
Abstract
Bacterial resistance to antibiotics continues to be a grave threat to human health. Because antibiotics are no longer a lucrative market for pharmaceutical companies, the development of new antibiotics has slowed to a crawl. The World Health Organization reported that the 8 new bacterial agents approved since July 2017 had limited clinical benefits. While a cohort of biopharmaceutical companies recently announced plans to develop 2-4 new antibiotics by 2030, we needn’t wait a decade to find innovative antibiotic candidates. Essential oils (EOs) have long been known as antibacterial agents with wide-ranging arsenals. Many are able to penetrate the bacterial membrane and may also be effective against bacterial defenses such as biofilms, efflux pumps, and quorum sensing. EOs have been documented to fight drug-resistant bacteria alone and/or combined with antibiotics. This review will summarize research showing the significant role of EOs as nonconventional regimens against the worldwide spread of antibiotic-resistant pathogens. The authors conducted a 4-year search of the US National Library of Medicine (PubMed) for relevant EO studies against methicillin-resistant Staphylococcus aureus, multidrug-resistant (MDR) Escherichia coli, EO combinations/synergy with antibiotics, against MDR fungal infections, showing the ability to permeate bacterial membranes, and against the bacterial defenses listed above. EOs are readily available and are a needed addition to the arsenal against resistant pathogens.
Keywords
The antibiotic era began in 1941 with the welcomed release of penicillin. However, Alexander Fleming, who discovered penicillin, warned that microbes are educated to resist penicillin. The Centers for Disease Control and Prevention (CDC) reported that bacterial resistance to penicillin developed just 1 year later in 1942. Antibacterial resistance has continued to evolve, assisted by the overuse of antibiotics in humans, and antibiotics used to increase food animal growth in factory farming. Ultimately, 2015 brought news that Pan-resistance to antibiotics used for Gram-negative bacteria had arrived with colistin resistance that developed in China.
Researchers from Chinese, British, and US universities published in Lancet Infectious Diseases their discovery of a new form of resistance to the antibiotic of last resort, colistin. The initial colistin resistance gene is called mcr-1. 1 Since this resistance presumably came from massive agricultural use of colistin in China, National Geographic headlined the news story “Apocalypse Pig.” 2 Before ending its use of colistin in animals at the end of April 2017, China had been using more than 8000 metric tons of colistin per year. By 2019, there were 9 mobilized mcr genes identified (mcr-1-mcr-9).
The German Center for Infection Research reported on the plasmid-mediated colistin resistance mechanism mcr-1 in an article entitled “Dangerous and ‘jumping’ mcr-1 resistance gene.” In studying the transferability of the easily transferred gene, they stated that the “mcr-1 gene not only exists on mobile plasmids, but [can] be integrated into chromosomes as well. Consequently, it can be reliably passed on to next generations.” 3
The “jumping” plasmid mcr-1 indeed jumped. Klebsiella pneumoniae, Shigella flexneri, Acinetobacter baumannii, Escherichia coli, and Pseudomonas aeruginosa are also now resistant to all known antibiotics.
