
Abstract
Background: Continuous glucose monitor (CGM) use has been linked with better glycemic outcomes (HbA1c), yet many adolescents with type 1 diabetes (T1D) struggle to maintain optimal CGM use. Methods: This study examined CGM use and its association with HbA1c and psychosocial factors among adolescents with T1D experiencing at least moderate diabetes distress (N = 198). We examined mean differences in HbA1c, diabetes distress, diabetes-related family conflict, and quality of life among CGM user groups (Current Users, Past Users, and Never Users). Results: Current Users demonstrated significantly lower HbA1c than Never Users and significantly lower diabetes distress than Past Users. CGM use was not associated with family conflict or quality of life. Conclusions: CGM use was associated with lower HbA1c and diabetes distress but not with other psychosocial outcomes. Longitudinal data may explain why many adolescents do not experience improvements in quality of life with CGM use.
Keywords
Introduction
Adolescence is a particularly challenging time to balance the high demands of type 1 diabetes (T1D) management, and adolescents are at risk for suboptimal glycemic outcomes and lower health-related quality of life (HRQOL).1,2 Diabetes distress, the negative emotional response to the burden of living with diabetes, is prevalent among adolescents with T1D, with estimates of one third of adolescents experiencing elevated diabetes distress. 3 The transition of diabetes management responsibilities from primary caregiver to adolescent may lead to diabetes-specific family conflict. 4 Family conflict, diabetes distress, and HRQOL are each associated with suboptimal glycemic outcomes in adolescents.3-5 Diabetes management and monitoring strategies have the potential to improve glycemic outcomes and lessen the psychosocial burden of T1D management for adolescents; thus, it is important to evaluate these strategies and their association with glycemic control and psychosocial variables.
Continuous glucose monitor (CGM) use has been associated with lower HbA1c and better glycemic outcomes; 6 however, less is known about the psychosocial impacts of CGM use. Continuous glucose monitor use has contributed to improvements in HRQOL in adults, 7 yet this association was not observed in several studies with a normative sample of adolescents.8,9 A review of family perspectives on CGM use reported benefits such as an increased sense of security and higher quality of life, as well as burdens including negative impact on family life through school, work, and financial interference. 10 The burdens of CGM use (e.g., painful insertion, visibility to others, device expenses, insurance coverage) may outweigh the benefits (e.g., ease of T1D management, fewer fingersticks, more security) resulting in infrequent use or discontinuation of CGM, particularly among adolescents; therefore, it is important to understand the psychosocial outcomes associated with this technology.11-13
The current literature related to the psychosocial associations of CGM use is limited, particularly among adolescents experiencing diabetes distress, and findings regarding psychosocial outcomes are mixed. 10 Here, we examine the association of CGM use with HbA1c, diabetes distress, family conflict, and HRQOL among a diverse sample of adolescents experiencing diabetes distress, a particularly vulnerable group at risk for worse psychosocial and glycemic outcomes. 14 We hypothesized that adolescents who were current CGM users would have lower HbA1c, lower diabetes distress, less family conflict, and higher HRQOL than adolescents who were not using CGM.
Methods
Adolescent-caregiver dyads were enrolled in an ongoing multi-site randomized controlled trial examining the efficacy of a positive psychology intervention for adolescents experiencing diabetes distress (clinicaltrials.gov identifier: NCT03845465). 14 Adolescents were eligible if age 13–17 years, ≥1 year since T1D diagnosis, fluent in English, experiencing at least moderate diabetes distress (total score ≥34) using the Problem Areas in Diabetes-Teen (PAID-T) scale 15 and had a text-messaging capable device. Exclusion criteria included other serious health conditions that interfere with diabetes care.
