
Abstract
Background:
With automated insulin delivery (AID) systems becoming widely adopted in the management of type 1 diabetes, we have seen an increase in occurrences of rebound hypoglycemia or generated hypoglycemia induced by the controller’s response to rapid glucose rises following rescue carbohydrates. Furthermore, as AID systems aim to enable complete automation of prandial control, algorithms are designed to react even more strongly to glycemic rises. This work introduces a rebound hypoglycemia prevention layer (HypoSafe) that can be easily integrated into any AID system.
Methods:
HypoSafe constrains the maximum permissible insulin delivery dose based on the minimum glucose reading from the previous hour and the current glucose level. To demonstrate its efficacy, we integrated HypoSafe into the latest University of Virginia (UVA) AID system and simulated two scenarios using the 100-adult cohort of the UVA/Padova T1D simulator: a nominal case including three unannounced meals, and another case where hypoglycemia was purposely induced by an overestimated manual bolus.
Results:
In both simulation scenarios, rebound hypoglycemia events were reduced with HypoSafe (nominal: from 39 to 0, hypo-induced: from 55 to 7) by attenuating the commanded basal (nominal: 0.27U vs. 0.04U, hypo-induced: 0.27U vs. 0.03U) and bolus (nominal: 1.02U vs. 0.05U, hypo-induced: 0.43U vs. 0.02U) within the 30-minute interval after treating a hypoglycemia event. No clinically significant changes resulted for time in the range of 70 to 180 mg/dL or above 180 mg/dL.
Conclusion:
HypoSafe was shown to be effective in reducing rebound hypoglycemia events without affecting achieved time in range when combined with an advanced AID system.
Keywords
Introduction
Automated insulin delivery (AID) systems represent a game-changing approach to treating type 1 diabetes (T1D).1-3 These advanced closed-loop systems aim to maintain the blood glucose (BG) level in a healthy range by integrating continuous glucose monitoring (CGM) sensors with insulin pumps through control algorithms that automatically regulate insulin infusion. 3 AID systems can operate in a hybrid closed loop (HCL) mode, requiring manual announcements, or a full closed loop (FCL) mode, which may not require user interaction. 1 Currently, commercially available AID systems are labeled for HCL use, with ongoing research into the FCL mode.1,2,4 The Inreda system has become the only FCL AID system approved by the European Commission.3,5
While AID systems offer significant benefits in improving glycemic control and reducing the burden of constant diabetes management, they are not exempt from limitations. 6 One crucial consideration is the risk of hypoglycemia, a condition that develops as an interplay of insulin excess and the compromised glucose counter regulation in T1D 7 and that is linked to consequences such as dizziness, blurred vision, cognitive impairments, and in extreme cases, seizures and diabetic coma.6,8-10
Different strategies have been devised to prevent hypoglycemia episodes in diabetes management. Monitoring systems now incorporate low-threshold alerts and/or hypoglycemia prediction alarms to enable users to take proactive measures.11,12 Personalized hypoglycemia predictive alerts have also been introduced using glucose-insulin models or long short-term memory models to predict glucose trends.9,13 In addition, different algorithms have been developed and integrated into AID systems to proactively reduce or suspend insulin infusion when hypoglycemia is predicted or present.8,10,14-19
Despite these efforts, hypoglycemia events can still occur. When they do, people with T1D usually take fast-acting (or rescue) carbohydrates to rapidly restore normoglycemia.20,21 However, this sudden change in BG levels can trigger an excessive control response, potentially inducing a second hypoglycemia episode. Lee et al 22 reported this oscillatory rebound hypoglycemia during a clinical validation of their HCL controller, where the controller overreacted to rapid BG increases after rescue carbohydrates. To address this issue, a dynamic insulin-on-board constraint was proposed to minimize the likelihood of controller-induced hypoglycemia following a rapid rise of glucose levels. 22 In addition, recent data from a clinical trial 4 (ClinicalTrials.gov ID NCT04877730) evaluating HCL and FCL modes of the UVA AID system revealed instances of rebound hypoglycemia (see the Supplemental Material for an example of rebound hypoglycemia observed in real-life data). Specifically, there were five rebound events during the HCL mode and three in the FCL mode across the 35 subjects, and 9% of hypoglycemic episodes were attributed to rebound lows induced by controller overcorrection. This underscores the need for strategies to counteract the controller’s overreaction to rescue carbohydrates.
