
Abstract
Background:
The correct injection technique is crucial for people with insulin therapy. However, barriers to insulin injections exist, which can lead to problems with injections. In addition, injection behavior may deviate from recommendations leading to lower adherence to the correct injection technique. We developed two scales to assess barriers and adherence to the correct technique.
Methods:
Two item pools were created to assess barriers to insulin injections (barriers scale) and adherence to the correct technique (adherence scale). In an evaluation study, participants completed the two newly created scales, as well as other questionnaires used for criterion validity. Exploratory factor analysis, correlational analysis, and receiver operating characteristics analysis were computed to analyze the validity of the scales.
Results:
A total of 313 people with type 1 and type 2 diabetes using an insulin pen for insulin injections participated. For the barriers scale, 12 items were selected achieving a reliability of 0.74. The factor analysis revealed three factors namely emotional, cognitive, and behavioral barriers. For the adherence scale, nine items were selected achieving a reliability of 0.78. Both scales showed significant associations with diabetes self-management, diabetes distress, diabetes acceptance, and diabetes empowerment. Receiver operating characteristics analysis showed significant area under the curves for both scales in classifying people with current skin irritations.
Conclusions:
Reliability and validity of the two scales assessing barriers and adherence to insulin injection technique were demonstrated. The two scales can be used in clinical practice to identify persons in need of education in insulin injection technique.
Introduction
People with type 1 diabetes must rely on exogeneous administration of insulin that can be injected multiple times a day in the subcutaneous tissue by themselves. In addition, due to the progressive nature of type 2 diabetes, insulin therapy likely involves increasing diabetes duration, and thus, people with type 2 diabetes may need to inject insulin once or multiple times a day. 1
Higher adherence to insulin therapy is associated with lower hemoglobin A1c (HbA1c) levels and lower rates of hospital admissions2,3 but surveys found that skipping insulin injections was identified in 44% to 57% of people with diabetes.4,5 In addition, for controlling glucose levels with insulin injections, the correct injection technique is crucial to ensure proper insulin action.6,7 With the correct injection technique, people with diabetes ensure that insulin is injected as recommended into the dedicated injection sites. For example, intramuscular injection can lead to a too rapid onset of insulin action, which increases the risk of hypoglycemia. 8 Injecting insulin in areas that are fibrous or poorly vascularized can lead to impaired insulin absorption and blunted action of insulin, leading to glucose fluctuations and impaired glucose control. 9 Furthermore, repeated injection into the same injection site can lead to lipohypertrophy, an enlargement of adipocytes in the subcutaneous tissue, probably due to the lipogenic effects of insulin. 7 A study by Lin et al demonstrated that rotation of injection sites and frequency of needle use were significant predictors of the development of lipohypertrophy. 10 A recent meta-analysis estimated the prevalence of lipohyertrophy at 41.8% 11 ; thus, it can be considered one of the most common cutaneous side effects of insulin therapy. 7 Lipohypertrophy can substantially affect insulin action when insulin is still injected into this altered tissue with unpredictable insulin absorption9,12 leading to higher glycemic fluctuations and higher mean blood glucose levels10,13 and also to unexpected hypoglycemia. 14 Interestingly, Ji et al estimated the excess annual insulin consumption costs due to lipohypertrophy in China at $297 million. 13
To avoid these unintended actions of insulin and cutaneous side effects, several expert groups provided recommendations for the correct injection technique.6,7,15 These recommendations highlight the need for rotating sites of injections to avoid lipohypertrophy, avoiding specific sites of lipohypertrophy, inflammation, infection or edema, and changing the needle after every use.6,7 They also highlight that psychosocial issues around insulin injection such as fear and misconceptions should be addressed. In summary, these recommendations call for effective education and training, as well as re-education of people with diabetes regarding the correct injection technique.6,7
The need for education and training can be seen in findings of the worldwide Injection Technique Questionnaire (ITQ) survey.5,16 Data from 13 225 participants with an average duration of insulin therapy of nine years showed that up to 56% do reuse their needles, with nearly 14% using their needles more than 10 times. Furthermore, 30.8% of participants did have lipohypertrophy, and 44% of those indicated that they still inject into these areas. These results corroborate previous findings that demonstrated the need for injection education.17 -19 Interestingly, studies showed that those with lipohypertrophy needed significantly more insulin, had a higher HbA1c, 16 and had more unexplained hypoglycemia and higher glucose variability. 20 In turn, education and training of the correct insulin technique can lead to optimized injection behavior and better glycemic control.18,21
Reasons that people with diabetes reuse needles include convenience and costs, 5 and reasons for injecting into lipohypertrophic tissue include that it is less painful, is a habit, and is convenient. 16 Peyrot et al additionally show that there is substantial dissatisfaction with injection pain and that 24% of insulin-dependent people with diabetes had a negative affect toward injections stating that they have to mentally prepare themselves before each injection, have some level of dread and embarrassment associated with taking daily injections, and that injections interfered with their lives. 4 Furthermore, these negative attitudes and experiences were associated with more-frequent insulin injection omissions. 4 Taken together, these findings demonstrate that, besides knowledge about the correct injection technique, attitudes and experiences of people with diabetes toward insulin injection play an important role for the adherence and technique regarding insulin injections.
