
Abstract
Background:
Acclimating to a new technology device, such as a continuous glucose monitor (CGM), can be challenging. Current resources may not sufficiently answer questions patients living with diabetes (PWD) may have. We asked how we might improve the process to onboard a PWD to CGM. Our specific aims were (1) to develop, employing a co-designing approach, a prototype of an app for facilitating onboarding to CGM and (2) to obtain early feedback on its usability.
Methods:
We applied a human-centered design (HCD) approach; this process first seeks to deeply understand the unmet needs and frustrations users face. After wearing a demonstration CGM; observing PWD onboarding with health care professionals (HCPs) in clinic; and interviewing 8 PWD and 2 HCP, we developed, tested, and refined a low-fidelity prototype of a clickable app. With insights from this initial round of feedback, we then created a high-fidelity prototype with 3 key features: (1) individual entry of goals and questions; (2) a daily progress tracker for these goals; and (3) a community portal that facilitates exchange of questions and answers. We used the validated System Usability Scale (SUS) to quantify user feedback.
Results:
Focus group participants found our early app to be usable and acceptable. Measurement of usability by the SUS yielded a score of 74, which is above average (68) reported for all applications tested, per usability.gov.
Conclusions:
Our early prototype app is a more personalized, additional tool that could bridge an information and support gap for patients who are new to CGM. This app could also help PWD on an ongoing basis, by evolving with them to enhance ease and engagement with diabetes self-management.
Keywords
Introduction
Although technology has simplified the glucose monitoring process, barriers to usability and access may hamper starting and consistently using devices. Continuous glucose monitors (CGM) and flash monitors can be daunting to use effectively, especially initially. Some patients living with diabetes (PWD) may find the initial print and video training resources provided to be insufficient and feel that “You have to go find it yourself.” 1
Despite advances in medications and devices, 17% of youths with type 1 diabetes (T1DM) and 21% of adults with T1DM are at goal hemoglobin A1c (HbA1c). 2 Only 50% of US adults with type 2 diabetes (T2DM) are at goal HbA1c. 3 Although an estimated 90% of diabetes care is self-management, 4 support for PWD is vital. On average, PWD only see their health care professional (HCP) teams for approximately 2 hours each year. Diabetes is a disease that demands significant vigilance to glucose readings, medication titration, diet, and exercise. Myriad daily challenges, such as family and career, can push these self-management tasks to the background. Time, distance, or lack of Internet access may hamper in-person or virtual support by HCP teams. Patients living with diabetes may thus have suboptimal clinical outcomes and quality of life. Devices or apps can help save time and reduce mental burden. Continuous glucose monitor alarm fatigue, or devices being conspicuous and serving as reminders to others of living with this chronic disease, can cause or increase friction that limits or discontinues use. Most are built without patient or HCP input.5,6
