawal effects are mild and include depression, anxiety, and nightmares. 6
In this narrative review, any study published in English language that presented any data related to Khat, C. edulis, or any known components of C. edulis concerning its effect on blood glucose or DM was included. Also included was any study of the adverse effects of Khat on humans. All types of articles, including experimental studies, clinical trials, observational studies, and reviews were also included while studies with grossly flawed methods, or unsupported conclusions were excluded.
Type 2 Diabetes Mellitus (Type 2 DM)
Diabetes mellitus (DM) is a collective term for a group of chronic metabolic disorders characterized by hyperglycemia. Type 1 and Type 2 DM are the two most common types. Type 1 DM is characterized by a complete lack of insulin as a result of autoimmune cell destruction. It is most frequently diagnosed before the age of 30, but it can occur at any age. Type 2 DM, on the other hand, is a slow and progressive disease that is caused by a combination of insulin deficiency, insulin resistance, and other hormonal abnormalities, most notably those involving glucagon. Hyperglycemia can result in long-term microvascular and neuropathic complications. 8
Around 422 million people worldwide have been diagnosed with DM, with the majority living in low and middle-income countries. Type 2 DM accounts for approximately 90% to 95% of all diagnosed cases of diabetes. Yearly, it is estimated that approximately 1.6 million mortalities are directly attributed to DM. 9
The risk factors of type 2 DM are presented in Table 1 below 8 ;
Risk Factors of Type 2 Diabetes Mellitus.
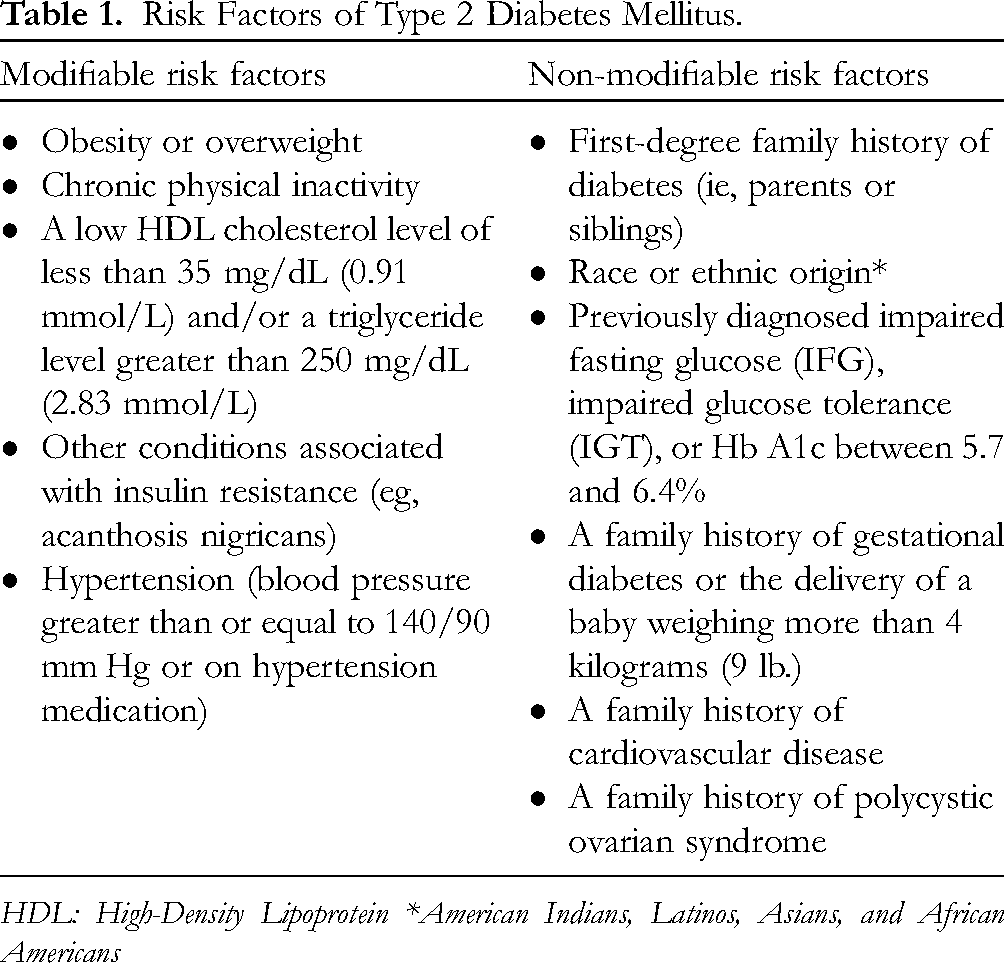
HDL: High-Density Lipoprotein *American Indians, Latinos, Asians, and African Americans
The diagnosis of diabetes mellitus is based on glycemic outcomes exceeding threshold values with one of three testing options (Table 2). A subsequent day must be used to confirm abnormal values unless unequivocal symptoms of hyperglycemia, such as polydipsia, polyuria, or polyphagia, exist. Hb A1c, fasting plasma glucose (FPG), and oral glucose tolerance tests are all acceptable methods for detecting DM. 10
American Diabetes Association (ADA) Criteria for Diagnosis of DM. 10

Hg A1c, hemoglobin A1c; DCCT, Diabetes Control and Complications Trial; FPG, fasting plasma glucose; Hgb, hemoglobin; NGSP, National Glycohemoglobin Standardization Program