In this work, a controller agnostic HypoSafe module is developed to prevent rebound hypoglycemia. Based only on preceding glucose conditions, HypoSafe sets constraints on subsequent control actions without relying on manual user inputs. To evaluate the efficacy of this strategy, we integrated HypoSafe into the University of Virginia (UVA) AID system 23 within the Food and Drug Administration (FDA)-accepted UVA/Padova T1D simulator. 24 Rebound hypoglycemia events and glucose outcome metrics are reported for two different simulation scenarios: one including unannounced meals and another including an over-sized manual bolus.
Methods
HypoSafe Module
The primary goal of the HypoSafe module is to prevent rebound hypoglycemia by informing the system with conditions preceding the current glucose value and then determining when to allow full control actions. To that end, a dynamic upper bound over the control action is imposed. It is to consider both basal and bolus actions, especially in the case of FCL controllers that can react to BG rises by triggering a bolus.
Based on the analysis of a prior glucose trace, the following design principles are desired: (1) the lower the glucose levels have been in the recent past, the stricter the constraint should be; (2) the lower the current glucose value, the stricter the constraint; (3) if minimum glucose in the recent past is at or above the glucose target, then the constraint is maximum, allowing for full control actions; and (4) if hypoglycemia is detected in the recent past, there should not be any insulin delivery above the subject’s predefined basal rate profile
Following these principles, the safety layer is then designed to apply an exponential decay constraint over the insulin delivery dose as a response to the minimum glucose value recorded in the last hour

with
HypoSafe can be applied to both basal and bolus commands with independent boundary constraints. For instance, in Figure 1, the set of curves depending on
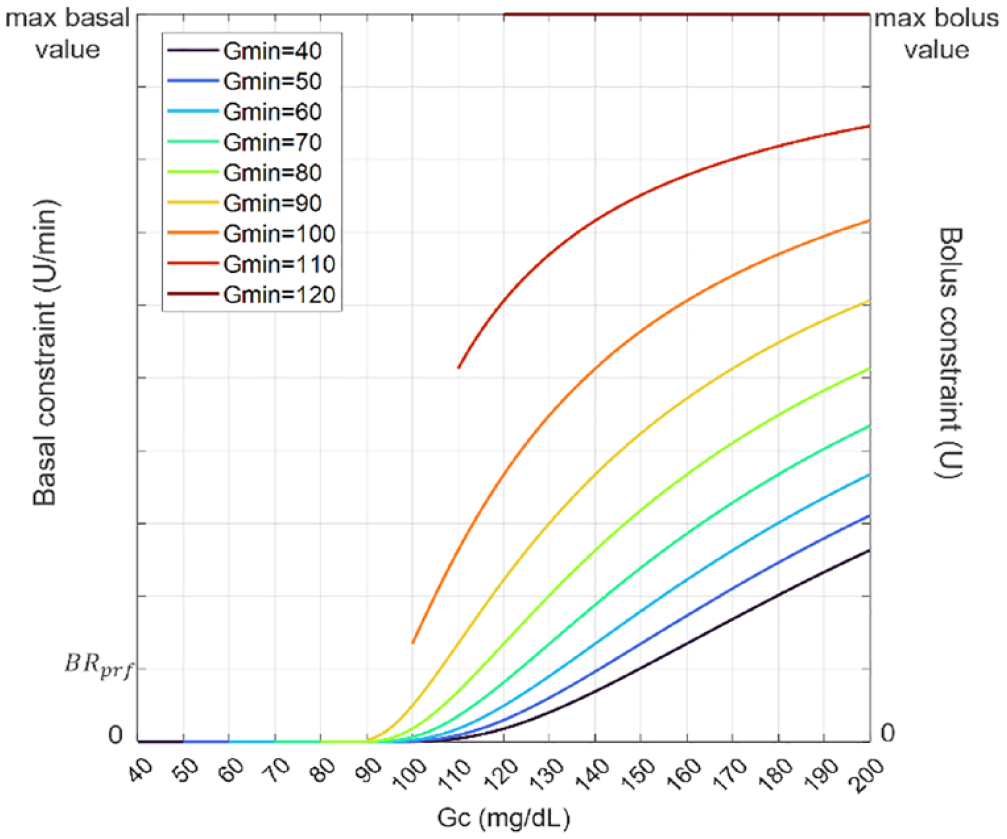
HypoSafe constraint for different values of
Integration With a Fully Closed-Loop Algorithm
The UVA AID system integrates (1) a safety system for imminent hypoglycemia mitigation (legacy SSM), (2) a hyperglycemia mitigation system (HMS), (3) a bolus priming system (BPS) to compensate for abrupt positive disturbances, and (4) a model predictive control (MPC) algorithm for background insulin regulation.