The assessment of such attitudes and experiences is therefore important to identify barriers for insulin injections. Furthermore, such an assessment can identify persons who might benefit from re-education regarding the insulin injection technique and address an individual’s personal issues with insulin injections. We, therefore, developed an assessment tool to systematically assess potential psychosocial and behavioral barriers for insulin injections and conducted a validation study to demonstrate its reliability and validity.
Methods
Development of the Assessment Tool
To comprehensively assess potential barriers for insulin injections, we decided to construct two scales: one scale to assess barriers toward insulin injections (Insulin Injection Technique Barriers [IIT-B]) and one independent scale to assess actual behavior or adherence to the recommendations for a correct injection technique (Insulin Injection Technique Adherence, IIT-A).
For the barriers scale, an initial item pool of 39 items was created. The items were designed as statements for which agreement can be rated on a five-point Likert scale from 0 “not at all” to 4 “completely” (eg, “When I have to inject insulin, I am tense every time”). Development of the adherence scale was based on the recommendations for a correct injection technique6,7 and the ITQ. 22 For the adherence scale, nine items were created reflecting injection behavior in the past two weeks. Items were designed as statements (eg, “For the last 2 weeks, I have changed my pen needle every time I injected insulin”) with the same response options as the barriers scale. All items were discussed with diabetes experts to ensure that all relevant topics were covered.
Design and Setting of the Study
The reliability and validity of both scales were assessed in an evaluation study conducted both as an online survey with participants from the dia·link diabetes panel (www.dialink-diabetes.de) and as a paper-pencil survey with inpatients from the Diabetes Clinic Mergentheim, Germany. Participants had to be at least 18 years of age, have type 1 or type 2 diabetes, and had to use an insulin pen to inject insulin. The evaluation study was approved by the Ethics Committee of the German Psychological Association (2021-08-03VA). All participants provided written informed consent.
To assess the validity of the two scales, the following questionnaires were used as validity criteria:
The Problem Areas in Diabetes (PAID) scale was used to assess diabetes distress. 23 The PAID scale consists of 20 items assessing different aspects of diabetes-specific emotional and regimen-related burdens. A total score was calculated and transformed to a scale from 0 to 100, with higher scores indicating higher diabetes distress.
The Diabetes Self-Management Questionnaire, Revised version, was used to assess different diabetes-specific self-management behaviors. 24 It contains 27 items for which a total score was calculated and transformed to a scale from 0 to 100, with higher scores indicating better diabetes self-management.
The Diabetes Acceptance Scale was used to assess integration of diabetes into daily life. 25 It consists of 10 items for which a total score is derived and transformed to a scale from 0 to 100, with higher scores indicating higher acceptance of diabetes.
The German Diabetes Empowerment Scale was used to assess diabetes-specific empowerment and self-efficacy. 26 It consists of 11 items for which a total score is derived and transformed to a scale from 0 to 100, with higher scores indicating higher empowerment.
The questionnaire for the assessment of diabetes-related problems and satisfaction with insulin treatment was used for the evaluation of diabetes treatment satisfaction. 27 It consists of 10 items for which a total score is calculated and transformed to a scale from 0 to 100, with higher scores indicating higher satisfaction.