Human-centered design (HCD), a problem-solving method focused on people to develop solutions customized to their needs and goals,7,8 could help PWD better harness the promise of diabetes technology to improve glycemic control and quality of life. Human-centered design is a continuous, nonlinear, iterative process that aims to understand the individual user, challenge assumptions, and redefine problems.9-11 Figure 1 shows a description of the steps. HCD has been termed “an essential tool for simplifying and humanizing.” 12 Although widely applied in diverse fields, from products to architecture, HCD has more recently emerged as a critical tool in health care improvement and research.13,14 HCD starts with gathering and applying evidence of how individuals actually interact with a product or service, instead of a theoretical picture. 10 By directly observing and speaking with the users, researchers discover pain points that individuals may not have considered or may have been unaware. Multiple potential solutions are then rapidly tested and refined. As both a process and a framework to guide the steps from challenge to solutions, HCD is particularly suited to diabetes, as there is no one-size-fits-all approach, and it is crucial to understand PWD’s goals. 15
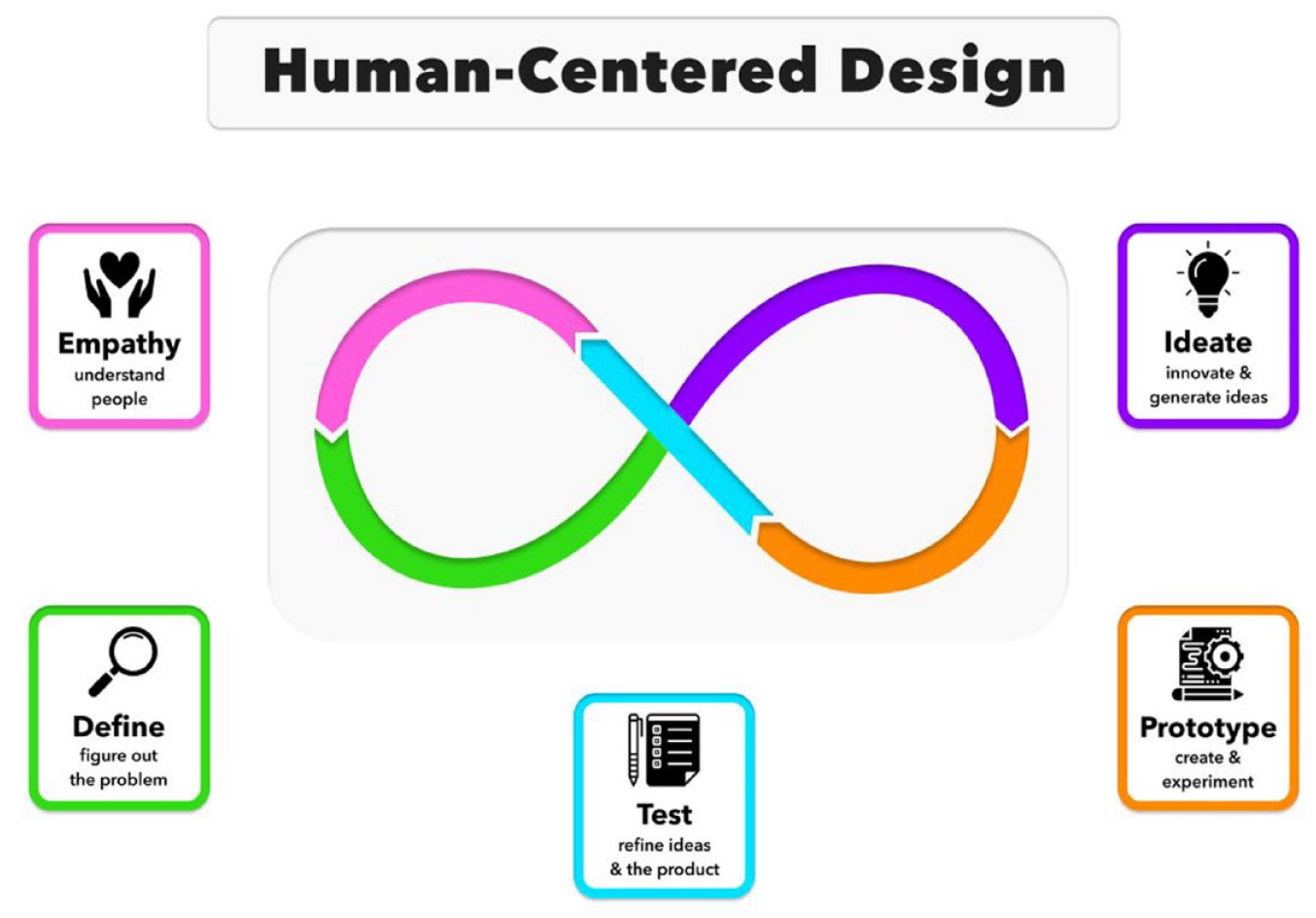
The 5 steps of the HCD process we applied based on design thinking. 16 These are not unidirectional, and subsequent stages can help refine earlier steps. Figure courtesy of Ashley DuBord.
HCD has been employed in health care, including an educational brochure for breast cancer patients; 17 developing a face mask for maxillary malocclusion; 18 a cardiovascular mobile health decision support tool in a resource-limited environment; 19 and a website to help enhance diabetes self-management.20,21 Although there has been discussion of the importance of PWD’s perspective in developing diabetes technology, 22 few studies have specifically examined HCD applied to diabetes.10,23-25
We investigated whether we could apply an HCD method and process to improve orienting PWD to CGM. Our specific aims were (1) to develop, applying a co-designing approach, a prototype of an app for facilitating onboarding to CGM and (2) to obtain early feedback on its usability.
With input from patients, community leaders, and advocates, a registered nurse who works with PWD, students learning design thinking, a design thinking practitioner, and a physician, we co-developed a clickable prototype app. GluClose combines: (1) PWD’s active participation, including entering their goals, motivation, and questions; (2) trackers recognizing progress on these individually-selected goals on a daily, regular basis, over the short- and long-term; and (3) a forum to ask questions, which fellow PWD can respond to; and HCP can review and endorse for accuracy. This app can complement and add to the patient onboarding experience, with potential for ongoing use. Our early study demonstrates that our prototype app has high usability and is a promising platform for further development and testing.