Research from the ensuing years has not been encouraging. While human-to-human spread of colistin resistance is to be expected, research has shown that even our waters are now carriers. Plasmid-mediated colistin-resistant ESBL-producing E. coli was retrieved from seawater at a public beach in Norway. According to the study, “This report illustrates that E. coli strains containing plasmid-mediated colistin resistance genes have also reached areas where this drug is hardly used at all. Surveillance of colistin resistance in environmental, veterinary, and human strains is warranted also in countries where colistin resistance is rare in clinical settings.” 4 A colistin-resistant ESBL-producing Enterobacteriaceae was isolated from river water and imported vegetable samples in Switzerland. 5 Sewage in Barcelona, Spain, carried mcr-1 Enterobacteriaceae. 6 Colistin-resistant mcr-1 E. coli was found on 2 Brazilian beaches, including Santos, the major beachfront city of the region with the largest shipping terminal in Latin America. 7 The colistin resistance gene was found in 18 different locations on the Haihe River in China. 8 ESBL, KPC-type, and mcr-1.2-producing Enterobacteriaceae contaminated wells, river water, and wastewater treatment plants in Northern Italy, 9 while a pan-drug-resistant isolate of A. baumannii was recovered in municipal waste water in Zagreb, Croatia. 10 Finally, we note a September 2019 study published in Infection Control & Hospital Epidemiology. Henig et al report using real-time polymerase chain reaction to identify 4 patients with the mobile colistin resistance mcr-1 gene in a hospital in Michigan. 11
With extensive drug resistance and pan resistance now worldwide, microbial transfer has taken on fearful new capabilities. A February 2017 study in Nature Microbiology linked flies for the first time to the spread of carbapenem resistance. The researchers reported: “Furthermore, local blaNDM dissemination (flies and dogs) increases… the probability of carriage by migratory birds such as swallows, the migratory winter destinations of which are usually South East Asia (including Cambodia, Vietnam, Laos, Thailand, Malaysia and Indonesia).” 12 A 2018 Sichuan University concurred stating “the movable colistin-resistance gene mcr-1 was detected among the colistin-resistant E. coli strains isolated from the river water and egret feces, which indicated the possibility of the environmental dissemination of this gene.” 13
The Multiple Mechanisms of Essential Oils
Schnaubelt discussed the antibacterial efficacy of essential oils (EOs): “Unlike antibiotics, which are active due to inhibiting an easily identifiable single target, the activity of EOs, impairing a bacterium in multiple physiological systems as well as in membrane functionality, is only now understood.” 14
A 2019 study lists some of the antibacterial pathways of EOs: “The most frequently reported mechanism of antibacterial action of both isomers [carvacrol and thymol] involves the disruption of bacterial membrane leading to bacterial lysis and leakage of intracellular contents… Other proposed mechanisms of antibacterial action include the inhibition of efflux pumps, prevention in the formation and disruption of preformed biofilms, inhibition of bacterial motility, and inhibition of membrane ATPases.” 15
A lesser-known aspect of EOs is while powerful against pathogenic bacteria, some studies suggest they have little effect on beneficial bacteria. An abstract presented at the Experimental Biology 2019 meeting reported: “Using cinnamon essential oil as an antibiotic alternative has shown to be a promising option with limited detrimental effects against the commensal bacteria.” Lead author Victoria R. Adams said further evaluation was needed to determine the benefits of utilizing a natural alternative. 16
A 2009 study showed “Carum carvi [caraway], Lavandula angustifolia Mill. [lavender], Trachysperum copticum [ajowan], and Citrus aurantium var. amara [neroli] essential oils displayed the greatest degree of selectivity, inhibiting the growth of potential pathogens at concentrations that had no effect on the beneficial bacteria examined.” 17 Si et al reported, “Thymol, cinnamon oil and carvacrol have previously demonstrated a broad spectrum of antimicrobial activities… Our results not only confirmed the activity of these compounds against E. coli and Salmonella, but also demonstrated their selectivity towards the pathogens with little effect on the beneficial gut bacteria.” 18 Also, a 2015 study in Microbiology reported that “thymol and geraniol at around 100 ppm could be effective in suppressing pathogens in the small intestine, with no concern for beneficial commensal colonic bacteria in the distal gut.” 19
Abreu et al explain that “plants, rather than relying on single metabolites, use a combination of strategies and a highly efficient defense system that includes very diverse molecules ranging from proteins to H2O2 and oxygen radicals, which most likely complement each other, to deal with microbial threats. The defense strategies may thus involve the synergistic activity of 2 or more compounds, which could act via different mechanisms and/or targets… It is important to bear in mind that millions of years of evolution have resulted in plant defense systems that have proved to be not readily susceptible to microbial resistance mechanisms.” 20
EOs Against Methicillin-Resistant Staphylococcus aureus
A 2019 case study and literature review in Therapeutic Advances in Infectious Disease reported that in “2013, the Centers for Disease Control and Prevention (CDC) highlighted methicillin-resistant Staphylococcus aureus (MRSA) as a serious drug-resistant threat citing over 80,000 invasive MRSA infections leading to over 11,000 deaths each year in the United States. MRSA frequently enters the blood stream and metastasizes resulting in endocarditis and osteomyelitis. This represents a major burden on the healthcare system, with 30- and 90-day mortality rates as high as 30% and 50% respectively.” 21 Deaths in the United States from antibiotic-resistant infections are more than 35 000 yearly. 22
In the study mentioned above, Abreu et al identified plant extract compounds that could act as antibiotic adjuvants “showing their great potential for application in the clinical therapy of infections with antibiotic-resistant microorganisms such as MRSA.” 20
A review by Chambers and Deleo noted CA MRSA has characteristics not found in HA MRSA. Tissue-destructive infections that include necrotizing fasciitis and fulminant, necrotizing pneumonia may be a result of CA MRSA genes that encode the virulence factor Panton-Valentine Leukocidin, which induces leukocyte destruction and tissue necrosis. 23 Please see Table 1 for more substantiated data.
