
Abstract
Mental illnesses (MIs) such as anxiety, epilepsy, major depression, schizophrenia, sleep disorder, and pain influence the quality of life severely. According to the World Health Organization Atlas for Mental Health (2014), the formal health sector in Lesotho has only 13.7 mental health workers per 100 000 of the population, which breaks down to 0.1 psychiatrist and other medical doctors, 0.3 psychologists, 4.7 nurses, and 5.2 social workers. Traditional health practitioners (THPs) have always played a significant role in the prevention and treatment of MIs, via utilization of Lesotho’s vast diversity of plants. This investigation aims to determine which medicinal plants are used for the treatment of MIs in the Berea, Leribe, and Maseru districts of Lesotho. A combination of unstructured and semistructured one-on-one interviews were conducted with 27 THPs. They were interviewed about the status of MIs in Lesotho, diagnostic methods, medicinal plants used, and preparation and administration of the herbal remedies in the treatment of MIs. A total of 43 different plant species (indigenous and exotic) were indicated by the THPs as commonly used to treat neurological disorders. With the exception of one unidentified plant, the plants represented 26 families and 42 genera. The most common families are the Asteraceae (9 species), Fabaceae (5 species), and Rosaceae (3 species). The most cited plant species were Morella serrata (Myricaceae) (26%), followed by Xysmalobium undulatum (Asclepiadaceae) (22%), and Afroaster hispidus (Asteraceae) (15%). This survey provides, for the first time, a database of Lesotho’s medicinal plants that are used to treat MIs.
Keywords
Mental illness (MI) is one of the most devastating, yet underestimated socioeconomic burden the world has ever experienced. MIs, including anxiety, epilepsy, major depression, schizophrenia, sleep disorder, and pain, add to the burden of neglected diseases with far-reaching results. They are believed to contribute an estimated 14% to the global burden of disease, 1 and research suggests that this problem is not given due attention in both developing and developed nations.
According to World Health Organization, 2 Lesotho is one of the southern African countries facing an increasing double burden of disease, reporting that there were increases in the burden of communicable as well as noncommunicable diseases in the country. According to Partners in Health Lesotho 3 one-fifth of Lesotho’s 2.2 million people suffer from some form of MI, predominantly depression and anxiety. Research further reveals that a significant proportion of people living with HIV in most countries in south-Saharan Africa have a diagnosable mental disorder, and Lesotho is no exception. Health care in Lesotho is in the hands of government, the private sector (churches and private surgeries), and civil society (traditional health practitioners [THPs]). However, currently, support from the government is directed toward its ministries only, especially the Ministry of Health, excluding the private sector and civil society organizations. The total expenditure on health as a percentage of gross domestic product in Lesotho was estimated at 8% in 2011, 1.8% of which was spent on mental health. 4
Statistical information about MIs is difficult to access, and that which is available is usually incomplete and indicates that the government’s attention toward mental health in Lesotho is inadequate. Although the government ensures that psychotic drugs are available for the mentally ill, many still do not access them for a number of reasons. First, MI is still stigmatized in Lesotho, making it difficult for the patients to openly seek Western medical attention. Secondly, language barriers between the patient and Western doctor, as well as difficulty in getting access to Western healthcare centers make matters worse. Finally, research suggests that many of the currently used psychotic drugs are costly, and associated with life-threatening side effects. Consequently, many Basotho still rely heavily on medicinal plants or indigenous remedies for primary healthcare. A challenge remains, however, to add more scientific evidence in support of their healing properties through thorough investigations. 5
Existing literature on Lesotho’s medicinal plants has focused on plant species that treat ailments ranging from pain, circulatory, degenerative, reproductive, digestive, skin infections, and so on and very little has been reported on the treatment of MIs. The scientific evidence of the healing properties of most of these plants is also lacking, thus making the documentation on the medicinal plants of Lesotho incomplete. This research, thus, provides a database of medicinally important plants that are used to treat MIs in Lesotho and forms a basis for future scientific work on these plants.
The main objectives of this survey were to interview THPs in the chosen study area to gather information about their experiences regarding psychotic disorders in the region, to document all relevant information about the status of MIs in the 3 districts, and to report all plant species which are used locally to treat such disorders.