Methods
Study Design
The HCD process begins with an interest in deeply understanding our PWD’s goals and objectives. Sparked by the question, “How might we improve PWD’s experience of initiating CGM?,” we sought to better appreciate and capture the daily challenges PWD face in managing their diabetes. We assembled a team of University of California, San Diego (UCSD) undergraduates with interest and training in design thinking. Dexcom (San Diego, California) and Abbott Diabetes Care (Alameda, California) donated demonstration versions of the Dexcom CGM and FreeStyle Libre flash monitor, or intermittently scanned continuous glucose monitor (isCGM). These simulated all aspects of the experience of using CGM and isCGM, except testing glucose levels (the demonstration versions did not allow actual glucose measurements). Wearing one helped facilitate empathy with PWD’s daily experience of using such a device. The Human Research Protections Program at the University of California, San Diego, reviewed our research plan and deemed our study to be human subjects research that is exempt from the requirements of the Federal Policy for the Protection of Human Subjects.
Study Settings
The study was conducted at the UCSD Design Lab. We interviewed participants- on Zoom. One student (Ms Mingjin Zhang) observed patients’ diabetes clinic visits with an endocrinologist during 2 separate, 30-minute appointments at University of California, San Diego Health. This physician also lives with T1DM, and thus provided a unique perspective as both a PWD and HCP. When discussing CGM with PWD, she would disclose that she herself also wore one.
Study Procedure
We also interviewed 10 participants, 8 of whom are PWD, or their caregivers, and 2 HCP (a nurse and a physician). All of the volunteers who are PWD are living with T1DM. Three PWD- were newly diagnosed; 4 PWD- had been diagnosed previously. The PWD ranged in age from 2 to 65 years. We asked each participant detailed questions about their experiences with starting to acclimate to CGM, including frustrating aspects. Three main themes emerged: (1) learning and keeping up to date on information can feel overwhelming; (2) PWD may find themselves seeking answers to questions on their own outside of clinic visits, such as via online or virtual interactions with individuals also living with DM; and (3) PWD may perceive a disconnect in communication with their HCP teams.
Our team conducted an analysis and synthesis of the observations and interviews to define the problem statement and identify early concepts to improve the experience of CGM onboarding and learning. With ongoing experimentation through sketches and prototypes, we developed the earliest version of a prototype, one that is low-fidelity, considered a rough draft of a solution (Figure 2).
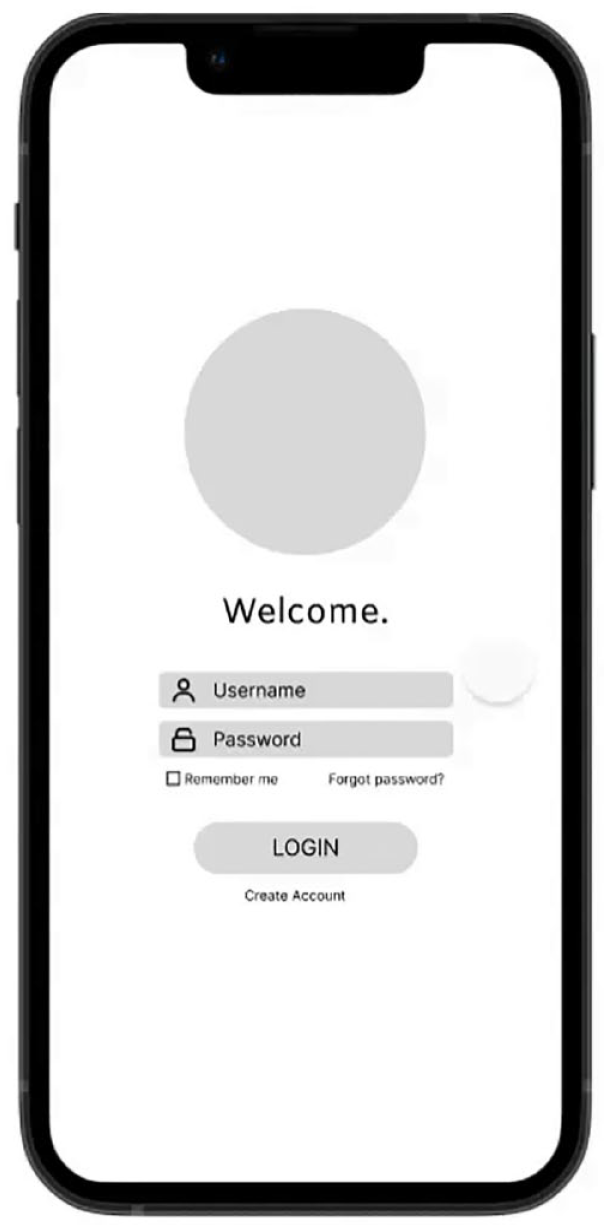
An example from our low-fidelity prototype.
We then conducted 2 rounds of testing with our participants to refine our prototype. We examined areas such as layout and design, workflow, usability, accessibility, and design interaction (Figure 3 displays user testing questions, and Figure 4 depicts a change that resulted from participant testing).