EO/Constituent Against MRSA
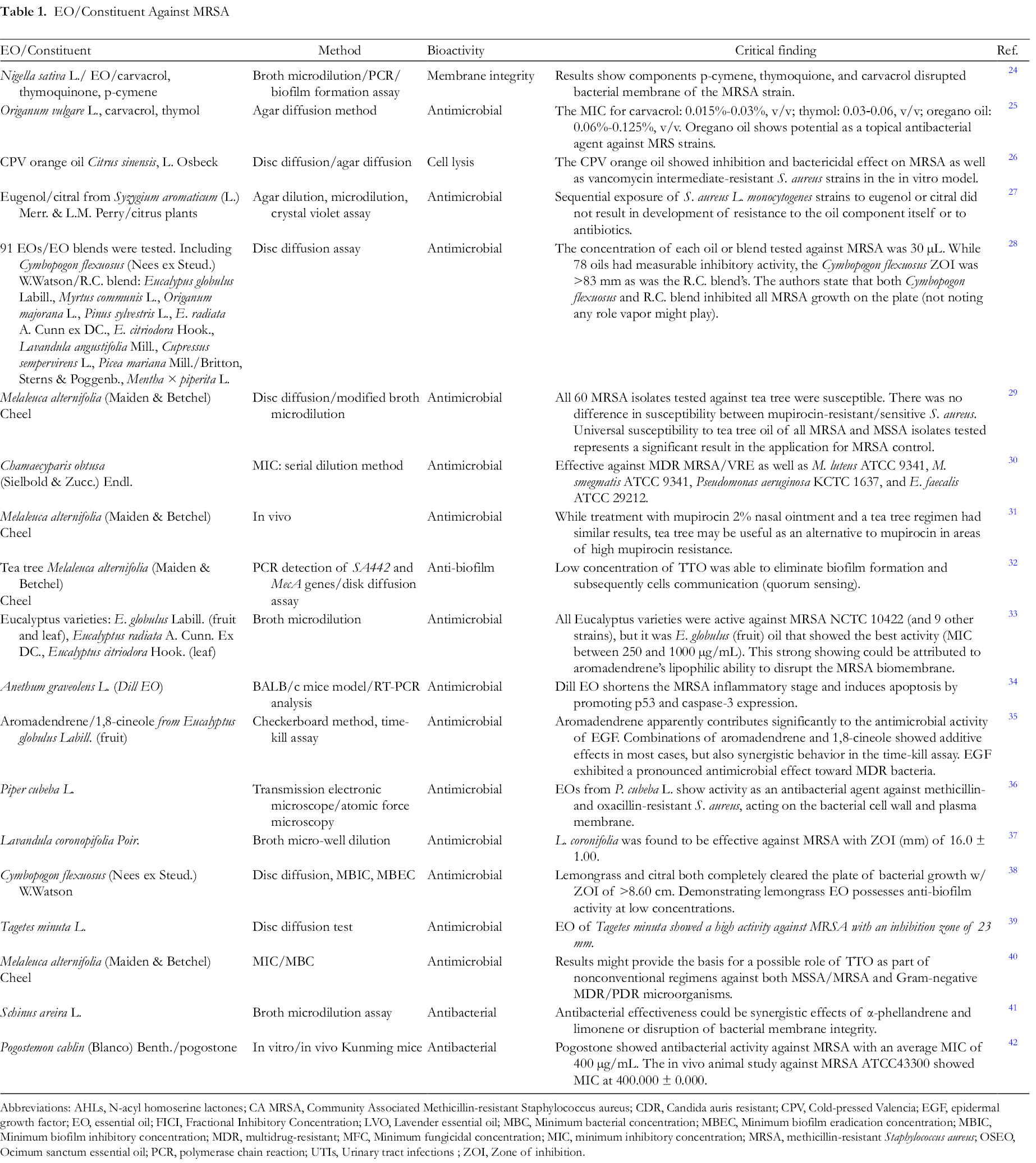
Abbreviations: AHLs, N-acyl homoserine lactones; CA MRSA, Community Associated Methicillin-resistant Staphylococcus aureus; CDR, Candida auris resistant; CPV, Cold-pressed Valencia; EGF, epidermal growth factor; EO, essential oil; FICI, Fractional Inhibitory Concentration; LVO, Lavender essential oil; MBC, Minimum bacterial concentration; MBEC, Minimum biofilm eradication concentration; MBIC, Minimum biofilm inhibitory concentration; MDR, multidrug-resistant; MFC, Minimum fungicidal concentration; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; OSEO, Ocimum sanctum essential oil; PCR, polymerase chain reaction; UTIs, Urinary tract infections ; ZOI, Zone of inhibition.