Caregivers reported on their adolescents’ CGM use and demographic information. HbA1c data were extracted from electronic medical records (point-of-care values) and at-home HbA1c kits (for adolescents who had telehealth diabetes visits). Adolescents completed the PAID-T, a validated measure to assess diabetes distress. Problem Areas in Diabetes-Teen scores range from 14 to 84, with scores ≥44 considered clinically significant. Cronbach’s alpha for this sample was 0.95. 15 Diabetes specific-HRQOL was assessed using the Type 1 Diabetes and Life (T1DAL) measure, a validated 23-item measure with scores ranging from 0 to 100 and higher scores indicating better HRQOL. 16 Cronbach’s alpha for this sample was 0.89. Adolescents also completed the Revised Diabetes Family Conflict Scale (RDFCS), a validated 19-item measure used to assess diabetes-related family conflict. 17 RDFCS scores range from 19 to 57 and higher scores reflect higher levels of diabetes-related family conflict. Cronbach’s alpha for this sample was 0.85. 18
The current study was a secondary analysis of baseline data collected between 2019 and 2022. Descriptive statistics were used to summarize demographic, glycemic, and psychosocial characteristics. Continuous glucose monitor use was categorized into 3 user categories: “Current,” “Past,” and “Never” Users. Although the CGM user groups differed in sample size, the Box’s M test was non-significant, indicating that a multivariate analysis of variance (MANOVA) was appropriate for evaluating group diffferences. We were missing HbA1c values from 20 participants, so we conducted an analysis of variance (ANOVA) with the smaller sample to test for differences in HbA1c related to CGM use, and a MANOVA with the full sample to evaluate differences in PAID-T, RDFCS, and T1DAL scores. Finally, we included HbA1c as a covariate in a multivariate analysis of covariance evaluating differences in psychosocial outcomes. All analyses were performed using IBM SPSS Statistics software, v28.
Results
Participants included 198 adolescents who endorsed elevated diabetes distress (see Table 1 for demographic and clinical characteristics). Our sample included 81% Current CGM Users (n = 161) and 19% non-CGM Users (n = 37; (10% Past Users [n = 20] and 9% Never Users (n = 17)). We did not find any significant associations between CGM use and the demographic variables. We observed no significant difference in CGM use versus