
Abstract
Background:
There is limited evidence that the diabetes in-person consult in hospitalized patients can be replaced by a virtual consult. During COVID-19 pandemic, the diabetes in-person consult service at the University of Miami and Miami Veterans Affairs Healthcare System transitioned to a virtual model. The aim of this study was to assess the impact of telemedicine on glycemic control after this transition.
Methods:
We retrospectively analyzed glucose metrics from in-person consults (In-person) during January 16 to March 14, 2020 and virtual consults during March 15 to May 14, 2020. Data from virtual consults were analyzed by separating patients infected with COVID-19, who were seen only virtually (Virtual-COVID-19-Pos), and patients who were not infected (Virtual-COVID-19-Neg), or by combining the two groups (Virtual-All).
Results:
Patient-day–weighted blood glucose was not significantly different between In-person, Virtual-All, and Virtual-COVID-19-Neg, but Virtual-COVID-19-Pos had significantly higher mean ± SD blood glucose (mg/dL) compared with others (206.7 ± 49.6 In-person, 214.6 ± 56.2 Virtual-All, 206.5 ± 57.2 Virtual-COVID-19-Neg, 229.7 ± 51.6 Virtual-COVID-19-Pos; P = .015). A significantly less percentage of patients in this group also achieved a mean ± SD glucose target of 140 to 180 mg/dL (23.8 ± 22.5 In-person, 21.5 ± 20.5 Virtual-All, 25.3 ± 20.8 Virtual-COVID-19-Neg, and 14.4±18.1 Virtual-COVID-19-Pos, P = .024), but there was no significant difference between In-person, Virtual-All, and Virtual-COVID-19-Neg. The occurrence of hypoglycemia was not significantly different among groups.
Conclusions:
In-person and virtual consults delivered by a diabetes team at an academic institution were not associated with significant differences in glycemic control. These real-world data suggest that telemedicine could be used for in-patient diabetes management, although additional studies are needed to better assess clinical outcomes and safety.
Introduction
Telemedicine, intended as the remote delivery of health care services without the need for a “face-to-face” encounter using information and communication technologies, has been increasingly utilized with the starting of the COVID-19 pandemic.1-3 In the United States, a large study of 40.7 million commercially insured adults suggests that the use of telemedicine for the management of chronic conditions is comparable with in-person visits when the measured outcome is the need for a follow-up visit 14 days after the initial encounter. 4 Among chronic conditions, the use of telemedicine for the management of glycemic control in patients with diabetes in the outpatient settings seems to be at least as effective as in-person encounters, both in patients with type 2 diabetes and with type 1 diabetes.5-7 In hospitalized patients, strategies to remotely identify patients requiring specialized diabetes management have been used and shown to improve glycemic control.8,9 These strategies rely on a virtual management service where the diabetes team remotely reviews the electronic health record (EHR), identifies patients with inadequate glycemic control and then provides recommendations to the clinical team.8,9 However, there is limited evidence that a diabetes in-person consult, which is generally requested for selected more complex cases, can be replaced by a virtual service. 10 Here, we report our experience during the COVID-19 pandemic when our diabetes consult service transitioned from in-person to virtual care.