The THPs of Southern Africa are practitioners of traditional African medicine and can be divided into the following groups:
THP: Lesotho healers who purport to have adequate knowledge about medicinal plants (herbs) and African traditional healing systems. It encompasses sangomas, diviners, herbalists, charlatans, and apprentices. For the purpose of this study, herbalists, diviners, and apprentices are collectively referred to as herbalists.
Herbalist: Herbalists are THPs who rely only on plants. They have extensive knowledge about different plants and which illnesses they prevent or cure. They diagnose and treat minor ailments, and if they are unable to cure the disease, they refer patients to a diviner. 6
Sangomas: Sangomas are THPs who draw their wisdom from their ancestors. A man or woman would normally receive a calling from ancestors before they can be sangomas. This calling, though, varies from one person to another and manifests itself in the form of illness that nobody can cure regardless of their expertise. Its symptoms include, but are not limited to, fits, headaches, psychosis, and sometimes belching uncontrollably. They usually have to go through initiation before they graduate into “sangomahood.” It is through this initiation process that they learn about the powers of ancestors, African traditional remedies, and divination.
Other healers in Lesotho include the following:
Religious healers: Religious healers have strong inclinations to God. They believe that only God heals, and nobody on earth has powers to heal if not instructed by God. Their remedies rely heavily on prayer. However, some may also use “holy” water and/or herbs.
Western practitioners: These are medical doctors who have received formal training in medicine. They diagnose patients, give advice (and sometimes counseling), and prescribe medication. Their remedies are scientifically based.
The Study Area
The survey was conducted in the 3 most densely populated districts of Lesotho (Lesotho Bureau of Statistics, 2013), namely Berea (29° 10′ 00″ S; 27° 55′ 00″ E), Leribe (29° 00′ 00″ S; 28° 00′ 00″ E), and Maseru (29° 19′ 00″ S; 27° 29′ 00″ E) (Figure 1). Maseru is the capital of Lesotho and the administrative center. It enjoys a fair degree of development in many aspects and departments. The order of degree of urbanization in the 3 districts is Maseru, Leribe, and then Berea. The main cities (Teyateyaneng, Hlotse, and Maseru city, respectively) for the 3 districts lie in the lowland area of the country and mark the busiest centers of activity both for practice of traditional healing and sales of indigenous medicinal plants. The districts perimeters, however, extend toward the foothill and the highland areas.

Location of Lesotho in South Africa, and location of municipal districts in Lesotho.
Study Methods
The ethnobotanical data were collected from November 2015 to January 2016. A combination of one-on-one unstructured and semistructured interviews 7,8 was employed in data collection. A total of 27 interviews were conducted with 24 males and 3 females practicing THPs at their muti shops and/or homes. The THPs were randomly selected on the basis of guidance from volunteers and people of good will, availability and accessibility, their willingness to participate in the survey, and having adequate experience in the field. No prior appointments were made and only native Lesotho THPs were interviewed. After the objectives and possible outcomes of the survey had been explained to the THPs, they were asked to sign a consent form before answering the questionnaires. The consent forms were presented in Sesotho, which is the local language of all the respondents.
Respondents were first asked to share their knowledge and experiences with regard to the seriousness of psychotic disorders and treatment of patients with psychotic disorders in Lesotho, second to describe the diagnostic characteristics of their patients and what they use to treat them, and third to give details about mode of preparation and administration of remedies. Other information sought included, but was not limited to the following:
names, ages, contact details, date, village, and district of the healer;
type of healer;
years of experience in the field;
level of education;
mode of attaining knowledge;
field of specialization;
gender and age groups most vulnerable to psychotic disorders;
relationship with other healers; and
relationship with Western doctors.
All the plant species mentioned by the THPs were collected from various regions throughout the 3 districts and identified by our botanist Mr M. Polaki (Director, National University of Lesotho Botanical garden, and Curator of the herbarium). Voucher specimens for 42 identified plant species were deposited at the National University of Lesotho herbarium.