In summary, the MPC relies on a mathematical description of the insulin-glucose interaction to calculate an optimal control policy of insulin deviations from the subject’s predefined
To prevent rebound hypoglycemia from basal and bolus commands, HypoSafe is coupled to both the MPC and BPS as depicted in Figure 2. For basal, the constraint was set to allow a maximum of 10 times the subject-specific
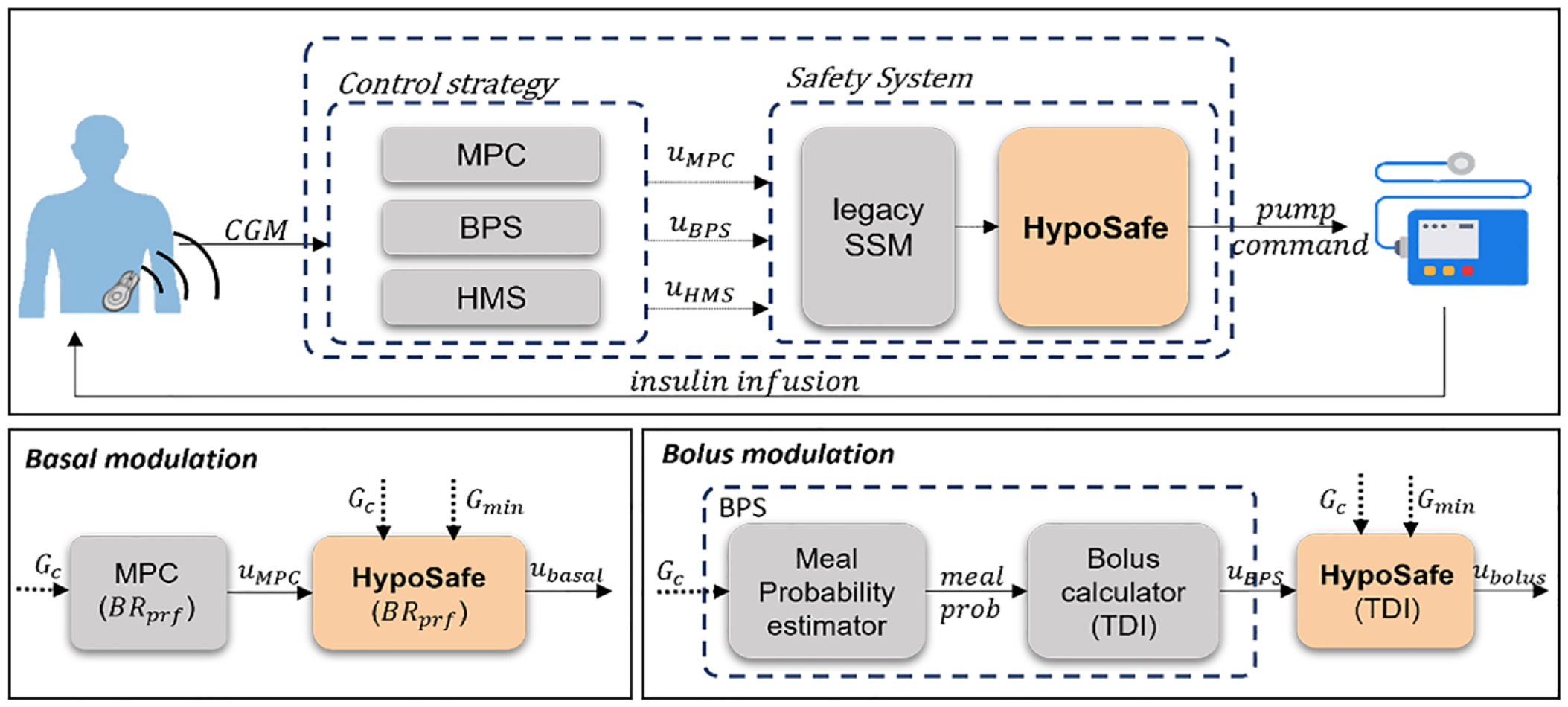
Upper panel: Integration of HypoSafe into the UVA AID system. Bottom-left panel: Basal modulation by constraining the output of the MPC. Bottom-right panel: Bolus modulation by constraining the output of the BPS.

with
In case of the BPS, the constraint was defined to represent fractions of the subject’s TDI (U) allowing up to 10% of its value

The final priming bolus is given by
Simulation Scenario and Outcomes
Experiments were run on the 100-adult cohort of the FDA-accepted UVA/Padova T1D simulator to assess the efficacy of the HypoSafe module. Two different scenarios were considered: (1) a nominal scenario consisting of 30 hours with three unannounced meals provided to each subject at 7 hours, 13 hours, and 19 hours with carbohydrate content of 70, 50, and 80 g, respectively, and (2) a 16-hour hypoglycemia-induced scenario where an overestimated manual bolus is provided for a single meal at 6 hours with 70 g of carbohydrates. For both scenarios, intra-day variability in insulin and dawn phenomenon is included, and hypoglycemia treatments of 15 g of fast-absorbing carbohydrates are provided every 20 minutes until glucose is above 60 mg/dL.
The primary outcome is the number of rebound hypoglycemia episodes caused by insulin delivery in the next 30 minutes of the first hypoglycemia event. A rebound hypoglycemia event was defined if BG <70 mg/dL within a two-hour window from a previous hypoglycemia event. In addition, basal and bolus commands within 30 minutes after a hypoglycemia event are reported. Overall glucose outcome metrics are also analyzed: mean BG, coefficient of variation (CV), and percentage of time spent between 70 and 180 mg/dL (time in range, TIR), above 180 mg/dL (time above range, TAR), and below 70 mg/dL (time below range, TBR), along the percentage of time in below 54 mg/dL, in a tight range of 70 to 140 mg/dL, and above 250 mg/dL.
