
Abstract
Background:
Hyperglycemia occurs in 22% to 46% of hospitalized patients, negatively affecting patient outcomes, including mortality, inpatient complications, length of stay, and hospital costs. Achieving inpatient glycemic control is challenging due to inconsistent caloric intake, changes from home medications, a catabolic state in the setting of acute illness, consequences of acute inflammation, intercurrent infection, and limitations in labor-intensive glucose monitoring and insulin administration.
Method:
We conducted a retrospective cross-sectional analysis at the University of California San Francisco hospitals between September 3, 2020 and September 2, 2021, comparing point-of-care glucose measurements in patients on nil per os (NPO), continuous total parenteral nutrition, or continuous tube feeding assigned to our novel automated self-adjusting subcutaneous insulin algorithm (SQIA) or conventional, physician-driven insulin dosing. We also evaluated physician efficiency by tracking the number of insulin orders placed or modified.
Results:
The proportion of glucose in range (70-180 mg/dL) was higher in the SQIA group than in the conventional group (71.0% vs 69.0%, P = .153). The SQIA led to a lower proportion of severe hyperglycemia (>250 mg/dL; 5.8% vs 7.2%, P = .017), hypoglycemia (54-69 mg/dL; 0.8% vs 1.2%, P = .029), and severe hypoglycemia (<54 mg/dL; 0.3% vs 0.5%, P = .076) events. The number of orders a physician had to place while a patient was on the SQIA was reduced by a factor of more than 12, when compared with while a patient was on conventional insulin dosing.
Conclusions:
The SQIA reduced severe hyperglycemia, hypoglycemia, and severe hypoglycemia compared with conventional insulin dosing. It also improved physician efficiency by reducing the number of order modifications a physician had to place.
Keywords
Introduction
Hyperglycemia occurs in 22% to 46% of hospitalized patients, and negatively affects patient outcomes, including mortality, inpatient complications, hospital length of stay, and overall hospital costs. In addition, a diagnosis of diabetes increases the rate of hospitalization by two- to sixfold.1-8 On the contrary, overly tight glycemic control is associated with hypoglycemia and is also associated with increased morbidity and mortality.9-13 Achieving appropriate glycemic control is challenging in hospitalized patients due to inconsistent caloric intake, changes from home medications, a catabolic state in the setting of acute illness, changes in renal and hepatic function, changing doses of glucocorticoids, surgery, acute causes and consequences of inflammation, infections, and limitations in labor-intensive glucose monitoring and insulin administration. 14
Hospitalized patient populations most at risk for both hyperglycemia and hypoglycemia include patients receiving total parenteral nutrition (TPN) or enteral tube feedings (TFs), and those who are nil per os (NPO). 15 These patients may frequently have hypoglycemia that is associated with higher risk of complications and mortality. 16 Historically, these patients have been placed on insulin sliding scale regimens. However, studies have demonstrated improved glycemic control with a basal-bolus insulin regimen compared with insulin sliding scale regimen alone.4,15,17 The American Diabetes Association and current Endocrinology Society inpatient guidelines now recommend basal insulin or a basal-bolus correction insulin regimen for noncritically ill hospitalized patients with poor oral intake or those who are NPO.18,19 For any of these situations, and whichever insulin regimen is chosen, a persistent problem of insulin adjustment inertia remains and necessary changes in the insulin regimens are delayed or never occur.20-22
To address challenges in achieving glycemic control in hospitalized patients who are NPO or on TPN or TF, we created a novel self-adjusting subcutaneous insulin algorithm (SQIA) integrated into the electronic medical record (EMR) as an opt in order set for adult patients who are NPO or on either continuous TPN or continuous TFs. Subcutaneous algorithms have been shown to be as effective as labor-intensive intravenous (IV) infusion protocols in the perioperative and intensive care unit (ICU) settings.23-25 Results of a pilot study of our SQIA demonstrated blood glucoses were maintained between 80 and 180 mg/dL for the majority of measured glucoses (66.8%), without any episodes of hypoglycemia (glucose <60 mg/dL). 26
In this study, we evaluate the effectiveness of our automated SQIA in achieving glycemic control compared with conventional, physician-driven insulin dosing in the first year of its implementation across a multi-hospital academic health system. We also evaluate its benefit in improving physician efficiency in terms of the effort required to manually place and modify insulin dosing, which is the hallmark of conventional insulin management. Demonstrating efficacy of our novel algorithm would enable it to become part of standard of care for patients on high-risk diets at and beyond our institution.