EO/Antibiotic Additivity & Synergism
Rosato et al reported peppermint EO/gentamicin and ampicillin synergism. The “results against Gram-negative bacteria [such] as K. pneumoniae and Pseudomonas aeruginosa are of particular interest as these bacteria are difficult to treat with commonly employed antibacterial drugs.” 43
The 2016 review by Aelenei et al noted that the intrinsic difference between Gram-positive and the more-difficult-to-kill Gram-negative bacteria is “due to an additional outer membrane acting as an effective barrier for amphipathic agents and over expression of efflux pumps responsible for innate antimicrobial resistance.” The authors concluded that their review “reveals that essential oils and their purified components enhance the efficacy of antibiotics against Gram-negative bacteria, being promising candidates for the development of new effective formulations against Gram-negative bacteria.” 44
In their research against MDR Pseudomonas aeruginosa, I Utchariyakiat et al found “cinnamon bark oil showed the strongest antimicrobial activity against all clinical-isolated MDR-PA strains with MIC of 0.0562 to 0.225% v/v and MBC of 0.1125 to 1.8% v/v.” This study also reported that “cinnamon bark oil and cinnamaldehyde combined with colistin demonstrated synergistic rates at 16.7% and 10%, respectively.” 45 Please see Table 2 for more substantiated data.
EOs Combined With Antimicrobials—Additivity/Synergistic Effects.

Abbreviations: EO, essential oil; FLC, fluconazole; FTIR, Fourier transform infrared; MDR, multidrug-resistant; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; NDM, New Delhi metallo-β-lactamase-1.
Escherichia coli: 2 Devasting Clone-Sequence Types: ST 405 and 1193
Gram-negative E. coli has increased in virulence. In 2016 in New Jersey, 2 mobile genes in E. coli were found to carry the mcr-1 and blaNDM-5 genes conferring resistance to colistin and carbapenems. 46 Co-author in this study, Barry Kreiswirth later stated: “The bad news is that… there are clearly other strains out there we haven’t detected yet. Both the carbapenem resistance and the colistin resistance genes are on separate plasmids, which means in principle they could spread to other bacteria.”
Tchesnokova et al discovered in 2019 a new MDR E. coli affecting younger adults (under age 40) E. coli clonal group, sequence type 1193 emerging in multiple US cities. This MDR-E. coli is 100% resistant to fluoroquinolones, 55% resistant to trimethoprim-sulfamethaoxazole, and 53% resistant to tetracycline. 47 The multipronged effects of EOs may provide a boost to antibiotics that are now ineffective for MDR E. coli. Please see Table 3 for more substantiated data.
EOs Against Escherichia coli and MDR-E. coli.

Abbreviations: EO, essential oil; MDR, multidrug-resistant; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus.
