
Abstract
With increasing prevalence of obesity and cardiovascular diseases, there is a growing interest in the use of glucagon-like peptide-1 receptor agonists (GLP-1RAs) as an adjunct therapy in type 1 diabetes (T1D). The GLP-1RAs are currently not approved by the US Food and Drug Administration for the treatment of T1D in the absence of randomized controlled trials documenting efficacy and safety of these agents in this population. The Diabetes Technology Society convened a series of three consensus meetings of clinicians and researchers with expertise in diabetes technology, GLP-1RA therapy, and T1D management. The project was aimed at synthesizing current literature and providing conclusions on the use of GLP-1RA therapy as an adjunct to automated insulin delivery (AID) systems in adults with T1D. The expert panel members met virtually three times on January 17, 2024, and April 24, 2024, and August 14, 2024, to discuss topics ranging from physiology and outcomes of GLP-1RAs in T1D to limitations of current sensors, algorithms, and insulin for AID systems. The panelists also identified research gaps and future directions for research. The panelists voted to in favor of 31 recommendations. This report presents the consensus opinions of the participants that, in adults with T1D using AID systems, GLP-1RAs have the potential to (1) provide effective adjunct therapy and (2) improve glycemic and metabolic outcomes without increasing the risk of severe hypoglycemia or diabetic ketoacidosis.
Keywords
Introduction
Background
Given the body of available evidence, the American Diabetes Association Standards of Care 20241 recommends automated insulin delivery (AID) systems for managing type 1 diabetes (T1D). AID system use is increasing both in the United States and Europe. 2 However, despite the best-available AID technologies, only 50% of adults with T1D can achieve the optimal glycemic goal, which is a hemoglobin A1C (HbA1c) level of less than 7%. 3 Moreover, the prevalence of overweight and obesity is increasing among adults with T1D. 4 Obesity is associated with insulin resistance, higher insulin doses, and increased risk of cardiovascular diseases (CVDs).5-7 Studies have reported excess morbidity and mortality attributed to CVD among people with T1D. 8 Therefore, in people with T1D, therapies adjunct to insulin are needed to tackle increased weight, insulin resistance, and CVD risk.
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are increasingly used in type 2 diabetes (T2D) in adults and adolescents where they improve glycemia, lead to weight loss, decrease insulin resistance, and decrease CVD risk. 9 They are also used in people without diabetes who are obese. 10 In the past few years, their off-label use in T1D is increasing. 11 Liraglutide, a GLP-1RA that is administered daily, was investigated in adults with T1D (ADJUNCT ONE and TWO studies).12,13 It failed to demonstrate a reduction in HbA1c of more than 0.4% (which had been designated as the efficacy threshold by the regulators) compared to placebo, and there was an increase in risk for documented symptomatic hypoglycemia and ketosis.
Newer weekly GLP-1RAs (including a dual glucagon-like peptide-1 [GLP-1] and glucose-dependent insulinotropic polypeptide [GIP] agonist, tirzepatide) are more potent than older drugs in this class and have been shown to significantly reduce weight, improve HbA1c, and reduce CVD risk. There is now a resurgence of interest among clinicians to prescribe these drugs in T1D for glycemic and metabolic effects. In the absence of randomized trials, these molecules are currently not approved for use in T1D by the US Food and Drug Administration (FDA). This article defines so called dual agonists and triple agonists containing at least one drug which is a GLP-1RA agent or has GLP-1RA properties to be GLP-1RA drugs.
Currently, there are limited published data on the outcomes of using GLP-1RAs in the management of T1D. Therefore, Diabetes Technology Society (DTS) convened a meeting among experts to review the existing literature, identify knowledge gaps, and provide conclusions on the safe use of GLP-1RAs as an adjunct to AID systems in adults with T1D.
The Panel Meeting Process
DTS assembled a panel of nineteen adult endocrinologists, pediatric endocrinologists, and engineers with expertise in the use of GLP-1RAs and in the use of AID systems for treating T1D. Panelists were mostly from the United States (sixteen members) and three were from Europe (one each from Austria, Denmark, and Germany). The panel included two chairs (Viral N. Shah and David C. Klonoff), two assistant chairs (Anne L. Peters and Guillermo E. Umpierrez), seven academic panelists (Signe Schmidt, Umesh Masharani, Ali Cinar, Peter G. Jacobs, Chiara Fabris, Grazia Aleppo, and Lia Bally), and eight clinical panelists (Julia K. Mader, Priya Prahalad, Halis Kaan Akturk, Rayhan A. Lal, Eric Zijlstra, Eda Cengiz, Kathleen Dungan, and Jennifer L. Sherr). The panelists met three times in 2024 and developed a set of 32 conclusions. After the panel completed its work, the panel members decided to write a report summarizing the reasons for their conclusions. This report presents the group’s conclusions as well as the ideas that went into the conclusions.
Section 1: Physiology of GLP-1RA Therapy in T1D
Signe Schmidt, MD, PhD1 and Julia K. Mader, MD2
1Steno Diabetes Center Copenhagen, Herlev, Denmark
2Division of Endocrinology and Diabetology, Medical University of Graz, Graz, Austria
Key points:
GLP-1RAs may improve glycemia in T1D through actions in the pancreas, gastrointestinal tract, and central nervous system.
The mechanism of GLP-1RAs does not cause hypoglycemia and may reduce but not eliminate the exogenous insulin dose in T1D.
GLP-1RA-associated side effects from the gastrointestinal tract resemble symptoms of diabetic ketoacidosis.
Effects of gastric emptying (and with this the efficacy in the effect of postprandial glucose control) of short- and long-acting GLP-1RAs can be affected by “tachyphylaxis,” which might lead to an attenuation of the initial efficacy over time.14,15
Adjunct therapies such as GLP-1RAs might improve the ability to achieve glycemic targets and reduce insulin requirements as well as body weight.
GLP-1 is a hormone released from enteroendocrine cells in the human gut in response to food intake. 16 It exerts diverse effects through receptors in several body organs, shown in Figure 1. Currently, the FDA has approved six GLP-1RAs for intermittent and continuous receptor activation to improve glycemia and reduce CVD risk in adults with T2D, summarized in Table 1. 17 Three of these (liraglutide, semaglutide, and tirzepatide, the latter of which belongs to both the GLP-1RA and the GIP receptor agonist classes) have also been approved for weight and CVD risk management in individuals with overweight and obesity. In 2020 FDA expanded its approval for injectable semaglutide label to also include reducing the risk of heart attack, stroke, or death in adults with T2D and known heart disease. 18 Oral semaglutide was approved by the FDA this year to reduce the risk of serious heart problems in adults with obesity or overweight. 10 However, none of them are currently indicated for use in people with T1D. Eventually an indication for T1D will be needed that is separate from that for obesity or to prevent heart disease.
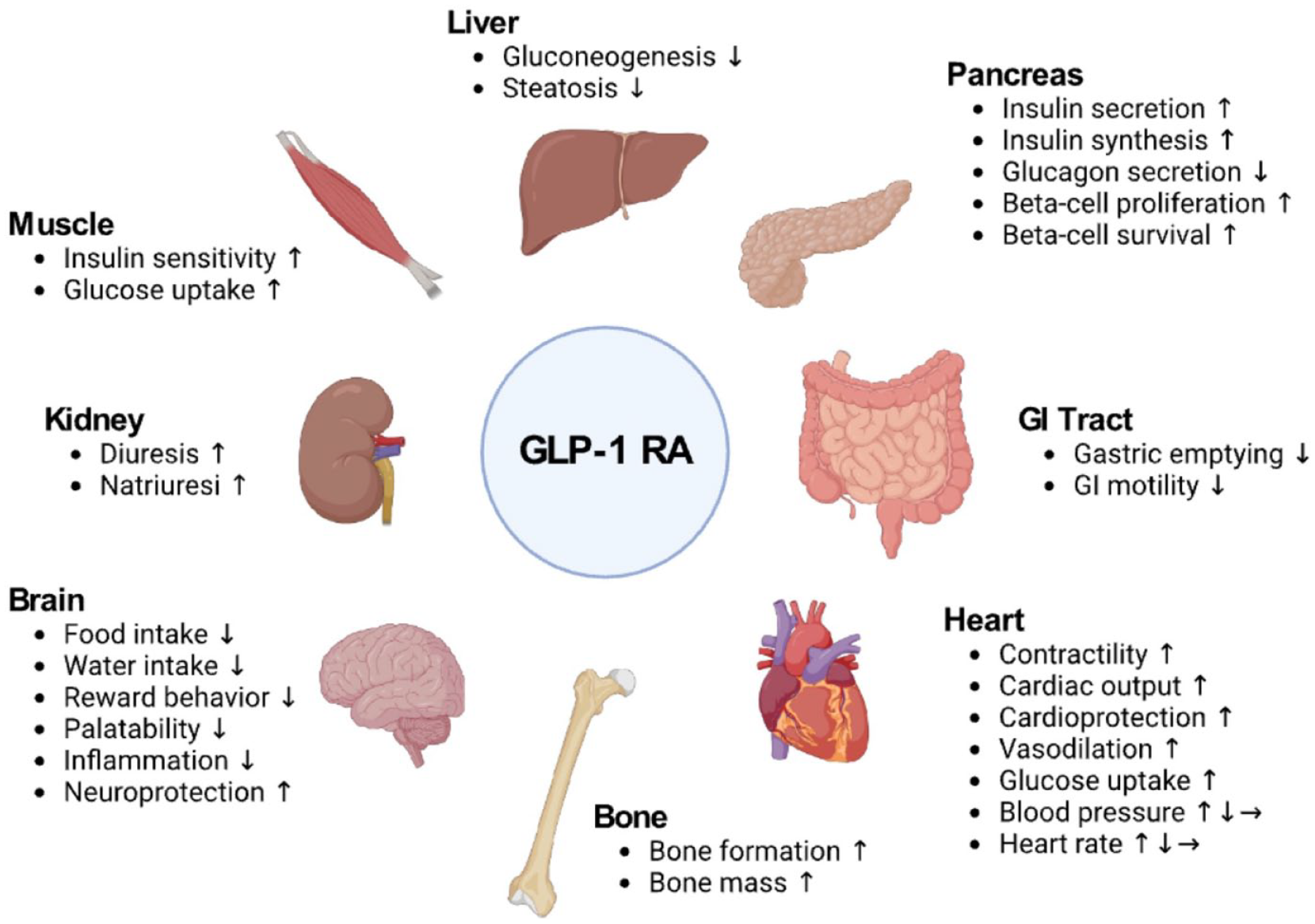
Glucose-lowering and weight-reducing mechanisms of glucagon-like peptide-1 receptor agonists in type 1 diabetes.