We analyzed the information we received about the medicinal plants used to treatment MIs via (i) the frequency index (FI) to compare the relevant importance of each plant species, (ii) the frequency of plant parts used (%), and (iii) the distribution of age and sex among the interviewees. The FI is the percentage frequency of citation of each plant species, and is calculated by using the following formula:
where FC is the number of THPs citing the plant and N the total number of THPs. 9
The THPs
Gender and Distribution by District
A total of 27 THPs (24 males [89%] and 3 females [11%]) participated in the survey. Ten THPs (including 1 female) were interviewed in the Berea district, 9 (including 1 female) were from Leribe, and 7 (including 1 female) were drawn from the Maseru district. The ratio between the genders is a clear indication that the practice of traditional healing is still a male-dominated profession, as substantiated by the same ratio found in the muti shops, which were predominantly manned by males. A similar observation was made by Moteetee and Van Wyk 10 in one of their ethnobotanical surveys done in the Maseru district of Lesotho, thus strengthening the African cultural and traditional belief that God has bestowed special powers on man to heal the world, and that women must be relegated to taking care of the household and the upbringing of children.
Demographic Characteristics
All questionnaires and accompanying documents were translated into Sesotho prior to interviews. A summary of the demographic characteristics of the healers is presented in Table 1. The youngest practitioner was between 20 and 30 years old while the oldest was above 61 years old. Thirty-seven percent of the healers were over 61 years old, while 59% were between the ages of 31 and 60 years. Therefore, the survey has managed to get the views from both young and old healers—from the learners and the experienced. The educational background of the healers reflects that most healers had attained elementary school education. This category makes up 67% of the respondents. Approximately 15% of THPs did not go to school at all. An interesting observation is that a significant 11% had attained college education and they were also the healers who combined indigenous healing methods with Western systems of healing, referring their patients to clinics or hospitals whenever the need arises.
Demographic Characteristics of Traditional Health Practitioners.

Although the primary objective of the survey was to interview THPs who use plants in treating their patients, we did not discriminate when it came to different modes of healing that were used by the healers. The modes of healing employed by the healers ranged from purely religious to Western indigenous. One religious healer indicated that she used “holy” water only for healing. A significant number (59%) of healers were herbalists, while others were either sangomas or several combinations of sangomas, herbalists, or Western healers. All respondents had minimum 5 years of experience in the field. Over 50% of the healers had more than 20 years of experience, thus providing a fair practical experience to trust the information shared.
With regard to the field of specialization, all THPs indicated that they did not specialize in a specific type of illness, claiming that they treated various illnesses ranging from mental, sexual, and respiratory diseases to headaches, wound healing, and skin infections and even cancers, a phenomenon characteristic of African traditional healing practices.
Knowledge Acquisition
As has been emphasized in the previous sections of this paper, indigenous knowledge in African traditional healing is verbally passed on from generation to generation. There could be good reasons for such mode of knowledge transfer, but one of the main reasons in our opinion was to preserve the secrecy of the practice. On the question of how the respondents acquired the healing knowledge and skills, 30% of them attributed their art of healing as a gift from the ancestors, and another 30% claimed to have attained their knowledge from their parents who were herbalists themselves. Conversely, the sole religious healer stated that her knowledge and wisdom of healing came from God. The rest of the THPs indicated that their knowledge came from working for experienced herbalists (in most cases as gatherers of herbs), or through training. A small proportion of these herbalists indicated that they had been herd-boys from a young age and that they started learning about herbs since childhood. All sangomas revealed that much of their training was attained from their mentors and supervisors during initiation. It is noteworthy that this survey has revealed that whether one attributed one’s knowledge as a gift from God, gods, or ancestors, every healer had learned from the experience of others, and that learning process never stops as long as one is in the profession.
Seriousness of the Disorder and Its Management
Frequency of consultations can be used as a measure of how serious a particular illness is. This survey sought to measure the seriousness of MIs in Lesotho by establishing from THPs how many mentally ill patients they treated at a given period of time. We learned, in general, that Basotho hardly seek professional help for illnesses that they regard as minor. These minor illnesses include depression, sleep disorder, anxiety, stress, mood fluctuations, and others. Professional help is sought for severe cases such as schizophrenia, panic disorder, epilepsy, and major depression. As a result, in this section, the responses given were based on the frequency of visits by schizophrenic patients. All respondents warned that, regardless of personal class or status, MIs are most common in the “middle-ages” (teenage to adulthood). This observation was in line with the global estimates that around 20% of the world’s children and adolescents have some form of mental problems. Respondents, however, indicated that they had treated MIs across all age categories, from children (3-12 years) to the old aged (65+ years).
