
Abstract
Keywords
To the editor,
Hybrid closed-loop (HCL) systems provide significant improvements in diabetes management1,2 which support their use as standard-of-care for people living with type 1 diabetes. International consensus guidelines of continuous glucose monitoring (CGM) metrics provide key targeted objectives, 3 but there is a real need to reduce the number of key indicators. The glycemic risk index (GRI) is a composite score that combines hypoglycaemia and hyperglycaemia risks into a single number. 4 The threefold aim of this retrospective longitudinal cohort analysis was to (1) evaluate GRI after initiation with the MiniMed 780G system (MM780G, Medtronic, Northridge, California) by analyzing real-world data from 202 adults and adolescents with type 1 diabetes, (2) explore its relationship with time in range (TIR) and other CGM metrics, and (3) identify subclusters of users for whom individual strategies are needed. Participants (Supplemental Table S1) were continuous subcutaneous insulin infusion (CSII) users, and most of them were equipped with a predictive low glucose system before HCL therapy. After initiation and follow-up with MM780G (Figure 1), all participants increased their TIR and decreased their GRI (Supplemental Figure S1). Adults and adolescents showed a mean increase of +13.5% and +14.4% in TIR (70-180 mg/dL) after one year and a significant decrease of −15.2% and −19.1% in GRI, respectively (Supplemental Table S2). Our results confirm that GRI was strongly inversely correlated with TIR 5 and extended these findings to different age groups. Multiple comparison analysis indicated that median TIR remained similar between M3 and M12, whereas GRI decreased initially but increased significantly thereafter (P < .001). Receiver operating characteristic (ROC) analyses indicated similar improvements for GRI (area under the curve [AUC] = 0.823) and TIR (AUC = 0.815) after three months, but AUCs for GRI decreased thereafter while remained stable for TIR. These changes were also noted in the distribution among grid zones (Supplemental Table S3). Clustering by age and GRI at baseline identified three groups of individuals associated with distinct outcome profiles after three months (Supplemental Figure S2 and Table S4). A baseline GRI below 38, the upper 99% confidence interval (CI) of mean in clusters 1 and 3, was predictive of higher TIR levels at three months (P < .0001). Glycemic risk index can identify those individuals with more extreme glucose excursions at baseline and during follow-up which can be helpful to guide diabetes management. The magnitude of improvement at one year was greater for GRI than