Methods
The SQIA Development
The SQIA is integrated into the EMR as a calculator embedded in the medication administration record (MAR). When a physician orders rapid-acting insulin to be administered to a patient who is NPO or on continuous TF or continuous TPN, there is an option to utilize the SQIA or proceed with conventional physician-driven insulin orders. If the SQIA is chosen, the clinician is only required to enter an initial starting insulin dose. The SQIA also provides suggestions for the initial dose based on the patient’s previous insulin dosing, when available. At insulin administration times, the nurse enters the patient’s current glucose level in the MAR, and the SQIA uses the prior insulin doses, prior glucoses, and current glucose to automatically calculate the new insulin dose (Supplemental Figure S1, Supplemental Table S1). If the nurse or provider wants to review the calculation, the SQIA is available through a hyperlink within the MAR. The SQIA is designed to titrate the glucose to 120 to 180 mg/dL for patients who are NPO, or on continuous TPN or TF. New guidelines 19 have a goal for these patients of 100 to 180 mg/dL, but as we use an algorithm, we prioritized minimizing risk for hypoglycemia, especially given the algorithm is automated and the goal is to minimize insulin adjustments. No new orders are required even if insulin is added to TPN, or changes are made to TF rates. For further details, refer to our initial paper on the SQIA pilot study. 26
The SQIA Implementation and Education
The SQIA order set became available on September 3, 2020 for all patients who are NPO, on continuous TPN, or on continuous TF at the three acute care University of California, San Francisco (UCSF) Health hospitals located in San Francisco. As these three hospitals share the same services, medical and nursing staff, administration, EMR, order sets, and formulary, they were analyzed as a single hospital with three locations. Optional online training that covered how to put in orders, why to use the orders, and a quick version of how the calculator works (<10 minutes in length) was provided to nurses, physicians, and pharmacists. In-person training sessions were provided to unit nursing managers and tip sheets were given to all nursing staff. During the implementation, we partnered with the nursing education department to create a five-minute mandatory e-learning module, with a brief introduction and reason for using the SQIA and details on how to use the SQIA calculator. The module was distributed to all nursing staff.
Patients and Eligible Intervals
All adult, nonobstetric patients admitted between September 3, 2020, and September 2, 2021, who were NPO, on continuous TPN, or continuous TF any time during their hospitalization were eligible for the SQIA. The only patients excluded were patients who were on cycle TPN or TF as the algorithm was only for use if on continuous TPN or TF. There were no exclusions for any changes in the types of enteral feedings or use of glucocorticoids (of any dose). The patient was assigned to either the SQIA or conventional insulin orders by the ordering physician. Our long-standing guidelines for use of basal insulin was shown in either order set and use of basal insulin remained up to the ordering physician. As these patients might not be NPO or on TF or TPN during the entire hospitalization, we limited our analysis to their eligible intervals, defined as inpatient intervals during which the patient was on an eligible diet order (NPO, TPN, or TF) and an eligible insulin order set (conventional or SQIA). Of note, a single patient’s hospitalization could include multiple eligible intervals. A single patient with multiple eligible intervals could also have been ordered for both the conventional and SQIA order sets if used at different time points during the hospitalization.
We excluded patients who received an average of <1 unit of insulin over 24 hours, as these patients had minimal insulin needs that are not clinically meaningful, and also excluded those who did not have any recorded glucose measurements, as the orders were not implemented.
Data Extraction
This was a retrospective cross-sectional study using EMR data. We queried the EMR database for eligible intervals during the study period (September 3, 2020, to September 2, 2021) and extracted point of care (POC) glucose measurements and insulin administration records. We eliminated spurious and repeated values by using a previously described protocol. 27
Glucose monitoring
The conventional insulin and SQIA order sets both include a POC glucose measurement every four hours. The primary glycemic control outcomes were percentage of measurements in four out-of-range categories: severe hyperglycemia (>250 mg/dL), hyperglycemia (181-250 mg/dL), hypoglycemia (54-69 mg/dL), and severe hypoglycemia (<54 mg/dL). We also measured the complementary percentage of measurements that were in range (70-180 mg/dL).
Physician efficiency
Physician efficiency was assessed using manual chart review of eligible intervals in which the patient was receiving continuous TF, due to longer duration of intervals, higher insulin dosages on average, and increased frequency of insulin order adjustments with a larger hypothesized effect size. We randomly selected 20 eligible intervals using conventional insulin dosing and 20 eligible intervals using the SQIA. Two of the authors (PBM and RJR) independently reviewed EMR and counted the number of times that a bolus insulin dosage was changed by a physician within an eligible interval. In our EMR system, order changes are documented on the insulin/glucose flow sheet. Reordering the same insulin dosage did not constitute an order change. After independently counting order changes, the authors reviewed discrepancies together and arrived at a consensus count for each eligible interval. This analysis was performed with the manual EMR review due to limitations in accurate data extraction of order modifications inherent to the EMR and data extraction software.
Analyses
The primary unit of analysis was the eligible interval, as defined previously. Baseline characteristics, including age at admission, length of stay, level of care at admission, admission service, and admission creatinine level, were compared using hospitalization as the unit of analysis. Creatinine was of interest, given renal clearance of insulin. A hospitalization was assigned to the conventional group, if it had at least one conventional insulin order interval, and to the SQIA group, if it had at least one SQIA order interval. Some hospitalizations included eligible intervals in both groups.