Methods
The Division of Endocrinology, Diabetes, and Metabolism at the University of Miami offers a diabetes consult service for glucose management in hospitalized patients. This is delivered by a diabetes team which includes an attending endocrinologist, an endocrinology fellow and every so often an internal medicine resident, a medical student, or an international observer rotating with the team. The service covers the University of Miami Hospital and the Jackson Memorial Hospital. In addition, the endocrinology fellow provides a consult service for the nearby Miami Veterans Affairs (VA) Healthcare System under the supervision of an endocrinologist staff physician. The diabetes team receives requests for consults from the primary teams based on their clinical judgment, for example for uncontrolled type 2 diabetes, through the EHR system or by the primary team directly contacting the endocrinology fellow on call who is equipped with a cellular smartphone. The consult can also be generated by a primary team member directly with an EHR alert when one of the following criteria is met: blood glucose >300 mg/dl or <70 mg/dL in two occasions, diagnosis of type 1 diabetes and use of an insulin pump device. The EHR system used varies by site and includes EPIC (University of Miami Hospital), Cerner (Jackson Memorial Hospital), and CPRS (Computerized Patient Record System, VA). The diabetes consult service is traditionally based on a face-to-face model where patients are physically seen by the team and then a note with clinical recommendations is entered in the EHR system. With the starting of the COVID-19 pandemic and then increasing concerns about health care providers’ exposure to the viral infection some consult services, including the diabetes service, transitioned to a virtual care model on March 15, 2020. After receiving a consult request, the endocrinology fellow on call contacted patients either on their personal phone or on the phone located in their hospital room. If the patient could not be reached by phone, a family member was contacted. In the case that neither the patient nor the families could be reached, the relevant medical history was gathered by the bedside nurse and/or the primary team. Blood glucose data, from capillary blood glucose measurements and laboratory tests, were reviewed daily. After the cases were discussed, clinical recommendations were entered in the EHR system. Before being discharged from the hospital patients were also provided with recommendations for diabetes management. For the data analysis, we included patients who were evaluated in-person (In-person) from January 16, 2020 to March 14, 2020 (60 days) and virtually from March 15, 2020 to May 14, 2020 (60 days). In addition, since all patients infected with COVID-19 were seen only virtually and COVID-19 infection can worsen glycemic control, data were analyzed by separating the virtual group in patients who were infected with COVID-19 (Virtual-COVID-19-Pos), and patients who were not (Virtual-COVID-19-Neg) or by combining the two groups (Virtual-All). Patients’ demographics were manually extracted by chart review from the three different EHR systems used as well as by reviewing the endocrinology fellows sign out notes. Glucose data were extracted from Epic and Cerner with the assistance of the Department of Information Technology of the University of Miami and Jackson Memorial System, respectively, and manually from CPRS in the case of VA patients.
Glucose Metrics
Patient-day was defined as a calendar day during which at least one blood glucose determination was associated with a unique patient.11,12 The average of all glucose readings taken for a single patient on a single day in the hospital was calculated and determined the mean glucose for each patient-day. Glycemic exposure was based on day-weighted methodology and calculated as the sum of the means for each patient-day, divided by the number of monitored patient-days. 12 Glucose targets range of 140 mg/dl to 180 mg/dl and 100 mg/dl to 180 mg/dL were chosen based on the recommendations of the American Diabetes Association for hospitalized patients with diabetes. 13 For each patient, the percentage of patient-days in any given range was calculated based on the count of patient-day values in that range divided by number of days of hospitalization. The occurrence of hyperglycemia and severe hyperglycemia were defined as a patient-day with at least a blood glucose ≥180 mg/dl or >299 mg/dL, respectively. 12 Similarly, the occurrence of hypoglycemia or clinically significant hypoglycemia was defined as a patient-day with at least a blood glucose <70 mg/dl or <54 mg/dL, respectively. 13 The occurrence of severe hypoglycemia using a blood glucose value <40 mg/dL recently proposed was also investigated. 14 For each patient, the percentage of hyperglycemic and hypoglycemic events was calculated based on the count divided by the number of days of hospitalization. To summarize data within each group of patients (In-Person, Virtual-COVID-19-Neg, and Virtual-COVID-19-Pos), the percentages for all patients were averaged.