Type 2 DM is managed both non-pharmacologically (without antidiabetic drugs) and pharmacologically (with antidiabetic drugs). Nonpharmacological management entails adhering to appropriate medical nutrition therapy, controlling weight, engaging in regular physical activity, receiving psychological assessment and care, and receiving influenza and pneumonia vaccinations on time. Pharmacological agents used in the treatment of Type 2 DM include biguanides (metformin), sulfonylureas, non-sulfonylurea secretagogues (glinides), thiazolidinediones, alpha-glucosidase inhibitors, dipeptidyl peptidase-4 inhibitors (gliptins), selective sodium-dependent glucose cotransporter-2 (SGLT-2) inhibitors central-acting dopamine agonists, bile acid sequestrants, and insulin. 8
Proposed Mechanism of Action of Catha edulis (Vahl) Endl
Figure 3 below presents the mechanisms of action of C. edulis. Cathinone, the primary active ingredient in Khat, is structurally similar to nor-ephedrine and acts similarly to amphetamine; thus, it stimulates catecholamine release from presynaptic nerve terminals. Catecholamines activate β-adrenergic receptors, increasing adrenocorticotropic hormone and serum cortisol levels while inhibiting insulin release via pancreatic alpha–2–adrenoceptor activation. 5
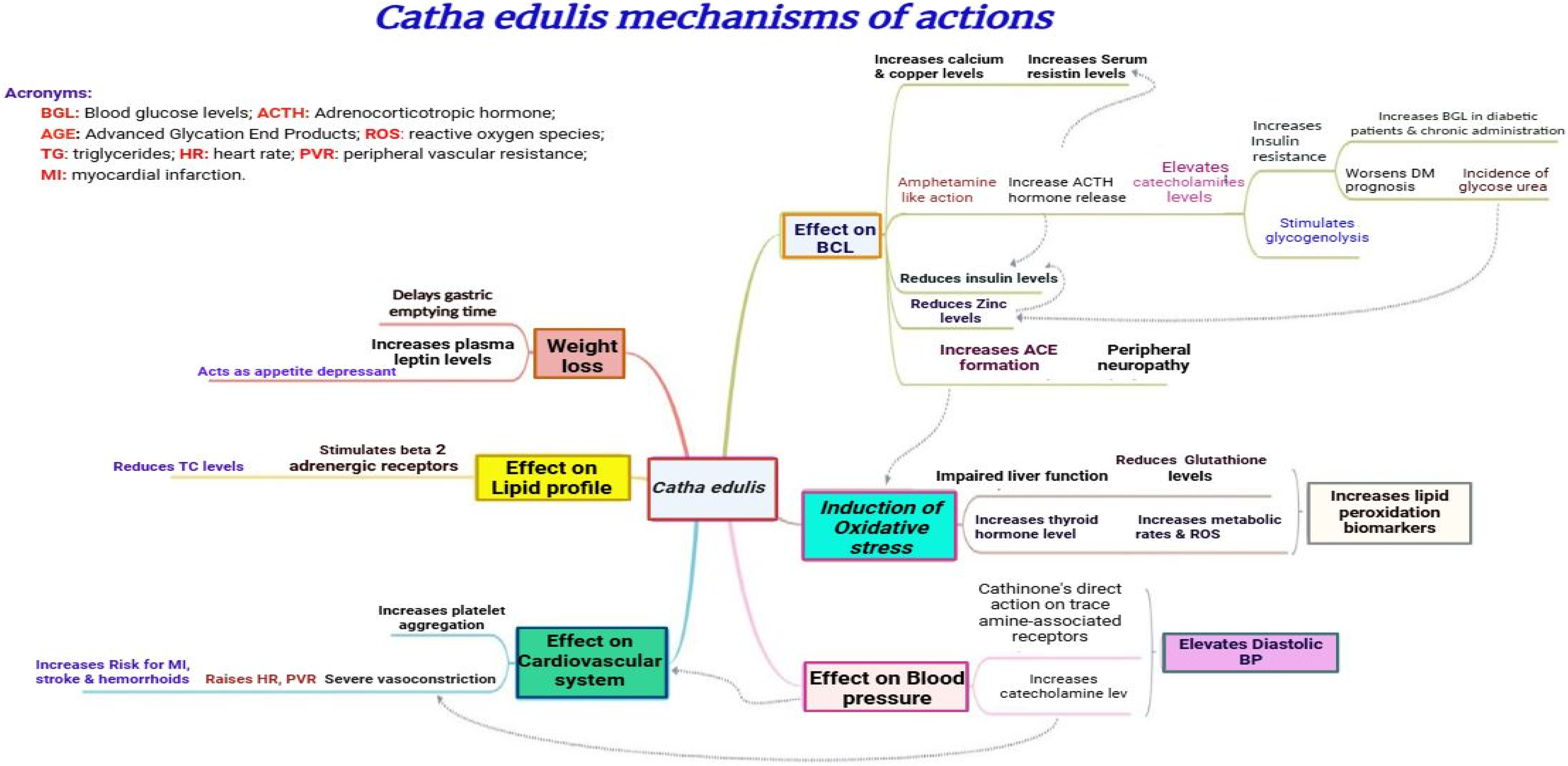
Catha edulis (Vahl) Endl. Mechanisms of Action. ACTH, adrenocorticotropic hormone; AGE, advanced glycation end products; BGL, blood glucose levels; HR, heart rate; MI, myocardial infarction; PVR, peripheral vascular resistance; ROS, reactive oxygen species; TG, triglyceride. 1
When cortisol levels rise, insulin secretion drops and insulin resistance develops. This happens because the resistin gene expression goes up, which causes serum resistin levels to rise. Resistin is involved in the development of insulin resistance in the liver and skeletal muscle, impairing insulin signaling and/or glucose metabolism. 5 Cathinone-induced catecholamine secretion also results in an increase in BGL through the activation of glycogenolysis in skeletal muscles and the liver via the β2-adrenoceptor-mediated response. 11
Serum zinc levels reduces when C. edulis is chewed and this can have several effects on diabetes since zinc helps to make insulin hexamers and protects the sulfhydryl groups on proteins and enzymes. Fibers, tannins, and calcium in Khat inhibit intestinal zinc absorption while increasing intestinal zinc excretion. Zinc deficiency may result in insulin resistance, as the hexamer conformation of insulin is unable to form, resulting in immature and/or inactive insulin. Hyperglycemia and Khat chewing both increase the level of oxidative free radicals and reduce the effectiveness of antioxidant defense systems, including zinc, implying that Khat chewing contributes to zinc consumption. 5
