
Abstract
The quality of clinician-patient relationship is integral to patient health and well-being. This article is a narrative review of published literature on concordance between clinician and patient perspectives on barriers to diabetes technology use. The goals of this manuscript were to review published literature on concordance and to provide practical recommendations for clinicians and researchers. In this review, we discuss the qualitative and quantitative methods that can be applied to measure clinician and patient concordance. There is variability in how concordance is defined, with some studies using questionnaires related to working alliance, while others use a dichotomous variable. We also explore the impact of concordance and discordance on diabetes care, barriers to technology adoption, and disparities in technology use. Published literature has emphasized that physicians may not be aware of their patients’ perspectives and values. Discordance between clinicians and patients can be a barrier to diabetes management and technology use. Future directions for research in diabetes technology including strategies for recruiting and retaining representative samples, are discussed. Recommendations are given for clinical care, including shared decision-making frameworks, establishing social support groups optimizing clinician-patient communication, and using patient-reported outcomes to measure patient perspectives on outcomes of interest.
Introduction
The clinician-patient relationship and patients’ participation in their own care have been recognized as central to outcomes for decades. 1 Patient-clinician concordance is a key aspect of this relationship. Patient-clinician communication quality can impact health outcomes, patient emotional well-being, and pain control. 2 A number of studies have described the impact of patient-clinician agreement and disagreement on health-related outcomes. A systematic review of interpersonal interventions aimed at improving the patient-clinician relationship found several benefits, including benefits to multiple health outcomes (e.g. physical function, mental health, and weight management) and improvement in both patient and clinician experience. 3 The patient-clinician relationship is crucial to both health outcomes and patient experience. In this publication, we present the current evidence based on measuring concordance and its role in diabetes management, with additional focus on the role of sociodemographic concordance and concordance in diabetes technology research.
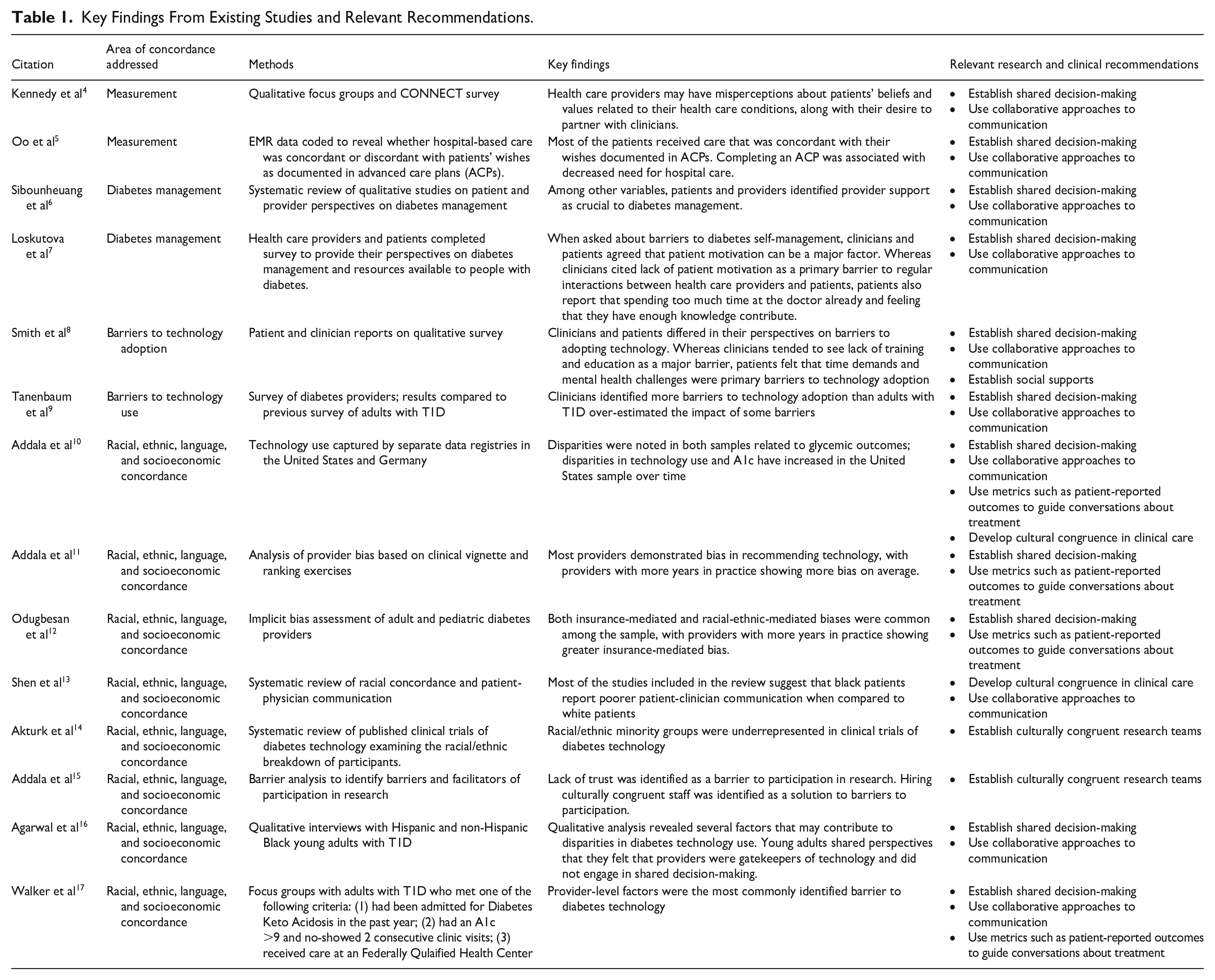
