
Abstract
Optimizing glucose control is of interest also for patients with type 2 diabetes (T2D). While systems for automated insulin delivery are widely used for patients with type 1 diabetes, as documented by many publications, this is not the case with T2D. Because of the number of such patients, this will change drastically in the next years. Manufacturers can transfer many learnings from type 1 to type 2; however, specific clinical aspects have to be considered. This commentary will discuss these aspects and some of the current activities. Future automated insulin delivery (AID) systems will take data from multisensor systems into account to individualize the AID algorithm, supported by artificial intelligence. There is a high need to document the benefits of AID systems in this patient group.
Keywords
Introduction
A literature search using the keywords “closed-loop, diabetes, type 2” yields significantly fewer hits (91, many of which were not appropriate/11 clinical studies/1 review) than when “type 1” is used in the search. Replacing “type 2” with “type 1” yielded almost 2000 hits, of which almost 1000 were in the last five years. Accordingly, there is little commentary on the use of automated insulin delivery (AID) systems in people with type 2 diabetes (T2D) in current consensus publications.1,2 A recent review of previous studies of AID systems in people with T2D was able to include only five randomized clinical trials. 3
The limited available data on the use of AID systems by people with T2D in Germany suggest that this has so far been exceptional (www.dut-report.de). On the contrary, there are many more people with T2D worldwide on insulin therapy than those with type 1 diabetes (T1D). Given the certain “maturity” of AID systems and the level of coverage already achieved in the use of AID systems among people with T1D, the topic addressed here will receive much attention in the coming years. From the manufacturers’ perspective, people with T2D represent an extremely attractive user group (= market). Although it is possible to learn from the experiences of people with T1D, the use of AID systems represents a challenge in its own right. The AID systems cannot be transferred 1:1 from one user group to the other. So, a question is, what are the specific clinical aspects of the usage of AID systems in people with T2D, and to what extent were these addressed in the clinical studies performed thus far? Therefore, the goal of this commentary is to present some current activities and medical aspects that are relevant to the use of AID systems by people with T2D (Table 1). One key question in this context is obviously, what is the percentage of people with T2D that benefit from an insulin therapy, especially from an intensified insulin therapy (more than two injections/day), and which subset may benefit from the usage of an AID system? Because of other therapeutic options of this patient group (see below), this is a discussion that goes beyond the aim of this commentary; however, this is needed, also taking the costs, and so on, associated with the different treatment options into account. Other patient populations may also benefit from using AID systems, for example, those with pancreatectomy or cystic fibrosis. Also, women with T2D during pregnancy might benefit.
Potential Benefits and Barriers to Adoption of AID Systems for People With Type 2 Diabetes.
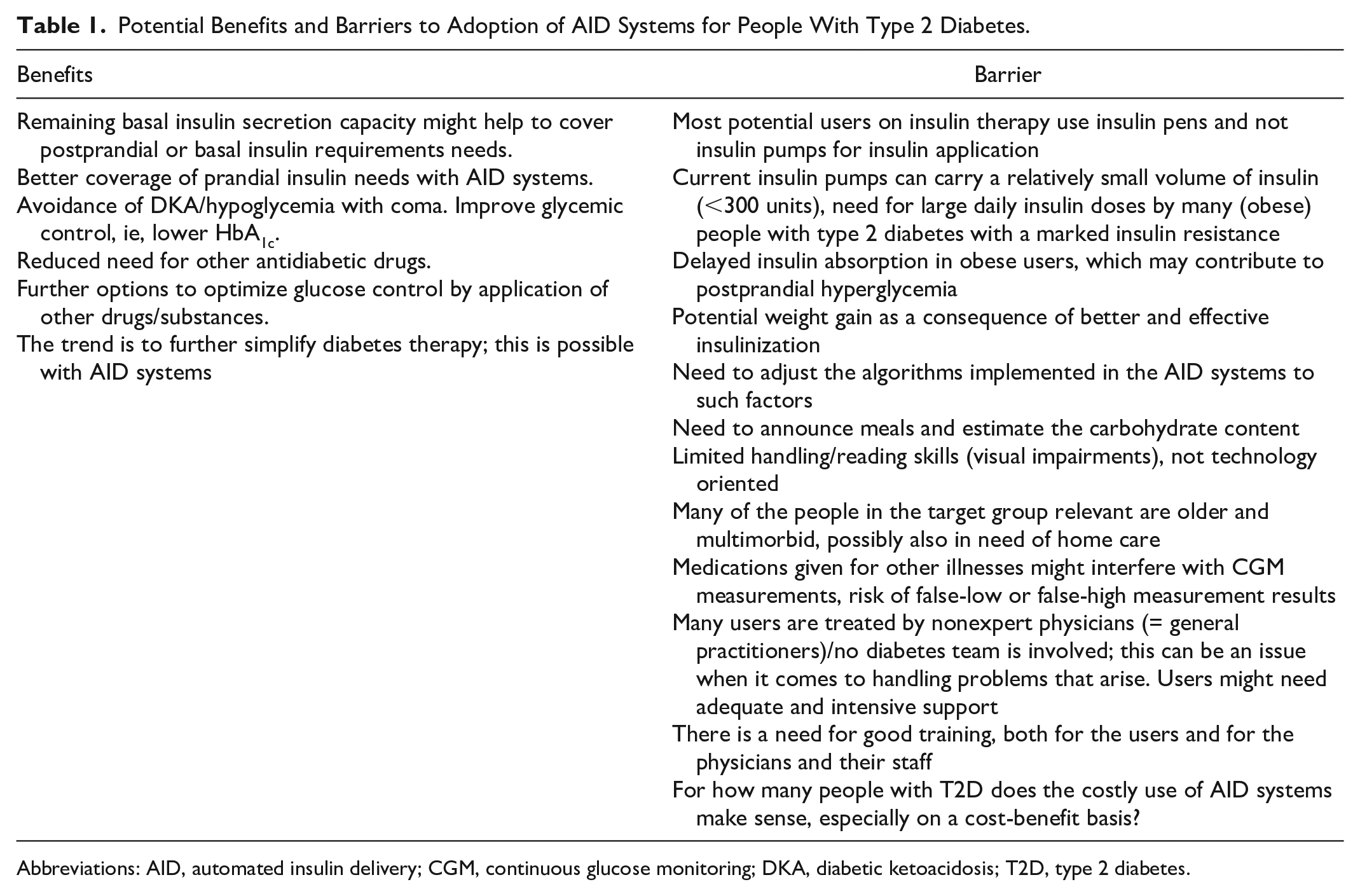
Abbreviations: AID, automated insulin delivery; CGM, continuous glucose monitoring; DKA, diabetic ketoacidosis; T2D, type 2 diabetes.
Current Development and Clinical Studies