Among healthy and diabetic chewers, Khat chewing has resulted to a significant increase in serum calcium levels leading to an increase in cytosolic calcium levels that reduces cellular insulin sensitivity and may contribute to the pathogenesis of Type 2 DM insulin resistance. 5 The resistin levels significantly correlate with calcium levels, and an increase in resistin levels raises cytosolic calcium levels in hepatic stellate cells. 12 Additionally, independent of parathyroid hormone, another study reported a positive correlation between serum calcium and FPG and insulin resistance in male patients with type 2 DM. 13
Chewing Khat leaves also elevates the serum copper level and copper acts as a pro-oxidant that may contribute to the formation of free radicals via metal catalysis. Copper and zinc are critical components of the oxidant/antioxidant mechanism; an imbalance results in increased susceptibility to oxidative tissue damage, which ultimately leads to the development of diabetes mellitus or diabetic complications. Additionally, researchers hypothesized that glycated proteins bind transition metals like copper and iron, significantly contributing to the etiology of peripheral vascular dysfunction and peripheral neuropathies in type 2 diabetes. 5
Wabe, 2 reported adverse effects of Khat in human cardiovascular, gastro-intestinal, respiratory and other systems and listed tachycardia, palpitations, hypertension, arrhythmias, tachycardia, palpitations, hypertension, arrhythmias, vasoconstriction, myocardial infarction, cerebral hemorrhage, pulmonary edema vasoconstriction, myocardial infarction, cerebral hemorrhage, dry mouth, polydipsia, dental caries, periodontal disease, chronic gastritis, constipation, hemorrhoids, paralytic ileus, weight loss, duodenal ulcer, hyperthermia, perspiration, hyperglycemia, upper gastro-intestinal malignancy pulmonary edema as major problems encountered in the intake of Khat.
Association Between C. edulis (Vahl) Endl. Use and Type 2 DM
Perceived Role of C. edulis (Vahl) Endl. in Treatment of Type 2 DM
Many compounds have been reported in Khat, including alkaloids, terpenoids, flavonoids, sterols, glycosides, tannins, amino acids, vitamins, and minerals. The major pharmacologic and toxic effects come from the phenylalkylamines and the cathedulins. 2 Traditionally, it was believed that Khat had a beneficial effect on type 2 diabetes and decreased BGLs. 14 Numerous studies have been conducted on the aforementioned subject, with inconsistent results. 1 A study showed a significant reduction in glucose and triglycerides concentration within six months in animals, 15 likewise, Taleb and Bechync 16 demonstrated that chewing Khat leaves significantly lowers BGLs in healthy non-diabetic patients: 61.22% decrease in BGLs within four hours of Khat consumption. 16 Heymann et al 17 in his study reported that chewing Khat leaves for two hours significantly prolonged the gastric emptying time of a semi-solid meal (half times ranging from 37 to 293 min), and this study supported the earlier finding that Khat is beneficial for type 2 diabetes. However, this study did not directly investigate Khat's hypoglycemic effect. 17