In addition, participants indicated whether they currently have and whether they previously had skin irritations at one of their injection sites (eg, swelling, bruising, signs of inflammation, redness). Severity of injection pain was assessed via a 11-point Likert scale from 0 “not at all” to 10 “severe.” Glycemic management was assessed with self-reported HbA1c and, if participants were using a continuous glucose monitoring system, self-reported percentages of glucose values below 3.9 mmol/L (time below range), between 3.9 and 10 mmol/L (time in range), and above 10 mmol/L (time above range).
Statistical Analyses
Item characteristics were calculated as the mean and standard deviation of item responses, as well as item selectivity expressed as the corrected item total correlation. Reliability was assessed using Cronbach’s alpha as a measure of internal consistency. An exploratory factor analysis was conducted using principal component analysis with Varimax rotation. Factors were selected according to the Kaiser criterion (Eigenvalues > 1) and inspection of the Scree plot using the elbow criterion. Correlations with validity criteria were computed as Pearson correlation coefficients. Differences between groups were tested using Student’s t tests with Cohen’s d as the effect size estimate. A receiver operating characteristics (ROC) curve was calculated to test the predictive power of both scales to classify those with current skin irritations. P values lower than .05 were considered significant in all analyses. All analyses were performed with SPSS 28 (IBM Corp., Armonk, NY).
Results
Sample Characteristics
A total of 313 people with diabetes participated in the evaluation study, with 54.3% having type 1 diabetes. Sample characteristics are presented in Table 1. Participants had a rather long diabetes duration with nearly 19 years and had rather optimal glycemic control with an HbA1c value of 7.7%. Approximately one quarter of participants reported that they currently experience injection-related skin irritations at least at one injection site, and almost 42% reported that they have previously experienced injection-related skin irritation at one of their injection sites. The vast majority of participants performed an intensive insulin therapy with multiple daily injections (84.9%), and 12.9% used an incretin in addition to insulin.
Baseline Characteristics of the Total Sample and the Sample Used for Analysis.
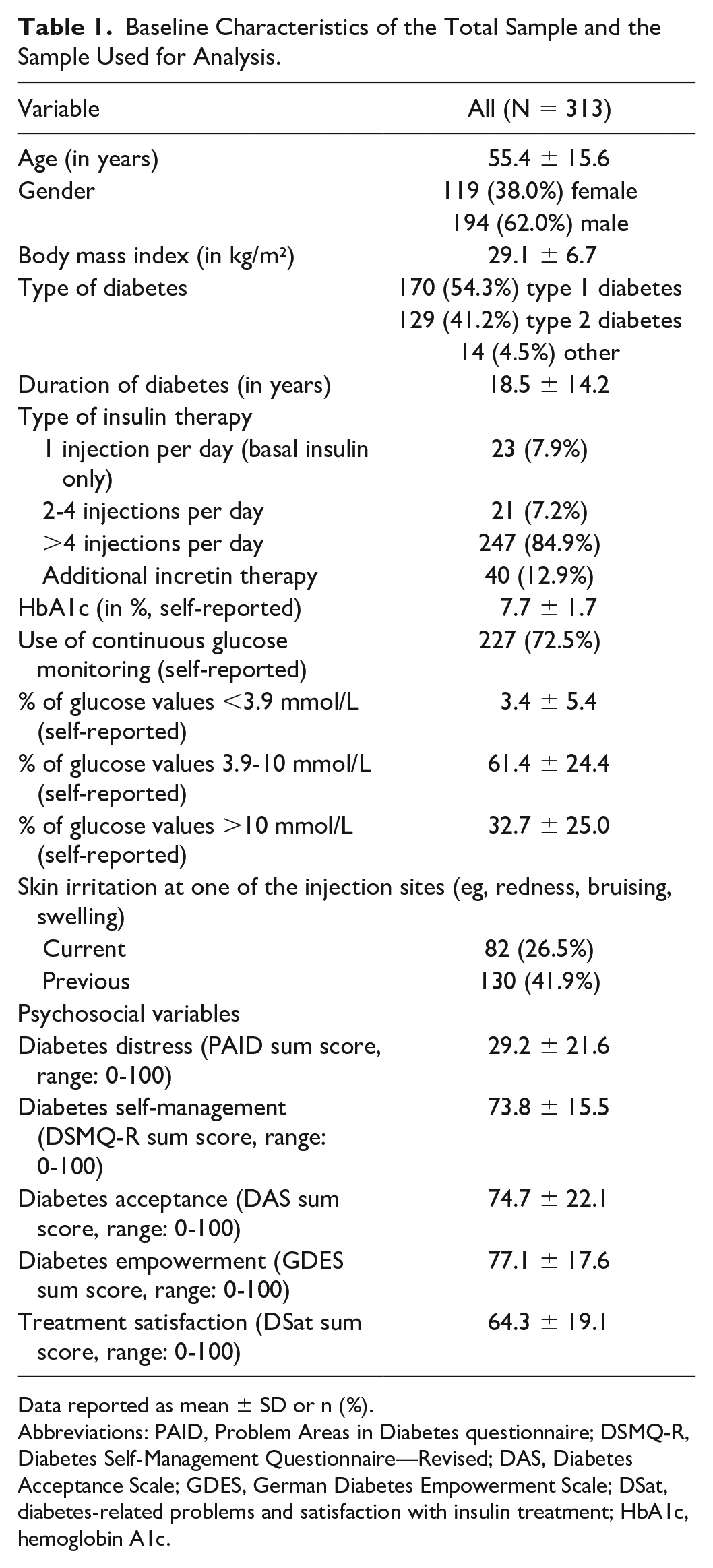
Data reported as mean ± SD or n (%).