for TIR, in both adults (35.1% vs 22.2%) and adolescents (33.3% vs 27.4%). As GRI adds weight to very high values, increase in TIR and decrease in GRI were supported by the significant reduction in the time above range (TAR) component. Previous HCL studies in children and adolescents have underlined the specificities of this age group and the difficulties to reach target outcomes. Challenges for optimal diabetes management remain high in this group of individuals. 6 Despite that, a large proportion of adolescents in our study improved their glucose control. We showed that clustering by age and baseline GRI provides simple tools for clinicians to predict outcomes and set individual strategies.
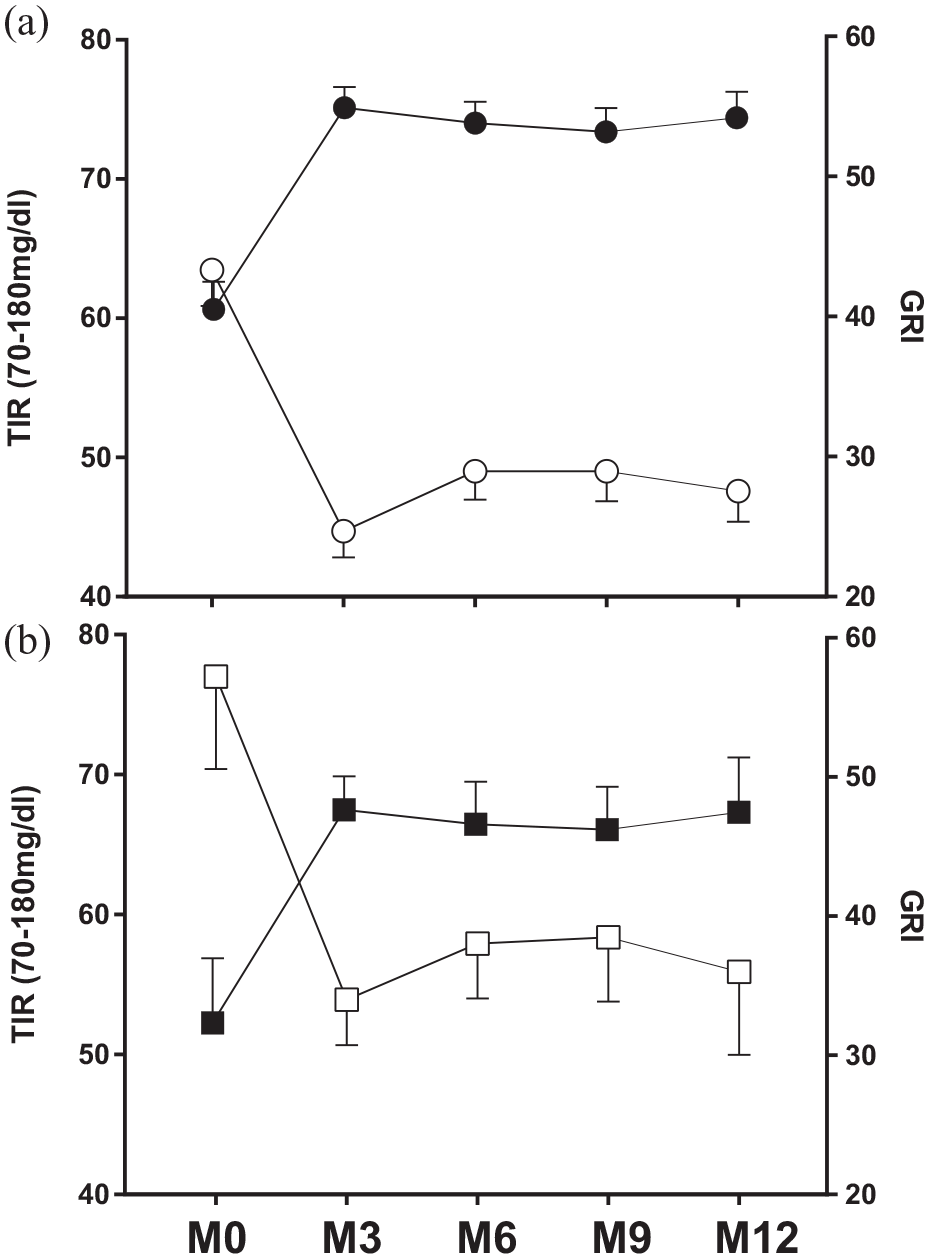
Evolution of TIR (closed symbols) and GRI levels (open symbols) at baseline and quarterly up to one year after MiniMed 780G HCL system initiation in adults (A, circles, n = 169) and adolescents (B, squares, n = 33).
We suggest that addition of GRI to endpoint measures during HCL therapy provides an additional information to TIR to monitor diabetes management and to set individual strategies.
Supplemental Material
sj-docx-1-dst-10.1177_19322968241258742 – Supplemental material for Ascertaining the Utility of the Glycemia Risk Index for Glucose Outcomes With Hybrid Closed-Loop Therapy in Adolescents and Adults With Type 1 Diabetes
Supplemental material, sj-docx-1-dst-10.1177_19322968241258742 for Ascertaining the Utility of the Glycemia Risk Index for Glucose Outcomes With Hybrid Closed-Loop Therapy in Adolescents and Adults With Type 1 Diabetes by Charles Thivolet, Maha Lebbar, Kevin Perge, Marc Nicolino and Sylvie Villar-Fimbel in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
Abbreviations
HCL, Hybrid Closed Loop; GRI, Glycemia Risk Index; CGM, Continuous Glucose Monitoring; TIR, Time in Range.
Author Contributions
CT wrote the manuscript and researched data. ML researched data and contributed to the discussion. SV-F, KP, and MN contributed to the discussion and reviewed/edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CT reports personal fees from Abbott Diabetes Care, Glooko, Lilly, Novo-Nordisk, Medtronic, and Sanofi and is an advisory board member for Insulet and Medtronic. SV-F reports personal fees from Abbott Diabetes Care, Lilly, Novo-Nordisk, Medtronic, Roche Diabetes Care, and Sanofi. ML and KP have no conflicts of interest. MN has received travel support for meetings, speaker fees and honoraria from Abbott Diabetes Care, Lilly, Novo-Nordisk, Roche Diabetes Care, and Sanofi, and is an advisory board member for Novo-Nordisk.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.