Statistical Analysis
The distribution of continuous data was tested using Shapiro-Wilk’s normality test. Given the non-normal distribution of numerical glucose metrics, the Mann-Whitney U test or Kruskal-Wallis test were used to compare differences among groups. The post-hoc Dunn’s test was subsequently performed to test the pairwise comparison between each pair and the P value adjusted by Bonferroni correction. The odds ratios (ORs) with corresponding 95% confidence interval (CI) were estimated using the generalized estimating equation. The correlation between categorical variables was explored using the chi-square test or Fisher’s exact test, as appropriate. Data are presented as mean ± SD. All statistical analyses were performed using RStudio statistical software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
We extracted data from 294 patients, 180 evaluated in-person and 114 evaluated virtually (Table 1). Most patients (> 80%) were either White Hispanic or Black, but there were no significant differences among groups. There were also no significant differences among groups for age, sex, diabetes control, type of hospital service, and length of stay. Only 15% of patients infected with COVID-19 were in a critical care unit. As expected, most patients had type 2 diabetes. From this population, we collected 9766 blood glucose measurements that resulted in 2289 patient-days (Table 2). In general, patients had 4.3 ± 1.6 blood glucose results per patient-day. Patients seen virtually had more frequent glucose testing compared with those seen in-person, but there were no significant differences when comparing In-Person, Virtual-COVID-19-Neg, and Virtual-COVID-19-Pos (4.2 ± 1.5 In-person compared with 4.4 ± 1.8 Virtual-All, P = .026; 4.4 ± 1.9 and 4.4 ± 1.6 for Virtual-COVID-19-Neg and Virtual-COVID-19-Pos, respectively). Only 3% of patient-days had one blood glucose result.
Demographics and Clinical Characteristics of the Patients.
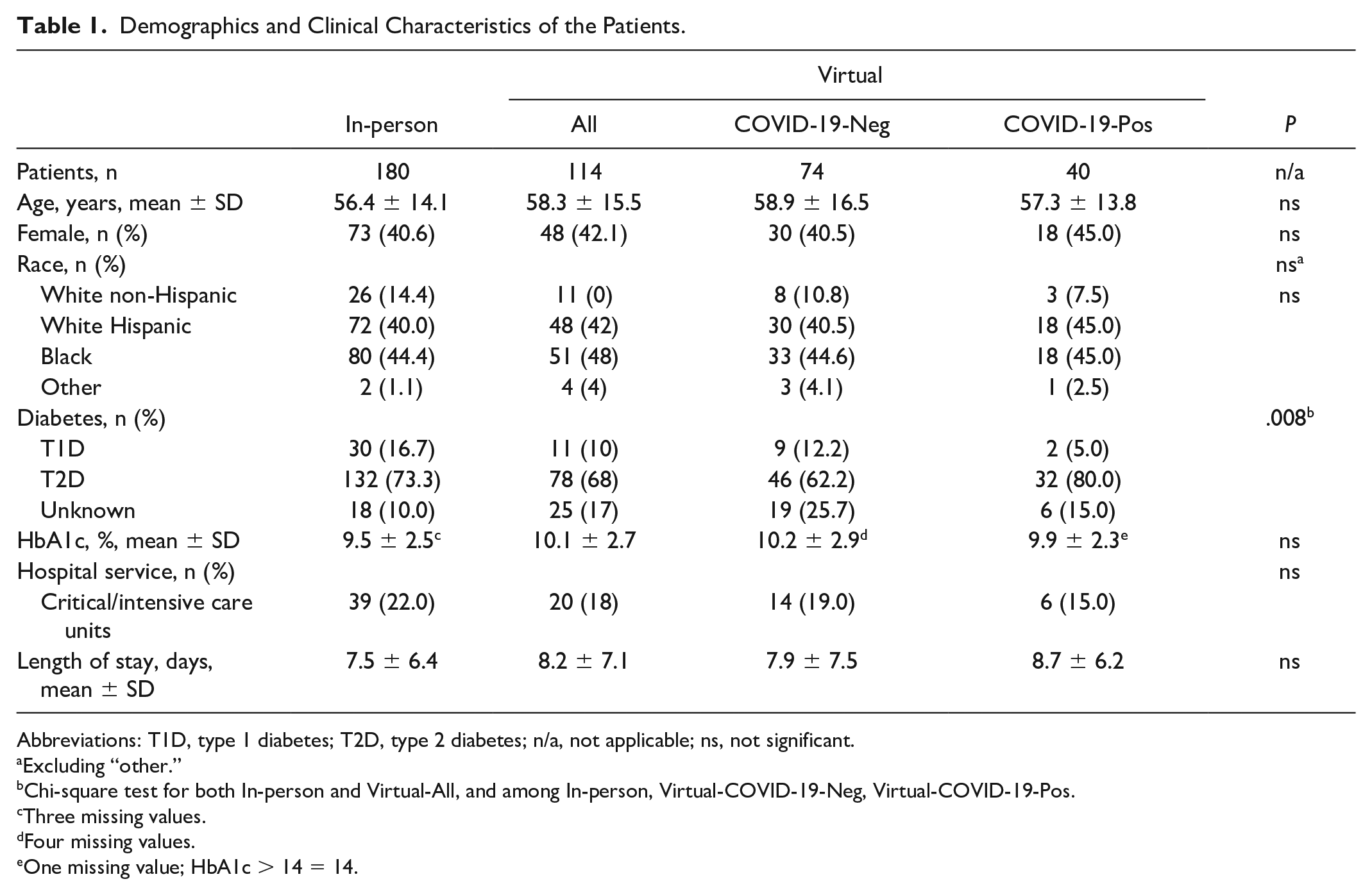
Abbreviations: T1D, type 1 diabetes; T2D, type 2 diabetes; n/a, not applicable; ns, not significant.