This publication is a narrative review of the literature on concordance and discordance in clinician and patient perspectives on barriers to technology use. Goals were to (1) review methods for measuring concordance and discordance between clinicians and patients; (2) review the literature on the relationship between clinician-patient concordance and technology use, taking into account disparities in technology use and sociodemographic congruence between clinicians/researchers and patients; and (3) provide recommendations for future work in research and clinical care. A summary of relevant literature and conclusions can be found in Table 1. We conclude with evidence-based strategies to incorporate concordance in a variety of clinical care scenarios (Figure 1).
Key Findings From Existing Studies and Relevant Recommendations.
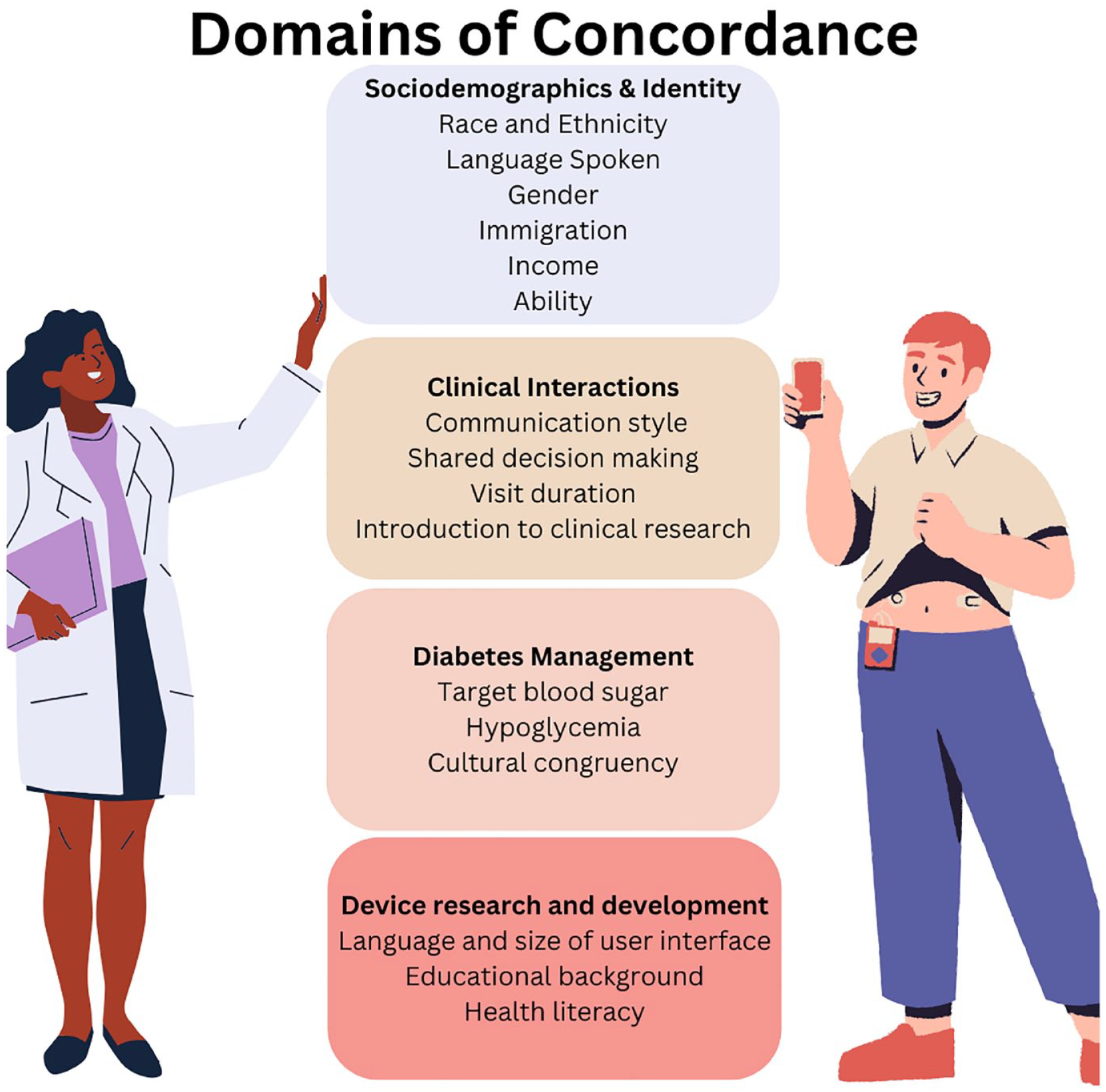
Domains of concordance between clinicians and persons with diabetes.
Measuring Concordance and the Impact on Health Outcomes
Patient and clinician agreement, or concordance, is one aspect of the patient-clinician relationship. Patients and clinicians may agree or disagree on various aspects of care, including treatment regimens, barriers to care, or the importance of social support. Previous studies have measured patient and clinician concordance and discordance using both qualitative and quantitative methods. Using questionnaires and qualitative focus groups, one study was able to measure the discordance in clinician and patient perspectives. Patient and clinician responses had differing reports on the patients’ beliefs about their health condition and values, including patients’ desire for partnership with their health care providers. 4 Another study measured concordance between patients’ preferences for care as documented in advanced care plans (ACPs) and their hospital-based care over the subsequent 12 months. 5 In this study, concordance was measured on a binary of either concordant or discordant with data collected from both ACPs and medical records. The authors determined whether ACPs and patient care were concordant (no deviations in patient wishes and medical care as documented in the medical record) or discordant (deviations between patient wishes and medical care). Using questionnaires, they were able to discover that more than 75% of their sample received care that was fully concordant with their preferences as stated in ACPs. The use of these methods can expose the unity in patient-clinician relationships.