Summary of the GLP-1RAs Approved by the US Food and Drug Administration.

Abbreviations: CVD, cardiovascular disease; GLP-1RA, glucagon-like peptide-1 receptor agonist.
Our understanding of GLP-1 physiology largely stems from studies in volunteers without diabetes and people with T2D. However, evidence suggests that the addition of GLP-1RAs to intensive insulin therapy, including AID, may address some of the biggest challenges faced by many with T1D, which are suboptimal glucose values, overweight, and obesity.17,19 The potential glycemic benefits of treatment with GLP-1RAs in T1D may be mediated by effects on (1) the pancreas (decreased glucagon secretion in everyone and increased insulin secretion in those with remaining functioning beta-cells), (2) the central nervous system (reduced intake of food and liquids and altered food preferences), and (3) the gastrointestinal tract (delayed gastric emptying and reduced motility).
In individuals with residual beta-cell function, GLP-1RAs potentiate glucose-stimulated insulin secretion and may, in some cases, reduce or even temporarily eliminate the need for exogenous prandial and basal insulin.20-22 As demonstrated in men without diabetes, stimulation of insulin release is glucose-dependent, ceasing when plasma glucose falls below normoglycemia, and therefore, GLP-1RAs in themselves should not cause hypoglycemia. 23 Independent of insulin secretion, GLP-1RAs reduce postprandial glycemic excursions, which offers benefits to individuals with and without functioning beta cells. 24 The underlying mechanisms include suppression of glucagon secretion and altered gastrointestinal motility. GLP-1RAs provide cardiorenal protection in individuals with T2D and CVD, CVD risk factors, and/or chronic kidney disease (CKD), and there is growing evidence that they may also be effective in treating non-alcoholic fatty liver disease.25-27 To date, studies of GLP-1RAs in T1D have not been of sufficient size and duration to determine whether these individuals achieve the same benefits from treatment. The FLOW trial demonstrated that in patients with T2D and CKD, semaglutide can significantly reduce the risk of major kidney disease events, such as kidney failure and death due to cardiovascular causes. 28 The STEP-HFpEF trial supported the use of semaglutide as an effective treatment to improving exercise function and reducing body weight for patients with obesity and heart failure with preserved ejection fraction. 29
Gastrointestinal symptoms, including nausea, dyspepsia, vomiting, diarrhea, or constipation, are common with GLP-1RAs, and it seems that they are even more frequent and appear at lower doses in those with T1D compared to other people. 19 Reports of pancreatitis have been observed following GLP-1RA exposure; however, it is still debated whether this is a direct effect of the drug or secondary to the drug-induced weight loss and the concomitant increased risk of gallstones. 30
In rodents, GLP-1RA exposure is associated with thyroid C-cell tumor development. 31 There is no evidence suggesting carcinogenic effects in humans, but since the introduction of the first long-acting GLP-1RA, an FDA-initiated surveillance program has been monitoring the annual incidence of medullary thyroid cancer in the United States to investigate any potential association. 32
Section 2: Outcomes of GLP-1RA Therapy in T1D
Umesh Masharani, MB, BS1 and Priya Prahalad, MD, PhD2
1University of California San Francisco, San Francisco, CA, USA
2Division of Endocrinology, Department of Pediatrics, School of Medicine, Stanford University, Stanford, CA, USA
Key points:
In people with T1D, the rates of being overweight or obese are similar to those of the general population.
The available evidence indicates that GLP-1RAs are effective in promoting weight loss in obese people with T1D.
GLP-1RAs depress the glucagon levels after meals; reduce postprandial glucose excursions; and modestly lower HbA1c levels.
GLP-1RAs may help people with T1D lose weight, lower their insulin doses, and improve their HbA1c.
People with T1D are interested in the weight loss benefits of GLP-1RAs.
People with T1D with remaining C-peptide achieve the greatest glycemic benefit from GLP-1RA use.
Historically, people with T1D have had a lean phenotype. However, this is no longer true. 4 The rates of being overweight or obese are now similar to those of the general population.2,3 Highlighting this, a study analyzing the National Health Interview Study data from 2016 to 2021 reported that 34% of people with T1D were overweight, and 28% were obese, which are about the same rates as people without diabetes.33-35 Obesity increases insulin requirements and leads to the onset of diabetes at a higher beta-cell mass. One study of adolescents found that a rise by one increment in body mass index (BMI) standard deviation was associated with a 25% greater risk for incidence of T1D. 36 In children with severe obesity, a 10% reduction in body weight is predicted to result in a 22% reduction in the incidence of T1D. 37
In the general population, obesity is associated with depression, decreased quality of life, increased risk of CVD, and many other medical problems. A Swedish National Diabetes Registry study of more than 25,000 people with T1D found that, after adjusting for various covariates including smoking, HbA1c, and duration of diabetes, obesity modestly increased overall mortality, major cardiovascular events (myocardial infarction or stroke), and heart failure in men but not women. 38
The mechanisms underlying increased obesity in people with T1D are likely to be similar to those that apply to the population without diabetes, such as influx of energy-dense foods, sedentary behavior, and socioeconomic factors such as food insecurity. 4 Additional factors that might be specific for people with T1D include intensive insulin therapy and hypoglycemia avoidance. 39 The Diabetes Control and Complications Trial study observed that, after an average of 6 years, the intensively treated group had an increase in weight of approximately 5 kg compared to the conventionally treated group. 40 AID systems do not necessarily prevent the weight gain associated with improved glycemic management. The pivotal trial of the MiniMed 670 G observed a 1.4-kg increase in weight in adults with T1D over the 3-month study period. 41
The usual treatments of diet and exercise can be instituted in people with T1D. Physical activity can enhance weight loss, but a major barrier for people with T1D is the issue of hypoglycemia with exercise due to difficulties in adequate adjustments of insulin therapy. There are very few studies specifically looking at the impact of different diets on weight loss in people with T1D. 42 Yet, it is likely that their effectiveness is similar to what has been documented in the general population.
GLP-1RAs and GLP-1/GIP dual receptor agonists are currently the most-effective therapeutic agents for weight loss for people with and without diabetes. They are involved in both peripheral and central pathways mediating satiety. 43 GLP-1 acutely inhibits postprandial gastric emptying, but this effect may be attenuated with continued use (tachyphylaxis). 15 The pharmacologically administered GLP-1RAs affect central nervous system satiety pathways by acting on vagal afferent neurons and by engaging GLP-1 receptors located in the central nervous system that are not protected by the blood-brain barrier.43,44
The weight loss benefit of GLP-1RAs and GLP-1/GIP dual-receptor agonists in people with T2D is now well established.45-47 These drugs can be used as first-line therapy for people with obesity and T2D. 47 There are, however, only limited data regarding their use in people with T1D. Liraglutide, which is an early-generation GLP-1RA, is the best-studied agent in this population. In randomized placebo controlled clinical trials in people with T1D, liraglutide resulted in weight loss up to 4.9 kg.12,13 The long-acting GLP-1RAs and GLP-1/GIP dual-receptor agonists are likely to be equally effective. There is a preliminary report that semaglutide therapy is effective in promoting weight loss in people with T1D, 48 and a retrospective chart review study also showed that that use of semaglutide (compared to computer-matched controls) in study patients with T1D and either overweight or obesity was effective in decreasing body weight and BMI and improving metrics of glycemia as measured by continuous glucose monitoring (CGM). 49
In the liraglutide studies, there was a modest reduction in HbA1c levels in the range of 0.2% to 0.3%.12,13 This is most likely due to depression of glucagon levels after meals and reduced postprandial glucose excursions.50,51 As tachyphylaxis to the gastric emptying effect of the agent is noted,15,52,53 it is unlikely that delayed gastric emptying is an important factor in lowering postprandial glucose excursions. Exenatide administration in people with T1D initially lowered postprandial glucose excursions, but the effect waned with time. 54 Table 2 presents results of a meta-analysis published in 2023 of 24 studies involving more than 3000 individuals with T1D that determined the effects on weight, HbA1c, and total daily insulin dose of four different GLP-1RA regimens as adjunctive therapy for T1D. 55
Mean Change in Glycemia, Weight, and Total Daily Insulin Dose Reported in a Recent Meta-Analysis of GLP-1RA Adjunctive Therapy in People With T1D. 55

Twenty-four studies were included in this meta-analysis (n = 3377, mean age 39.3 years, 54% men with mean duration of T1D 15.8 years and mean weight 80.6 kg). Sixteen trials used liraglutide, 6 trials used exenatide, and 1 trial used albiglutide. We did not include the albiglutide study (Pozzilli et al) 56 because it was aimed at evaluating beta-cell function in newly diagnosed T1D instead of glycemia and weight loss efficacy. Similarly, study by Ballav et al 57 was excluded for the meta-analysis outcomes as authors reported only changes in post-meal glycemic excursion during mixed meal test in T1D.
