
Abstract
Continuous glucose monitors (CGMs) improve glycemic outcomes and quality of life for many people with diabetes. Research and clinical practice efforts have focused on CGM initiation and uptake. There is limited understanding of how to sustain CGM use to realize these benefits and limited consideration for different reasons/goals for CGM use. Therefore, we apply the Information-Motivation-Behavioral Skills (IMB) model as an organizing framework to advance understanding of CGM use as a complex, ongoing self-management behavior. We present a person-centered, dynamic perspective with the central thesis that IMB predictors of optimal CGM use vary based on the CGM use goal of the person with diabetes. This reframe emphasizes the importance of identifying and articulating each person’s goal for CGM use to inform education and support.
Introduction
Continuous glucose monitors (CGMs) have transformed diabetes self-management, with access to real-time glucose levels, viewable patterns over time, alerts to cue behavioral responses to prevent/manage hypo/hyperglycemia, and ability to share data with others including clinicians, family, and friends. 1 In the United States, CGM is standard of care for type 1 diabetes,2,3 and uptake is rapidly increasing for type 2 diabetes across medication regimens. 4 Consistent CGM use is required to realize the benefits of automated insulin delivery (AID) systems, 5 and CGM use without AID can improve adults’ hemoglobin A1c (HbA1c), time in range (TIR), reduce hypoglycemia, and improve quality of life.6-11
However, outcomes do not improve universally and substantial interindividual variability in CGM wearing and viewing CGM data likely drive variability in benefits.11-14 Complex ongoing behaviors have different predictors than one-time actions like filling the first CGM prescription. The Information-Motivation-Behavioral Skills (IMB) model 15 has been successfully applied to explain and promote ongoing health behaviors in diabetes16-23 and other contexts.15,20,24 Herein, we apply the IMB model to understand CGM use as a complex ongoing self-management behavior and propose meaningful additions to include CGM use goals (i.e., why an individual is using CGM and what they hope to gain from it). These goals vary across individuals and time and can help define education/behavioral supports and operationalize CGM use. Centering CGM use goals creates a framework that is applicable across diabetes types.
IMB Model for CGM Use
The IMB model 15 stipulates that to consistently perform a health behavior, an individual needs behavior-specific information, personal and social motivation, and behavioral skills.15,19,24-27 The primary outcome for the IMB model is the behavior. Here, that behavior is CGM use conceptualized as a continuous variable, least to most optimal (in contrast to a dichotomous variable, using vs. not). For instance, wearing a CGM for a higher proportion of time is associated with better diabetes outcomes, although exactly how much wear time is necessary for benefits is undetermined.28-30 Sustained CGM wearing requires behaviors to navigate barriers related to adhesive, skin issues, insurance coverage, and ensuring supplies are available when needed. Particularly among CGM users not using an AID system, additional behaviors are a necessary part of beneficial CGM use including checking CGM data throughout the day, viewing data trends, and responding to data and alerts.