non-use related to sex: 84% of males and 79% of females were CGM users (χ2 = 0.86, P = .35). We also did not find significant differences in CGM use related to adolescent age (P = .19), duration of diagnosis (P = .21), race (χ2 = 1.61, P = 0.90), or ethnicity (χ2 = 1.33, P = 0.25). Duration of CGM use was correlated with lower HbA1c (r = 0.20, P = .02) but was not significantly associated with any of the psychosocial variables.
Demographic, Diabetes, and Psychosocial Participant Characteristics.
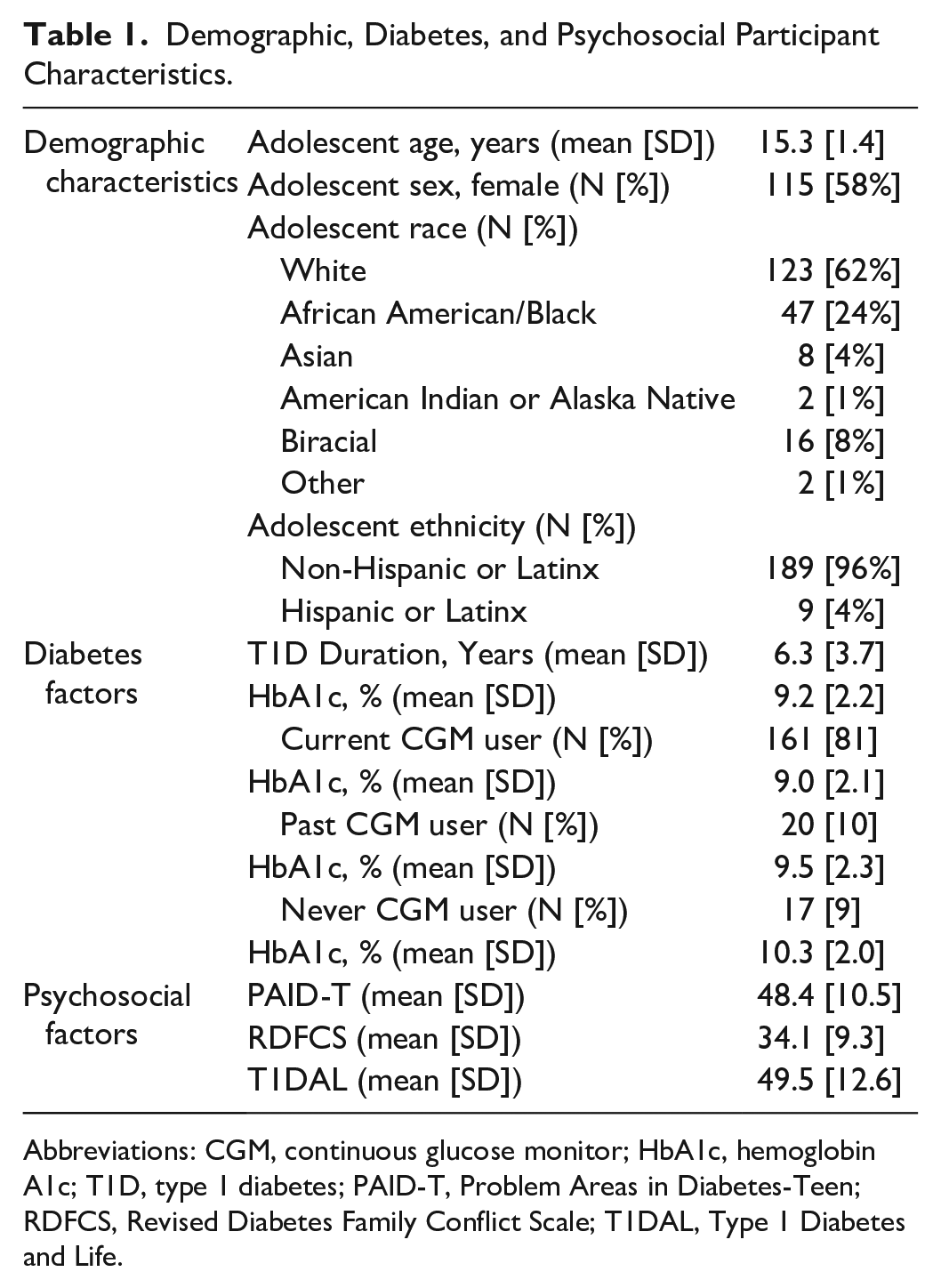
Abbreviations: CGM, continuous glucose monitor; HbA1c, hemoglobin A1c; T1D, type 1 diabetes; PAID-T, Problem Areas in Diabetes-Teen; RDFCS, Revised Diabetes Family Conflict Scale; T1DAL, Type 1 Diabetes and Life.
The ANOVA indicated significant differences in HbA1c between user groups (F = 3.18, P = .04). Post-hoc analyses revealed that HbA1c was significantly lower in Current Users when compared to Never Users (P = .02), but the difference between Current Users and Past Users was not significant (P = .31), and the difference between Past Users and Never Users was not significant (P = .27). All 3 CGM user groups had an average HbA1c above the American Diabetes Association’s recommended pediatric HbA1c target of <7.0%. 2
We also found significant differences in PAID-T scores between user groups (F = 3.26, P = .04). Post-hoc analyses revealed significantly lower distress reported by Current Users than Past Users (P = .04) but no significant difference between Current Users and Never Users (P = 0.10) or between Past Users and Never Users (P = .80). It is possible that some adolescents discontinued CGM use due to diabetes distress. Continuous glucose monitor use was not significantly associated with diabetes-specific family conflict on the RDFCS (F = 1.15, P = .32) or quality of life on the T1DAL (F = 0.65, P = .53). Figure 1 depicts the mean psychosocial scores of each CGM user group. Finally, when we adjusted for HbA1c, we found similar results; there was a significant association between CGM Use and diabetes distress (F = 3.41, P = .04), but not for family conflict or quality of life.
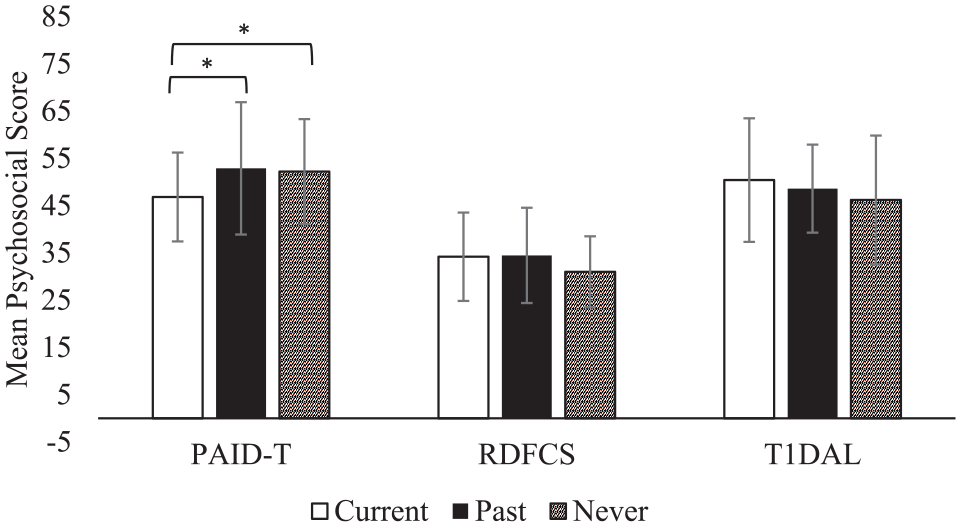
Average score of the PAID-T, RDFCS, and T1DAL (mean ± SD) for each CGM user group. Abbreviations: PAID-T, Problem Areas in Diabetes-Teen; RDFCS, Revised Diabetes Family Conflict Scale; T1DAL, Type 1 Diabetes and Life; CGM, continuous glucose monitor.