Recently, a nonprofit organization (Tidepool; Palo Alto, CA, USA) and an established manufacturer of medical products (Embecta; Wilmington, Delaware, USA) announced their cooperation to develop a patch pump for people with T2D. By using one of the number of the different AID algorithms that Tidepool has developed, this can be converted into an AID system for this user group. The company Tandem (San Diego, CA, USA) has also published study results on this subject. 4 Also, other companies have worked on such developments; however, some have gone out of business.
Nevertheless, most clinical trials in people with T2D to date have been conducted with the Cambridge AID system (CamAPS), but there is also a clinical trial with an Insulet AID system in this user group. 5 Other uses for AID systems in people with T2D include rapid glucose compensation after diabetes diagnosis (short-term use) or in acute situations in the hospital.
CamAPS in Ambulatory Patients With T2D
In a recent publication in Nature Medicine, Daly et al 6 report the results of a clinical trial in people with T2D showing that an AID system is safe and effective in these users. This study involved 26 adult people with T2D on insulin therapy who had poor glucose control (mean baseline HbA1c 9.0%). The study had a crossover design, meaning that participants used the AID system for eight weeks and the prestudy insulin delivery method for eight weeks, with the order determined by randomization. Thus, each participant serves as his or her control, minimizing the possibility of confounding factors affecting the study results.
The improvement in glucose control achieved with the AID system was substantial, that is, the time in the target range (70-180 mg/dL) measured with a continuous glucose monitoring (CGM) system blinded to the control period was 66% using the AID system compared with 32% in the control phase, a difference equivalent to a reduction in time >180 mg/dL of 8.4 hours per day. This reduction in hyperglycemia resulted in a decrease in HbA1c from 9.1% at baseline to 7.2% at the end of the first phase. Few hypoglycemic episodes occurred at baseline (which is not unexpected in such a population), so the ability of the AID system to reduce hypoglycemic episodes cannot be assessed.
The magnitude of improvement in time-in-range is greater than what has been observed in studies of AID systems in people with T1D, with improvements in the range of 9% to 14% compared with controls. 7 This difference may be attributed to a poorer baseline (the poorer the baseline control, the more room for improvement) and to the fact that participants did not use rtCGM as part of diabetes management during the control period. However, even after accounting for a CGM effect, the contribution of the AID system to the results of this study would still be substantial.
The fully closed-loop AID system used in this study does not require meal announcement or carbohydrate content input, making the results of the study all the more impressive. However, there was still an average of eight hours of hyperglycemia per day. It is interesting to note that the variability in insulin requirements among participants in this study was at least as high as that observed in studies of people with T1D.
In this study, there was probably no close monitoring of body weight (there is no mention of this in the publication). An increase in body weight due to increased insulinization is a significant problem in this user group, not only is this highly undesirable from the user’s point of view but it is also associated with a further increase in insulin resistance.