Excluding “other.”
Chi-square test for both In-person and Virtual-All, and among In-person, Virtual-COVID-19-Neg, Virtual-COVID-19-Pos.
Three missing values.
Four missing values.
One missing value; HbA1c > 14 = 14.
Comparison of Glucose Metrics in Different Groups.
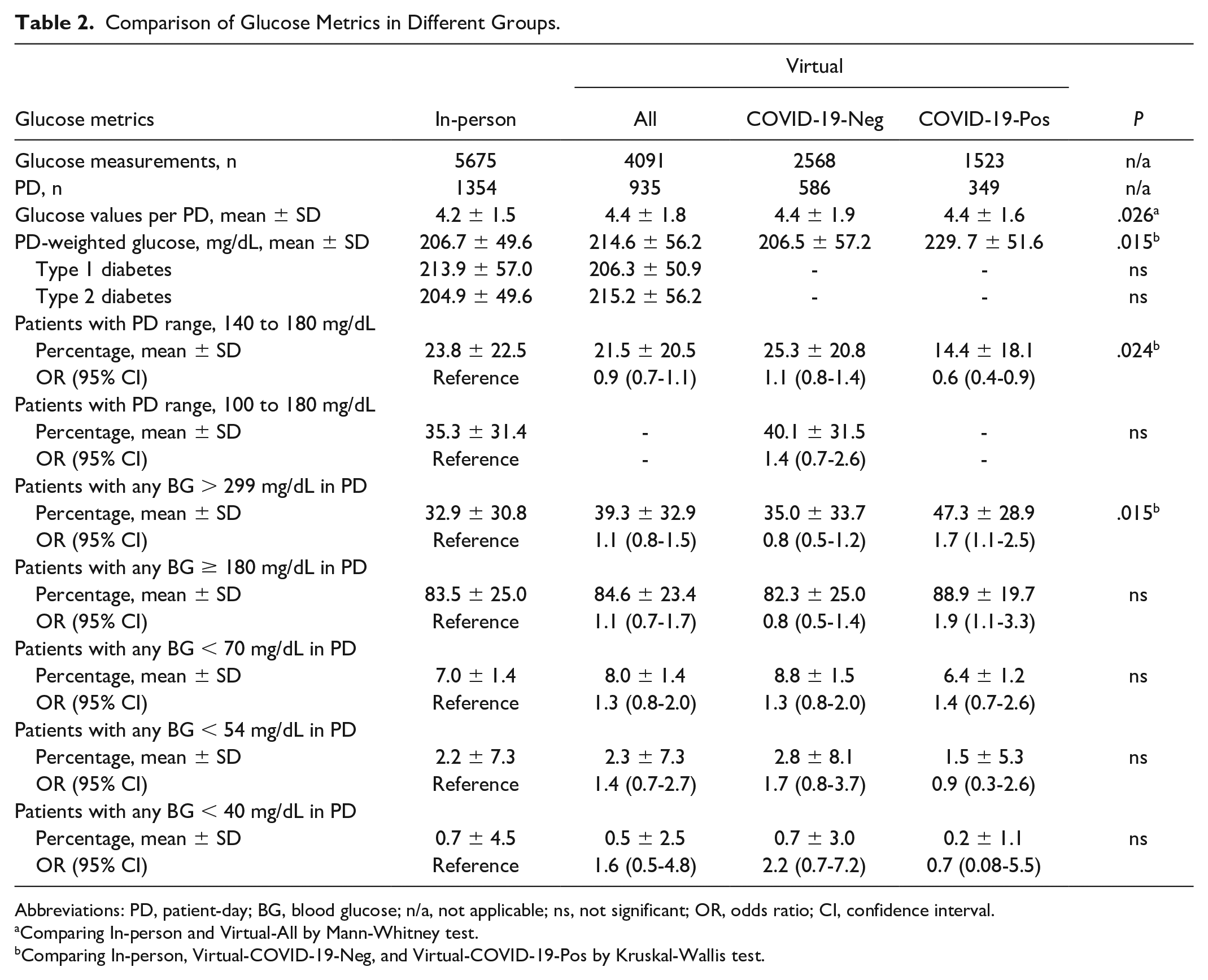
Abbreviations: PD, patient-day; BG, blood glucose; n/a, not applicable; ns, not significant; OR, odds ratio; CI, confidence interval.
Comparing In-person and Virtual-All by Mann-Whitney test.
Comparing In-person, Virtual-COVID-19-Neg, and Virtual-COVID-19-Pos by Kruskal-Wallis test.
Glycemic control measured as patient-day–weighted mean glucose showed no differences between the In-person and Virtual-All, and no differences when comparing In-Person and Virtual-COVID-19-Neg; however, compared to In-person and Virtual-COVID-19-Neg, Virtual-COVID-19-Pos presented worse glycemic control (206.7 ± 49.6, 206.5 ± 57.2, 229.7 ± 51.6 mg/dl, respectively, P = .015) (Table 2, Figure 1a). Virtual-COVID-19-Pos was also significantly more likely to receive steroids as part of the COVID-19 treatment protocols compared with In-Person (OR = 7.8, 95% CI = 3.7-16.8), whereas the Virtual-COVID-19-Neg was not. No differences in glycemic control were observed between In-Peron and Virtual-All regardless that patients had type 1 or type 2 diabetes (Table 2). Analyzing the percentage of patients with a glucose target range of 140 mg/dl to 180 mg/dL, which is recommended for most of critically ill and noncritically ill patients 13 also revealed that compared with In-Person and Virtual-COVID-19-Neg, a reduced percentage of Virtual-COVID-19-Pos patients was able to achieve this glucose target (23.8 ± 22.5, 25.3 ± 20.8, and 14.4 ± 18.1 %, respectively, P = .024) (Table 2, Figure 1b). Virtual-COVID-19-Pos patients were also 40% less likely of achieving the glucose target compared with In-person (OR = 0.6, 95% CI = 0.4-0.9) (Table 2). However, despite this difference, a similar proportion of patients was able to achieve the target glucose range when comparing In-Person and Virtual-COVID-19-Neg and In-Person and the two Virtual groups combined. Similarly, using a glucose target range of 100 mg/dl to 180 mg/dL, which has been more recently recommended for noncritically ill patients with “new” hyperglycemia and those with known diabetes prior to admission, 13 resulted in no differences when comparing In-person and Virtual-All.