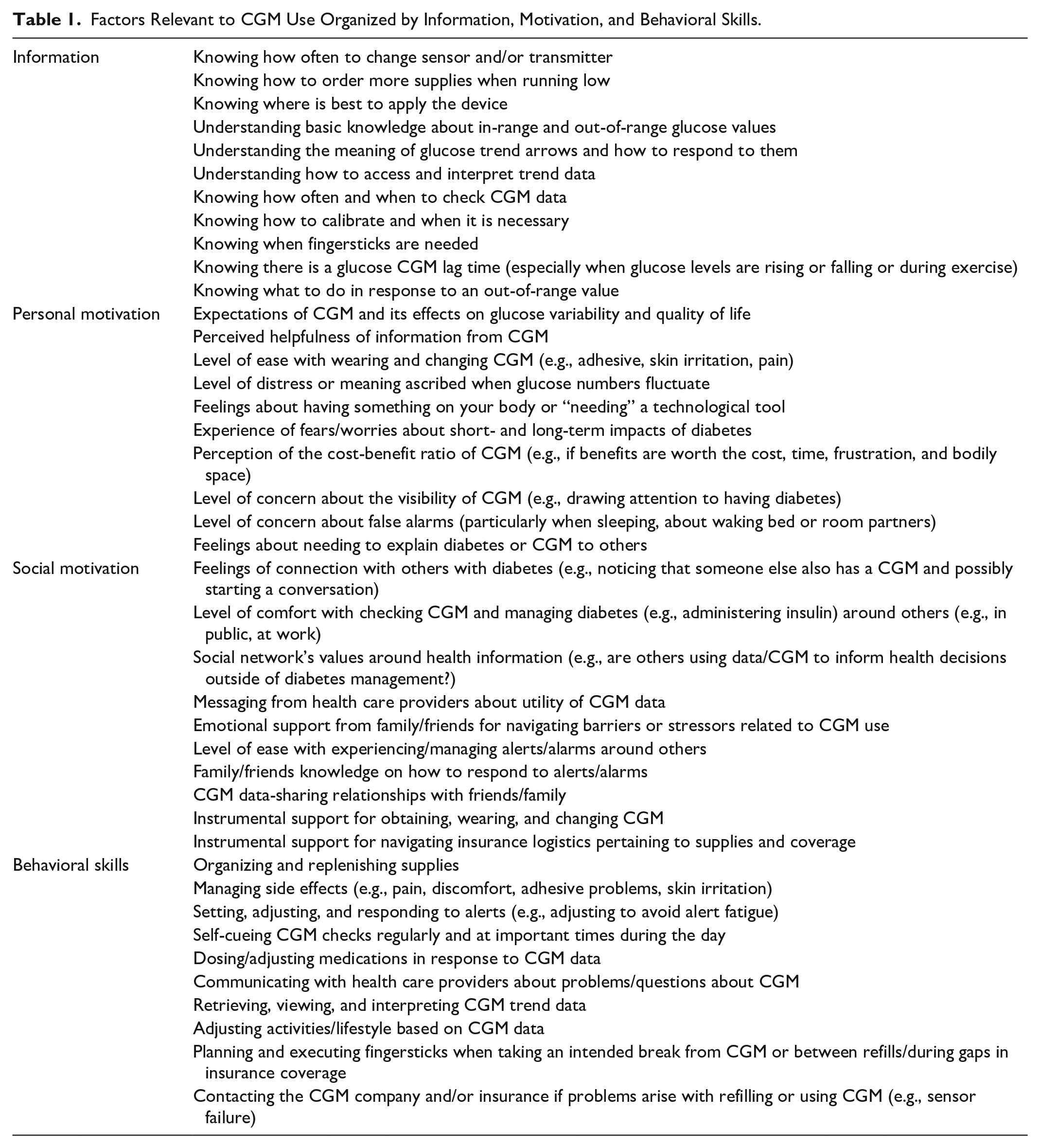
In addition to defining “CGM use” as a complex ongoing behavior, our application of the IMB model categorizes different determinants of sustained CGM use and highlights their interrelatedness. Table 1 includes specific examples of barriers and facilitators of CGM use, organized by IMB domain. The model stipulates that more optimal CGM use should be associated with favorable health outcomes (Figure 1) which, in turn, contribute to increased information, motivation, and, by extension, behavioral skills over time via a feedback loop.
Factors Relevant to CGM Use Organized by Information, Motivation, and Behavioral Skills.