Glucose monitoring
We compared the actual number of POC glucose measurements using Poisson regression, with eligible interval duration as the offset and adjusted for diet (NPO, TF, or TPN) and level of care (acute, telemetry, or ICU). To calculate the incidence rate for out-of-range versus in-range measurements, we used Poisson regression with number of POC glucose measurements as the offset, again adjusted for diet and level of care. In the Poisson regression, variances were calculated accounting for clustering by patient. As TFs occur more frequently in the ICU, last longer, and require higher insulin doses and more frequent insulin titration, we planned a subgroup analysis of eligible intervals for TFs specifically.
Physician efficiency
The manual record review resulted in a count of order changes for each randomly selected eligible interval. We then calculated the incidence rates for order changes per 24 interval hours along with the incidence rate ratio.
Results
From September 3, 2020, to September 2, 2021, the SQIA or conventional insulin was ordered during 1556 unique hospitalizations, with a total of 1198 hospitalizations where SQIA was ordered and 552 hospitalizations where conventional insulin was ordered. As mentioned previously, because one patient could have multiple eligible intervals during which either insulin order set could have been ordered, there were 194 hospitalizations during which the patient received both conventional insulin and SQIA orders during their hospitalization.
During the study period, there were 2554 eligible intervals in which the patient was on an eligible diet (NPO, TPN, and TF) and on an eligible insulin order set (conventional or SQIA). These eligible intervals were associated with 1750 distinct hospitalizations. Of the eligible intervals, 32.9% (839 intervals, 552 hospitalizations, and 1.5 intervals per hospitalization) were on the conventional order set and the other 67.1% (1715 intervals, 1198 hospitalizations, and 1.4 intervals per hospitalization) were on SQIA (Table 1).
Baseline Characteristics of Hospitalizations.
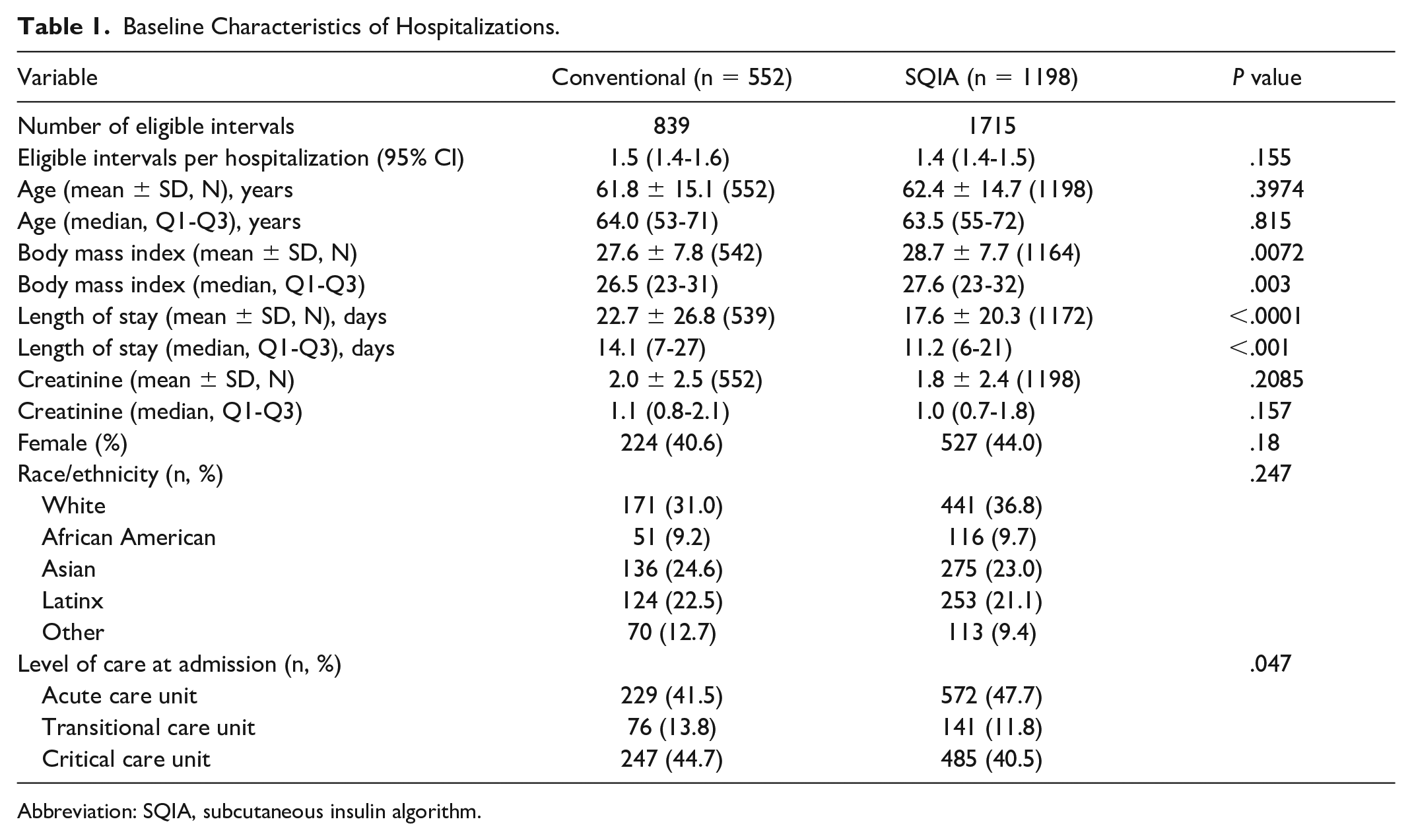
Abbreviation: SQIA, subcutaneous insulin algorithm.