Catha edulis (Vahl) Endl. and Risk of Type 2 DM
Saif-Ali et al 18 demonstrated that chronic Khat chewing has no effect on serum glucose and C-peptide levels in healthy non-diabetic individuals, but increases both serum glucose and C-peptide levels in Type 2 DM patients, particularly in those with serum glucose between 200 and 450 mg/dl at 2 h post-meal. 18 Mohammed and Hatem reported that chewing Khat leaves increases resistin, cortisol, fasting blood glucose, plasma blood glucose, Homeostatic Model Assessment-Insulin Resistance (HOMA-IR), calcium, and copper serum levels in diabetics and non-diabetic Khat chewers. However, these metabolic effects were greater in diabetics than in non-diabetic Khat chewers. On the other hand, diabetic Khat chewers had significantly lower serum zinc and insulin levels than diabetic non-Khat chewers. Thus, this study established a strong correlation between chronic Khat use and worsening in type 2 diabetes, owing to increased insulin resistance caused by elevated resistin levels and cathinone-induced catecholamine secretion, resulting in increased blood glucose, HOMA-IR, cortisol, copper, and calcium levels, and decreased zinc and insulin levels. 5
According to a study conducted by Al-Sharafi and Gunaid 14 among Type 2 DM patients attending an endocrinology clinic in Sana'a, Yemen, they reported that patients who chewed Khat had a mean HbA1c of 9.8% (95% confidence interval [CI] 9.6-10), compared to those who did not chew Khat, who had a mean HbA1c of 9.1% (95% CI 8.9-9.4). Additionally, the study discovered that Khat chewers were younger at the time of type 2 diabetes diagnosis, with a mean age of 43.3 years, compared to non-Khat chewers, who had a mean age of 45.9 years at the time of DM diagnosis. 14
A recent meta-analysis of scientific studies on the glycemic effect of Catha edulis (Vahl) Endl. showed that the majority of studies indicated that C. edulis has a mild hypoglycemic effect. However, the reduction in blood glucose was not statistically significant (Mean Difference (MD)=−9.70, 95% CI: −22.17 to 2.76, P value = 0.13), and high heterogeneity between subgroups (I2 = 88.2%, P value < 0.0001). The pooled MD in BGLs between non-diabetic animals, diabetic animals, and non-diabetic humans revealed a non-significant decrease in BGLs (MD = −18.55, 95% CI: −39.55 to 2.50, P < 0.08, MD = −52.13%, 95% CI: −108.24 to 3.99, P = 0.07 and MD = −2.71%, 95% CI: −19.19 to −13.77, P = 0.75) respectively. In diabetic humans, however, a significant increase in the pooled mean difference of blood glucose was observed (MD = 67.18, 95% CI: 36.93-−97.43, P < 0.0001). 