Results
Figure 3 shows the evolution of glycemia, basal, and bolus of a representative subject under the closed-loop system with (pink) and without (blue) the HypoSafe module in the hypoglycemia-induced scenario. It is observed that around 11:30
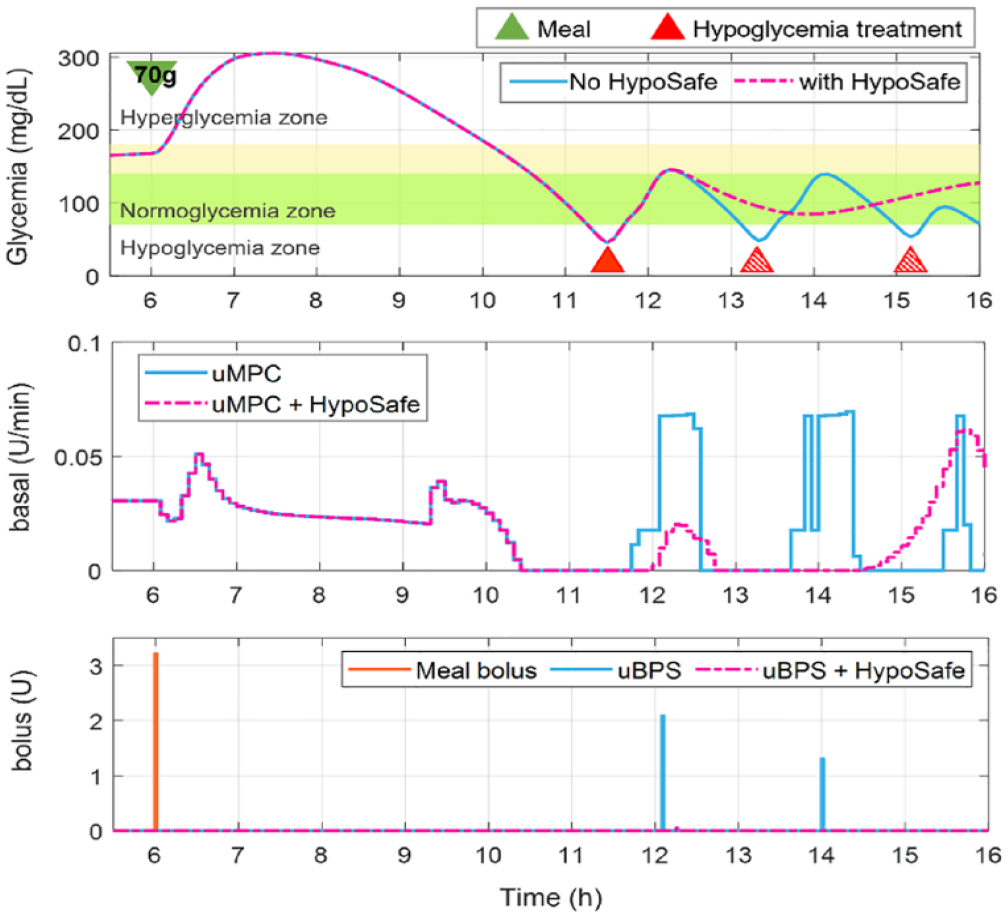
Comparison of glucose, basal and bolus traces in a representative subject during the hypo-induced scenario using the UVA model predictive controller (uMPC) with (pink) and without (blue) HypoSafe. Green triangle represents meal intake, and red solid and red patterned triangles represent rescue carbohydrates after the first hypoglycemia event and after rebound hypoglycemia, respectively.
Population results for both scenarios are reported in Table 1.
Population Outcome Metrics in Nominal and Hypoglycemia-Induced Scenario.
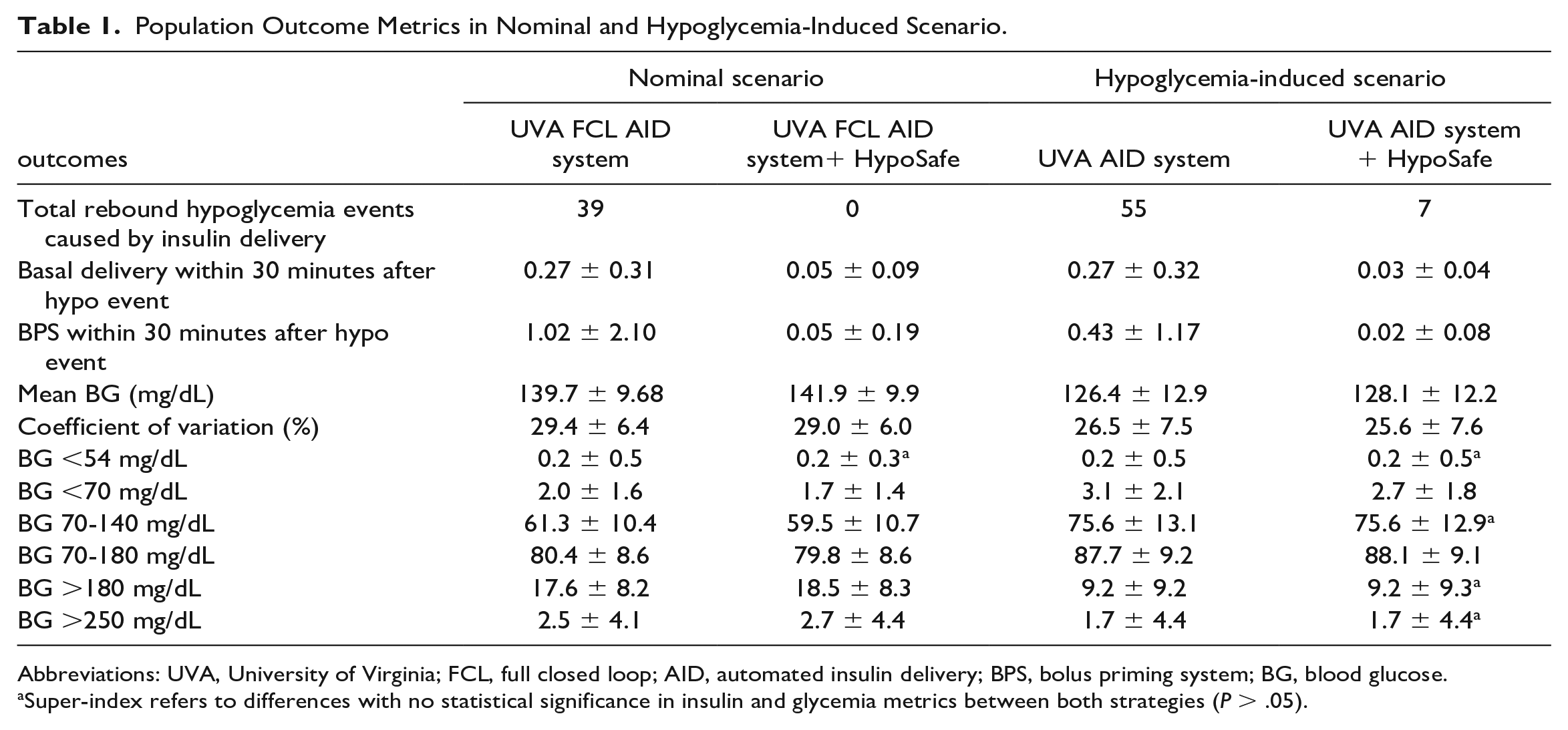
Abbreviations: UVA, University of Virginia; FCL, full closed loop; AID, automated insulin delivery; BPS, bolus priming system; BG, blood glucose.
Super-index refers to differences with no statistical significance in insulin and glycemia metrics between both strategies (P > .05).
In the nominal scenario, the UVA AID strategy led to 39 rebound hypoglycemia events. In contrast, when adding the HypoSafe module, all these events were avoided. In addition, results show no clinically significant differences in TIR (FCL = 80.4 ± 8.6 vs. FCL + HypoSafe = 79.8 ± 8.6), TBR (FCL = 2.0 ± 1.6 vs. FCL + HypoSafe = 1.7 ± 1.4), or TAR (FCL = 17.6 ± 8.2 vs. FCL + HypoSafe = 18.5 ± 8.3).
In the hypoglycemia-induced scenario, rebound hypoglycemia events were reduced from 55 to 7 with HypoSafe. Insulin delivery from basal and bolus doses was significantly reduced within the 30 minutes following a hypoglycemia event. Glucose outcome metrics show no clinically significant differences with and without HypoSafe.