Abbreviations: PAID, Problem Areas in Diabetes questionnaire; DSMQ-R, Diabetes Self-Management Questionnaire—Revised; DAS, Diabetes Acceptance Scale; GDES, German Diabetes Empowerment Scale; DSat, diabetes-related problems and satisfaction with insulin treatment; HbA1c, hemoglobin A1c.
Selection of Final Items and Reliability of Scales
Based on item characteristics (item difficulty, item total correlation), factorial structure (factor loadings, communality), and analysis of content, the final items for the two scales were selected.
For the barriers scale, 12 items were selected for the final scale that achieved a Cronbach’s alpha of 0.74 (Table 2). Deleting an item would not have resulted in a substantial increase in Cronbach’s alpha while simultaneously not leading to a loss of information. The exploratory factor analysis revealed three factors that explained 55.2% of the variance (Table 2). After inspection of content, these three factors were named “emotional barriers of injection” (five items, Cronbach’s alpha = 0.83), “behavioral barriers of injection” (four items, Cronbach’s alpha = 0.54), and “knowledge barriers of injection” (three items, Cronbach’s alpha = 0.53). For the 12 items, a sum score was calculated and transformed to a scale from 0 to 100, with higher scores indicating greater barriers toward insulin injection.
Item and Scale Characteristics of the Barriers Toward Insulin Injections Scale (IIT-B).
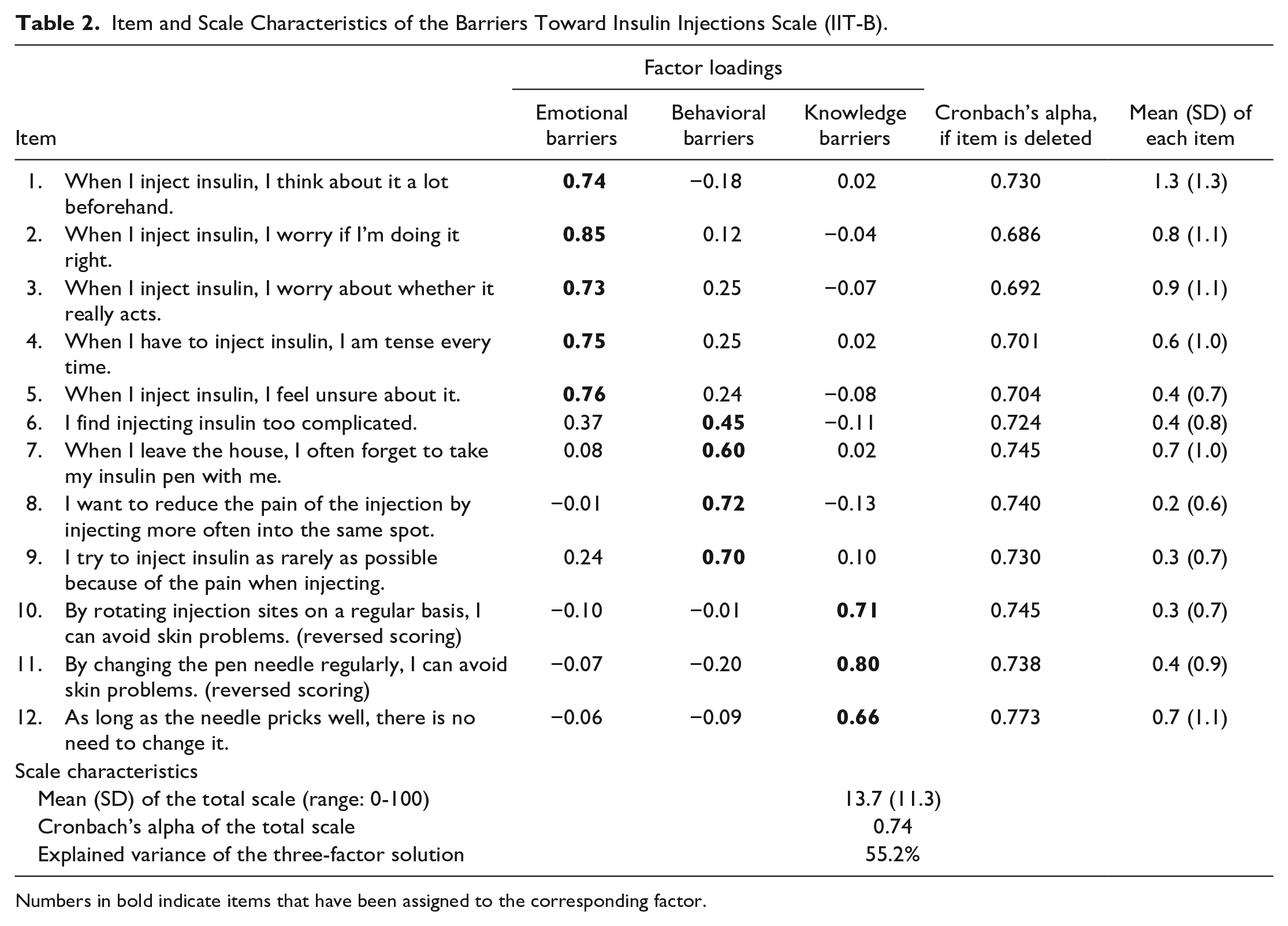
Numbers in bold indicate items that have been assigned to the corresponding factor.
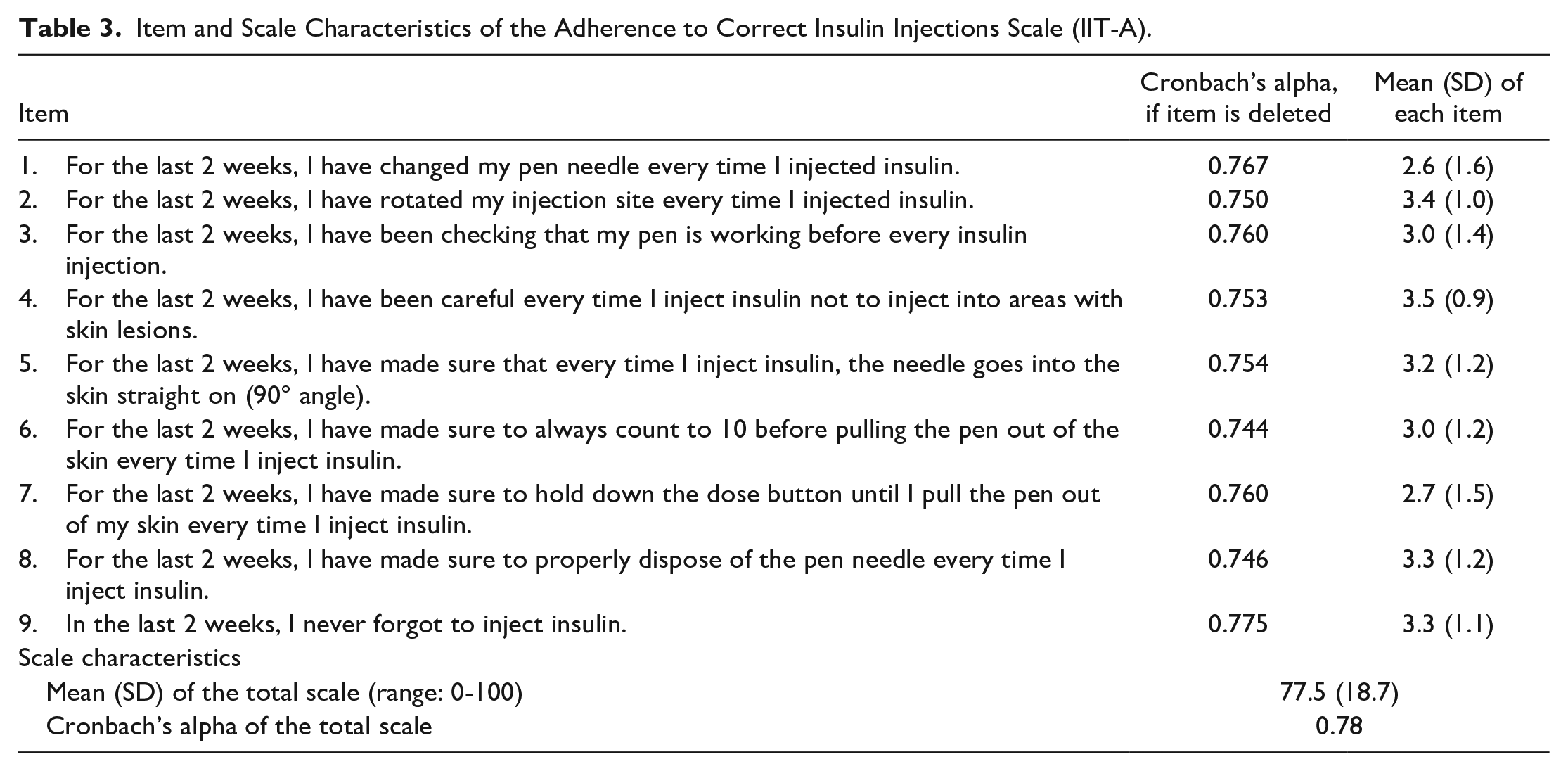
For the adherence scale, all nine items were selected, achieving a Cronbach’s alpha of 0.78 (Table 3). Deleting an item would not have resulted in an increase in Cronbach’s alpha. A one-factor solution was chosen based on inspection of the Scree plot, which explained 37.8% of variance. For the nine items, a sum score was calculated and transformed to a scale from 0 to 100, with higher scores indicating higher adherence to the correct insulin injection technique.
Item and Scale Characteristics of the Adherence to Correct Insulin Injections Scale (IIT-A).
Validity
The barriers scale was significantly negatively correlated with the adherence scale (Table 4). Thus, greater barriers toward insulin injections were associated with lower adherence to a correct insulin injection technique. Both scales showed significant associations with the other questionnaires selected as criterion validity parameters (Table 4). Greater barriers were associated with higher diabetes distress, less optimal diabetes self-management, lower diabetes acceptance, lower diabetes empowerment, and lower treatment satisfaction (all P < .001). Furthermore, greater barriers were associated with more injection pain, lower time in range, and more time above range (all P < .05). Higher adherence to the correct injection technique was associated with less diabetes distress, more optimal diabetes self-management, higher diabetes acceptance, higher diabetes empowerment, and higher treatment satisfaction (all P < .05).
Criterion Validity of the Barriers and Adherence Scale.