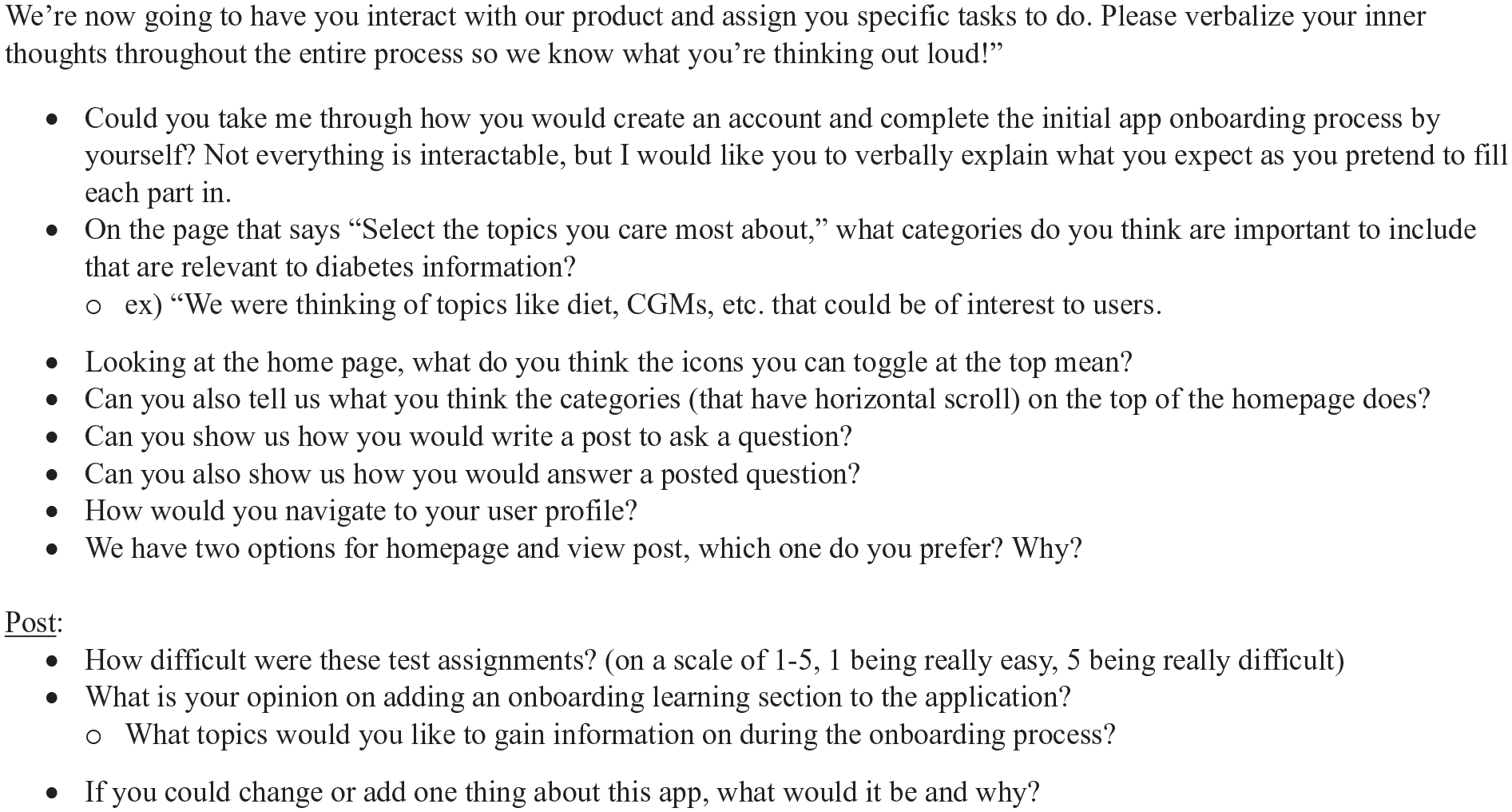
User testing questions to gain insight for refining our low-fidelity prototype.