Treating People With T2D in the Inpatient Setting With CamAPS
Cambridge colleagues have evaluated the use of their AID system in the inpatient setting in a whole series of well-designed and executed studies. Using the fully closed-loop version of this, it was shown to be safe and effective even in people with difficult glucose control.8-10 Interestingly, the variability in insulin requirements between and among the people studied is not less than that in people with T1D.
In a group of hospitalized people with T2D, the influence of different foods on the postprandial glucose response was evaluated when the AID system did not receive information about the meal. 11 Reducing the number of carbohydrates relative to fat or protein results in better glucose control under these conditions.
Dialysis and CamAPS
The use of this AID system in outpatients with T2D with end-stage renal failure requiring dialysis results in improved glucose control and prevention of hypoglycemia.12,13 This randomized controlled trial enrolled 26 adults who lived under home conditions during two 20-day intervention periods and were randomly selected. The study compared a fully closed-loop AID system with standard insulin therapy. On average, users were in the glucose target range for more than 3.5 additional hours per day and spent less time in the hypoglycemic range when using the AID system. CamAPS has been used in even more studies in patients requiring dialysis. 14
Pan-European CLOSE Initiative
The availability of easy-to-use and safe AID systems can provide significant relief for people with T2D, their family caregivers, and outpatient providers. This is especially true for the care of older people with advanced T2D and comorbidities who rely on home health care. It is interesting to see how little information is available on this use case, that is, there are no robust figures on how large this user group is and what costs this form of care generates. Inquiries with health insurance companies indicate that this group of people—which has received rather little attention to date—is considerably large. The provision of care is associated with considerable costs and often leads to unsatisfactory clinical results in individual cases. In this user group, AID systems might prevent extreme, often unrecognized, lapses in glucose control, especially hypoglycemia. A frequently observed downward spiral of frailty and loss of health to the point of independence and multimorbidity could thus be slowed down. It could also reduce or even avoid hospitalizations, one of the strongest cost drivers in people with T2D.
Against this background, and supported by a European funding program (EIT Health), the pan-European CLOSE initiative (a consortium of different companies and academic groups) has been working for several years to develop a portfolio of AID solutions for people with T2D that reflects their diversity in terms of comorbidities, frailty, mobility, and living environment. CLOSE stands for “Automated Glucose Control at Home for People with Chronic Disease.” This initiative was launched by the French homecare service provider Air Liquide Healthcare and the German Profil Institute for Metabolic Research. The focus was on the development of an AID system for a specific user group, that is, effective, safe, and cost-efficient care for people with T2D receiving home care. 15 In France, health insurance–funded use of diabetes technology in people with T2D is already relatively widely established. French homecare providers have fully integrated care platforms that facilitate the establishment of AID development partnerships at the interface between people, health care professionals, prescribers, and insurers, which should, in particular, reduce the burden on caregivers.
The CLOSE project takes a holistic approach to development that addresses stakeholder management, and thus issues such as evidence generation, training needs, reimbursement, and business models, in addition to technology adaptation from the outset. Accordingly, the CLOSE consortium integrates competencies in medical technology, clinical trials, regulatory affairs, diabetes care, and health economics.
For technology design, CLOSE is taking a top-down approach that includes design-to-cost analysis. The impact of AID design options on manufacturing and maintenance costs, time-to-market, further development potential, and user satisfaction is consistently examined. Furthermore, much attention has been paid to the aspects of training and education (train-the-trainer) from the outset. By using appropriate performance indicators, an attempt was made to identify those users who benefit most from the use of an AID system. Therefore, the outcome parameters evaluated were not only the impact of the use of the AID system on medical parameters, but also the quality and effectiveness of this type of care in a broader sense.
The aim of a current clinical trial (the CLOSE AP+ trial) is to clinically evaluate the first AID system for “homecare”-requiring people with T2D with a minimum of two daily insulin injections in a randomized, controlled, real-world trial conducted at ten centers in France (ClinicalTrials.gov, NCT04233229). The algorithm used in the study (Control IQ) has so far only been approved in Europe for use in people with T1D and not for use in people with T2D.
In the course of a postfunding evaluation of the CLOSE project, the Fraunhofer Institute for International Management and Knowledge Economics (IMW) modeled that the use of AID systems could save up to €3.9 billion (Europe) and €640 million (Germany) in hospitalization costs annually for the group of people with microvascular and macrovascular complications alone. 16
In the medium term, this French-influenced paradigm is to be further developed into a so-called “AP+ portfolio” that meets the diversity of people with T2D and the requirements for value-based health care in different geographic regions. The bottom line is that this should drive the transition to connected health and social care.
