
Abstract

Continuous glucose monitoring (CGM) systems may help individuals with type 1 diabetes manage glycemia around exercise.1,2 However, applying this technology to enhance performance in athletes without diabetes is a novel and evolving field.3,4 There is currently limited understanding of how CGM readings respond to varying exercise intensities in athletes without diabetes. In addition, the impacts of rising blood lactate concentrations ([La−]) during physical activity may reflect shifts in metabolic pathways, 5 but the potential impact of [La−] on CGM readings has not been thoroughly examined. Using a minute-by-minute CGM (Abbott Libre Sense Glucose Sport Biosensor), this study investigated capillary glucose dynamics, CGM accuracy, and the influence of [La−] on CGM readings during exercise in healthy athletes.
This observational study involved 10 well-trained male athletes (36 ± 10 years; 178 ± 6 cm; 72.7 ± 7.2 kg, VO2peak: 59.5 ± 6.1 mL/kg/min). Participants completed four bicycling sessions: a ramp test to exhaustion (Ramp) and three cycling sessions that lasted up to 30 minutes (at low, moderate, and high intensities). 915 CGM-glucose pairs were analyzed to assess sensor accuracy using mean absolute relative difference (MARD), a modified Clarke error grid, 6 and Bland-Altman bias plots. The relationship between [La−], capillary glucose, and CGM readings was also examined. The study received ethics approval.
Results showed that mean capillary glucose was significantly elevated with the high-intensity exercise (99 ± 2 mg/dL) compared with the other exercise intensities (Ramp: 93 ± 3 mg/dL [P = .02]; low: 90 ± 2 mg/dL [P = .001]; moderate: 93 ± 2 mg/dL [P = .03]). However, the increase in glucose concentrations with higher exercise intensity was not reflected with CGM (P > .05, Figure 1a). Despite these discrepancies, overall CGM accuracy remained acceptable, with MARD below 15% across all intensities (Figure 1b).
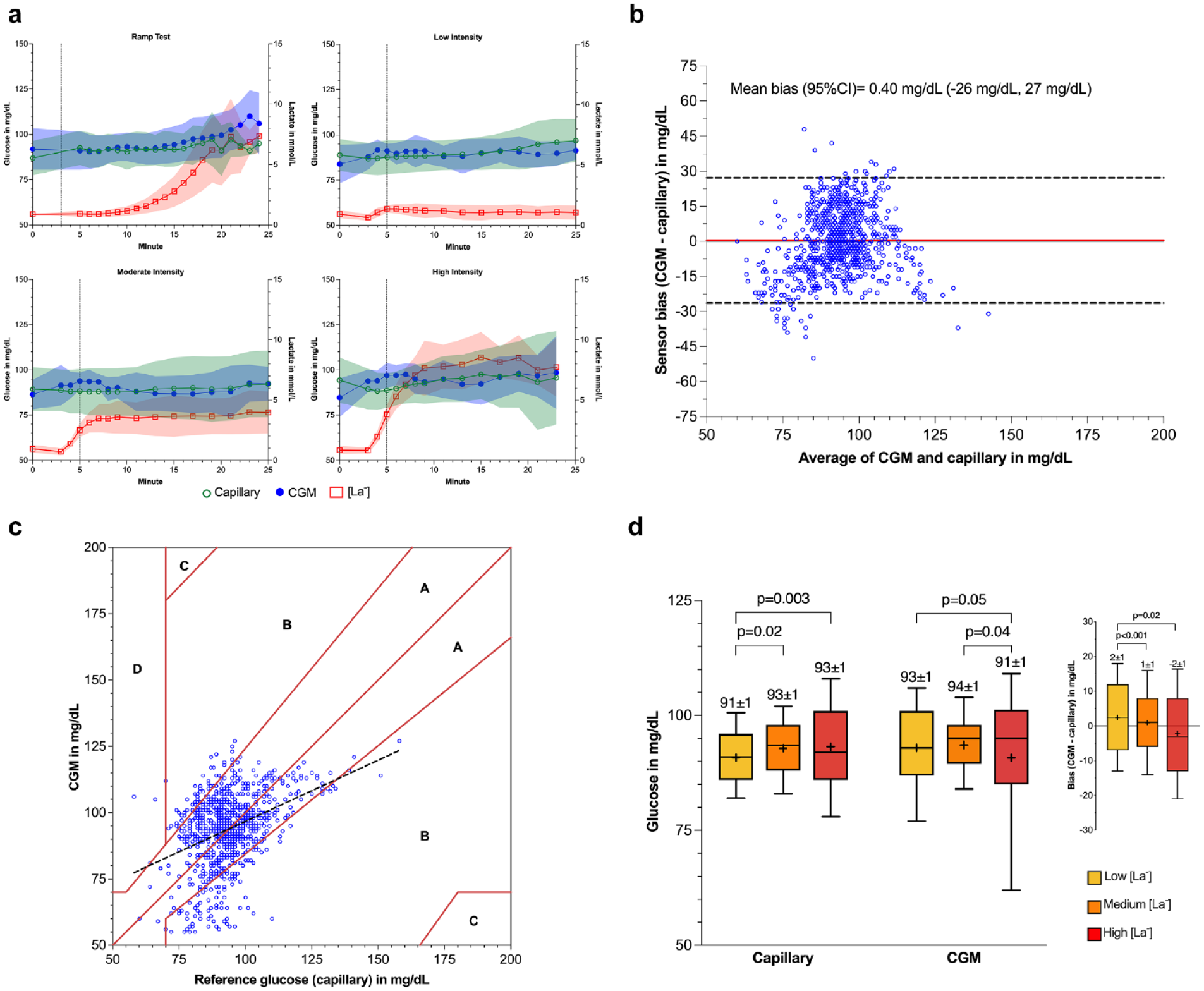
(a) Capillary glucose (green open circle), CGM glucose (blue closed circle), and lactate (red open square) levels during the bicycling ramp test, and the low (~70% of peak oxygen uptake), moderate (~80-85% of peak oxygen uptake), and high (~90-95% of peak oxygen uptake) intensity. Dashed vertical line signifies the end of a warm-up (~5 min at 30 Watts) and start of exercise, solid lines connect means, shaded regions denote standard deviation. (b) Bland-Altman plot (mg/dL) of mean sensor bias. The continuous red line denotes mean bias between measures (0.40 mg/dL) and horizontal dashed lines are 95% limits of agreement -26 mg/dL (lower) to 27 mg/dL (upper). (c) Modified Clarke-Error Grid analyses designed for people without diabetes of CGM versus capillary glucose (mg/dL) in Zones: A = within 20% of the capillary glucose; B = outside 20% of the capillary glucose; C = well outside of the capillary glucose; D = CGM values not detecting biochemical hypoglycemia (<70 mg/dL). Long dashed