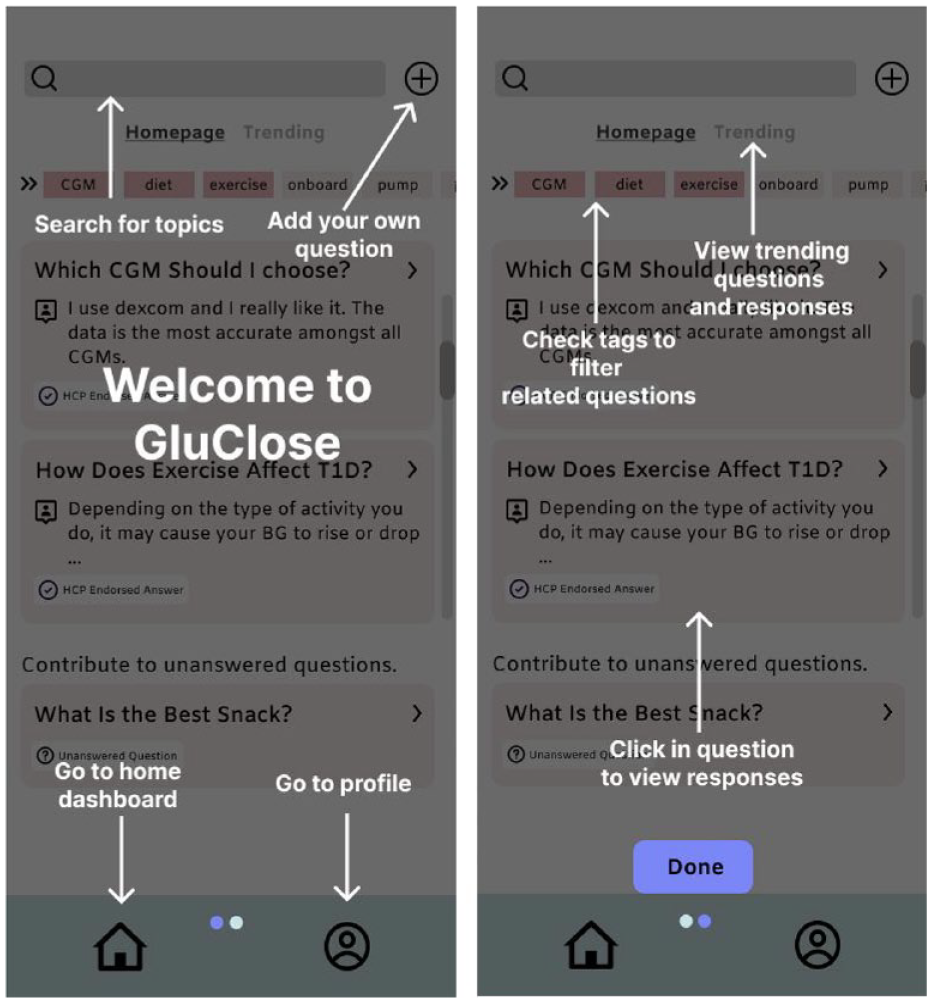
An example of explanatory overlays (white text with arrows), which study participants suggested for ease of use.
We next collated these insights to construct user personas, which are archetypes of patients, that help teams avoid designing for atypical or idealized users, who are more removed from actual patients (Figure 5).
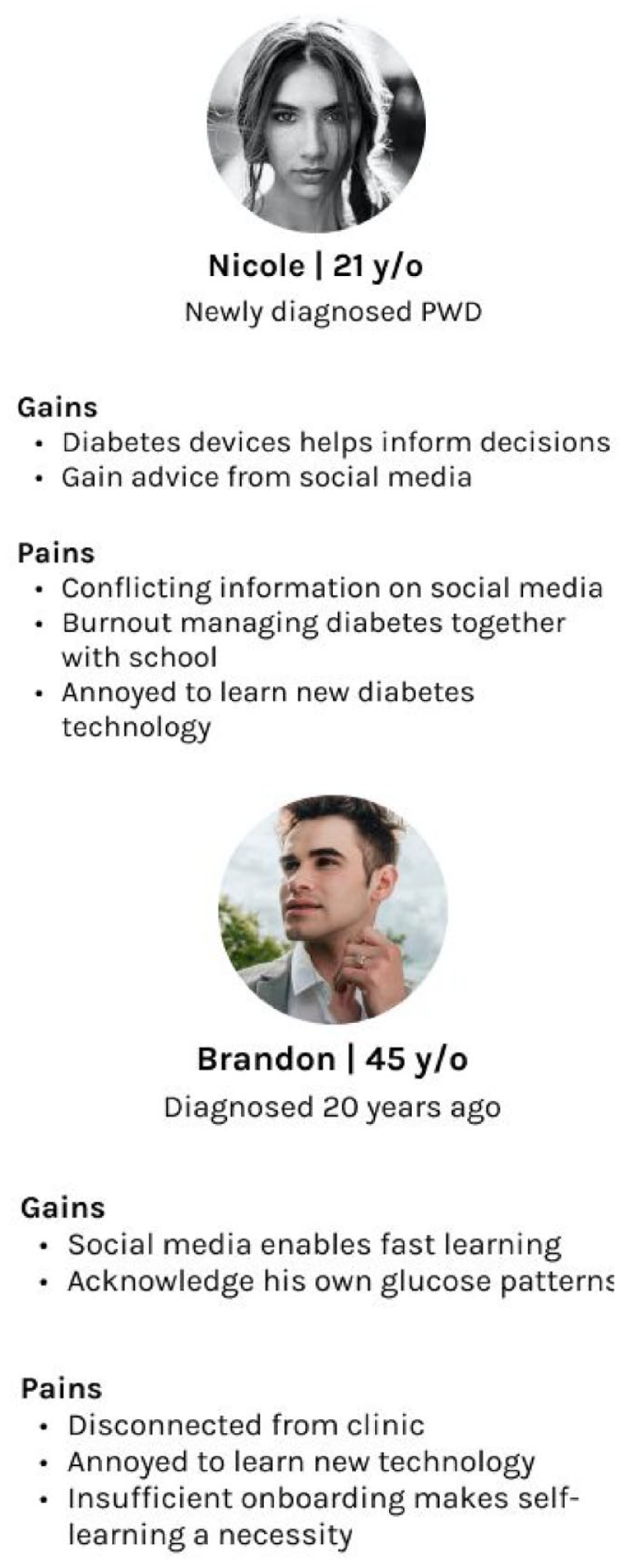
Personas from participant interviews. The insights from these interviews helped form the low- and high-fidelity prototypes of our app.