Abbreviations: CI, confidence interval; HbA1c, hemoglobin A1c; kg, kilogram; mg, milligram; T1D, type 1 diabetes; TDD, total daily insulin dose.
Symptomatic, but not severe, hypoglycemic episodes were more frequent with liraglutide therapy.58,59 However, the use of a more flexible insulin regimen might have mitigated the frequency of hypoglycemia. Two small studies have investigated the use of liraglutide in conjunction with closed loop systems, both using early-generation systems where the use of the closed loop was confined to an inpatient research unit admission. One study solely administered one dose of liraglutide 1.2 mg during one study visit, 59 while the other had a ~3- to 4-week dose titration phase with a goal of using liraglutide 1.8 mg during the closed-loop session. 58 Both trials achieved a reduction in peak postprandial glucose levels and reduction in insulin doses without increased rates of hypoglycemia. 59 As might be expected, the most common adverse reaction with liraglutide was nausea, which tended to occur at dose initiation and dose escalation, with this symptom waning over time.12,13 During the outpatient dose titration phase, participants were noted to lose 3.2 ± 1.8 kg, which occurred alongside a 26% reduction in their total daily insulin dose.
In conclusion, GLP-1RAs and GLP-1/GIP dual-receptor agonists effectively treat obesity in people without diabetes and those with T2D. Therefore, the use of these agents to treat obesity in people with T1D may be of benefit. Hypoglycemia that occurs with weight loss can be ameliorated by proactively adjusting the insulin doses.
Section 3: What Is Lacking in AID Systems Therapy in T1D: Better Sensors
Ali Cinar, PhD1 and Halis Kaan Akturk, MD2
1Department of Chemical and Biological Engineering, Illinois Institute of Technology, Chicago, IL, USA
2Barbara Davis Center for Diabetes, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Key points:
Further improvements in AID performance (such as a better percent time in range [% TIR] or greater safety against unexpected events) necessitate more information in real time from sensors reporting complementary data to the blood glucose concentration.
Data should best be interpreted by various statistical techniques (such as machine learning [ML]) to provide information leading to dosing of insulin, glucagon, or adjunctive therapy medications.
Integration of modeling, detection, and control activities both at the device level (AID pump, smartphone, cloud) and at the algorithm level (statistical, systems engineering, ML, and artificial intelligence [AI] techniques) will be necessary to develop AID systems with greater than 90% TIR.
Improvement in sensor accuracy, especially in hypoglycemia ranges, may help to improve glycemic management with the use of adjunctive GLP-1RAs by reducing unnecessary insulin suspensions. Sensors should be more accurate to use in AID systems.
Sensors will require significantly less inaccuracy caused by interfering substances for optimal control of an AID.
Sensors for alternate novel biochemical, behavioral, and environmental metrics must be capable of connecting to all AID systems that meet the requirements of integrated CGMs.
AID systems, also known as hybrid closed loop for the current commercial AIDs, have improved the lives of people with T1D. Studies have shown significant increases in the % TIR (70-180 mg/dL) and reduction in the time spent in hypoglycemic and hyperglycemic ranges compared to multiple daily injections and sensor-augmented pump therapy.60,61 As people with T1D become accustomed to the performance of current AID system, there will be a desire for further improvements including methods to further increase in % TIR, eliminate the need for manual entry of meals or to announce exercise, improved diagnosis of faults of the AID system, and mitigation of the effects of unexpected events.
Several approaches have already been proposed to address these needs and have been illustrated in simulation studies and exploratory studies. Two different philosophies have generated alternatives that can be used exclusively or integrated: (1) the use of historical data of a person collected over several weeks to capture the patterns in their sensor glucose in response to various disturbances and start conservative corrective actions when such trends are detected in current data from CGMs; and (2) collection of information from other sensors that report physiological data (usually from wristbands) or multianalyte sensors, interpretation of the data in real time, and initiation actions based on the diagnosis of the source cause of impending or current variations in glucose levels. An example of a wristband used to collect physiological data is shown in Figure 2. With either approach, data should be interpreted by various statistical, systems engineering, and ML techniques to provide information that will lead to alteration of insulin, glucagon, or adjunctive therapy action.
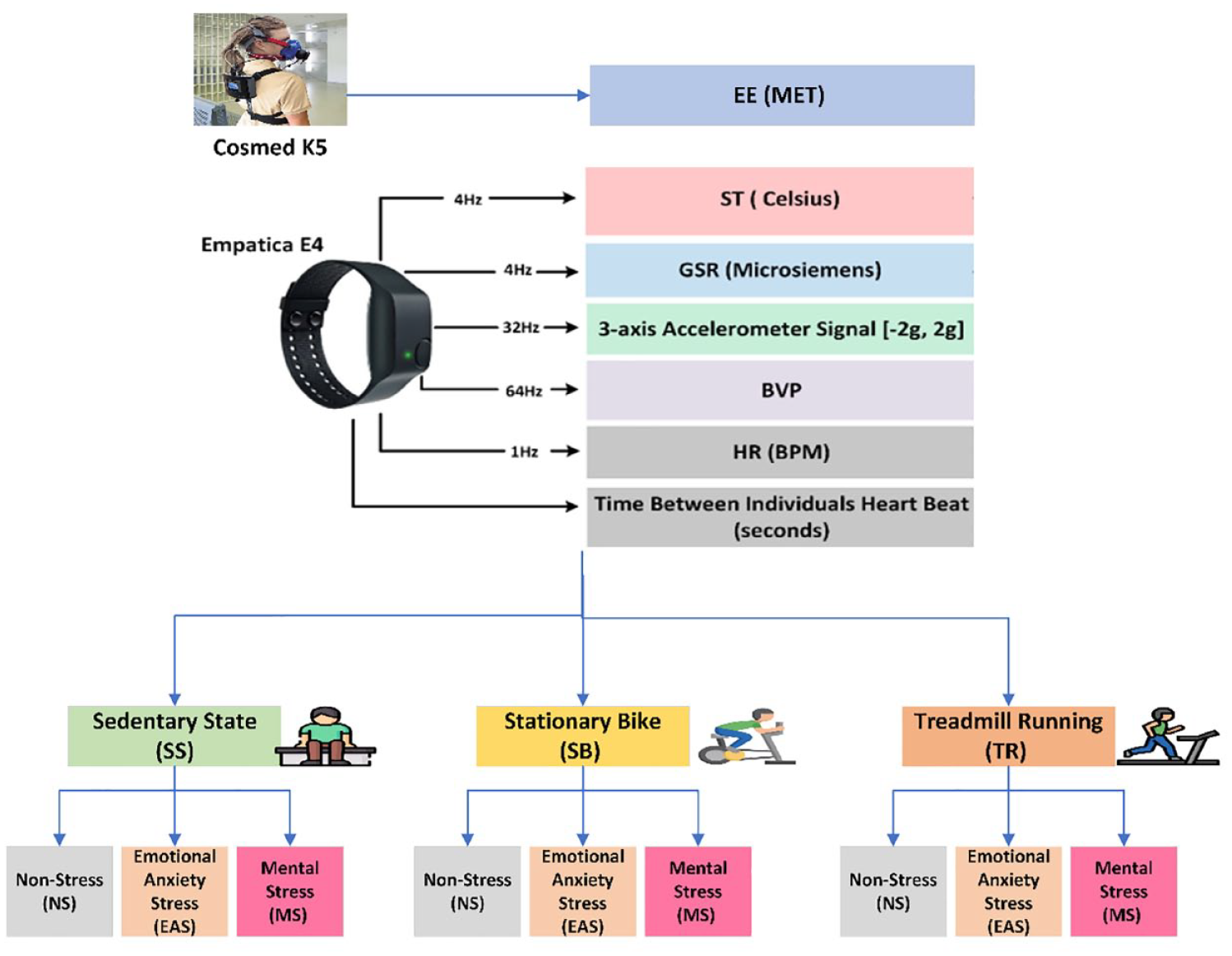
Data collected from a wristband (Empatica E4) for detection of stand-alone or concurrent physical activities and acute psychological stress for use in multivariable AID (mvAID) systems. The interpretation of these signals provides information (presence of physical activity—PA and/or acute psychological stress—APS) well before these factors affect the BGC, reducing the delay in reacting to them by an AID system. COSMED K5 is a portable indirect calorimeter system that generates gold-standard energy expenditure (EE) information. Its results are used only during calibration to assess the accuracy of EE estimated from the E4 wristband data. Empatica E4 measures 4 variables (ST, GSR, 3-axis accelerometer signal and BVP) at frequencies specified in the figure, extracts HR and HR variability from them and report the results to the mvAID. ML modules linked with the mvAID interpret these data, detect the presence of PA and/or APS, and estimate their intensities. The control module of the mvAID (not included in the figure) uses this information for computing the optimal dose of insulin to be infused, stop insulin bolus, reduce basal insulin, and/or modify the target glucose concentration automatically, as appropriate.