Nearly half of the THPs stated that they rarely came across severe mental cases such as schizophrenia in their practices. They estimated that over a period of 5 years, they treated no more than 2 schizophrenics. On the other hand, 31% of THPs estimated that they treated between 2 and 3 schizophrenic patients over the same period of time. The remainder of THPs (23%) indicated that they encountered and treated 3 and more severe mental cases (especially schizophrenia) over a period of 5 years. We learned that a larger population of Basotho seems to resort to quick in-house remedies for milder cases of MI, and hardly seek professional help.
On the issue of which gender is most vulnerable to MIs, 26 THPs responded, and their responses were based on 1 disorder, being schizophrenia. Fifty-six percent of the respondents stated that schizophrenia is most common in males, 7% argued that schizophrenia affects females more, while 37% reported that schizophrenia does not discriminate on the basis of gender. All THPs echoed that compared to other common illnesses such as headaches, venereal diseases, respiratory infections, and stomach complaints, MIs were less common in the study area. Judging by the numbers of patients treated by the healers, it is evident that MIs are under-reported, or not a serious problem in the chosen study area. However, Madikizela et al 9 reported that even though the history of MI stretches back to ancient times in Lesotho, the common population still regards it as something evil and violent and stigmatizes sufferers of MIs. Families should be encouraged not to “hide” members with schizophrenia, thereby depriving them of the opportunity to find a cure, and remedies that have been found to be effective must be fully utilized.
Diagnostic Symptoms
The medical art is depicted in the skill of interviewing the patient to elicit important information, the ability of using the senses to identify signs of abnormality on the body, and intuition and judgment to extract relevant symptoms, signs, laboratory data, and discard all the rest. 10 Diagnostic symptoms of MIs reported by the THPs can be divided into 2 categories: category I and category II. Category I symptoms are associated with schizophrenic patients, while category II symptoms are observed for other MIs like anxiety, depression, sleep disorder, and epilepsy.
It must be highlighted that this is the part of the interview that THPs seemed not to understand. The interviewer observed that THPs could not really differentiate among the different types of mental disorders that are known in the biomedical world (depression, anxiety, sedation, epilepsy, and so on), except for the severe schizophrenia. Consequently, their responses sought to describe how they diagnosed schizophrenic patients. Asked on how they diagnose the mentally ill, traditional healers gave a series of signs and symptoms that they look for on a patient, and these are summarized in Table 2. All THPs indicated that schizophrenics are known by conversation abnormalities, nightmares, hallucinations, uncontrolled fear, violence, eye contact avoidance, sound quietness, and so on. On the other hand, milder forms of MIs such as stress, depression, sleep disorders, and anxiety are traditionally placed under 1 category. The most common diagnostic symptoms mentioned included depressive moods, anger, headaches, insomnia, memory loss, and loss of consciousness.
Diagnostic Symptoms of Schizophrenia and Other MIs.

MI, mental illness.
Clearly, the responses that are summarized in Table 2 highlight the fact that in traditional health practice, diagnosis remains one of the mysterious challenges to date. Haslam 11 observed that mental disorder is not like infectious disease, which is characterized by a single, identifiable cause underlying a group of symptoms. Most psychiatric symptoms spring from a tangled multiplicity of causes. In addition, many symptoms are not specific to a single condition. Many THPs argued that the intuition and directions for treatment were given by gods, God, or the ancestors.
Materials Used for Treatment
Plants have always played a vital role in the well-being of man since the beginning of life itself. They have consistently been used as sources of food, fuel, medicines, shelter, and clothing. This survey revealed that plants and plant-derived products are the primary choices in the treatment of MIs. With the exception of 1 religious healer who stated that she used “holy” water and prayer only in her treatments, all other THPs indicated that their remedies were made up of plant-derived products. None of the respondents claimed to use animals or animal-derived products as the only ingredients in their concoctions. However, 33% of the healers revealed that they used animal fat in the preparation of some remedies for MIs, and sometimes certain parts of animals may be incorporated into their remedies. Results are presented in Figure 2.

(a) Materials used for healing patients, and (b) plant parts used.
With regard to the specific parts of the plants used, most healers cited roots and leaves (57%) as the plant organs used most frequently in the preparation of remedies for mental disorders. The second most used plant organ were roots only (23%). Few THPs cited leaves only (8%), whole plants (8%), and rarely tree trunks/barks (4%) (Figure 2). While all plant parts seemed equally useful, we note that most herbal remedies for MIs were derived predominantly from a combination of roots and leaves. Our take is that future scientific evaluations should, therefore, concentrate more on these plants parts. Since the use of plant roots for medicinal purposes often lead to plants’ destruction, we suggest that THPs should practice sustainable harvesting methods.