These personas served as foundations for storyboards, which are visual representations of a user’s experience and potential use cases. These help visualize and further explore a user’s journey interacting with a device, as well as further uncover potential problems. Personas come from secondary research and interviews. Trust and peer-to-peer advice play significant roles in endorsing answers on the community forum. We confirmed these themes during our interviews with our participants.
We included the various stakeholders throughout the design process, which included weekly stand-ups: meetings during which the team provided progress updates, discussed the latest research findings, and design iterations. We conducted 2 stakeholder workshops at the midpoint and end of the process to align on the prototype. We used a prioritization framework (testing the usability of individual features, to better understand users’ preferences, and thus help decide what to focus on next) at the midpoint workshop with HCP, PWD, and invited community leaders to support the design decisions. The feedback from both PWD and HCP provided overall design direction, user interface, and potential value for the high-fidelity prototype (see Figure 6).
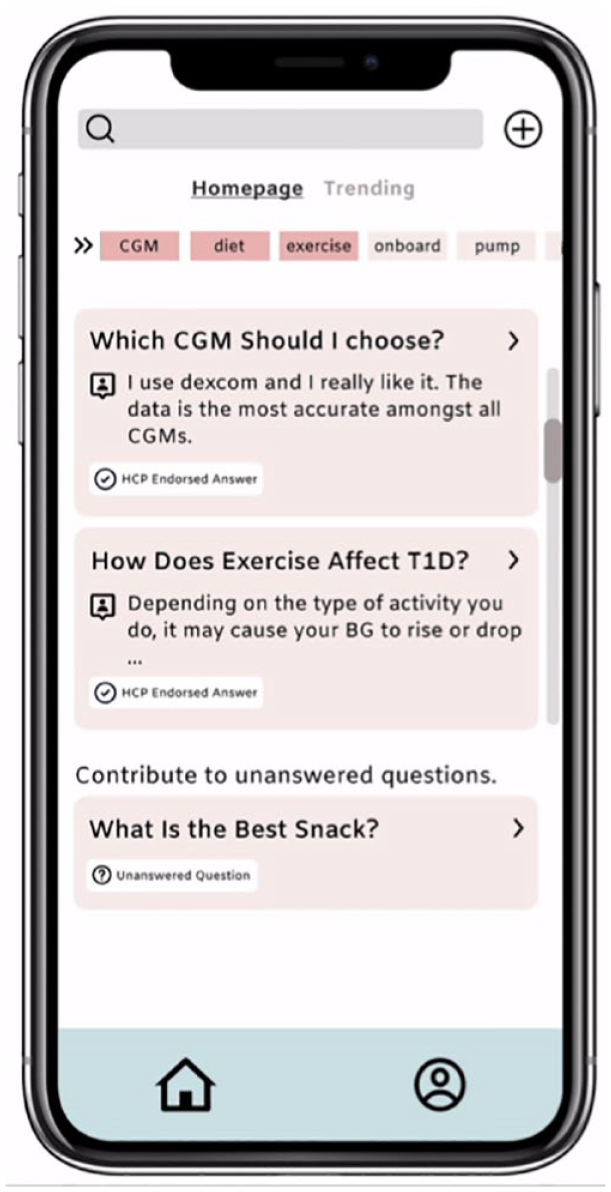
A sample screen from our high-fidelity prototype.
During user testing, our participants remarked that they could see the potential for experiencing more individualized communication with their HCP; a greater sense of comfort in their ability to share and learn from other fellow PWD; and feeling that they received more CGM onboarding support, along with ongoing learning. We included this as one of the core features of this prototype app, along with narrative sections for entering goals and questions, and a daily tracker to record progress toward goals set by PWD.