For automated meal detection, there are two separate tasks: detection of starting a meal and estimation of the carbohydrates consumed. Three alternative technologies can be used separately or together: wrist movement, sensor glucose trends captured from historical data, and interpretation of real-time CGM data. The first can only detect the start and duration of a meal. The other techniques can also estimate carbohydrate consumption and initiate mini-boluses of insulin to mitigate meal effects.
Other disturbances, such as physical activities, acute psychological stress events, and irregularities in sleep could be captured and quantified more easily from interpreting physiological or hormone data in real time. At present, activity monitors provide reliable and comprehensive physiological data as surrogates for multianalyte sensors that provide hormone data, although such sensors are currently being developed.
Multi-level integration of modeling, detection, and control activities both at the device level (AID pump, smartphone, cloud) and algorithm level (statistical, systems engineering, ML, and AI techniques) would be necessary to develop the next generation of AID systems, with the goal of targeting over 90% TIR.
Section 4: What Is Lacking in AID Systems Therapy in T1D: Better Algorithms
Peter G. Jacobs, PhD1, Rayhan A. Lal, MD2
1Department of Biomedical Engineering, Oregon Health & Science University, Portland, OR, USA
2Division of Endocrinology, Department of Medicine, Stanford University, Stanford, CA, USA
Key points:
Since GLP-1RAs impact gastric emptying, the need for insulin delivery may reduce (similar to pramlintide), especially in the 2 to 4 hours after meal consumption. The impact on delayed gastric emptying may benefit glucose outcomes for meal insulin delivered automatically because of a meal detection algorithm, since less of the meal has been absorbed by the time that the meal insulin is delivered. However, this needs to be studied further.
GLP-RAs may reduce carbohydrates consumption (i.e. quantity per meal and frequency of feeding) because of its effect on satiation and satiety. Future studies tracking nutrient intake with GLP-1RAs and AID systems are required.
Without meal announcements, systems must uptitrate insulin in response to glucose excursions from meals. Determining how and when to decrease insulin delivery is crucial for preventing hypoglycemia. To optimize this reduction, in this context, it is necessary to understand the typical and longest meal absorption times while on GLP-1RAs to optimize glycemia.
Future studies on effects of exercise along with GLP-1RA and AID use are needed.
Current commercial AID systems are superior to either multiple daily injection therapy or conventional therapy but yield only modest improvements in glucose outcomes, reducing HbA1c by 0.2% to 0.5% compared with open-loop pump therapy.63-65 However, the target for people living with T1D is to achieve a HbA1c of under 7% or TIR >70% and time below range (TBR) <4%. 66 Yet, achievement of these glycemic targets has remained elusive for many individuals using AID devices in the real world. In a study by Choudhary and colleagues using the Medtronic Advanced Hybrid Closed Loop system (780G), while improvement was noted in this 3-month RCT that recruited individuals with suboptimal glycemia at baseline (>8%) with a mean reduction in HbA1c of 1.42%, only 27.8% of the participants were able to achieve the glycemic goal of an HbA1c <7%.67,68 Most of the glycemic benefit of AID systems compared with open-loop therapy occurs at night, in the absence of meals. 69 Boughton et al showed that older adults with T1D using AID systems had improved glucose outcomes overall compared with open-loop therapy. However, they had improved glucose outcomes during overnight hours (0000 h-0559 h) compared with daytime hours (0600 h-2359 h), depicted in Figure 3. 70 Most commercial AID systems are hybrid, meaning that people must announce exercise and meals to the system and correctly estimate carbohydrates. People oftentimes forget or are late to announce meals, and carbohydrate estimates are usually incorrect. 71 New AID algorithms can anticipate meals in the future based on patterns from the past 72 and can predict if a meal has occurred and dose a portion of meal insulin when detected. 73 The Medtronic 780g can dose meal automatically if it detects a rapid rise in glucose that may be caused by a meal as shown by Shalit et al. 74 Despite these novel approaches, AID systems may still struggle to perform well because of the slow kinetics of subcutaneously delivered insulin relative to meal absorption. “It is expected that basal insulin modulation of currently available AIDs may adapt to reduced insulin requirement with GLP-1RA use. However, studies are needed to evaluate the functionality and adaptability of these algorithms with changing insulin dose and weight loss with GLP-1RA use in T1D.”
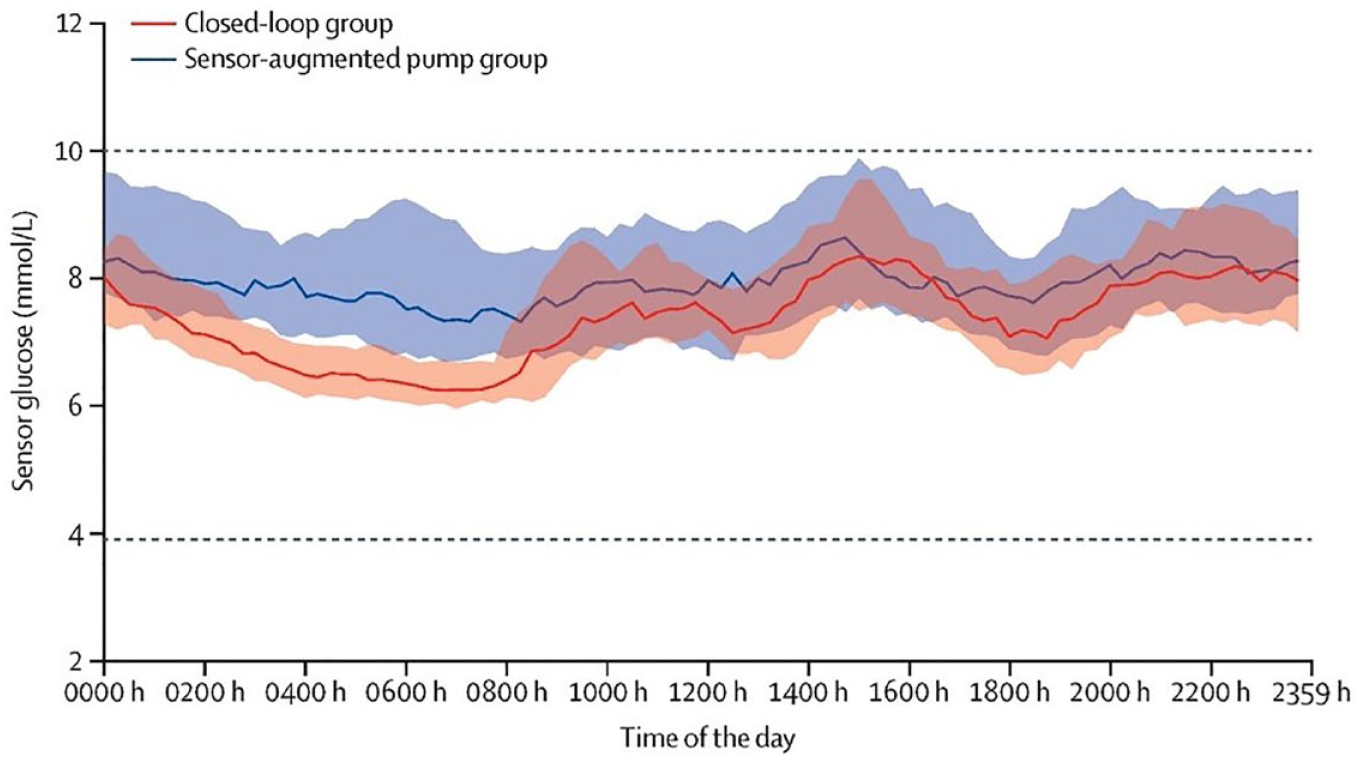
Median and interquartile ranges for older adults on AID versus sensor-augmented pump therapy in a study by Boughton et al 70 showing that the benefit of AID is clearly during the evening hours (0000 h-0559 h) when meals and exercise typically are not occurring.
