
Abstract

The use of advanced hybrid closed-loop (AHCL) systems in type 1 diabetes (T1D) in maintaining glucose time in range during physical activity is promising 1 ; however, even with AHCL systems, managing glucose levels around exercise may still be challenging, as insulin requirements vary with different types of physical activity 2 and higher risks of hypoglycemia may last up to several hours after exercise. 3 Furthermore, as exercise during postprandial state provides additional challenges and the use of AHCL devices in such period has not been fully evaluated yet, 4 we performed an open-label, randomized, crossover study in order to evaluate the performance of a specific AHCL system, Tandem t-slimX2 with Control-IQ (C-IQ) algorithm, during postprandial moderate-intensity aerobic activity (AER) and high-intensity interval training (HIIT) in adults with T1D.
Ten adults (M/F 3/7, median age 34 years, median diabetes duration 19 years, median HbA1c 6.8%) with T1D for at least 1 year, using a C-IQ system for at least 6 months, with regular physical activity (≥150 minutes/week) and without microvascular complications or severe hypoglycemic events in the last 2 weeks before exercise sessions, were enrolled. Each participant completed two physical activity sessions (AER and HIIT) on two different days, in randomized order. A standardized lunch was consumed at 12:00 p.m., and the appropriate insulin bolus was reduced by 30% to 50% according to glucose trends. The “exercise activity” AHCL function was started at 1:30 p.m., while each session started at 2:00 p.m. and lasted 150 minutes as follows: 60 minutes of rest, 30 minutes of physical activity on a cycle ergometer, and 60 minutes of recovery. Subjects performed AER, at 60% heart rate reserve (HRres), in one session and HIIT, alternating 2 minutes of exercise at 50% HRres and 60 seconds of exercise at 80% HRres, in the other one.
As reported in Table 1, no significant differences were observed between AER and HIIT for all glucose metrics during physical activity, in the subsequent recovery phase and during the following night. Furthermore, the automatic suspension time of basal insulin was significantly longer during HIIT than AER (33 vs 20 minutes; P = .021), possibly because of a slower rise in glucose levels after HIIT, reflecting a suboptimal balance between glucose uptake by muscle and rise in hepatic glucose production. 5