Results
As a key criterion is ease of use, we asked participants to rate the app during user testing using the System Usability Scale (SUS) (see Figure 7 for the questions).26-28 This 10-item questionnaire is considered the industry standard for assessing products or websites. The SUS can be valid for as few as 2 participants, although 6-20 are suggested. Our prototype received an average SUS of 74 (from 7 participants), which is higher than the average industry standard device score (68) reported by usability.gov. We also assessed ease of use on a scale of 1 to 5, with 1 being easiest to use; 6 participants scored our prototype a 1, and 1 rated it as 2.
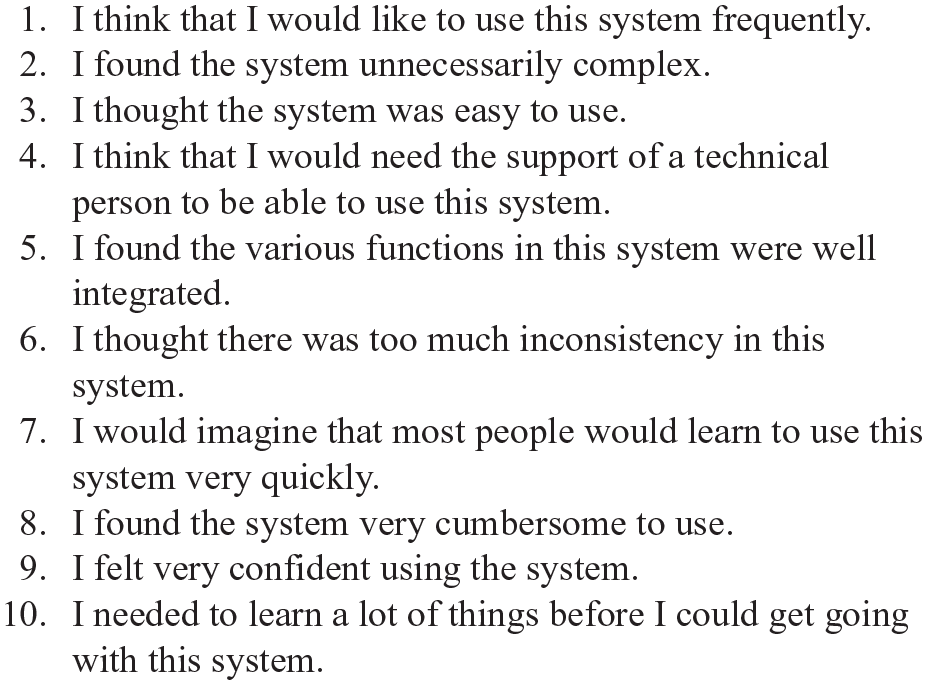
The System Usability Scale— each item, is scored on a 5-point scale, from 1 (strongly disagree) to 5 (strongly agree).
Participants provided comments; these included a recommendation to “figure out how to drive user engagement; we want people to come back and use it as an informational resource” and a suggestion to allow patients to exchange messages amongst themselves to “provide a larger sense of community, mentorship and learning.”
Discussion
Our prototype app supports both active individual and community participation in onboarding as a new CGM user with 3 key features, to facilitate a more personalized experience: (1) a narrative section for entering actionable goals and questions; (2) a daily progress tracker; and (3) a community forum, for asking for and providing help. Our participants identified a need for and inspired the community portal, which can provide opportunities to exchange information with their peers on diabetes-related topics; and explore answers endorsed by HCPs. The SUS score for GluClose was 74, which is considered above average on a widely-used, validated questionnaire.26-28
Our study extends the efforts and findings of other groups, particularly Petersen and Hempler, who employed a design thinking approach in developing an app for patients newly diagnosed with T2DM. 24 After gathering insights from interviews of 12 patients, the authors developed a prototype app with 5 main functions: overview of diabetes activities after diagnosis; recording of health data; reflection games and goal setting; knowledge games; and recording of psychological data such as sleep, fatigue, and well-being. Fourteen PWD tested this over 4 weeks. The authors noted that PWD favored apps with multiple functions; having physicians recommend and introduce apps is pivotal; and that tailoring apps to increase individual personalization is important. 24
A recent preliminary study, Overcoming Barriers and Obstacles to Adopting Diabetes Devices (ONBOARD), demonstrated acceptability, feasibility, and increased time in range (TIR) (70-180 mg/dL, P- = .03) for 22 adults living with T1DM who were within their first year of using CGM. 29 The participants underwent 4 60-minute telehealth sessions that covered: physical barriers; social barriers; managing CGM data; and trust in CGM accuracy.