Patients hospitalized in the two groups were similar with respect to age, creatinine, sex, and race/ethnicity. The conventional group had a longer median length of stay than the SQIA group (14.1 days vs 11.2 days, P < .001) and a greater proportion initially admitted to the ICU (44.7% vs 40.5%, P = .041). They also had a lower median body mass index (BMI; 26.5 vs 27.6). The admitting service with the most patients was hospital medicine with 25.1%. Across admission services, the average proportion of hospitalizations assigned to the SQIA group was 68.5%. This proportion was higher for hospitalizations to the surgical subspecialty services (78.7%) and lower for cardiology and cardiac surgery services (57.1% and 56.7%, respectively; Supplemental Table S2).
Overall, 31% of the eligible intervals were on TF. This proportion was higher in the conventional group than the SQIA group (34.0% vs 29.2%, P = .039; Table 2). Only 5.5% of the eligible intervals were on TPN. The median interval duration was longer for TF intervals. After stratification by diet (NPO, TF, or TPN), eligible interval durations were similar between the conventional and SQIA groups. The median insulin dosage rates were higher in the TF intervals (31.7 units per 24 hours) than in the NPO and TPN intervals (17.8 and 20.3 units per 24 hours, respectively). The SQIA was associated with lower insulin dosage rates than conventional insulin for TF intervals, but with higher dosage rates for NPO and TPN intervals.
Eligible Intervals Characteristics.
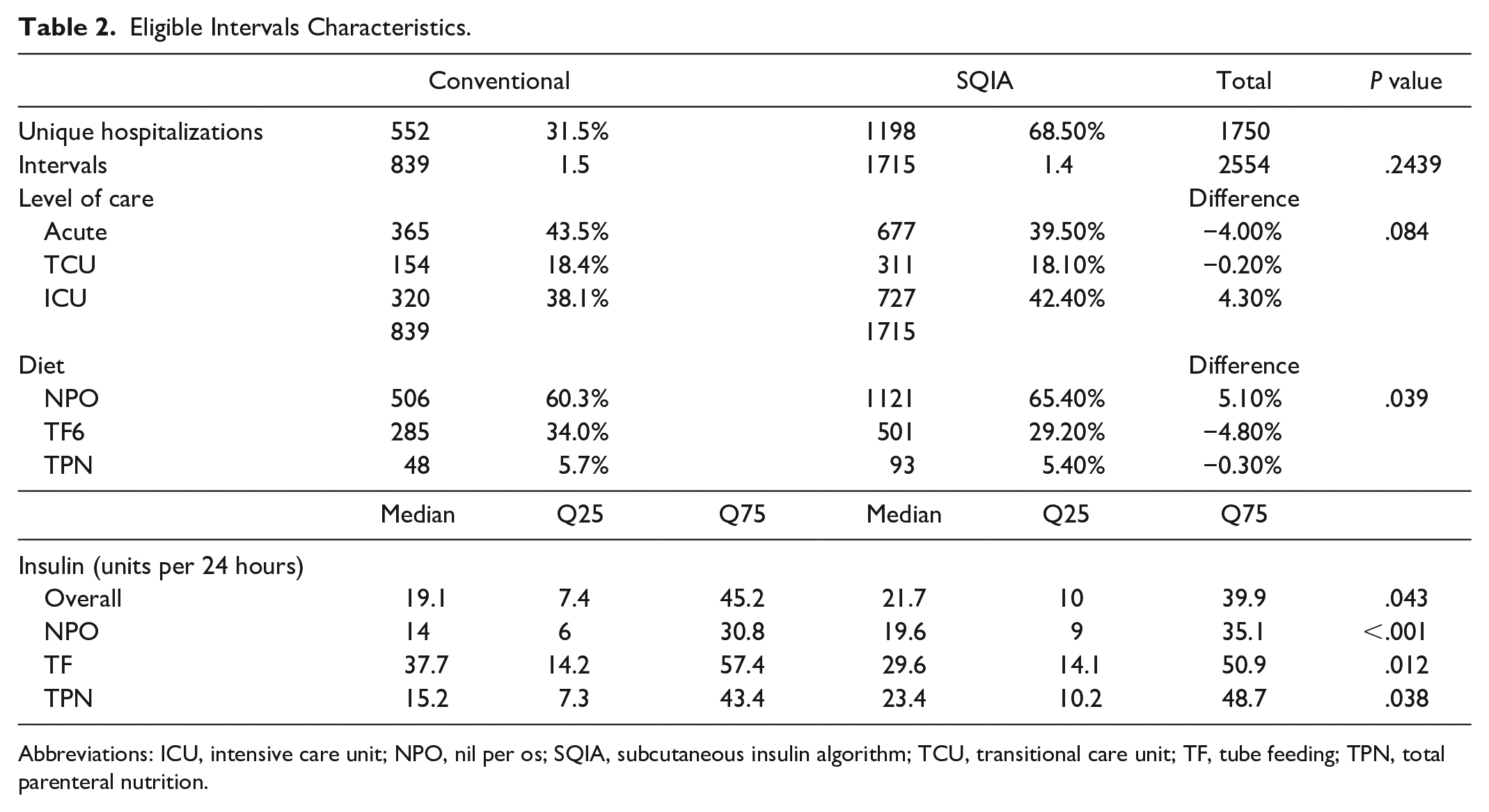
Abbreviations: ICU, intensive care unit; NPO, nil per os; SQIA, subcutaneous insulin algorithm; TCU, transitional care unit; TF, tube feeding; TPN, total parenteral nutrition.
The SQIA intervals had fewer POC glucose measurements per 24 hours (SQIA 6.2 vs conventional 6.4, P = .007; Table 3). The percentage of measurements that were in range (70-180 mg/dL) was slightly higher, but not statistically significantly higher, in the SQIA group than in the conventional group (SQIA 71.0%, conventional 69.0%, P = .153). Most of the out-of-range measurements were in the hyperglycemia category (181-250 mg/dL), and the proportions did not differ between the two order sets (SQIA 24.2%, conventional 24.4%, P = .912). The proportions in the severe hyperglycemia, hypoglycemia, and