Candida auris: The Deadly MDR Fungi Hospitals Would Not Disclose
April 2017 news reports told of an outbreak of pan-resistant Candida auris in New York, New Jersey, and Illinois. One deadly case was at Northwestern Memorial Hospital in Chicago contracted by a patient from a catheter or intravenous line. It has been reported that nearly half the people who contract this die within 90 days. There was no announcement to the community about the outbreak. 80
This nonaction followed a model of suppression set by Royal Brompton Hospital outside London. Only after the intensive care unit at Royal Brompton was shut down for 50 Candida auris cases did they acknowledge the outbreak. Patients were moved to another floor for 11 days.
A newspaper article told how London hospital workers used a device to spray aerosolized hydrogen peroxide throughout the room of a patient with Candida auris. 81 After a week’s treatment the “settle plate” used to confirm bacterial efficacy showed just 1 organism grew back: Candida auris.
The 2016 European C. auris outbreak was discussed by Schelenz et al who reported, “Despite a comprehensive review of modern technologies for environmental decontamination there is currently no published data in the literature on the effectiveness of cleaning agents or decontamination of the environment for C. auris specifically.” 82
In 2018, China had its first cases of pan-echinocandin-resistant Candida tropicalis and pan-echinocandin-resistant Candida glabrata, which suggests monitoring for antifungal susceptibility trends in all Candida species. 83
We note a 2014 study in Acta Biochem Pol. as just one of many showing antifungal effects of EOs. Budzyńska et al state: “This report includes the results proving the influence of clove oil, geranium oil, lemon balm and citronella oil on possible mechanisms reported to be relevant for Candida pathogenesis, namely germ tube and mycelium formation, adhesive and invasive properties and extracellular production of various enzymes.” 84 Please see Table 4 for more substantiated data.
EOs Against MDR Fungal Infections.

Abbreviations: EO-ACs, essential oil active components; HPLC, high-performance liquid chromatography; MDR, multidrug-resistant; MIC, minimum inhibitory concentration; RT-PCR, reverse transcriptase polymerase chain reaction.
EO Effects on Bacterial Cell Membrane
A 2013 Italian study described EO mechanisms of action against microbes. “Toxic effects on membrane structures and function are generally used to explain the antimicrobial activity of EOs. In fact, the mechanisms of action of the EOs include the degradation of the cell wall, damaging the membrane proteins, increased permeability leading to leakage of the cell contents, reducing the proton motive force, reducing the intracellular ATP pool via decreased ATP synthesis and augmented hydrolysis that is separate from the increased membrane permeability and reducing the membrane potential via increased membrane permeability.” 100 Please see Table 5 for more substantiated data.
EO Effects on Bacterial Cell Membrane.

Abbreviations: EO, essential oil; MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; SEM, scanning electron microscopy.
EO Effect on Biofilms/Efflux Pumps/Quorum Sensing
In 2013, Bjarnsholt reported on the “category of chronic infections caused by bacteria growing in slime-enclosed aggregates known as biofilms. Biofilm infections, such as pneumonia in cystic fibrosis patients, chronic wounds, chronic otitis media and implant- and catheter-associated infections, affect millions of people in the developed world each year and many deaths as a consequence.” 123 Wang et al noted that “The increasing multidrug resistance has become a major threat to the public health. Overexpression of multidrug efflux pumps is one of the major mechanisms of drug resistance in bacteria.” 124 Defoirdt stated: “Many important plant, animal, and human pathogens regulate virulence by quorum sensing, bacterial cell-to-cell communication with small signal molecules.” 125 EOs and their components have multifaceted effects against these powerful bacterial defenses. We recommend the 2019 review “Anti-quorum Sensing and Antimicrobial Effect of Mediterranean Plant Essential Oils Against Phytopathogenic Bacteria” by Camele et al. Please see Table 6 for more substantiated data.
EOs Against Biofilm, Efflux Pump, Quorum Sensing.

Abbreviations: EO, essential oil; EtBr, ethidium bromide; MDR, multidrug-resistant; qPCR, quantitative polymerase chain reaction; SEM, scanning electron microscopy.