We focused on a distinct subgroup: designing for those living with diabetes who were new to CGM, who reported at times feeling isolated due to uncertainty about resources to consult, beyond those initially offered by their HCP and device manufacturers; a and feeling that there is a lack of consistent and ongoing information in between clinic visits. Participants advised that a community forum would be a pivotal feature. Patients living with diabetes should have a supportive, safe environment to discuss questions and concerns—what one - study volunteer termed “real talk.” 29 Our prototype could potentially improve patient experience and motivation for CGM use by offering online peer-to-peer support combined with HCP endorsement.
Limitations of this study include a small sample size. The qualitative feedback from our participants is subjective, and we would need to assess individuals’ ratings of the prototype with further formal measures.
Patients value peer-to-peer health advice as a crucial supplement to information they receive from HCP teams. In a recent phone survey, 1 in 4 Internet users living with hypertension, diabetes, cardiac disease, pulmonary disease, cancer, or another chronic ailment reported going online to find other individuals with similar health concerns.30,31 Numerous discussion boards exist, but may not be vetted. Health care professionals can comment on responses. Yet, HCP already grapple with multiple time-consuming tasks, including spending hours on electronic medical records before and/or after clinic hours. How willing HCP are able to engage on this additional platform is a vital, open question. Future investigations could further explore balancing participants’ preference for interacting with HCP on the app, with the already significant time constraints HCP have to navigate. Whether artificial intelligence (AI) could assist HCP is an interesting area to further explore.
Measures to protect the privacy of all information patients enter would also be crucial. Any app must have a streamlined interface and simple process to navigate, to be as accessible and appealing to as a wide array of individuals’ experience and comfort level with technology as possible. Future work should draw on input from a similarly diverse cohort of participants, including those who are less familiar with technology, or even app nonusers, to facilitate such factors.
Another area to further consider and explore is patient engagement, defined as individuals being “equipped, enabled, and empowered” concerning their own health. This proactive stance has been shown to be linked with improved outcomes.32-34 Parker and colleagues introduced the term “celebratory health technology”: “highlighting positive interactions, meanings and values.” 35 Health care professional interactions with patients, in clinic or in written materials, are often couched in proscriptive terms. Adding the positive aspect, including asking PWD what they have improved upon since the last visit, what is going well, or reminding PWD to recognize and appreciate the progress they have made are equally important. Our app prototype provides PWD the ability to do so in the narrative section, the personal progress tracker, and the community portal.
Testing this prototype in a large number of PWD-, for a substantive period of time, would also be essential and will be the subject of future work. Further studies that employ an HCD approach 36 will continue to contribute to enhancing our understanding of the strengths and limitations of this process. Altman and her team noted that there are currently few HCD studies that are large, randomized clinical trials. 36 Investigations that directly compare HCD with traditional studies would also be critical.
To our knowledge, this is the first known study of employing HCD to enhance CGM onboarding for individuals living with diabetes. We must leverage PWD’s perspective in developing digital health solutions that reduce the gaps between daily care and clinic, to help enhance motivation, education, and self-management support. Technology cannot by itself provide motivation or spark engagement; the tools can supplement traditional resources, such as peer-to-peer exchanges. Digital resources could enhance clinic visits with HCP by helping PWD track and recognize progress, ask questions, and remind them of their underlying drivers for striving for their goals. Applying an HCD process, we found that this prototype could potentially help with onboarding and continue to assist on an ongoing basis. By enhancing the patient’s experience of a self-management task of monitoring glucose, technology can open a new way to greater ease and engagement.
Conclusions
Any tool, including an app, is only as useful as it is accessible, engaging, and inviting. Technology should not only be appealing initially, but also continue to facilitate consistent, long-term use. Potential obstacles to successfully starting or sustaining use of diabetes technology, such as CGM or isCGM, can be countered by technology that more fully considers and applies PWD’s perspective. Being equipped with knowledge and a sense of support by a community could bolster confidence and empower a user to more fully benefit from diabetes health solutions.
Footnotes
Acknowledgements
The authors gratefully acknowledge the patients who volunteered for our study. Kacey Creel of Diversity in Diabetes assisted with connecting us with patients. Abbott Diabetes Care and Dexcom generously donated demonstration versions of continuous glucose monitoring devices. The authors appreciate the contributions of each of the students on our team: Alfonso Alfonso, Goldie Chu, Grayson Emery, Sam Wong, Annie Ye, and Wanting Yang. The authors also thank Eliah Aronoff-Spencer, MD, for reviewing the manuscript, for providing suggestions, and for for his providing study staff time and resources that were crucial to this project’s success.
This publication is the result of work supported with resources by the Veterans Administration San Diego Healthcare System; the contents do not represent the views of VA or the United States Government.
Abbreviations
DM, diabetes mellitus; HCD, human-centered design; CGM, continuous glucose monitor; PWD, patients living with diabetes; HCP, health care professional
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a University of California, San Diego—Accelerating Innovations to Market Grant.