GLP-1RA adjuncts to AID may help improve glucose outcomes during the daytime (when meals occur) by reducing carbohydrate intake and slowing absorption time. Ilkowitz et al 59 showed that the use of the GLP-1RA liraglutide as a one-time dose of 1.2 mg in combination with the Medtronic Paradigm AID system improved glucose outcomes during the day and postprandially compared with the AID system alone. Postprandial glucose was substantially reduced in the liraglutide arm compared with control, demonstrated in Figure 4. While less insulin was needed in the liraglutide arm, there was not increased hypoglycemia, indicating that the AID system was able to respond appropriately without knowledge that liraglutide was being taken. Sherr et al 58 evaluated how adjunctive therapeutics of pramlintide and liraglutide improved postprandial glucose responses compared with AID systems alone, using a 3- to 4-week outpatient dose titration period to optimize insulin doses and maximize the dose of the adjunctive therapy. They found that liraglutide reduced postprandial glucose area under the curve by 35%. Importantly, as the system relies on total daily insulin dose to determine algorithmic parameters, after inputting a lower total daily dose on the admission with adjunctive liraglutide, there was still a 28% reduction of insulin required in the liraglutide arm of the study, indicating that AID systems may need to be notified that liraglutide is being administered. However, there were again not significantly more hypoglycemia events in the liraglutide arm (8 events) compared with control (7 events). Early results indicate that the use of a GLP-1RA may improve glucose outcomes during the day when meals are occurring. Significantly less insulin appears to be required when using a GLP-1RA with an AID system, indicating that AID algorithms may benefit from GLP-1RA usage.
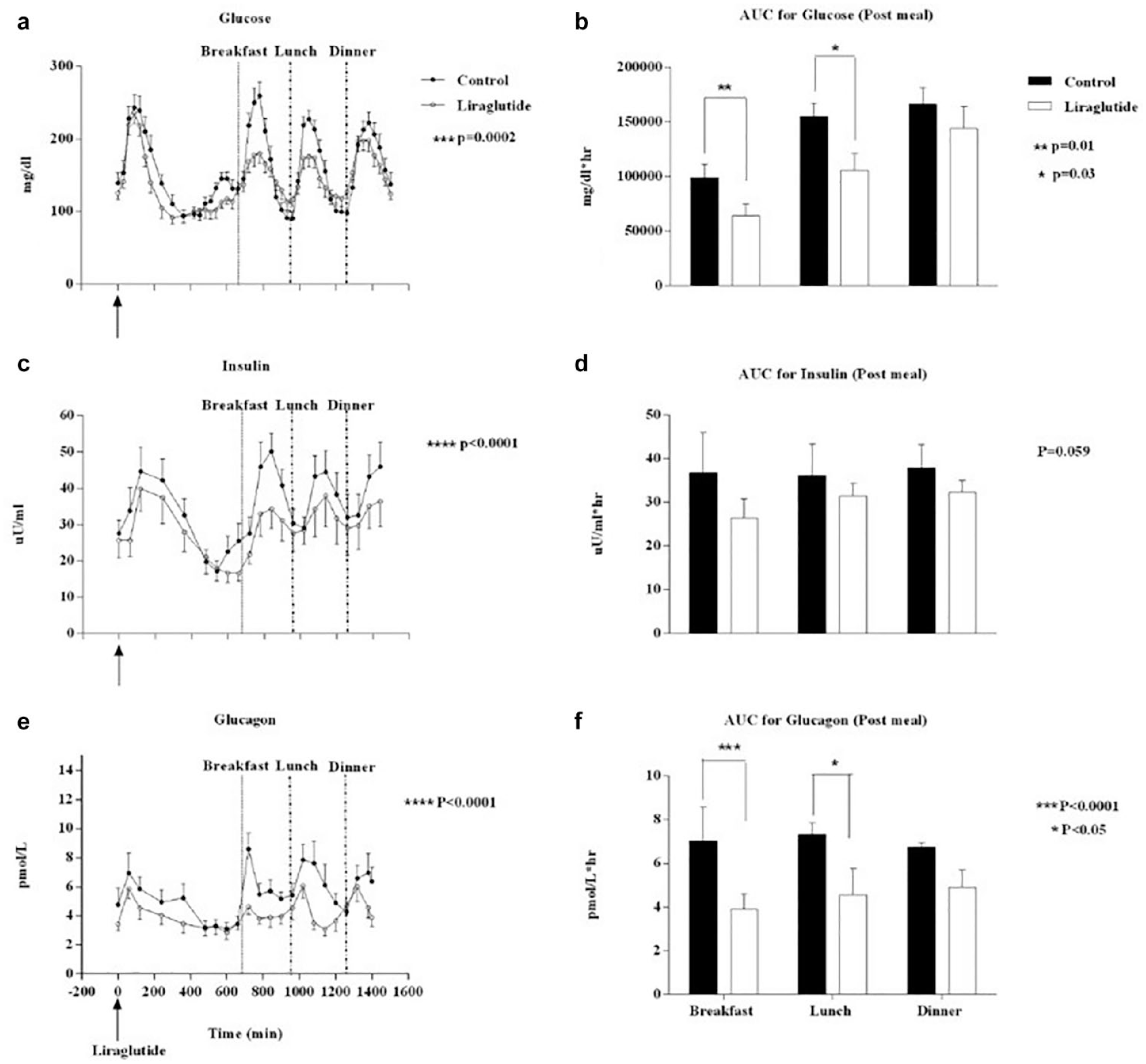
Glucose, insulin, and glucagon responses to meals during the study by Ilkowitz et al. 59 The postprandial glucose response is substantially smaller following administration of a single dose of liraglutide before dinner on the day prior to the measurements of glucose, insulin, and glucagon. Postprandial insulin and glucagon responses levels were also reduced in the liraglutide arm of the study.
Section 5: What Is Lacking in AID Systems Therapy in T1D: Better Insulin
Chiara Fabris, PhD1 and Eric Zijlstra, PhD2
1Center for Diabetes Technology, School of Medicine, University of Virginia, Charlottesville, VA, USA
2Profil, Neuss, Germany
Key points:
Faster insulin analogs may or may not cover rapid changes in glucose levels, and residual risk of hyperglycemia in the early postprandial period and risk of hypoglycemia in the late postprandial period remain. Faster insulin analogs have the potential of simplifying the problem of postprandial excursions, especially in the case of fully-automated insulin delivery.
Current data do not establish superiority of faster insulin either for hybrid or fully-automated insulin delivery systems.
With subcutaneous insulin administration, potential room for further improvement in glucose management may be limited.
Current insulin analogs were designed to primarily target glucose with improved time-action profiles, whereas the impact of insulin use on several other pathophysiological mechanisms in persons with T1D may be limited or even disadvantageous, such as weight gain, decreased risk of hypoglycemia, and cardiovascular benefits.
AID technologies provide the great advantage of adjusting insulin doses based on a feedback loop informed by CGM measurements. While AID systems allow users to obtain targeted glucose levels overnight,69,70 prandial excursions remain a challenge, 71 and even more so as the field progresses toward fully-automated insulin delivery systems.
Challenges related to prandial glucose excursions in the context of AID are associated to the mismatch between timing of insulin action via subcutaneous administration and meal glucose appearance, as the latter is typically characterized by faster rise and decay as compared to the former. This mismatch results in an increased risk of hyperglycemia in the early postprandial period when carbohydrates entering the circulation are not counteracted by sufficient insulin, followed by an increased risk of hypoglycemia in the late postprandial period, because of a relative excess of active insulin. In this context, the use of faster insulin analogs has been explored as a way to reduce the described mismatch.
Multiple formulations of faster insulin analogs are currently available, including inhaled insulins and insulins for subcutaneous delivery with faster pharmacokinetic/pharmacodynamic (PK/PD) profiles. A number of studies have evaluated the benefit of using faster insulin analogs in individuals with T1D, who are using hybrid or fully-automated closed-loop systems, under different experimental settings and across different age ranges.75-81 Overall, data do not show evidence of superiority of faster insulin analogs vs standard rapid-acting insulins when used within AID systems, in terms of glycemic outcomes and quality of glycemia, as presented in Table 3.
Summary of Studies Investigating the Use of HCL and FCL With Faster Vs Standard Insulin Analogs.

Abbreviations: FCL, fully closed loop; HbA1c, hemoglobin A1C; HCL, hybrid closed loop; HCL-A/L, HCL with insulin aspart/lispro; HCL-F, HCL with faster insulin aspart; PPG, postprandial plasma glucose; SC, standard care; TAR, time above range; TBR, time below range; TIR, time in range.
One limitation of the studies investigating the impact of faster insulins in AID systems is the lack of control algorithms optimized for these faster PK/PD profile insulins. Thus, improved glycemic outcomes might be possible with the use of faster insulin analogs combined with optimized controllers. Yet further improvement may be achieved by combining faster insulin analogs and GLP-1RA drugs. GLP-1RAs slow gastric emptying and may further reduce the insulin action-glucose appearance mismatch. GLP-1RAs (and possibly future functionally selective insulins) also have the potential to provide additional benefits such as less body weight gain, decreased risk of hypoglycemia, and cardiovascular benefits, not addressed by current insulin analogs.
Section 6: How Will GLP-1RA Therapy as Adjuvant Therapy With AID Systems Improve Performance in T1D and Which Patients Are Most Likely to Benefit?
Grazia Aleppo, MD1, Eda Cengiz, MD, MHS2, and Anne Peters, MD3
1Division of Endocrinology, Metabolism and Molecular Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA
2University of California San Francisco, San Francisco, CA, USA
3Keck School of Medicine of USC, University of Southern California, Los Angeles, CA, USA
Key points:
The use of GLP-1RA therapy in adjunction to AID may help reduce mealtime insulin requirements and slow the post prandial rate of rise of glucose making AID systems more effective at managing post prandial glucose excursions.