line is a simple linear regression between capillary and CGM values (y = 0.46*X + 51 mg/dL; R 2 = 0.15; P < .001). (d) Box plots demonstrating the relationship between low (<2.0 mmol/L; yellow), medium (2.0-4.0 mmol/L; orange) and high (>4.0 mmol/L; red) capillary lactate concentrations and glucose levels as measured in the capillary and interstitial CGM. CGM bias based on lactate concentrations is shown as an inset graph. Box plots extend from the 25th to the 75th percentile, whiskers extend from the 10th to the 90th percentiles. Within the boxes horizontal lines depict medians and plus sign the mean. Mean ± standard deviation and significant P-value determined from a linear-mixed-effects model denoted above each box plot.
Bland-Altman analysis showed a mean sensor bias of 0.40 ± 14 mg/dL, with narrow limits of agreement (Figure 1b). Modified Clarke-Error Grid analysis, Figure 1c, showed that 81.3% of readings were in Zone A, 18.4% in Zone B, with only 0.3% in Zone D.
The [La−] and CGM rate of change predicted CGM bias (P < .001 and P = .006, respectively), together accounting for 6.0% of the variability. The rise in [La−] appeared to associate with a rise in capillary glucose but not in CGM readings (Figure 1d). Specifically, capillary glucose was higher at [La−] of 2.0-4.0 mmol/L and above 4.0 mmol/L (both 93 ± 1 mg/dL), compared with 91 ± 1 mg/dL when [La−] was below 2.0 mmol/L. However, in CGM readings, lower glucose values were observed when [La−] exceeded 4.0 mmol/L (91 ± 1 mg/dL). Overall, when [La−] was below 2.0 mmol/L, CGM readings tended to have a positive bias, which diminished or became negative as [La−] increased.
This small study demonstrates that the Abbott Libre Sport Biosensor has reasonable accuracy across different exercise intensities in well-trained male athletes. However, elevated [La−] may cause the CGM to underestimate blood glucose concentrations, particularly during the early stages of exercise where [La−] may be elevated. These findings highlight the utility and accuracy of a novel glucose biosensor and the influence of lactate on CGM accuracy. Future studies should better understand how this technology may be used to enhance sport performance.
Footnotes
Abbreviations
CGM, continuous glucose monitoring; [La−], blood lactate concentrations; Ramp, ramp test to exhaustion; MARD, mean absolute relative difference; VO2peak, peak oxygen uptake.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.S., F.Y.F., and H.C.Z. were consultants for Supersapiens (TT1 Products, INNC, Atlanta, GA, USA) at the time of the data collection but the company did not support the actualization of the manuscript. A.J. and M.C.R. were previously scientific advisors for Supersapiens (TT1 Products, INNC, Atlanta, GA, USA). The views expressed in this article are those of the authors and do not reflect the position or policy of Supersapiens (TT1 Products, INNC, Atlanta, GA, USA). Other authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.