Discussion
Although the American Diabetes Association recommends CGM for all adolescents with T1D, 19 little is known about the psychosocial implications of CGM use. The current study contributes to the limited literature related to the psychosocial associations with CGM use and is one of the first studies to examine these associations among adolescents experiencing elevated diabetes distress.8,9,20,21
Consistent with current literature, Current Users demonstrated significantly lower HbA1c levels when compared to adolescents who had never used CGM.6,21 Current Users also endorsed significantly lower diabetes distress when compared to Past Users. These results indicate that CGM use has the potential to improve glycemic outcomes and reduce the burden of diabetes management for adolescents. In contrast to our hypothesis, there was no significant variation in diabetes-related family conflict or quality of life by CGM user groups. While CGM use has been linked with improvements in HRQOL in parents of young children with T1D 11 and adults with T1D, as well as a reduction in conflict with family and friends, 7 the lack of associations found in the current study may be explained by the unique burdens related to CGM use in adolescence. For example, use of CGM may increase the potential for lower HRQOL if adolescents find it painful to insert, feel overwhelmed or discouraged by glucose data, or are embarrassed to wear the device. 22 Additionally, most CGM devices allow caregivers to have constant access to their adolescents’ glucose numbers, which may minimize family conflict related to reminders to check blood glucose levels; 17 however, it may also be perceived as intrusive and increase the potential for family conflict. 23
The current study has many strengths. Research on diabetes technologies has primarily been conducted with non-Hispanic White participants, and the current sample is diverse and largely representative of the clinics from which participants were drawn, offering more generalizable outcomes to the population of adolescents with T1D. Additionally, participants were recruited from 2 large pediatric diabetes clinics, encompassing patient populations from urban and rural areas, resulting in a geographically diverse sample. Despite these strengths, this study is not without limitations. Due to the cross-sectional nature of this study, the direction of effects cannot be determined. Additionally, only English-speaking participants were included, which limits the generalizability of the results. Also, the current study includes a sample of adolescents experiencing elevated diabetes distress which may have limited the variability in this measure. We were unable to determine whether adolescents were using real-time CGM or intermittently scanned CGM, or which generation of device they were using, since these analyses were based on self-report of CGM use. Finally, it is important to note that diabetes technology advances rapidly and the psychosocial measures may not encompass the unique benefits and burdens posed by the current technology.
Conclusions
Among a sample of adolescents experiencing diabetes distress, current CGM use was associated with lower diabetes distress but not HRQOL or family conflict.8,9,20 Current CGM use was also associated with better glycemic outcomes when compared to adolescents who had never used CGM. These findings suggest that although CGM use may benefit glycemic outcomes and reduce some of the burdens of diabetes management, additional support may be needed to improve adolescent psychosocial outcomes. Longitudinal data on specific barriers may explain why many adolescents do not experience improvements in quality of life with CGM use. 12 Behavioral interventions that provide additional psychosocial support to decrease the burdens associated with CGM use may be needed to promote optimal use of CGM and improve quality of life in adolescents with T1D.
Footnotes
Abbreviations
CGM, continuous glucose monitor; HbA1c, hemoglobin A1c; T1D, Type 1 Diabetes; HRQOL, Health-Related Quality of Life; PAID-T, Problem Areas in Diabetes-Teen; T1DAL, Type 1 Diabetes and Life; RDFCS, Revised Diabetes Family Conflict Scale; ANOVA, analysis of variance; MANOVA, multivariate analysis of variance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institutes of Diabetes and Digestive and Kidney Diseases, (R01DK121316).