19 Therefore, the meta-analysis indicated a non-significant reduction in BGLs among non-diabetic and diabetic animals as well as in non-diabetic humans. However, a significant increase in BGLs was observed in diabetic humans. Additionally, demographic and epidemiological reports suggested that chewing C. edulis could be a risk factor for developing type 2 DM. 19
Badedi et al 20 established an association between Khat chewing and the development of Type 2 DM in a cross-sectional analytical study involving randomly selected participants from primary healthcare centers in Jazan and concluded that Khat users had a more than threefold increased risk of developing Type 2 DM compared to non-users. However, no correlation was found between Khat chewing and glycemic control in type 2 DM 20
Moreover, another study conducted in Yemen showed that Khat chewing by type-2 DM patients significantly increases proteinuria and hastens the progression of renal nephropathy. 21 Additionally, Khat chewing is associated with a transient increase in systolic and diastolic blood pressure, a transient increase in heart rate, 22 and dyslipidemia. 23 A recent study in Somaliland showed the association of Khat chewing with mental disorders 24 which is an important issue since depression is one of the common complications in type-2 DM patients. In one study, 42.9% of type-2 DM patients tested positive for one or more mental disorders, and 25.6% had depression. 25 Comparably, in Ethiopia, hypertensive patients who chewed Khat had significantly lower self-care practices than those who did not chew Khat. 26 This negative effect of Khat chewing on self-care practice might worsen glycemic control in type 2 DM patients and contribute to diabetes-related complications.
Erectile dysfunction (ED) has a prevalence of 52.5% in diabetic male patients, as described in a meta-analysis of 145 studies that included 88,577 men with type 1 and type 2 diabetes. 27 In human studies, chronic users of Khat had dramatically lower semen volume, sperm motility, and count, as well as reduced libido or erectile dysfunction (ED) and this suggested that Khat can have serious implications for male fertility and sexual health.28,29 Given sexual dysfunction being one of the most common complications of diabetes, the sexual adverse effects of C. edulis may be devastating, hence, Khat chewing should be avoided by all diabetic patients, particularly, those with impotency or suspected infertility.