Preparation and Administration of Medication
When it came to mode of preparation and administration of remedies, THPs were very reluctant to provide such “very confidential” information. However, we learned that preparation and administration are guided by 2 main factors: (i) the type of illness to be treated (schizophrenia, epilepsy, mood disorder, and so on) and (ii) the physical, mental, and/or psychological state of the patient. For example, a quick remedy for headaches is best given in the form of inhalations (snuff) of powdered roots or leaves. A violent schizophrenic will normally not be given oral medication, until their violence subsides. It is noteworthy that all oral preparations (teas, infusions, and other decoctions) and steam baths are prepared in water, indicating that most of the metabolites that are utilized by the healers in their remedies are naturally of high polarity. The general modes of administration for various MIs are summarized in Table 3.
General Modes of Administration of Remedies for Different Mental Illnesses

On the question of whether MIs were curable or not, all 27 THPs confidently stated that they were curable. However, strong emphasis was placed on the fact that patients should be taken for diagnosis and treatment with the first signs of suspicious symptoms. One THP, through informal talks with the researcher, stressed that treatment strategies for people with MIs must be directed toward the causes, and not the symptoms as was common practice. In his opinion MIs predominantly arise as a result of prevailing socioeconomic, personal, and/or psychosomatic circumstances surrounding man. Therefore, a holistic approach that touches the mind, body, and soul must be adopted in rooting out MI.
Working Relationships and Recommendations
Traditional health practice in Africa is increasingly acknowledged as an integral component in health sector. Moshabela et al 12 argued that the merging of biomedical and traditional healing paradigms could provide a complementary system of plural health care, which would offer patients a truly holistic and comprehensive form of health care. The question is to what extent can this dream come to reality? Research carried out in South Africa revealed that despite the milestones achieved by several stakeholders in trying to merge these 2 spheres of knowledge, tensions continue to dominate the landscape of research and policy debates on the roles and practices of THPs with respect to historical injustices, gaps in scientific evidence, mistrust on the part of biomedical practitioners, and toxicity of medicines. 12 This is perhaps an African phenomenon. THPs interviewed in this survey described the relationships among themselves as being very complex. Generally, there is no unity among THPs, not only in the area under study, but throughout the country of Lesotho. Occasionally, 1 THP may team up with a friend, a family member, or close acquaintances. Sometimes working relationships develop between a scholar and teacher healer, though it normally is not guaranteed that it would last beyond the completion of studies. Where it occurs, knowledge sharing among THPs is minimal. In a number of cases, such relationships quickly disintegrated upon the realization that it benefited only 1 party. These are perhaps some of the reasons why there is no noticeable growth and development in the traditional healing sector and addressing this issue will not only benefit the healers, but society as a whole.
Regarding their relationships with biomedical practitioners, all THPs interviewed indicated that they had no defined working relationships with Western practitioners, either at regional or country level. A series of interventions initiated by the Ministry of Health (Lesotho) to discuss how best THPs could be incorporated into the national health system did not bear any fruit. According to the THPs, biomedical practitioners do not recognize them as their colleagues, yet they (THPs) are ready to work hand-in-hand with them.
Three practitioners indicated that in the area where they operated, they had good relationships with the staff and management of local clinics where some of their patients were referred to for specialized services like blood transfusions and CD4 counts. However, they (THPs) did not receive any referrals from the clinics. Clearly, barriers still exist between Lesotho THPs and their biomedical counterparts, thus hindering potential developments in the health sector.
The THPs made the following recommendations that, if put into practice, could help reduce the incidences of MIs in the country: (i) abstinence from drug abuse, proper diet, and improved hygiene; (ii) improvement of communication; (iii) seeking professional help whenever confronted by challenges; (iv) equal sharing of resources; (v) avoiding marriages at a tender age; (vi) avoiding multiple partners; (vii) taking notice of behavioral changes and taking decisive action on time; (viii) avoiding unrealistic aspirations; (ix) maintenance of stable families; (x) early diagnosis and treatment of diseases (especially neurological diseases); (xi) avoiding hatred; (xii) improving working relations among herbalists and Western practitioners; (xiii) unity; (xiv) submitting to ancestral calls; and (xv) strong faith in God and prayer.