severe hypoglycemia categories were all lower in the SQIA group than in the conventional order group. The incidence rate ratios were statistically significantly less than 1.0 for severe hyperglycemia (0.80) and hypoglycemia (0.72), but not for severe hypoglycemia (0.69). The results were similar in the subgroup of 786 TF intervals with respect to level of care, duration, and average insulin dosage (units per 24 interval hours; Table 3).
Glycemic Control on Conventional Insulin Versus SQIA.
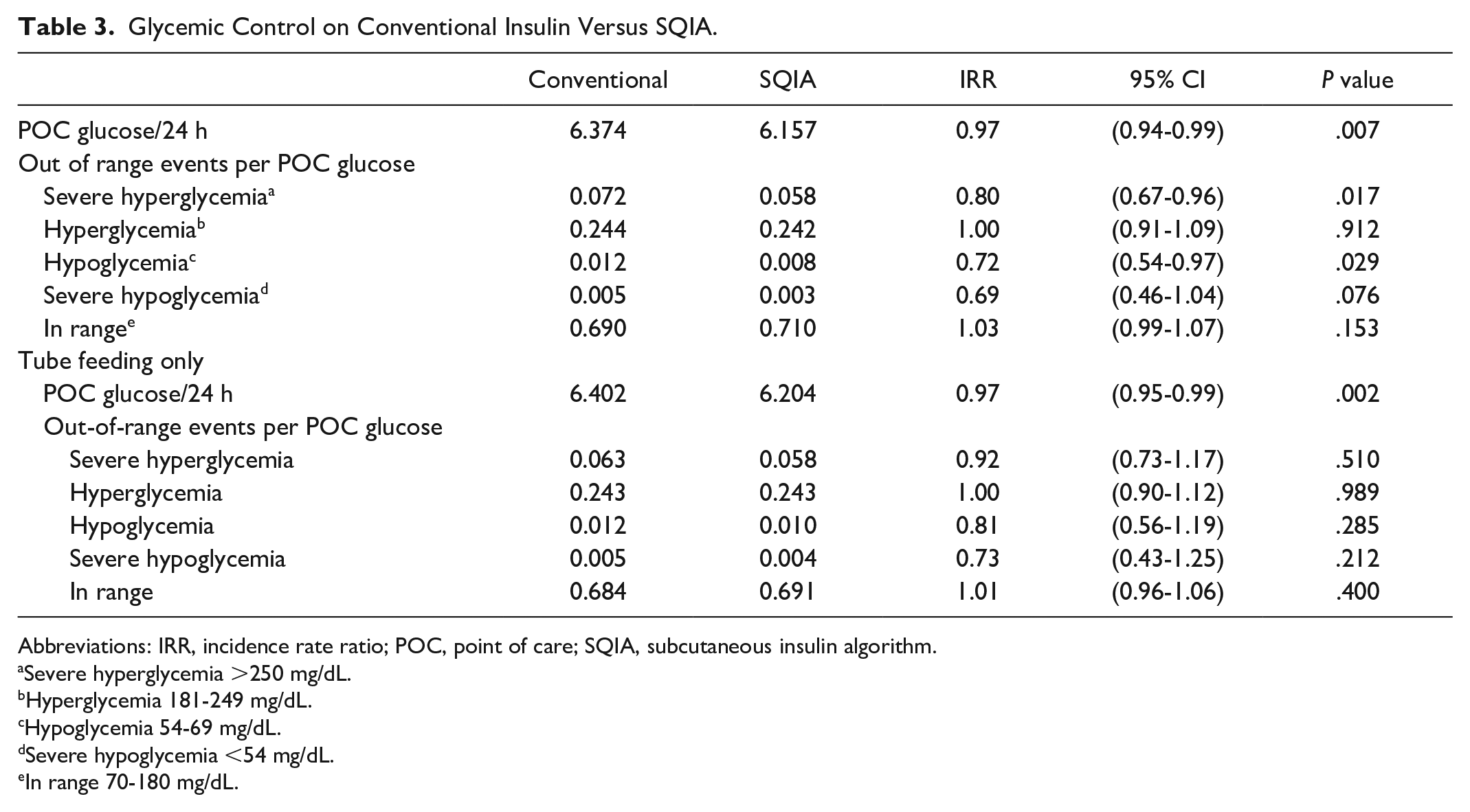
Abbreviations: IRR, incidence rate ratio; POC, point of care; SQIA, subcutaneous insulin algorithm.
Severe hyperglycemia >250 mg/dL.
Hyperglycemia 181-249 mg/dL.
Hypoglycemia 54-69 mg/dL.
Severe hypoglycemia <54 mg/dL.
In range 70-180 mg/dL.
Comparison of order changes showed that the conventional order set required more than 12 times the number of order changes than SQIA (incidence rate ratio [IRR] 12.5; 95% CI: 3.0-52.2, P = .001; Table 4).
Order Changes.
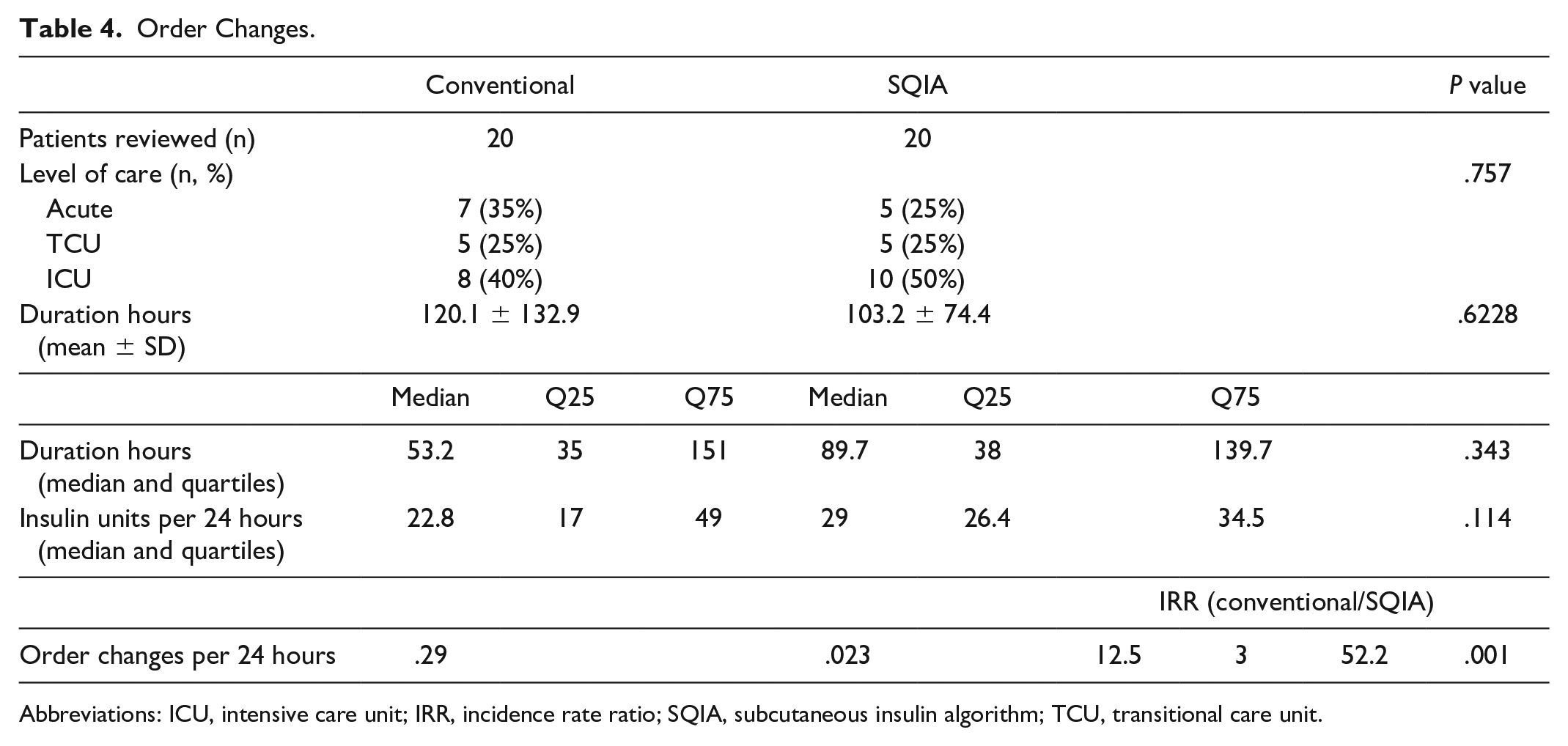
Abbreviations: ICU, intensive care unit; IRR, incidence rate ratio; SQIA, subcutaneous insulin algorithm; TCU, transitional care unit.