These methods are not only important in measuring the concordance between clinicians and patients, but also the relationship quality. The idea of a “working alliance” between clinician and patient has been in psychotherapy literature for decades. Working alliance refers to the degree of collaboration between a therapist and patient and is believed to be central to positive change in therapy. 18 The concept of a working alliance has also been applied to the physician-patient relationship. Working alliance can be measured via a questionnaire. In the psychotherapy literature, the working alliance inventory 19 (WAI) measures therapist-patient working alliance; the Physician Patient Working Alliance Inventory (PPWAI) measures working alliance between physicians and their patients. 6
There are limitations in current methods used to measure concordance between health care providers and patients. Some studies have used a dichotomous variable of concordant or discordant. 5 Although this captures whether patient preferences have been met, additional aspects of concordance may be missing. These can include the measure of the extent to which patients feel heard or understood by their care provider or their impression that there is a working alliance between patient and caregiver. Many studies may use one measure of discordance instead of multiple methods, limiting the conclusions that can be drawn.
Concordance in Diabetes
Literature on diabetes demonstrates that clinician and patient perspectives may vary, and clinicians may be unaware of their patients’ beliefs and perspectives. A systematic review of qualitative studies of patients with type 2 diabetes, and their providers revealed that whereas clinicians and patients expressed similar perspectives on many aspects of diabetes management, some nuances point to discrepancies in perspectives and challenges in the clinician-patient relationship. Themes related to lifestyle modification and diabetes self-management revealed that clinicians may feel frustrated when they cannot help patients meet their goals or perceive that patients are not motivated for change. One subtheme highlighted the importance of clinician communication, with many patients reporting that their clinician had poor communication skills and lectured them rather than talking to them. Patients also emphasized needing to have health care providers who understand and support them. 6 These findings demonstrate that clinicians and patients may have varying perspectives on diabetes care that go unaddressed. Furthermore, patients may perceive clinician characteristics as a barrier to effective care.