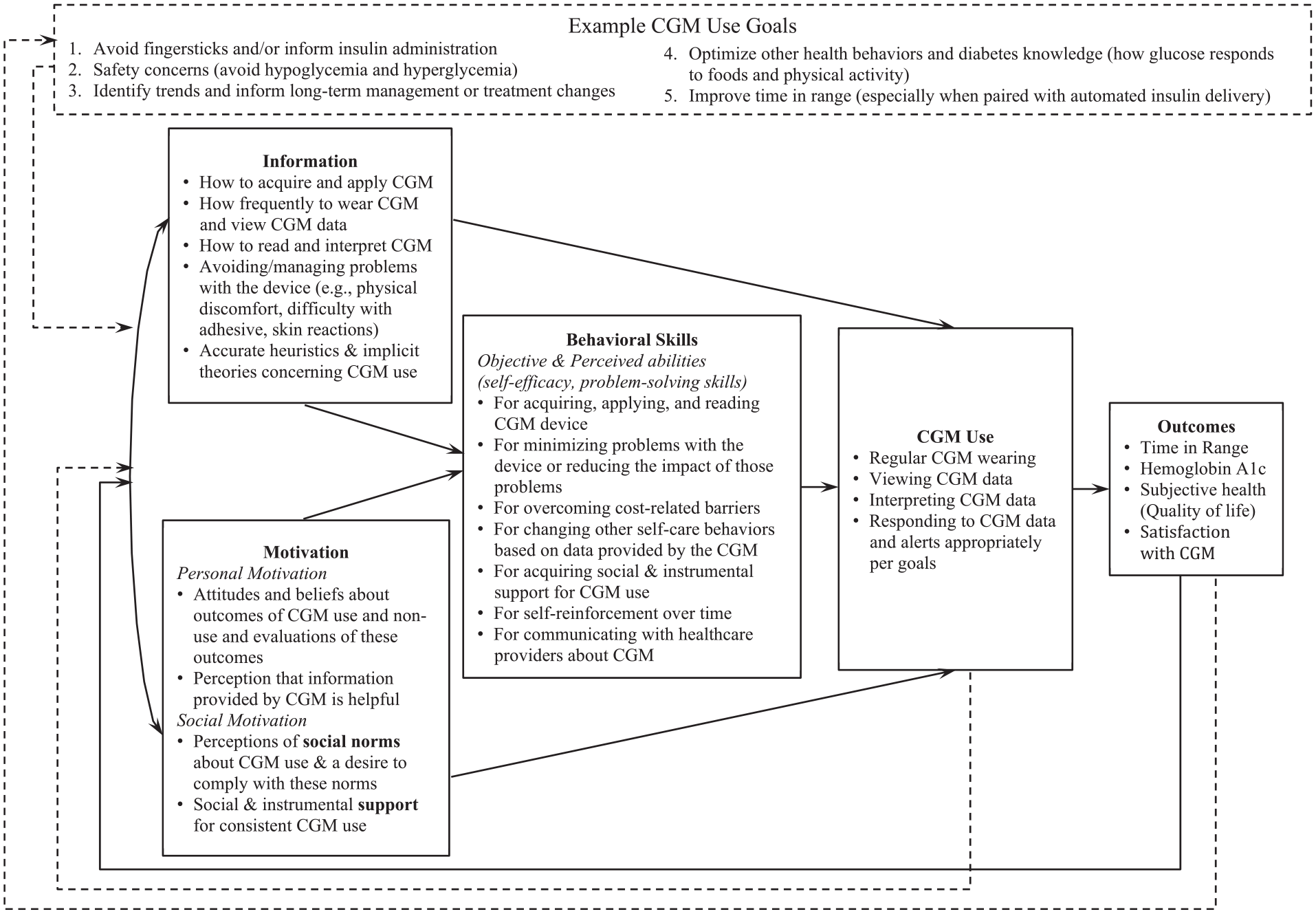
Information-Motivation-Behavioral Skills (IMB) Model of CGM Use.