Discussion
There are currently several strategies reported in literature and implemented in commercial devices that aim to alert or suspend insulin infusion for hypoglycemia prevention.6,11,14,26 Typically, these strategies are based on glucose thresholds or short-term glucose predictions. However, once the subject treats a hypoglycemic event and BG levels rise rapidly, there can be an overreaction of insulin leading to rebound hypoglycemia or rollercoaster patterns.22,27
In particular, a recent analysis on rebound hypoglycemia for subjects under multiple daily injections and continuous subcutaneous insulin infusion found 29.4% of hypoglycemic episodes were rebound events. 28 There was also an indication of behavioral overcompensation of carbohydrate intake when hypoglycemic and aggressiveness to correct resulting hyperglycemia. 28
This overreaction to rapid glucose increases has also been observed when using AID systems 22 (see Supplemental Material). Features of the controller depending on glucose value or rate of change may trigger basal or bolus corrections after rescue carbohydrates, potentially leading to rebound hypoglycemia. This phenomenon is more common in FCL-enabled control strategies, which are designed to react more aggressively to positive glucose changes such as meals.
In this study, a HypoSafe module was developed to prevent rebound hypoglycemia caused by the controller overreacting to the effect of rescue carbohydrates. This safety layer is agnostic to the control strategy, ie, it acts as an outer layer that does not depend on the controller’s internal logic, it is simple to integrate, and only uses the last hour of CGM data as input, avoiding the need of requiring hypoglycemia treatment announcement and thus being suitable for FCL strategies.
The integration of this new control layer prevented rebound hypoglycemia events and lessened oscillatory glucose level behaviors in simulated experiments. The oscillatory response that can happen after a controller overcorrection following rescue carbohydrates is explicitly shown in Figure 3. This behavior is avoided by integrating HypoSafe as it restricts basal and bolus commands after the initial hypoglycemia treatment.
In addition, it has been observed that including HypoSafe has no clinically significant effect on glucose outcome metrics. This is advantageous since the module does not compensate for the reduction of hypoglycemia events by lowering TIR or increasing TAR. Hence, the performance achieved with the base controller design is maintained.
This work is limited to in-silico results comparing the performance of an AID system with and without HypoSafe. Conditions for hypoglycemia treatments were standardized for all virtual subjects (15 g every 20 minutes until BG >60 mg/dL), which can artificially reduce TBR for strategies with and without HypoSafe, but in free-living conditions, subject preferences and hypoglycemia awareness may differ from the testing scenario. This layer was integrated into the UVA AID system in a recent clinical trial (clinicaltrials.gov NCT05528770), where rebound hypoglycemia was not observed.
Conclusion
AID systems can increase the risk of rebound hypoglycemia after reacting to rescue carbohydrates. In this work, a HypoSafe module that can be easily integrated into an AID system has been developed to constrain insulin doses. HypoSafe is based on the minimum glucose measurement in the last hour and the current glucose concentration, avoiding the need of manual announcements. The proposed HypoSafe module was shown to be effective in reducing rebound hypoglycemia events without clinically affecting achieved TIR when combined with an advanced FCL system.
Supplemental Material
sj-docx-1-dst-10.1177_19322968231212205 – Supplemental material for Integration of a Safety Module to Prevent Rebound Hypoglycemia in Closed-Loop Artificial Pancreas Systems
Supplemental material, sj-docx-1-dst-10.1177_19322968231212205 for Integration of a Safety Module to Prevent Rebound Hypoglycemia in Closed-Loop Artificial Pancreas Systems by María F. Villa-Tamayo, Patricio Colmegna and Marc D. Breton in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
AID, automated insulin delivery; BG, blood glucose; BPS, bolus priming system; CGM, continuous glucose monitoring; FCL, full closed loop; FDA, Food and Drug Administration; HCL, hybrid closed loop; HMS, hyperglycemia mitigation system; MPC, model predictive control; T1D, type 1 diabetes; TDI, total daily insulin; TIR, time in range; TAR, time above range; TBR, time below range; UVA, University of Virginia.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.F.V.-T., P.C., and M.D.B. receive research support and royalties from Dexcom handled by the University of Virginia’s Licensing and Ventures Group. M.D.B. reports consulting and speaker engagement from Dexcom, Tandem Diabetes Care, Sanofi, Roche, and Portal Insulin LLC.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH grant 5R01DK129553.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.