Concordance and Barriers to the Adoption of Diabetes Technology
Clinicians may not be aware of patients’ perspectives on barriers to diabetes care and technology use. One study elicited both patient and clinician perspectives on diabetes management. Patients found it difficult to engage in conversations with health care providers related to their diabetes, reporting that they feel that they already know a lot, are working hard, and spend a lot of time at doctor’s appointments. 7
Clinicians and patients may perceive a variety of barriers to diabetes technology use. One study found that clinicians and patients differed in their perspectives on the most important barriers to adopting technology. 8 However, clinicians thought that a lack of knowledge, feeling overwhelmed, and needing more support were barriers to adopting technology, patients felt that technology was a time commitment, interfered with other responsibilities, and cited difficulty with mental health concerns as barriers to technology use. In another study, clinicians over-approximated the barriers to starting diabetes technology, including cost and insurance considerations, lack of knowledge of what to do with technology, and on-body experience. 9 These discrepancies may contribute to suboptimal outcomes for the patients. For instance, clinicians perceiving cost or insurance to be prohibitive to technology use may not present technology as an option to their patients. Furthermore, clinicians may provide education centered on barriers that are not relevant to their patients, waning their interest in the devices.
Racial, Ethnic, Language, and Socioeconomic Concordance
Three emerging and contemporaneous phenomena in type 1 diabetes (T1D) underscore the need to understand and address sociodemographic congruence between clinicians and individuals living with T1D. First, the incidence of T1D is rising preferentially in individuals of minoritized racial ethnic backgrounds, thereby diversifying the face of T1D.20,21 Second, disparities in diabetes management including technology access and utilization have been worsening over the last decade, driven in part by clinician and researcher bias.10-12,22 Disparities are most apparent in the study and use of diabetes digital technology which is associated with improvements in glycemic outcomes and in quality-of-life measures.23-26 Third, diversifying the recruitment into medicine and research is recognized as a sustainable solution to address the many drivers of health disparities.27-30 The negative impact of racial, ethnic, language, and socioeconomic discordance between clinicians and persons with T1D is seen as propagating disparities in diabetes technology.
The current work force is not representative of the individuals living with T1D. 22 Sociodemographic concordance between a clinician and the individual living with a long-term condition is a well-established protective factor for improved outcomes; however, it is underutilized as a solution to improve health outcomes. Studies in a broad range of medical fields and medical education support diversifying workforce to improve health outcomes. This is primarily because of the key role social determinants of health and implicit bias play in health outcomes and the inherently protective effect of a diverse workforce to counter these factors. 22 Diversifying the pipeline into clinical care is a well-established solution that addresses upstream drivers of disparities and improves clinical engagement.27-30 Sociodemographic discordance between clinicians and individuals with long-term conditions is associated with decreased satisfaction in the clinical care received, poorer communication, decreased quality of clinical interactions, shorter visits, and less shared decision-making. 13 Although underexplored in T1D and technology use, a parallel presents itself on the impact discordance has on the initiation and sustained use of diabetes technology. Shorter visits, poorer communication, less shared decision-making, and poorer satisfaction with clinical care all add to lower uptake of diabetes technology in minoritized families.
Lack of researcher and person-with-diabetes concordance is a likely driver of disparities in clinical research participation of diabetes technologies. Most of the current diabetes-specific researches are not representative of the individuals living with T1D.14,31 Inequities in clinical research recruitment and participation continue to result in the systematic underrepresentation of racial/ethnic minority, low socioeconomic, and publicly insured groups, particularly in digital health technologies.14,32 This gap in diverse representation in research is a moral, ethical, and scientific concern, as clinical research drives the application of innovative, cutting-edge therapies in the studied subgroups. 33 Furthermore, a lack of disease-representative recruitment and retention into clinical research has historically contributed to a variety of adverse health outcomes in understudied groups.34-36 Lack of diversity in investigators further compounds this disparity in research37,38 particularly given the positive impact that congruent research and clinical personnel have on participant engagement and health outcomes.39,40
Individuals living with diabetes recognize the impact of discordance by key sociodemographic identities. This manifests as mistrust, lack of autonomy over one’s diabetes care and management, and the experience of discrimination for individuals and families living with T1D.15-17 For clinicians, this often manifests as racial and insurance-mediated implicit biases against recommending diabetes technology.11,12 Thus, concordance in clinicians, who determine the provision of clinical care and research participation, can have a significant impact on equitable distribution and utilization of diabetes technology.