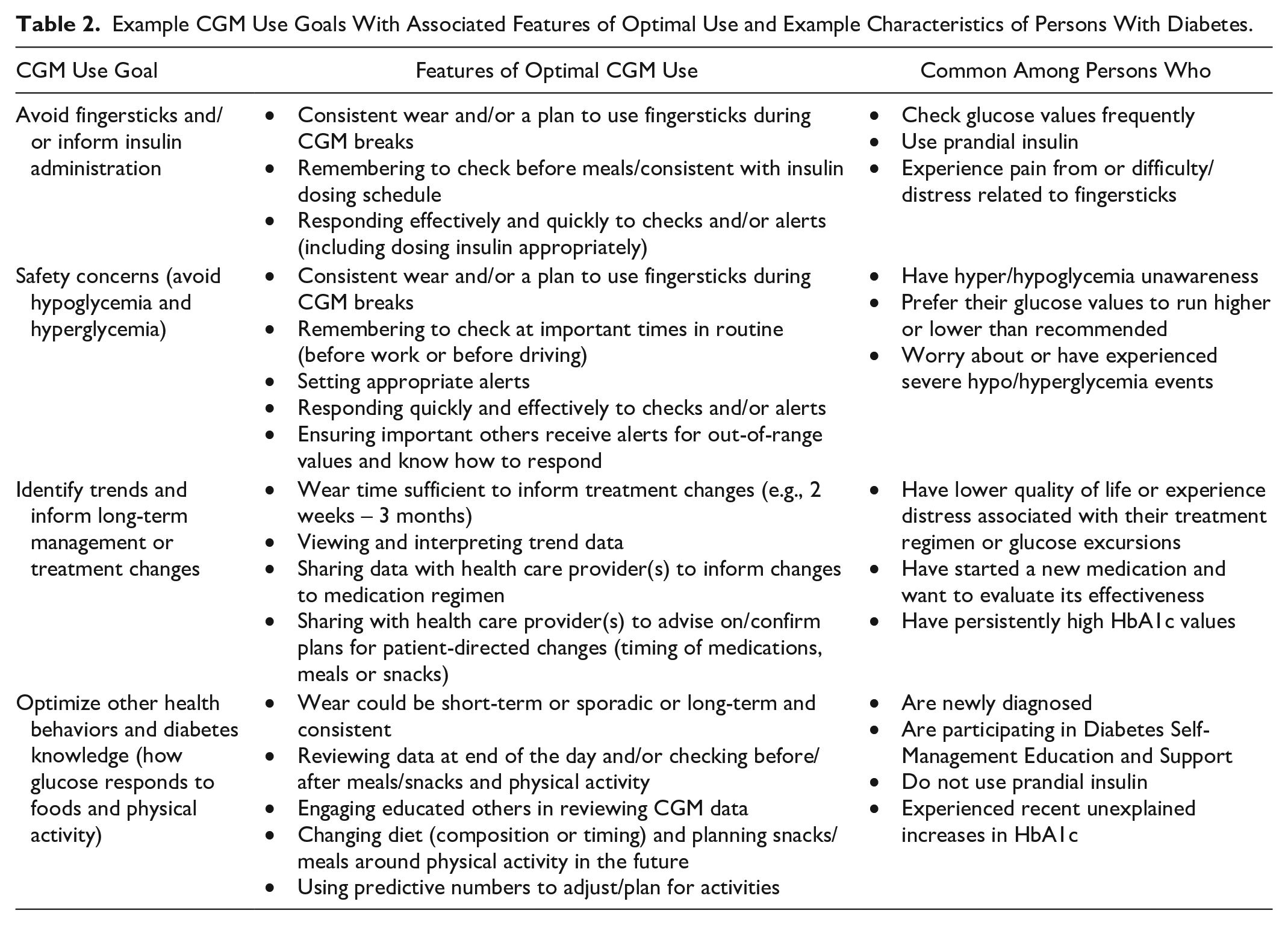
Given that CGM use itself provides frequent feedback, we propose a new second feedback loop from CGM use back to information and motivation capturing the learning and increased motivation that comes from seeing changes in glucose levels or TIR in response to behaviors or medication changes. We also propose a new overarching frame for the model which acknowledges each person’s goal for CGM use and its influence on IMB components and the definition of “optimal” use (Table 2). Relationships between the IMB model components (solid lines; Figure 1) are expected to remain as hypothesized regardless of CGM use goal. The IMB model already allows for each component of the model to vary—we add CGM use goal to organize that variation and suggest optimal CGM use and intended health outcome(s) may be different based on one’s goal. A new third feedback loop from outcomes to CGM use goal allows for goals to change over time.