MDR and XDR Tuberculosis
It is important to include EO impact on the major health problem, MDR and extensively drug-resistant (XDR) strains of tuberculosis, which affect millions. The US CDC reports that tuberculosis is one of the world’s deadliest diseases with one-fourth of the world’s population infected with it. According to the World Health Organization (WHO): “A total of 1.5 million people died from TB in 2018. Multidrug-resistant TB (MDR-TB) remains a public health crisis and a health security threat. WHO estimates that there were 484,000 new cases with resistance to rifampicin—the most effective first-line drug, of which 785 had MDR-TB.” Of the 10 million individuals who became ill with TB in 2018, approximately three million were “missed” by health systems and do not get the care they need, allowing the disease to continue to be transmitted. 126
The 2018 study by Kazemian et al noted the lengthy treatment time for TB, hepatotoxicity of drugs, and the emergence of multidrug-resistance and extreme-drug-resistant strains. Their research on medicinal plants of the Lamiaceae family showed MDR-TB was completely inhibited by Zataria multiflora Boiss. at 78 µg/mL while Satureja rechingeri and Satureja khuzestianica showed MICs of 156 µg/mL against MDR Mycobacterium tuberculosis. 127
Other EOs showing efficacy in studies against MDR- and XDR-TB are Myrtus communis L. 128 and Nigella damascena. 129
Conclusion
On April 21, 2019, a segment on CBS News asked: “Could Antibiotic-Resistant ‘Super Bugs’ Become a Bigger Killer Than Cancer?” Interviewee Ramanan Laxminarayan, senior research scholar at Princeton University, has tracked the rise of superbugs for nearly 20 years. He discussed what would not be possible without effective antibiotics. “Everything that we think of whether it’s cancer chemotherapy, transplants, hip replacements, knee replacements, colorectal surgery, all of these require effective antibiotics to perform.” 130
What has been the response to the antibiotic-resistance threat? “By 2006, the European Union had banned all nonmedicinal antibiotics in animals… In 2005, the emergence of fluoroquinolone-resistant Campylobacter jejuni in the clinical setting in conjunction with fluoroquinolone administration in animals prompted the FDA to ban fluoroquinolone use in poultry.” 131 The authors of the study just quoted reported that following the avoparin ban in Europe, “the prevalence of VRE in farm animals rapidly declined… However, this did not translate directly to a decrease of VRE in humans.”
A systematic review and meta-analysis on reducing antibiotic use in food-producing animals was published in Lancet Planet Health in November 2017. The Lancet study concluded:
Interventions that restrict antibiotic use in food-producing animals are associated with a reduction in the presence of antibiotic-resistant bacteria in these animals. A smaller body of evidence suggests a similar association in the studied human populations, particularly those with direct exposure to food-producing animals. The implications for the general human population are less clear, given the low number of studies. The overall findings have directly informed the development of WHO guidelines on the use of antibiotics in food-producing animals. 132
Acting on causes of antibiotic resistance is certainly a part of solving this bacterial crisis. But foremost is research for deterrents. The synchronicity of EOs and antibiotics has been reported by Owen and Laird “as a potential solution to antibiotic resistance.” They note, however, that “a lack of consistency in methods and interpretation criteria makes drawing conclusions of efficacy of studied combinations difficult.” 133 The multipronged effects of EOs on resistant microorganisms must be added to the antibacterial arsenal. With a paucity of new antibiotics in the pipeline, the call is now urgent for more and better designed EO/antibiotic synergy research.
Lahmar et al documented the often-surprising power of combining an EO with an antibiotic:
In the interactive experiment essential oils were found highly effective in reducing the resistance of Methicillin-resistant Staphylococcus aureus to amoxicillin, tetracycline, piperacillin, ofloxacin and oxacillin and resistance of Acinetobacter baumannii to amoxicillin and of ofloxacin in interactive manner. Furthermore, the results proved synergism among essential oils and both antibiotics ofloxacin and novobiocin against the Extended-Spectrum Beta-Lactamase producing E. coli (ESBL). 134
We close by recommending the 2014 review by Langeveld et al that stated: “Several modes of action have been put forward by which antibiotics and the EO components may act synergistically, such as by affecting multiple targets; by physiochemical interactions and inhibiting antibacterial-resistance mechanisms. Many reported assays show additivity or moderate synergism, indicating that EOs may offer possibilities for reducing antibiotic use.” 135
Footnotes
Acknowledgments
In Memoriam: This is the 17th and final study sponsored by D. Gary Young (1949-2018).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.