The use of GLP-1RAs combined with AID may be beneficial in improving maximum post prandial glucose concentrations.
The use of GLP-1RA therapy in T1D using AID may require changes in insulin to carbohydrate ratio.
In the setting of GLP-1RA use and AID systems, it is likely that the timing or the type of a meal bolus requires modifications, based on the type of algorithm used (e.g. by implementing extended boluses or dosing insulin post prandially).
The use of GLP-1RA therapy and AID may facilitate weight management in people with T1D, especially those who are overweight or obese.
The use of GLP-1RAs as an adjunct to AID can achieve further cardiovascular and renal benefits in people with T1D.
Reduction of total daily dose could allow patients on pump or pod AID systems and high daily insulin requirement to change their pumps or pods less often.
In addition to the reduction of post prandial glucose concentrations, the use of GLP-1RAs in conjunction with AID therapy may also facilitate reduction of snacking and alcohol intake.
The use of GLP-1RAs in conjunction with AID therapy could change the timing of mealtime dosing, reducing the need for pre-bolusing, and/or allow for post prandial dosing.
The use of GLP-1RAs in conjunction with AID therapy could, in some cases for meals with a reduced carbohydrate content, reduce the need for mealtime insulin completely, if the AID system can adjust for the slight postprandial rise.
The use of GLP-1RAs in conjunction with AID therapy could help individuals who restrict insulin due to fear of weight gain to feel more confident in increasing their insulin doses.
GLP-1RAs in conjunction with AID therapy could allow for an increase in physical activity with a reduction in body weight.
Improve hepatic function in people with metabolic dysfunction associated steatotic liver disease and T1D.
Improve polycystic ovarian syndrome in women with type 1 diabetes.
Data on the use of GLP-1RAs in people with T1D are limited, especially in the setting of AID systems. Previously discussed data on clinical trials in T1D not on continuous subcutaneous insulin infusion (CSII) nor AID systems (see Section 2) revealed glycemic benefits as well as weight reduction.12,13
A study of 44 participants with T1D using CSII plus liraglutide 1.8 mg daily vs placebo plus CSII showed significant reductions in HbA1c and insulin dose (compared to increases for these two outcomes in the placebo plus CSII subjects) and significantly greater total weight loss in CSII users plus liraglutide without an increase in the rate of hypoglycemia. 82 A greater advantage of the use of GLP-1RAs as adjuvant therapy with CSII in T1D was seen when overweight adults were randomized to daily liraglutide 1.8-mg plus CSII vs placebo plus CSII. Total fat and lean body mass decreased in liraglutide-treated participants, and energy derived from added sugars decreased by 27% in the liraglutide arm compared with an increase of 14% in the placebo arm. 83
The advent of AID systems has transformed the approach to insulin therapy in T1D by facilitating greater dosing flexibility, lower hypoglycemia rates, and increased time spent in target range. These sophisticated systems modulate insulin delivery based on CGM input through an algorithm. 84
Recent studies have investigated the effects of adding GLP-1RAs to people with T1D using sensor-augmented pumps or AID systems. In a small study of 11 participants, adding low-dose semaglutide 0.5 mg weekly to the sensor-augmented pump insulin regimen for 6 months resulted in an absolute reduction of 8.8 kg from baseline to end of study; weight decreased from 82.8 ± 10.9 kg at baseline to 76.9 ± 10.6 kg at 3 months (P = .003) and to 74 ± 11.9 kg at 6 months (P = .037) with a relative reduction of 10.6% body weight. Furthermore, a decrease in bolus insulin doses was noted at 3 and 6 months with reduction from 0.28 units/kg/day at baseline to 0.22 units/kg/day at 3 months (P = .006) and 0.24 units/kg/day at 6 months (P = .017). Carbohydrate intake decreased from baseline to month 6 from 131 grams/day to 112 grams/day (P = .01) with a target range remained stable at 73% throughout the study. 85 Two additional retrospective studies have been recently published, in which subjects with T1D overweight or obese were treated with semaglutide and tirzepatide. The semaglutide study was a retrospective case-control analysis where semaglutide had been prescribed and used for at least 3 months, and subjects were followed up for 12 months. In this cohort, 64% of participants in the intervention group used an insulin pump as well as CGM although the specific use of AID systems was not reported. The results showed overall decrease of 0.6% for semaglutide users vs 0.17% (P = .0046) in the control group, an overall decrease of BMI of 1.44 vs 0.2 (P = .0029), a change in weight of 8.4 lbs. vs an increase of 0.53 lbs. (P = .0009). Both parameters improved overtime with the greatest changes present at 12 months. Furthermore, CGM parameters also showed an increase in TIR and decrease in time above range. No total insulin dose reduction was noted between groups (P = .1099). 49 Similarly, the Tirzepatide study followed up with T1D subjects who were overweight or obese for 1 year. In this retrospective study, 83% of the participants were using an insulin pump or an AID system. At 12 months, the overall change in BMI was 6.5% in the tirzepatide group, with a weight reduction of 46.5 lbs., a 18% reduction in weight, and a change in total insulin dose of 22.8 units (all P < .0001). The reduction in insulin dose at 12 months was −9.1 ± 8.8 units/day for basal (P < .0001) and 13.7 ± 14.4 units/day for bolus (P < .05). 86
Although the data on GLP-1RA use in T1D have not yet studied a cohort using only AID systems, these recent studies emphasize the potential role of GLP-1RAs in T1D using AID systems where the CGM-modulated insulin dose delivery could potentially mitigate the reported increases in hypoglycemia risk from ADJUNCT ONE and TWO trials where insulin doses could not be decreased in real time with impending hypoglycemia.12,13 Of note, the increase in hypoglycemia risk was not seen in two studies using CSII,82,83 nor in the more recent studies.49,85,86 In people with T1D wearing AID systems, the adjunctive use of GLP-1RAs could provide multiple benefits: (1) weight reduction, especially if the individual with T1D is overweight or obese; (2) reduction of total daily insulin dose; (3) reduction of postprandial glucose elevations; and (4) reduction of total carbohydrate intake.83,85 An example of the potential benefit of GLP-1RAs in people with T1D using AID systems is portrayed in Figure 5. Similarly, the use of GLP-1RAs could also (1) permit modifications of various AID settings such as insulin to carbohydrate ratios and (2) type and timing of meal boluses delivered, to optimally match the timing of insulin action and food absorption. Severe insulin resistance can limit the feasibility of AID in some patients because of high insulin requirements that exceed the capacity of the reservoir or maximum bolus. This results in more frequent infusion site changes or off-label use of concentrated insulins. Adjunctive GLP-1RAs could mitigate this problem.
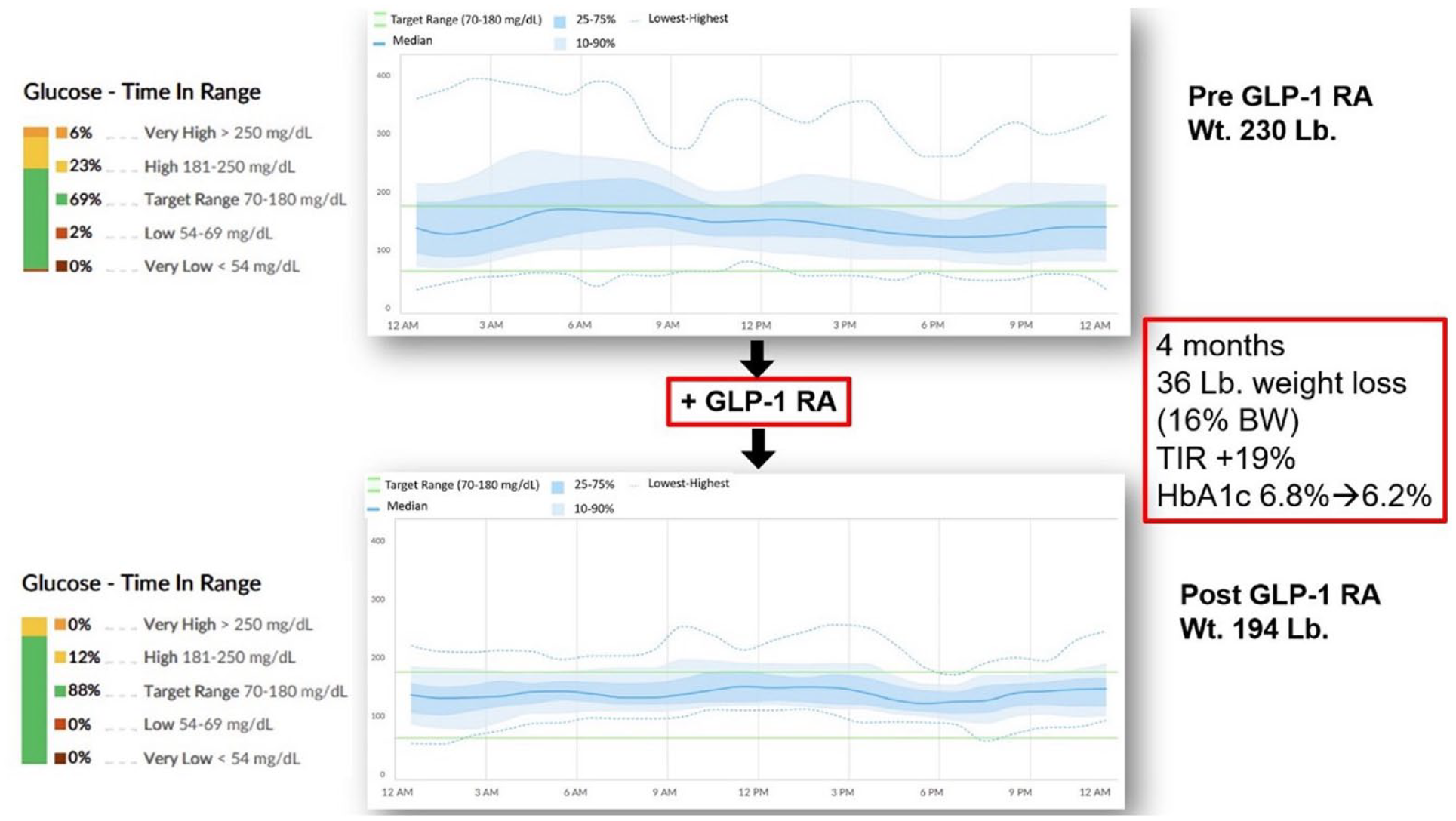
Example of potential GLP-1RA benefit in people with T1D using AID systems. Over 4-month use of a GLP-1RA, HbA1c decreased by 0.6%, weight decreased by 36 lbs. or 16% body weight, and percent in time in target range (TIR, 70-180 mg/dL) increased by 19% (BMI decreased from 31 kg/m2 to 26 kg/m2).