Example CGM Use Goals With Associated Features of Optimal Use and Example Characteristics of Persons With Diabetes.
Information
CGM use information includes accurate knowledge about wearing a CGM, viewing and interpreting data, and responding when challenges arise. It also includes having accurate heuristics and theories that support CGM use as opposed to inaccurate heuristics (e.g., any glucose variation is harmful). Knowledge of how and when to read CGM data and respond to alerts requires general diabetes education and knowledge about in-range and out-of-range glucose values, the meaning of trend arrows, and how to access and interpret trend data. Certain information and heuristics are essential for enhancing trust in the CGM glucose values: knowing about false lows due to compression of the device, understanding discrepancies between CGM values and fingerstick values, and knowing how long it takes for insulin administration to affect values. Knowledge that uncontrollable factors (hormonal changes, weather, illness, stress) affect glucose may be necessary when accessing continuous glucose data. Per the IMB model, levels of information are associated with levels of motivation. Information and motivation directly impact behavioral skills and indirectly impact CGM use.
Motivation
Personal motivation reflects individuals’ attitudes about CGM use which are based on beliefs or expectations that CGM can benefit them, and perceptions of the information provided by the CGM as helpful. A person’s overall perception of knowledge about their diabetes-related numbers can range from useful and informative to distressing, anxiety-inducing, or shame-inducing. Continuous glucose monitors can exacerbate or challenge these existing perceptions, impacting motivation for ongoing use. Other relevant beliefs are the meaning of “needing” a medical device or technology and of wearing a device on the body. Relevant expectations require balancing positive expectations of how CGM can provide benefit with realistic expectations about potential burdens of CGM use. Maintaining CGM use may require realistic expectations that include experiences of distress and hassles as well as benefits of CGM use.
Social motivation for CGM use rests on perceived social norms endorsing CGM use and social and instrumental support for CGM use. Relevant social norms include concerns about the visibility of CGM and diabetes stigma. In some groups, CGM use may be normative, whereas in other groups, a person wearing CGM may have to address repeated inquiries about the device. Continuous glucose monitor alarms in social, work, or public settings may increase stigma and negative feedback about diabetes. Social and instrumental support for CGM use includes reinforcement from clinicians that CGM is useful and informative. This may involve clinicians reviewing CGM data to inform clinical care decisions and expressing the importance of these data. In addition, family/friends may offer emotional support (listening and expressing empathy for hassles and feelings about addressing others’ inquiries) and instrumental support including help navigating insurance, family/friends knowing how to respond to CGM alerts or alarms. Others’ response to seeing CGM on the body or hearing alerts may be harmful or conflictual and nighttime alarms may strain relationships with bed or room partners.
Sharing CGM data with friends/family may be a social motivation factor unique to CGM. The literature on CGM data sharing demonstrates benefits for both the person with diabetes and the share partner. 31 However, to ensure a successful data-sharing relationship, it is critical to establish ground rules.32,33 Ground rules are intended to honor the person with diabetes’s preferences and autonomy by setting forth expectations of how the friend/family should respond to the data. Knowing and articulating CGM use goals may inform ground rules and maximize benefits of sharing.
Personal and social motivation influences one another. For instance, personal beliefs may affect interest in CGM data sharing. CGM may be viewed as increasing autonomy and reducing concerns of family members, or as impeding autonomous diabetes management. The degree to which sharing CGM data supports or interferes with those perceptions likely informs comfort with data sharing. Similarly, social norms, personal beliefs, or values around privacy may reduce motivation to seek social support through CGM data sharing.
Behavioral Skills
Behavioral skills include objective and perceived abilities to maintain CGM use across different situations including obtaining and applying the device; setting, adjusting, and responding to alerts; dosing/adjusting insulin in response to CGM data; and/or adjusting activities/lifestyle based on CGM data. Moreover, behavioral skills include problem-solving skills to overcome challenges with CGM use, such as managing and overcoming technical difficulties, and communicating with health care providers or insurance companies if problems/questions arise.