Diversity of Medicinal Plants Used
Although they lack scientific evidence, traditional herbal remedies have proven to be effective in a number of situations over the years. It is common knowledge that indigenous knowledge has been verbally passed on from generation to generation. Unless it is documented, some of this knowledge gets lost with time. Today, scientists have revealed that plants contain constituents that can work in synergy to effect certain properties of medicinal value. In addition, a considerable number of individual constituents (pure compounds) possess certain pharmacological properties that make them ideal drugs for treatment of diseases. Therefore, traditional indigenous knowledge that is substantiated by scientific evidences ensures a better appreciation of the power of plants in the field of medicine.
In our survey, a total of 43 different plant species (indigenous and exotic) were cited by the THs as commonly used to treat patients with psychotic disorders (Table 4). Available literature about these plants—particularly that which relates to MIs—is given for comparison’s sake. With the exception of one as yet unidentified plant (locally known as morentsoene), the plants represented 26 families and 42 genera. The most cited families were Asteraceae (9 species), Fabaceae (5 species), and Rosaceae and Apocynaceae (3 species each). Hyacinthaceae were represented by 2 species, while the rest of the families were represented by 1 species each. Nearly 88% of the families cited in this survey have reported psychoactive uses in southern African healing tradition. 13 It is noteworthy that the families Geraniaceae, Myricaceae, and Urticaceae have never been linked with psychotic activity and are reported for the first time in this survey. The most cited plant species was Morella serrata (Myricaceae) (26%), followed by Xysmalobium undulatum (Apocynaceae) (22%), and A. hispidus (Asteraceae) (15%).
Plant Families, Species, and Sesotho Name, Voucher Number, Citation (%), and Ethnomedicinal Uses
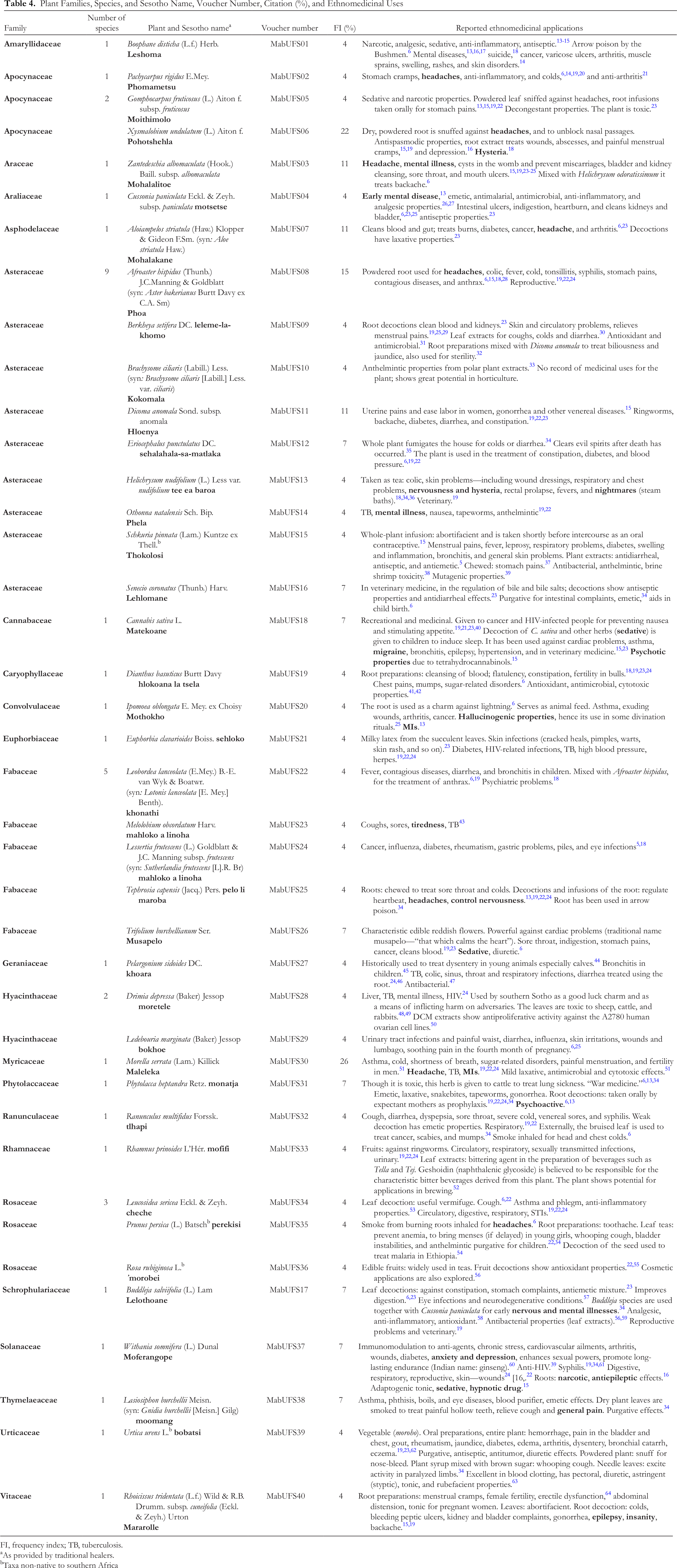
FI, frequency index; TB, tuberculosis.