Discussion
Our prior studies demonstrated the feasibility of a self-titrating SQIA in a paper-based form prior to widespread EMR utilization and in a pilot program of an EMR-based SQIA.23,26 This study demonstrates the feasibility and effectiveness of a system-wide EMR implementation of the SQIA.
Glucose Management
Our study not only confirms the viability of SQIA as a strategy to manage inpatient glucose control but also supports SQIA as a safer alternative to conventional insulin dosing. Compared with conventional insulin dosing, the SQIA achieved a statistically significant decrease in both severe hyperglycemia (glucose >250 mg/dL) and hypoglycemia (glucose 54-69 mg/dL) and was noninferior in terms of in-range glucose measurements, hyperglycemia, and severe hypoglycemia. Of note, UCSF implemented an endocrinologist-led virtual glucose management service (vGMS) in 2013 that is automatically activated for patients with poor glycemic control (at least two POC glucose measurements <70 or >225 within 24 hours) and had achieved a 39% decrease in patients with hyperglycemia and a 36% decrease in hypoglycemia. 28 In the years before the introduction of the SQIA, while physicians were taught to aggressively rewrite insulin orders as needed to achieve glucose control, glucoses often remained high, and the vGMS was triggered and a note placed to suggest further insulin adjustments. After the implementation of the SQIA, with most patients on NPO, TPN, and TF moving to the SQIA, a patient in this group appearing in the daily high glucose vGMS report was a rare event. Thus, the benefit of the SQIA may be even greater in a different hospital system where there has not been extensive physician education and insulin orders are not guided by a vGMS.
The SQIA was also associated with higher insulin dosage rates for NPO and TPN intervals. This may be due to physicians practicing more conservatively and prescribing lower dosages to minimize risk of hypoglycemia while on high-risk, nonoral diets, particularly while NPO. The SQIA demonstrates the potential of the SQIA to appropriately increase insulin dosage to reduce severe hyperglycemia events, while reducing hypoglycemic episodes. Furthermore, the SQIA was able to achieve improved glycemic control with decreased variation in insulin dosing. The interquartile range for the SQIA insulin dosage is narrower than that of conventional insulin dosing (29.9 vs 37.8).
In many institutions, glucose management teams, physicians, nurse practitioners, bedside nurses, and pharmacists spend significant time dealing with glucose fluctuations through direct assessment of glycemic trends and manual adjustment and rewriting of insulin orders. As such, the SQIA may not only improve the effectiveness of glycemic control efforts, but it may also improve efficiency by decreasing provider time spent calculating and reordering insulin, reducing pages between bedside nurses and providers about adjusting insulin doses, and improving patient outcomes such as length of stay.
For purposes of our data presentation, we excluded patients who had either the automated algorithm or conventional insulin dosing ordered, but their glucose level did not rise high enough so that insulin dosing was required. Generally, glucose averages for hospitalized patients are based on all patients who have glucoses more than 120 mg/dL. Including patients not requiring insulin would have led to lower average glucoses but would not have reflected the impact of the algorithm.
Physician Efficiency
The SQIA led to improved physician efficiency, reducing the frequency of order modifications by a factor greater than 12 when using the SQIA, while also improving glycemic control. The SQIA may reduce the cognitive burden on physicians 29 and enhance clinical decision making in other aspects of patient care.