A more recent review also concluded that after Khat consumption, in addition to its direct appetite suppressant effects, cathinone acts centrally on the hypothalamus, causing delays in gastric emptying. The review also showed that long-term users of Khat usually develop complications, such as acute and chronic liver disease, fibrosis, and cirrhosis. 7
Lastly, the in vitro report suggested that C edulis extract has the potential to affect CYP3A4 activity at high doses. The combination treatment showed a significant increase in metformin's blood sugar-lowering effects, potentially resulting in hypoglycemia. 30 In summary, Khat chewing has been conclusively shown to increase the risk of getting type 2 DM at a younger age, significantly increase BGLs in type 2 DM patients, and has been shown to contribute to the occurrence or/and worsening of numerous adverse effects that are particularly common in type 2 DM patients: increased blood pressure, dyslipidaemia, erectile dysfunction, mental illness, and gastrointestinal disorders.
Catha edulis (Vahl) Endl. in Diabetic Wound Healing
On the other hand, a recent preclinical study suggested that Catha edulis extract-loaded scaffolds were nanofibrous, antioxidative, and non-toxic to skin cells. An in vivo study demonstrated that the stem cell and C. edulis extract-loaded scaffolds had the highest rate of wound closure and histomorphometric parameters compared to other treatment groups. Moreover, gene expression studies showed that the developed wound dressings increased the expression of the vascular endothelial growth factor (VEGF) gene and reduced the expression of the glutathione peroxidase gene. 31 Moreover, several in vitro studies of C. edulis extracts have shown significant antibacterial activities in some species; and this may contribute to its wound healing effects. 15 The use of C. edulis extract-loaded scaffolds is thought to be minimally absorbed into the systemic circulation and cause little adverse effects in type 2 DM patients. However, the human in vivo studies on this has to be considered in the future.
Limitations
Being a narrative review, this article presented what is considered relevant for the topic and the aim of the review, but without a specified methodological plan for a systematic review. One potential bias in this review was the use of the findings reported by the majority of the studies to reach conclusions whereas the minority of studies with different findings were presented but not considered while concluding. The other bias noted was that the positive effects of Khat chewing impacting or affecting BGLs in non-diabetic patients and animals were not considered because the primary objective of the current review was to address the effects of Khat chewing in patients with type 2 DM. Accordingly, the authors reached conclusions by focusing solely on the findings of studies that reported the effect of Khat chewing in patients with type 2 DM. On the other hand, the contradictory effects of Khat chewing in animals and non-diabetic individuals should be studied by rigorous systematic reviews and meta-analyses.
Conclusion
The effect of Khat on BGLs in non-diabetic persons and animals is largely inconclusive. On the other hand, multiple studies conclusively and independently showed that Khat chewing significantly increased BGLs, and this scenario can worsen glycemic control in patients with type 2 DM. Similarly, the studies conclusively showed chewing Khat induces or deteriorates many complications that are known to be common among patients with type 2 DM. Lastly, no beneficial effects of Khat chewing were reported by clinical studies involving type 2 DM patients and this could be associated with the increase in BGL that could trigger the type 2 DM.
Therefore, patients with type 2 DM and individuals at a high risk of having type 2 DM should be counseled to avoid chewing C. edulis. This intervention should be integrated with the comprehensive care of patients with type 2 DM, particularly in areas with a high prevalence of C. edulis use. Moreover, to reach conclusions on the effect of Khat chewing in non-diabetic patients, randomized controlled trials, rigorous systematic reviews, and meta-analyses of the previous studies are recommended to be conducted in future studies.
Footnotes
Abbreviations:
Acknowledgments
The authors would like to thank Mbarara University of Science and Technology for facilitating access to the digital library while compiling this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.