Concordance and Future Diabetes Technology Research
Diabetes technology studies are generally not representative of the population living with T1D, often under-representing individuals from minoritized backgrounds. 14 A lack of disease-representative recruitment and retention into clinical research has historically contributed to a variety of adverse health outcomes in understudied groups.34-36 Lack of diversity in investigators further compounds this disparity in research37,38 particularly given the positive impact that congruent research and clinical personnel have on participant engagement and health outcomes.39,40 Taken together, concordance for effective diabetes technology research can be operationalized into concordance of two groups, the population recruited and the researchers, to reflect the population with living with T1D.
Ensuring concordance between the population recruited and the population living with T1D requires a multipronged solution; however, these strategies are both under-studied and under-reported. Clinicians and researchers can use the electronic medical record to systematically identify all eligible participants. Once identified, a concordant research staff member can approach the participant for a culturally and linguistically congruent recruitment effort. Key in this approach is ensuring that all eligible participants are approached, irrespective of clinician or researcher perspective of the individual’s readiness or interest in participation. Partnering with community organizations and community health centers is a helpful strategy as these organizations often have authentic and accurate awareness of the local needs. 15 With concordant clinical trial cohorts, researchers, clinicians, and device manufacturers are likely to receive feedback and insights that will result in the development of diabetes technologies that are effective to a diverse group. To encourage concordant clinicians and researchers into diabetes care and diabetes technology research, institutions, funders and industry must all proactively sponsor diverse individuals into the field.
Currently concordance is not evaluated systematically in diabetes research. Incorporating the measures to evaluate concordance as discussed in earlier sections is one strategy. When reporting results from clinical trials, it may be important to report the sociodemographics of the clinical and study team to evaluate concordance between the cohort and the clinicians and researchers. Similarly, concordance between the clinicians, researchers, and study population with the characteristics of the population living with T1D is another useful marker to evaluate concordance in diabetes care.
Concordance in Clinical Care
Social Support
Technology implementation does not only entail an additional requirement of technical support, but also social support. Notably, research has shown that an increase in social care led to an adherence to diabetes care. 41 It is beneficial to highlight that patients reported having an extensive support group, whereas clinicians underestimated the amount of social support their patients receive. 7 Investigating the effects of clinicians consistently assessing the extent of social support can result in an understanding of social needs between patient and clinicians for long-term management. Consequently, by recording a patient’s belief in diabetes management before and after an introduction of social support networks (community-based programs, familial attendance, and clinic workshops), we may be able to evaluate if there is a change in a patient’s perception of being surrounded by an adequate support network and if it aligns with the clinician’s assessment.
Approaches to Collaboration With Patients
Shared decision-making is an evidence-based strategy to build on patient-clinician relationships with concordance and offer a reparative strategy for discordant relationships.42,43 The S.H.A.R.E framework outlines five essential steps in the process of shared decision-making. 44 The first step starts with seeking patient participation which includes an explicit and authentic invitation from clinicians to invite their patients to be involved in health decisions and communicate the choices that exist in their health. The second step is to help explore and compare treatment options including discussing the benefits and harm of each and every options. The third step is to assess the patient’s values, preferences, and situations with specific care to use open-ended questions to identify what matters most to patients. Step 4 is to reach a decision with your patient and arrange a follow-up to facilitate the fifth step to evaluate the patient’s decision on their health outcomes.
Preferred Communication
Communication is one aspect of the patient-clinician relationship that can contribute to improved outcomes. Piemani et al published a systematic review assessing a fundamental concept regarding perceptions of patient-clinician communication. This study concluded that patients’ perceptions of optimized communication led to higher levels of patient compliance and less stress related to their long-term diseases. 45 To achieve successful communication, physicians can practice active listening, acknowledge patient emotions, and use encouraging tones rather than authoritarian ones in their clinical practices to align with their patient’s perceptions.