Future fully-automated insulin delivery systems equipped with algorithms to anticipate meal events might optimize glycemic management even better when they are combined with GLP-1RA treatment. Further research is needed to understand GLP-1RAs’ full potential in cardiovascular-renal risk reduction when used in adjunct with AID to expand the therapeutic indications and to determine their optimal use in clinical practice.
Section 7: What Are the Knowledge Gaps, Controversies, and Recommendations for Research in the Use of GLP-1RAs as Adjuvant Therapy With AID Systems in T1D?
Lia Bally, MD, PhD1, Kathleen Dungan, MD, MPH2, and Guillermo E. Umpierrez, MD, CDCES, FACE, MACP3
1Inselspital, University Hospital of Bern, University of Bern, Bern, Switzerland
2Division of Endocrinology, Diabetes and Metabolism, College of Medicine, The Ohio State University, Columbus, OH, USA
3School of Medicine, Emory University, Atlanta, GA, USA
Key points:
The use of CGMs and/or AID systems may mitigate the risk of hypoglycemia associated with GLP-1RA-based therapy.
Long-acting GLP-1RAs may improve postprandial glucose excursions because of effects that are independent of changes in eating behavior (e.g. slowing of gastric emptying and inhibition of glucagon).
The effect of GLP-1RAs on peak bone mass attainment when used in children and/or adolescents requires further research.
GLP-1RAs harbor immunomodulatory properties, which may support functional beta-cell mass in newly diagnosed people with T1D using AID systems.
The long-term cardiovascular safety of GLP-1 based therapy in T1D needs further investigation.
Data on efficacy/safety of newer GLP-1 based therapies in people with T1D are lacking.
The appropriate insulin dose adjustment strategy for persons with T1D beginning GLP-1-based therapy has yet to be established.
Despite advancements in insulin delivery devices, many individuals with T1D struggle with postprandial glucose excursions. It is likely that GLP-1RA-based therapy may reduce post prandial glucose excursions in people with T1D using AID systems.
GLP-1RA therapy may decrease basal and prandial insulin doses in persons on AID systems. Thus, there is a need to understand the appropriate insulin dose adjustment strategy for persons with T1D beginning GLP-1 based therapy.
GLP-1RAs may result in weight loss and reduction of HbA1c, particularly in individuals with T1D who are overweight or obese. It is unknown whether weight loss is magnified in persons using AID systems.
The use of GLP-1RAs as an adjunct to AID treatment offers new avenues in the care of people with T1D, but several research gaps remain and are outlined in Table 4. In T1D, GLP-1RAs influence glucose levels by altering eating behavior and glucose absorption kinetics. 54 Because short-acting GLP-1RAs have a more enduring effect on postprandial hyperglycemia than long-acting agents, studies are required to determine whether the added complexity of short-acting agents outweighs the benefits. Potent long-acting GLP-1RAs may induce substantial weight loss and, consequently, reduce insulin requirements. This may be beneficial for people with excess body weight. However, decreased appetite and gastrointestinal side effects may be undesired in people with normal weight or in children and adolescents given the growth and development associated with this age. Given that the risk of fractures in people with T1D is 2 to 5 times higher than 87 that in the general population, 88 GLP-1RA-induced weight loss, particularly in elderly people with T1D, may negatively affect bone and muscle health.89-91 Lowering insulin requirements may predispose to hypoglycemia if insulin dosing is not adjusted properly. 12 Although AID systems may mitigate against GLP-1RA-associated hypoglycemia, prolonged periods of insulin suspension or reduced delivery can increase the risk of diabetic ketoacidosis. 13 Thus, optimal mitigation strategies, including appropriate device-specific adjustment of settings and sick day protocols, are needed.
Research Agenda.

Abbreviations: AID, automated insulin delivery; GLP-1RA, glucagon-like peptide-1 receptor agonist; T1D, type 1 diabetes; TAR, time above range; TBR, time below range; TIR, time in range.
Another area of uncertainty is whether certain subpopulations of people with T1D using AID benefit more than others, such as those with residual C-peptide, obesity, high insulin requirements, or cardiac risk factors. 92 In T2D and people with overweight and obesity, GLP-1RAs have assumed a prominent role in treatment guidelines because of their beneficial cardiorenal effects in clinical trials. 87 Although cardiovascular and CKD comorbidities in middle-aged and older people with T1D are still unacceptably high, 93 cardiovascular and renal outcome trials in people with T1D using GLP-1RAs are lacking. The use of GLP-1RAs was significantly associated with an elevated risk of diabetic retinopathy in some, but not all, analyses of studies involving persons with T2D.94,95 This is most likely explained by rapid glycemic improvement; in the SUSTAIN-6 trial, the increase in risk was eliminated after controlling for change in HbA1c; moreover events were observed mainly in individuals with >1.5% reduction in HbA1c who had pre-existing retinopathy. 96 Nevertheless, whether the use of AID may further aggravate this complication by acting synergistically on glucose control remains to be investigated. 96 Caution is advised with the use of GLP-1RAs in people with gastroparesis—a diabetes-related complication that is more prevalent in people with T1D than in those with other forms of diabetes. 97 GLP-1RA-induced weight loss, particularly in older people with T1D, may raise concern for negative effects on bone and muscle health, yet some studies show possible benefit. Moreover, the long-term effect on peak bone mass and growth in adolescents is largely unknown. 98 Although no prospective randomized controlled trial in T1D of withdrawing GLP-1RAs prior to surgery has been conducted, a real-world evidence study in T2D showed no increased risk of peri- or post-operative complications associated with the use of GLP-1RAs prior to surgery. 99 Finally, an interesting avenue is the use of GLP-1RAs in people with antibody-positive asymptomatic or newly diagnosed T1D given their potential immunomodulatory and β-cell-preserving effects. 100
Section 8: What Should Be the Role of GLP-1RAs With AID Systems in T1D?
Viral N. Shah, MD1 and Jennifer L. Sherr, MD, PhD2
1Division of Endocrinology & Metabolism, Indiana University School of Medicine, Indianapolis, IN, USA
2Yale University, New Haven, CT, USA
Key points:
AID systems provide a more physiologic means of insulin delivery. They have been shown to improve glycemic outcomes in people with T1D and are the standard of care for managing T1D.
Glycemic improvement with AID systems is mainly observed during nighttime. Even with AID, achievement of glycemic targets remains a struggle during the daytime, and the problem is largely related to meal-related glucose excursions.
GLP-1RAs have the potential for improving AID outcomes further by improving insulin sensitivity, reducing total daily insulin requirements, and optimizing post prandial glycemia.
The majority of adults living with T1D have a concomitant diagnosis of being overweight or obese.
Given the mechanism of action of GLP-1RAs, appetite suppression, and weight reduction accompany improvement in glycemia. Furthermore, the cardiorenal benefit derived from GLP-1RAs have led to their consideration as a first-line therapy for those living with T2D and/or obesity.