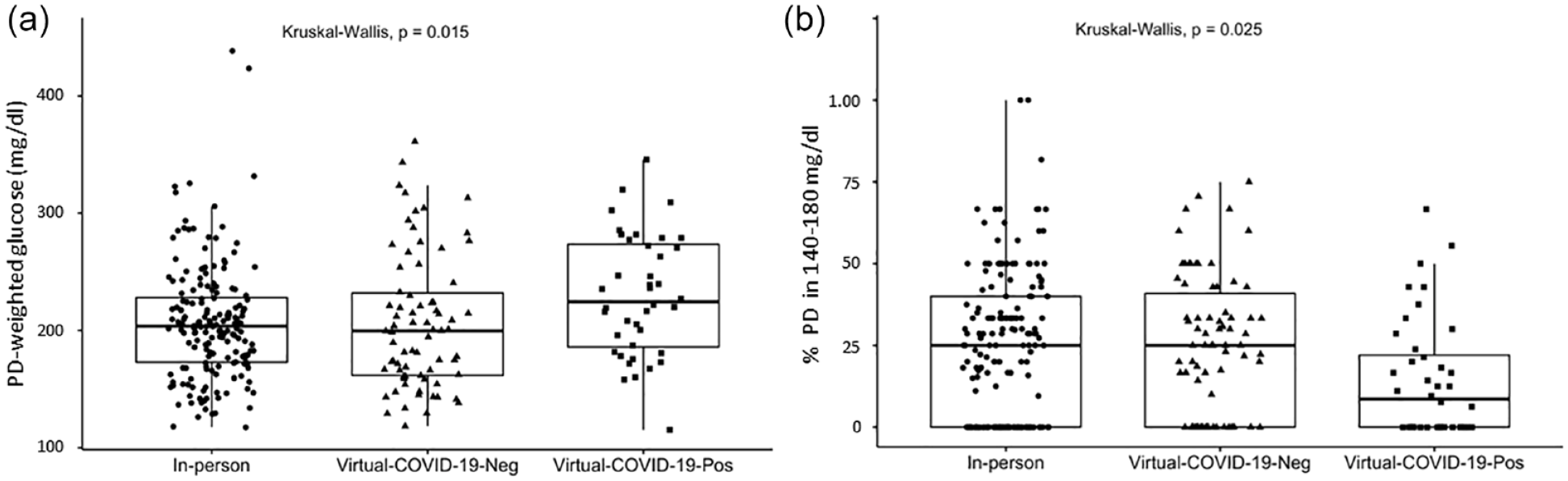
Glycemic control comparison between in-person and virtual consults in hospitalized patients with diabetes. (a) Box-and-whiskers plots representing the PD-weighted glucose for each patient and (b) the percentage of PD with values in the 140 mg/dl to 180 mg/dL range for each patient. In-person (n = 180), Virtual-COVID-19-Neg (n = 74), Virtual-COVID-19-Pos (n = 40). Abbreviations: PD, patient-day.
In this study, we also investigated the percentage of patients who experienced episodes of hyperglycemia and hypoglycemia (Table 2). Compared with the In-Person and Virtual-COVID-19-Neg, a higher percentage of Virtual-COVID-19-Pos patients experienced a patient-day with at least one blood glucose > 299 mg/dL (32.9 ± 30.8, 35.0 ± 33.7 and 47.3 ± 28.9%, respectively, P = .015). This level of hyperglycemia was also more likely to occur in the Virtual-COVID-19-Pos compared with In-person (OR = 1.7, 95% CI = 1.1-2.5). No significant differences were observed between when comparing patient-day with at least one blood glucose ≥ 180 mg/dL, although this level of hyperglycemia was more likely to occur in Virtual-COVID-19-Pos compared with In-person (OR = 1.9, 95% CI = 1.1-3.3). Finally, of the 2289 patient-days we analyzed, less than 10% of patients experienced episodes of hypoglycemia with any blood glucose in a patient-day <70 mg/dL, less than 5% of patients experienced episodes of hypoglycemia with any blood glucose in a patient-day <54 mg/dL, and less than 1% of patients experienced episodes of hypoglycemia with any blood glucose in a patient-day <40 mg/dL. No significant differences were observed when we compared the percentage of patients experiencing hypoglycemia (Table 2). No significant differences were also observed when comparing the occurrence of the single episodes of hypoglycemia in patient-day among groups.