Patient-Reported Outcome Measures
There has been a movement in recent years toward patient-reported outcome measures (PROMs), questionnaires on health-related outcomes that are completed by patients. There are a number of PROMs available that are either general (e.g., quality of life) or specific to patients’ conditions PROMs can be used to elicit patients’ perspectives on outcomes relevant to their clinical condition and overall well-being, as well as patient perspectives on change in outcomes over time. They may also be a useful tool for health care providers to understand patients’ perspectives. In addition, the use of PROMS by physicians can become an essential tool to help individualize diabetes care and allow physicians to adapt and discuss recommendations based on the patient’s responses. By incorporating this shared decision-making in their diabetes care, patients will have the chance to have an active role in choosing their preferred treatment options, areas of focus, and tracking their progress, ameliorating discordance on options in their health care.
Motivational Interviewing
Approaches such as motivational interviewing 46 can be useful to align with patients in identifying barriers to technology and can be used to discuss implementing solutions to barriers. A key aspect of motivational interviewing is focusing, in which a topic related to behavior change is identified. Clinicians should engage in collaborative agenda setting with patients as part of focusing (e.g. “What 1-2 things would be the most important to you to discuss during our time together today?”). Motivational interviewing also includes OARS skills (open-ended questions, affirmation, reflective listening, and summary) that can be used to understand barriers to patient engagement in diabetes technology, patient readiness to engage in behavior change related to technology, and to begin planning steps towards behavior change when patients are ready for change. A provider may consider open-ended questions to identify patient perceptions of diabetes technologies (e.g. “What are some of the things you feel are not so great when it comes to using a pump or a Continuous Glucose Monitoring [CGM]?” and “What are some of the ways a pump or CGM might help with your diabetes-related goals?”), as well as patients’ goals related to diabetes care (e.g. “What is most important to you when it comes to your diabetes care?”). Providers can provide affirmations “You’ve clearly thought a lot about how technology might work for you, and what some of the challenges might be with changing your regimen” as well as ask permission to provide information “I’d like to give you some additional information of what I sometimes see as the challenges and benefits to technology use. Would that be okay?”
Discussion
This paper reviewed the existing literature on concordance between diabetes clinicians and patients on diabetes technology use. Whereas previous research has identified concordance as a facilitator to successful diabetes technology use, limitations exist, and additional work is needed. Some areas of concordance have been examined in depth, and systematic reviews have been published with high-quality evidence. Other areas of study are emerging and would benefit from additional research. Further research on patient and clinician perspectives is needed to actively address and diminish the adverse impact of discordant relationships and optimize concordant relationships. Future studies can collect patient reports quantifying the amount of time required by participants to integrate various techniques including diabetes technology into their routines, alongside a clinician’s estimation of the timeframe. Review of these comparative results can give clinicians greater insight into the reality of the integration process and result in a suitable intervention. Other factors that could be collected and compared in the patient-clinician relationship to identify discordance are perceived cost demands, device technical support, usefulness of the technology, and changes in device preference over time.
Subsequent research on varied communication styles and additional training programs for clinicians can measure a clinician’s attention toward communicative variances and the most effective communication approach tailored to a patient’s needs. Within this process, subgroups with similar communication preferences may be discovered.
Given that racially and ethnically concordant patient-clinician relationships benefited in improved communication, 47 additional research can be explored on cross-cultural training for clinicians in race-discordant relationships. Measuring patient behavior outcomes (level of communication, technology adherence, attendance in follow-up appointments, etc.) following multicultural training for clinicians can provide insight into challenges or improvements between race-discordant relationships. Investing in the research to advance concordance between clinicians and patients is the next step to ensuring a collaborative clinician-patient relationship and ultimately the optimal health outcomes for patients.
Footnotes
Abbreviations
ACPs, advanced care plans; CGM, continuous glucose monitoring; OARS skills, open ended questions, affirmation, reflective listening, and summary; PPWAI, Physician Patient Working Alliance Inventory; PROMs, patient-reported outcome measures; T1D, type 1 diabetes; WAI, working alliance inventory.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AA, KH, and YH do not have any relevant disclosures. LE receives salary support from NIDDK; has received research support from Breakthrough T1D, Medtronic, Abbot, and Mannkind; has served on the advisory board of Diabetes Center Berne and Medtronic. She has received consulting fees from Jaeb, Tandem Diabetes Care and Ypsomed, Sequel and has received honorarium fee from Medtronic and Insulet.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.