Continuous Glucose Monitoring (CGM) Metrics During and After Both Sessions of Physical Activity.
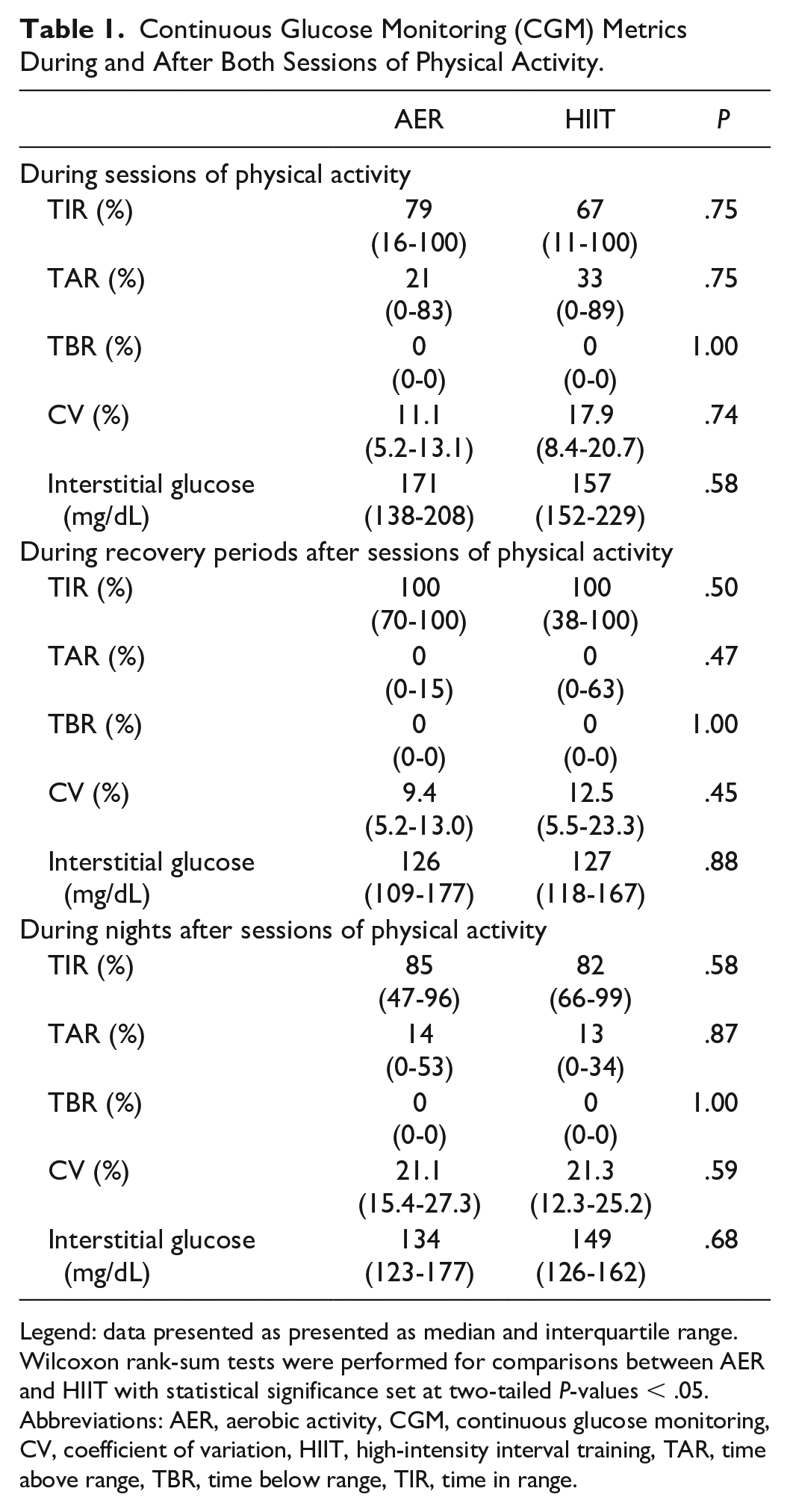
Legend: data presented as presented as median and interquartile range. Wilcoxon rank-sum tests were performed for comparisons between AER and HIIT with statistical significance set at two-tailed P-values < .05.
Abbreviations: AER, aerobic activity, CGM, continuous glucose monitoring, CV, coefficient of variation, HIIT, high-intensity interval training, TAR, time above range, TBR, time below range, TIR, time in range.
To our knowledge, only one other study evaluated this specific AHCL system during physical activity, 1 but it involved only children and adolescents without specifying the timing of the activity carried out. In our study, physical activity was carried out 3 hours after the meal and an exercise target was set 90 minutes before the start of the sessions, as suggested by Tagougui et al. 6
Although limited to a small sample size and short-duration exercise, our results showed how the C-IQ is safe and effective in adults with T1D at minimizing time in hyperglycemia and hypoglycemia during both postprandial AER and HIIT and up to the following night. Unfortunately, the results of our study are not generalizable to other AHCL systems, as each algorithm has specific peculiarities whose impact during physical activity will have to be evaluated during further studies.
Footnotes
Abbreviations
AER, aerobic activity; AHCL, advanced hybrid closed-loop; C-IQ, control-IQ; CGM, continuous glucose monitoring; CV, coefficient of variation; HIIT, high-intensity interval training; HRres, heart rate reserve; T1D, type 1 diabetes; TAR, time above range; TBR, time below range; TIR, time in range.
Author Contributions
MT, EB, and GDP designed the study. GDP, AC, MP, and LC collected the clinical data. AC, MT, and LS contributed to data interpretation and statistical analyses. GDP wrote the first draft of the letter. MT and AC contributed to further revisions of the letter. All the authors contributed to the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.