Discussion
Patients with diabetes mellitus are at increased risk of hospitalization and negative outcomes, which includes increased morbidity and mortality. 13 A dedicated in-patient diabetes consult service can reduce the length of stay and readmission rates.15,16 However, the utilization of this type of service is generally limited to selected cases given that up to 30% to 50% of hospitalized patients have diabetes or can experience hyperglycemia during their hospital stay. The use of telemedicine by a diabetes team can partially overcome the limited available resources by providing care for many patients without the needs of in-person encounters. In the DINGS (Diabetes Inpatient Glycemic Survey), the implementation of a process for the remote of care of all hospitalized patients with glucose values < 70 mg/dl or > 350 mg/dL by a team of diabetes specialists resulted in improved glycemic quality metrics. 8 A different study, but with a comparable approach for hospitalized patients with glucose values ≥ 225 mg/dl and/or < 70 mg/dL also resulted in a similar outcome. 9 A complementary approach is to explore the impact of virtual care by a diabetes team when the virtual consults are compared with the traditional in-persons consults and not to the management by the clinical teams, which was the aim the present study. Few months after the starting of the pandemic, a small study supported by limited data analysis but of sure interest at the time of publication suggested that virtual and in-persons consults by a diabetes team results in comparable glycemic control. 17 Our study supports and expands these initial findings. We show that the implementation of virtual consults results in similar glycemic control compared with in-person consults and also show that the glycemic control is worse in COVID-19-infected patients receiving virtual care compared with the other groups. If this a consequence of COVID-19 infection, which can cause hyperglycemia 18 or the result of COVID-19 treatment protocols requiring administration of high-dose steroids was not fully explored in this study, but patients infected with COVID-19 were more likely to receive steroids compared with the other groups. Our study also investigated the glycemic control in patients with type 1 diabetes or type 2 diabetes, which was not done in the other studies. The management of patients with type 1 diabetes in the hospital presents specific challenges that include starting a proper insulin basal bolus regimen, matching the dose of rapid insulin with carbohydrates, heterogeneous insulin sensitivity, and frequency of blood glucose testing, just to mention a few. Despite these and other challenges, our data show that in-person and virtual consults result in comparable glycemic control both in patients with type 1 and type 2 diabetes. We further analyzed the glycemic control in our population also considering different glycemic targets. Guidelines for the management of diabetes in hospitalized patients suggest a target range of 140 mg/dl to 180 mg/dL for most critically ill and noncritically ill patients. 13 In addition, a target of 100 mg/dl to 180 mg/dL has been recently adopted for noncritically ill patients with recent hyperglycemia onset and patients with known diabetes prior to admission.13,19 We did not observe significant difference among groups for both glycemic targets except for patients infected with COVID-19 who presented higher blood glucose values and were also more likely to have hyperglycemia defined as a patient-day with at least one blood glucose ≥ 180 mg/dl or > 299 mg/dL. It should be noted, however, that less than 50% of the patients that we analyzed had glucose values within the recommended target ranges most likely because of the poor glycemic control at admission. In fact, the mean glycated hemoglobin (HbA1c) at the time of hospitalization was ≥ 9.5% across all groups. Finally, in this study, we investigated the occurrence of hypoglycemia which in hospitalized patients is associated with increased mortality and length of stay.20-22 We did not observe significance differences in the occurrence of clinically significant and severe hypoglycemia in patients seen in-person compared with those seen virtually.
Conclusions
Overall, our data suggest that the transition from in-person to virtual consults was not associated with different glycemic control and therefore we did not find evidence against the use of telemedicine in hospitalized patients with diabetes. We recognize that this study presents several limitations. Data about the use of different insulin regimens, for example the use of a sliding scale or basal bolus regimen, were difficult to extract and therefore could not be used for a more sophisticated analysis. Also, we were unable to consistently verify whether the insulin regimens we recommended were implemented. Data about comorbidities and concomitant therapies were also not collected, although the patient-based data analysis we have conducted may have mitigated this bias. On the other hand, the population we studied was mostly Hispanic and Black, reflecting the demographics of Miami-Dade County, which is generally poorly represented in clinical studies. There are many uncertainties regarding the future of telemedicine due to several barriers, including insurance coverage. We believe that our study provides valuable real-word data suggesting that telemedicine can be used for in-patient diabetes management, although additional studies are needed to better assess clinical outcomes and safety.
Footnotes
Abbreviations
EHR, electronic health record; CPRS, Computerized Patient Record System.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.