Information and motivation work primarily through behavioral skills to affect CGM use. For instance, having accurate knowledge of how to respond to an out-of-range CGM alert (information), the belief that addressing an out-of-range CGM alert is beneficial (personal motivation), and comfort addressing an out-of-range value around others (social motivation) all affect whether a person will have self-efficacy and adequate behavioral skills to respond to CGM alerts consistent with their broader goals to manage diabetes.
Model Application
Optimal education and support for CGM use will require identification of each person’s goal to guide which aspects of IMB skills to emphasize. For example, a person using prandial insulin whose goal is to avoid hypoglycemia may prefer to avoid gaps in CGM use, develop habits to view CGM data at key times, and respond to alerts and arrows in a timely fashion. In this case, CGM-related education and support may emphasize information about the meaning of arrows and alerts and associated required changes in insulin administration. Social motivation may include sharing alerts for hypoglycemia with others with whom they spend time (partners, coworkers). Desired benefits may include increasing TIR and improving quality of life.
In contrast, a person not using prandial insulin may use CGM with the goal of optimizing other health behaviors, allowing for more time-limited use (wearing when making behavior changes or undergoing changes in their medications) and viewing trends at the end of each day or week. Education may focus on how CGM informs dietary, physical activity, or medication adherence changes. CGM education and support may focus on how to view and interpret trend data and emphasize the feedback loop from glucose data to information and motivation. They may choose to share and/or review data with someone who understands how behaviors affect glucose for people with diabetes (e.g., a health care professional, family/friend with diabetes). Desired benefits may be lower HbA1c or more TIR.
Conclusion
CGM use is a complex ongoing self-management behavior, conceptualized with the IMB model to guide efforts to realize long-term glycemic and quality-of-life benefits for people with diabetes. This framework can be applied to understand heterogeneous experiences and outcomes of CGM use, and to guide education, support, and interventions for CGM use. This model emphasizes that CGM is a tool to support a person with diabetes and highlights how diabetes education can be tailored to identify what information is needed in accordance with an individual’s goals and desired outcomes. Certain goals may be more prevalent based on diabetes characteristics like diabetes duration, medication regimen, HbA1c level, and frequency of hyper/hypoglycemia. CGM goals may evolve depending on life demands and time/experience with diabetes and with CGM, thus, ongoing evolving support may be needed for sustained and effective CGM use.
The IMB model is designed to explain, predict, and guide interventions on an individual level, with acknowledgment of the role of social motivation and its drivers. The model does not incorporate health care system-level factors known to be critical (CGM-related costs, insurance coverage, billing codes, and expertise of clinicians)34-36 or aspects of the CGM technology/device. However, a strength of the IMB model is the dynamic consideration of changes in the individual’s knowledge, motivation, and behavioral skills which are affected by these factors.
At this point, the IMB model of CGM use is proposed as a useful organizing framework based on existing literature and our experiences with clinical care and intervention research. Important next steps include identifying/developing necessary measures and applying them toward validation of the IMB model of CGM use. Further research should elucidate which specific aspects of each IMB component are most relevant for different CGM use goals. We also suggest operationalization of sustained CGM use should allow different degrees of ongoing use to be considered “optimal” for different use cases and goals. Our framework can inform the types and frequency of clinician support required, which is essential as use of CGM in primary care settings increases.4,36 IMB model interventions should tailor content to individuals’ goals and barriers, dynamically over time, and evaluate intervention effects on CGM use and anticipated outcomes.15,16,22
Footnotes
Abbreviations
AID, automated insulin delivery; CGM, continuous glucose monitor; HbA1c, hemoglobin A1c; IMB, information-motivation-behavioral skills; TIR, time in range
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors’ contributions to this work were supported by the Leona M. and Harry B. Helmsley Charitable Trust (Author LSM is PI). Author NAA received consulting fees from Diathrive Health and has a grant from Dexcom for equipment being used in an NIH-funded research project. KH received consulting fees from Cecelia Health and Sanofi.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This collaboration was supported by the Leona M. and Harry B. Helmsley Charitable Trust (grant no. R-2203-05822).