aAs provided by traditional healers.
bTaxa non-native to southern Africa
MIs are controlled by gamma aminobutyric acid (GABA) receptors, which are found in mature mammalian nervous systems, especially the brain. GABA is an endogenous inhibitory neurotransmitter that binds to these receptors, thereby influencing motor control, vision, and many other cortical functions. It also regulates anxiety. Several drugs (eg, benzodiazepines and barbiturates) that are already used to treat different types of neuronal disorders have been shown to influence the activity of GABA receptors. In the same manner, many plant-derived constituents (crudes and pure compounds) directly (in competition with GABA) or indirectly (allosterically) influence the activity of GABA receptors. It is these intrinsic abilities (to influence GABA receptors) that define psychotic medicines. According to the literature, extracts from the most cited plant species, M. serrata, showed antimicrobial activities. 51 The plant is also used to treat headache and MIs. 19,22,24 There is, therefore, a close correlation between the literature and survey findings regarding this plant. Xysmalobium undulatum belongs to the Apocynaceae family. According to Bhadane et al, 65 several members of this family have medicinal properties. Although they are largely consumed as food, some members are known to be poisonous. Apocynaceae are rich in alkaloids, terpenoids, flavonoids, glycosides, lactones, phenolic substances, and hydrocarbons. 65 Few studies have reported the antioxidant, anti-inflammatory, and antimicrobial properties and cytotoxicity of crude extracts and pure compounds from this family. Locally, X. undulatum is traditionally used to treat headache and depression, 16 suggestive of its central nervous system (CNS)-stimulating property. While A. hispidus is the third most cited plant species in this survey, there are currently no literature reports showing any CNS-stimulating or GABAergic activities of this plant. Several members of this family like O. natalensis and some Helichrysum species have shown sedative and other nervous activities, validating their traditional use in the treatment of MIs.
Conclusion
The outcome of this survey demonstrates that ethnobotanical knowledge is generally preserved in Lesotho, and that the THPs are the main repositories. The preservation of indigenous remedies must be a priority, even if the secrecy of the art must be upheld. It seems that mental disorders are not seen as a serious threat to Lesotho, but due to the stigma associated with MIs they are probably vastly under-reported. The public will benefit from general education on the causes, nature, and treatment of various MIs to lessen this stigma and bring relief to hidden and silent sufferers. MIs can be treated using a wide range of medicinal plants from various families and genera. Among the variety of plant species, genera, and families cited by THPs in this survey, the families Geraniaceae, Myricaceae, and Urticaceae have never been associated with psychotic activity. Although they received low percentage citation indices, the long historical uses of C. paniculata, Z. albomaculata, and W. somnifera in the treatment of MIs cannot be overlooked in our future evaluations. This survey provides, for the first time, a database of Lesotho medicinal plants used for the treatment of mental illnesses. Pharmacological and phytochemical investigations on these plants are in progress to validate indigenous traditional uses.
Footnotes
Acknowledgments
We thank the University of the Free State for funding, and the National University of Lesotho (NUL) for staff development leave given to Mr Mabaleha. We are grateful to the Basotho THPs for taking part in this survey. We thank Mr Moretloa Polaki (Director, NUL Botanical garden, and Herbarium Curator) for assistance in the identification of medicinal plants, and the preparation and preservation of herbarium samples. We further acknowledge Lesotho Ministry of Agriculture and Food Security for import permits (Agricultural Research Department).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.