Implementation
Our findings that, in 68.5% of hospitalizations and 67.1% of eligible intervals, the physicians selected to use SQIA over conventional insulin dosing in the first year of rollout throughout the health system demonstrate the success and traction of our novel SQIA. Key components of our implementation include launching our pilot program at a single hospital; providing training to nurses, physicians, and pharmacists; creating an active log of issues and feedback gathered from staff; and implementing real-time changes. 26
Optimization
The data presented here represent year 1 of full implementation across the UCSF Health system. We have followed Gall’s Law that A complex system that works is invariably found to have evolved from a simple system that worked. A complex system designed from scratch never works and cannot be patched up to make it work. You have to start over with a working simple system.
Year 1 represented a highly developed, yet simple algorithm. In the subsequent two years, the automated system has been programmed to determine whether the patient is receiving enteral feeding and, if so, determine whether the feedings have been interrupted. With this change and a change in the lower end glucose cutoffs, we hope to show a decrease in the already low rate of hypoglycemia. In addition, changes have been made in the algorithm to be more aggressive in increasing insulin doses when glucoses remain high.
Limitations
One limitation of our study was that the selection of patients for either the SQIA or conventional insulin order set was not randomized, but rather, was at the primary physician’s discretion. Reassuringly, most patient characteristics were ultimately similar in the two groups, except for length of stay and level of care at admission. The conventional insulin group had a longer median length of stay than the SQIA group, which may be explained by the conventional insulin group having a greater proportion of patients initially admitted to critical care as well (44.7% vs. 40.5%). However, a greater proportion of eligible critical care intervals were for SQIA than for conventional insulin (42.4% vs. 38.1%). This suggests that critical care physicians selected the SQIA over the conventional insulin order set and that fewer severe hyperglycemia and hypoglycemia episodes occurred even in sicker patients. Future research could randomly assign patients to either the SQIA or conventional insulin to address this limitation.
Future research could control for additional variables, including prior diabetes diagnosis, continuation of home diabetes medications, and admission diagnosis to further elucidate utilization cases for the SQIA. In addition, future research could conduct a subgroup analysis of patients with glucocorticoid use. Furthermore, given a single patient may have multiple eligible intervals, future research could compare glycemic outcomes within the same individual, when assigned to SQIA versus conventional insulin within the same admission, although this may become increasingly difficult as the SQIA is now the predominant form of treatment in these patients.
Conclusions
Our findings suggest benefits of more widespread implementation in similar patient populations at other health systems and the potential for its application in patients on lower risk diets. Future research should study implementation of the SQIA in patients on more liberalized diets. In addition, we would anticipate that the typical insulin therapeutic inertia seen on adjusting insulin doses in many institutions would be overcome by the decreased need for adjusting the insulin doses.
Supplemental Material
sj-docx-1-dst-10.1177_19322968241232673 – Supplemental material for Novel Automated Self-adjusting Subcutaneous Insulin Algorithm Improves Glycemic Control and Physician Efficiency in Hospitalized Patients
Supplemental material, sj-docx-1-dst-10.1177_19322968241232673 for Novel Automated Self-adjusting Subcutaneous Insulin Algorithm Improves Glycemic Control and Physician Efficiency in Hospitalized Patients by Paras B. Mehta, Michael A. Kohn, Esther Rov-Ikpah, Craig San Luis, Craig Johnson, Gwendolyn Lee, Suneil Koliwad and Robert J. Rushakoff in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-2-dst-10.1177_19322968241232673 – Supplemental material for Novel Automated Self-adjusting Subcutaneous Insulin Algorithm Improves Glycemic Control and Physician Efficiency in Hospitalized Patients
Supplemental material, sj-docx-2-dst-10.1177_19322968241232673 for Novel Automated Self-adjusting Subcutaneous Insulin Algorithm Improves Glycemic Control and Physician Efficiency in Hospitalized Patients by Paras B. Mehta, Michael A. Kohn, Esther Rov-Ikpah, Craig San Luis, Craig Johnson, Gwendolyn Lee, Suneil Koliwad and Robert J. Rushakoff in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-3-dst-10.1177_19322968241232673 – Supplemental material for Novel Automated Self-adjusting Subcutaneous Insulin Algorithm Improves Glycemic Control and Physician Efficiency in Hospitalized Patients
Supplemental material, sj-docx-3-dst-10.1177_19322968241232673 for Novel Automated Self-adjusting Subcutaneous Insulin Algorithm Improves Glycemic Control and Physician Efficiency in Hospitalized Patients by Paras B. Mehta, Michael A. Kohn, Esther Rov-Ikpah, Craig San Luis, Craig Johnson, Gwendolyn Lee, Suneil Koliwad and Robert J. Rushakoff in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
EMR, electronic medical record; ICU, intensive care unit; IV, intravenous; MAR, medication administration record; NPO, nil per os; POC, point of care; RR, incidence rate ratio; SQIA, subcutaneous insulin algorithm; TF, enteral tube feed; TPN, total parenteral nutrition; UCSF, University of California, San Francisco; vGMS, virtual glucose management service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.