Intensive insulin therapy has been associated with increased risk of severe hypoglycemia. 101 CGMs and AID systems have been shown to improve glycemic outcomes without increasing the risk of hypoglycemia in people with T1D across all ages. 102 With overwhelming evidence to support these technologies, the American Diabetes Association Standards of Care 2024 recommends the use of AID systems for the management of T1D. 1
Despite increasing the use of AID systems for T1D management, only 30% to 50% of people with T1D are able to achieve the glycemic targets recommended by the American Diabetes Association with a goal of HbA1c <7%.3,103,104 The difficulty with attaining more targeted glycemia is multifactorial; however, two factors are likely most instrumental with this struggle. First, postprandial glycemic excursions remain exaggerated, even with the use of current generation AID systems, as these systems require user-initiated meal boluses for optimal outcomes.65,105,106 Second, the prevalence of overweight and obesity is increasing among people with T1D, which is associated with insulin resistance, higher insulin requirements, and suboptimal glycemia. 107 Indeed, the frequency of overweight and obesity for those living with T1D mirrors the picture seen in the general population.33-35 Therefore, there is a need for an adjunct therapy to reduce weight, insulin resistance, and meal-related glycemic excursions in people with T1D. Several therapies have been studied as potential adjuncts to insulin therapies in T1D including metformin, dipeptidyl peptidase-4 agonists, sodium glucose co-transporter 2 inhibitors, and GLP-1RAs.107,108 Metformin and Dipeptidyl Peptidase-4 agonists have very modest effects on weight and HbA1c. 108 Sodium Glucose co-transporter 2 inhibitors have been shown to improve glycemia significantly, but the use of this class of medications is associated with increased risk of diabetic ketoacidosis.109-111 Thus, enthusiasm is tempered for this therapy, and it has not been approved by the FDA for management of T1D.
Newer-generation GLP-1RAs such as semaglutide and tirzepatide were initially approved for management of T2D, and the indication has now been expanded to those with obesity regardless of whether there is a comorbid diagnosis of diabetes. In addition, these agents have been shown to reduce adverse cardiovascular and renal outcomes. Small pilot studies in participants with T1D using an AID system have documented improvement in mean glucose and % TIR with short-term use of liraglutide.59,58 Yet liraglutide had no effect on plasma glucagon during mixed meal tolerance tests, 112 suggesting that GLP-1RAs may not blunt dysregulated glucagon secretion in response to meals. 112 Previous studies with the use of GLP-1RAs in participants with T1D using AID systems are limited by small sample sizes and short durations of combined AID system and GLP-1 use (only a few days),59,58 with one of the trials utilizing an outpatient dose titration phase to optimize the dose. 58 Therefore, these feasibility trials are unable to provide evidence for long-term efficacy and safety of GLP-1RAs in individuals with T1D using AID systems.
A few real-life studies in people with T1D have shown improved HbA1c without an increase in the risk of hypoglycemia or diabetic ketoacidosis with the use of GLP-1RAs.113-115 Thus, to tackle the issues likely underlying the inability for more people with T1D to achieve glycemic targets despite the increased use of advanced technology, the time is now to conduct randomized trials of GLP-1RAs as an adjunct therapy in people with T1D regardless of insulin delivery modality.
Discussion
GLP-1RAs administered weekly are increasingly used to treat T2D. Their target site of action affects the gastrointestinal system, the islet cells, and the brain. Two drugs in this family (semaglutide 116 and tirzepatide) 117 have also been approved for chronic weight management in overweight or obese individuals. One of them (semaglutide) is approved to reduce the risk of serious heart problems in adults with obesity or overweight. However, no medication in this class is approved for the treatment of T1D.
Two pivotal trials of a daily GLP-1RA (liraglutide) as adjunct therapy for T1D published in 2016 (ADJUNCT ONE 12 and ADJUNCT TWO) 13 failed to demonstrate sufficient safety and effectiveness to gain FDA approval, and no pivotal trials for GLP-1RA in T1D have been conducted since. The two trials reported hypoglycemia, hyperglycemia, and ketoacidosis in numbers that the FDA considered to be too high.
Meanwhile, after the two liraglutide trials were conducted, CGMs have become widely used and continuous ketone-monitoring systems are under development.118,119 Based on their mechanisms of action, GLP-1RAs should have a place in the treatment of T1D and this international consensus group of experts in treating diabetes thought that this family of drugs would be particularly useful in people with T1D using an AID system. The 30 conclusions made by the panelists, each endorsed by at least 80% of the panelists, related to the mechanisms of action of GLP-1RAs, their potential use in people with T1D, and their potential use in people with T1D using an AID system. The group felt that if GLP-1RAs can be demonstrated to be effective in this subset of people with T1D, then it will be more likely that they can eventually be widely approved for all people with T1D. The widespread use of CGMs in people with T1D makes it likely that the benefits of this family of drugs will not be offset by hypoglycemia or hyperglycemia because these conditions can be identified with the use of CGMs. Furthermore, when CGMs are used as a foundational component of an AID system, hypoglycemia and hyperglycemia may be prevented because of algorithmic alterations in insulin delivery. Hence, compared to the time when ADJUNCT ONE and TWO were conducted, today we are in a new world where sensor use is commonplace, and we have more advanced insulin delivery methods. We encourage the pharmaceutical industry to test these GLP-1RA drugs once again in people with T1D using an AID system, so that these individuals may have an opportunity to use these agents if they prove to be safe and effective upon review by regulatory bodies.
Consensus Group Conclusions
Thirty-Two Recommendations About GLP-1RAs With AID Systems in T1D
The panelists voted on 32 proposed recommendations. Based on the panel vote, 31 recommendations were classified as either strong (80%-100% concurrence) or mild (60%-79% concurrence). One recommendation failed to reach consensus. The consensus panel’s recommendations are presented in Table 5.
Consensus Recommendations on GLP-1RAs as Adjunctive Treatment for Individuals With T1D Using an AID System by the Consensus Panel.

Footnotes
Acknowledgements
The authors acknowledge Annamarie Sucher-Jones for her editorial expertise.
Correction (November 2024):
Abbreviations
AI, artificial intelligence; AID, automated insulin delivery; BMI, body mass index; CGM, continuous glucose monitor; CKD, chronic kidney disease; CSII, continuous subcutaneous insulin infusion; CVD, cardiovascular disease; DTS, Diabetes Technology Society; FDA, United States Food and Drug Administration; GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide-1; GLP-1RA, glucagon-like peptide-1 receptor agonist; HbA1c, hemoglobin A1C; ML, machine learning; PD, pharmacodynamic; PK, pharmacokinetic; T1D, type 1 diabetes; T2D, type 2 diabetes; TBR, time below range; TIR, time in range.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VNS received research support from Novo Nordisk, Insulet, and Tandem Diabetes Care and received honoraria from LifeScan for advisory board attendance and from Dexcom, Embecta, and Insulet for speaking arrangements. ALP is on the advisory board of Medscape, Vertex, and Lilly; has received research support from Insulin and Abbott; and reports stock options from Omada Health. GEU has received research support (to Emory University) from Abbott, Bayer, Dexcom, and Sanofi. HKA received research support through University of Colorado from Dexcom, Tandem Diabetes, Senseonics, Medtronic, Eli Lilly, REMD Biotherapeutics, IM Therapeutics, and IAFMS and received honoraria through University of Colorado from Senseonics and Mannkind for advisory board attendance. GA has received research support to her institution Northwestern University from Fractyl Health, MannKind, Insulet, Tandem Diabetes, and Welldoc. GA has received consulting fees from Dexcom and Insulet. LB reports having participated in advisory boards of Eli Lilly, Novo Nordisk, Oviva, Roche Diabetes Care, Sanofi, and Ypsomed and received speaker fees from Dexcom, Ypsomed and Oviva. EC is an advisory board member and consultant for Novo Nordisk, Eli Lilly, Adocia, MannKind, Lexicon, Arecor, PortalInsulin, and Proventionbio. EC was also a speaker for Novo Nordisk. KD discloses research support from Dexcom, Sanofi, Viacyte, Abbott, and Insulet; consulting with Eli Lilly, Insulet, Oppenheimer, Dexcom; and honorarium from UptoDate, Medscape, Med Learning Group, Impact Education, and Elsevier. CF receives royalties from Dexcom and Novo Nordisk managed through her institution. PGJ reports receiving grants from the National Institutes of Health, The Leona M. and Harry B. Charitable Trust, the Juvenile Diabetes Research Foundation, Dexcom, and the Oregon Health & Science University Foundation; consultancy fees from CDISC; US patents 62/352,939, 63/269,094, 62/944,287, 8810388, 9,480,418, 8,317,700, 61/570382, 8,810,388, 7,976,466, and 6,558,321; and reports stock options from Pacific Diabetes Technologies, outside submitted work. RAL reports consulting fees from Abbott Diabetes Care, Biolinq, Capillary Biomedical, Deep Valley Labs, Gluroo, PhysioLogic Devices, ProventionBio, and Tidepool. JKM is a member of the advisory board of Abbott Diabetes Care, Becton-Dickinson, Boehringer Ingelheim, Eli Lilly, Embecta, Medtronic, Novo Nordisk A/S, Prediktor A/S, Roche Diabetes Care, Sanofi-Aventis, and Viatris and received speaker honoraria from Abbott Diabetes Care, AstraZeneca, Boehringer Ingelheim, Dexcom, Eli Lilly, Menarini, MSD, Novo Nordisk A/S, Roche Diabetes Care, Sanofi, Servier, and Ypsomed. JLS has conducted clinical trials for Eli Lilly, Insulet, and Medtronic and has received in-kind support for research studies from Dexcom and Medtronic. She has consulted for Eli Lilly, Lexicon, Medtronic, and Sanofi. She has been a member of advisory boards for Bigfoot Biomedical, Cecelia Health, Eli Lilly, Insulet, the T1D Fund, and Vertex. DCK is a consultant for Afon, Better Therapeutics, Integrity, Lifecare, Nevro, Novo, Samsung, and Thirdwayv. AC, UM, PP, SS, EZ, CNH, ATA, TT, and REA have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.