Further Technical Development
The AID systems available to date represent transitional technologies toward fully integrated multisensor systems. 2 The vision is to make a multitude of data collected in everyday life, supported by artificial intelligence, usable for personalized control of (drug) therapies. Given challenging regulatory requirements in Europe for market approval of medical devices, while life and development cycles are shortening, pan-European curated initiatives such as CLOSE can develop the agility needed to make the latest therapeutic options rapidly available to people with chronic diseases and the teams that care for them, in an evidence-based manner, through the collaborative meshing of key competencies.
The targeted development of AID systems for the user group of interest here requires that the technical components be “simple” to use; indeed, such simplicity was a key reason for the market success of a particular CGM system (Abbott’s Libre). 17 In this sense, an AID system (Omnipod 5, see above) will meet the interest of many people with T2D, which is about to be launched in Germany. The patch pump used here is comparatively discreet and easy to use, and no insulin infusion catheter needs to be placed.
There are several approaches to further individualization of AID systems through the use of artificial intelligence; adapting the algorithms to the lifestyle of the individual user will almost certainly lead to further improvements in glucose control. 17 Especially in obese people with T2D, the use of other routes for insulin application may be of interest, for example, a faster onset of insulin action is achieved with inhaled insulin than with subcutaneous application, which contributes to better postprandial glucose control, with basal insulin coverage provided by an insulin pump. 17
Current Developments in the Antidiabetic Drug Therapy of People With T2D
Parallel to the pronounced technological developments, there have been massive changes in recent years in the available antidiabetic therapy of people with T2D, which in total led to a significant decrease in the need for (early) insulin therapy in many such people. The remarkable clinical success with the use of GLP-1 drugs (= reduction of body weight, improvement in glucose control without acute derailments) comes first and that of SGLT-2 inhibitors second. The upcoming launch of distinctly long-acting insulins (with once-weekly or even monthly applications) will probably reduce the need for AID systems, but there is still a considerable group of people who can benefit from such systems. This will also depend on cost aspects.
Costs Due to the Use of AID Systems by People With T2D
The sharp increase in the use of CGM systems in recent years already places a significant burden on health insurers (and thus our health care systems). So what does it mean if increasing numbers of people with T2D are using AID systems? Even if the cost of AID system components and consumables per user decreases with increased production volume and more competition among AID systems, in the aggregate, this change in diabetes therapy will be a cost burden.
It will take clear evidence of the benefits of the AID system used by this user group for payers to go along with this. Manufacturers will point to cost savings from a reduction in treatment costs of secondary diseases with improved glucose control. Different economic models are used in such calculations. Also due to the rather few clinical studies (= lack of evidence) so far, it is not yet possible to make any statements on the cost/benefit ratio when using AID systems in people with T2D. However, this is an important aspect of the CLOSE project (see above). Disparities are an important topic when it comes to the usage of diabetes technology in different groups of people with T1D; however, this also holds true for those with T2D. The relevance of this topic can differ considerably between countries/health care systems.
The call for larger and longer studies with different AID systems in this target group is trivial, but these are needed to assess the benefits (especially from a cost perspective) of this innovative therapeutic approach in a wide range of different user groups; indeed, especially in T2D, the assumption today is that there are clinically quite different subtypes. 3 Since people with T2D are often not treated by specialists, it is important to evaluate this technology in a setting where AID systems have not been used so far.
Start of Insulin Therapy
Many people with T2D are reluctant to start insulin therapy, which is seen as a “last resort” and associated with risks (Table 1). This leads to the fact that the treating physicians probably start insulin therapy too late, even if it would be indicated (“clinical inertia”). The availability of easy-to-use AID systems, as well as the therapeutic environment (general practitioners), can facilitate the early initiation of insulin therapy. Several factors predict which people with T2D will be started on an insulin pump at the current time and they are associated with more careful diabetes management. These include the use of a CGM system, a history of severe metabolic decompensation (eg, diabetic ketoacidosis (DKA), hypoglycemia with coma), high HbA1c, and the use of fewer classes of other diabetes medications.
Summary
In people with T2D who require insulin therapy, the use of an AID system supports the optimization of glucose control according to the clinical study results available to date. The constant adjustment of the insulin dosing to the current insulin requirement by the AID algorithm also prevents acute glucose derailments to a large extent. An AID ecosystem can enable cost-effective improvement in the care of many people with T2D.
Footnotes
Acknowledgements
I thank Prof David Klonoff, Prof Dr Freimut Schliess, Dr Andreas Thomas, Prof Dr Susanne Reger-Tan, and Dr Jens Kröger for their helpful comments.
Abbreviations
AID, automated insulin delivery; BG, blood glucose; CamAPS, Cambridge AID system; CGM, continuous glucose monitoring; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LH is a consultant for several companies that are developing novel diagnostic and therapeutic options for diabetes treatment. He is a shareholder of the Profil Institut für Stoffwechselforschung GmbH, Neuss, Germany.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.