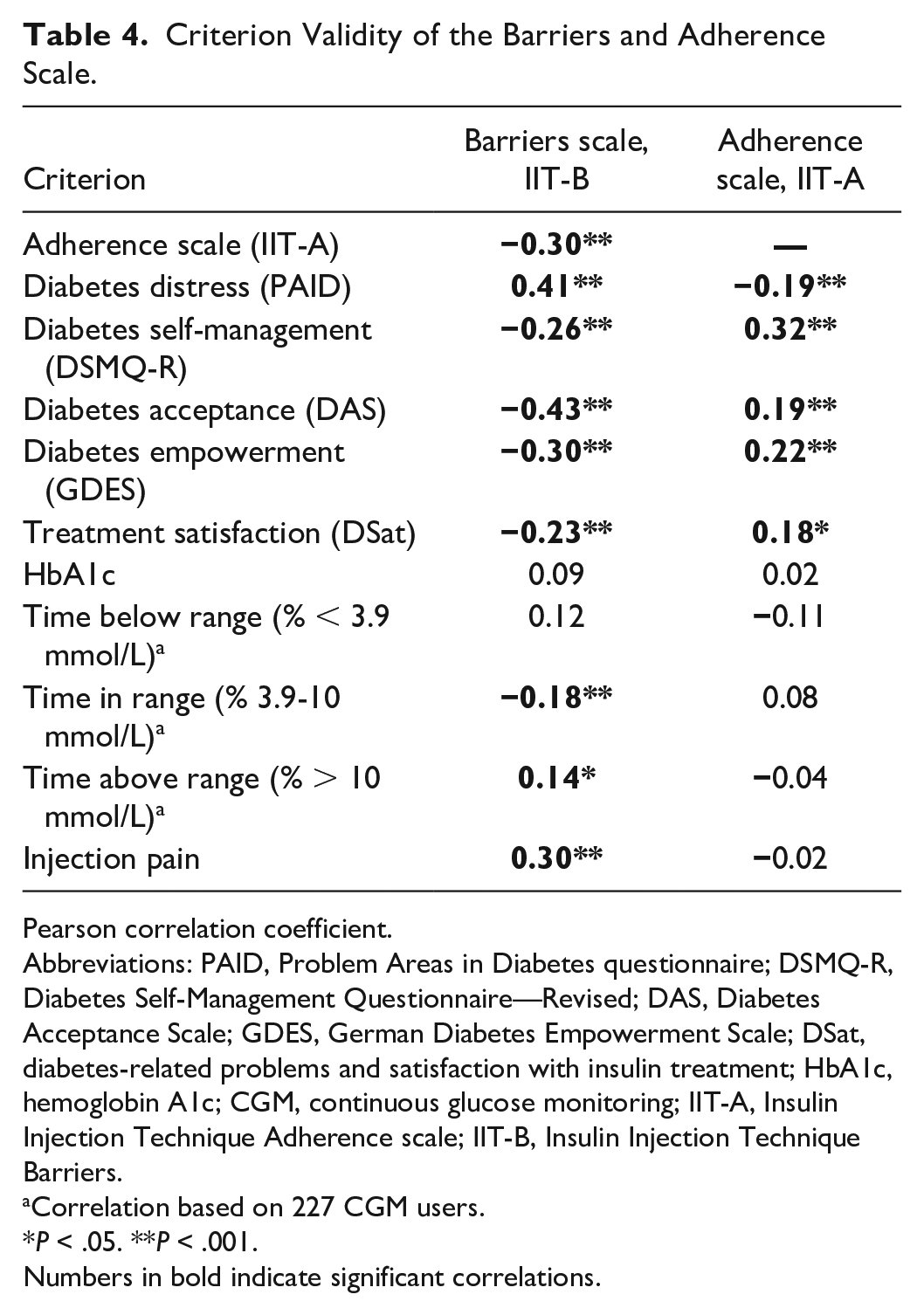
Pearson correlation coefficient.
Abbreviations: PAID, Problem Areas in Diabetes questionnaire; DSMQ-R, Diabetes Self-Management Questionnaire—Revised; DAS, Diabetes Acceptance Scale; GDES, German Diabetes Empowerment Scale; DSat, diabetes-related problems and satisfaction with insulin treatment; HbA1c, hemoglobin A1c; CGM, continuous glucose monitoring; IIT-A, Insulin Injection Technique Adherence scale; IIT-B, Insulin Injection Technique Barriers.
Correlation based on 227 CGM users.
P < .05. **P < .001.
Numbers in bold indicate significant correlations.
Group differences were calculated for those with versus without current skin irritations at least at one injection site. Those with current injection-related skin irritations reported significantly greater barriers (16.3 ± 10.7 vs 12.8 ± 11.4; P = .018; Cohen’s d = 0.31) and a significantly lower adherence (72.4 ± 20.1 vs 79.4 ± 17.9; P = .004; Cohen’s d = 0.38).
Receiver Operating Characteristics
Receiver operating characteristics analysis (Table 5) showed significant areas under the ROC curve (AUC) of the barriers (AUC = 0.62; P = .002) and adherence (AUC = 0.61; P = .004) scales. For the barriers scale, a cutoff value ≥10 would result in a sensitivity of 71.3%, with a specificity of 50.2% to detect skin irritations at an injection site. For the adherence scale, a cutoff value ≤87.5 would result in a sensitivity of 74.7% with a specificity of 40.5% to detect skin irritations at an injection site.
Receiver Operating Characteristics (ROC) Analysis When Classifying People With Current Skin Irritations at One Injection Site.
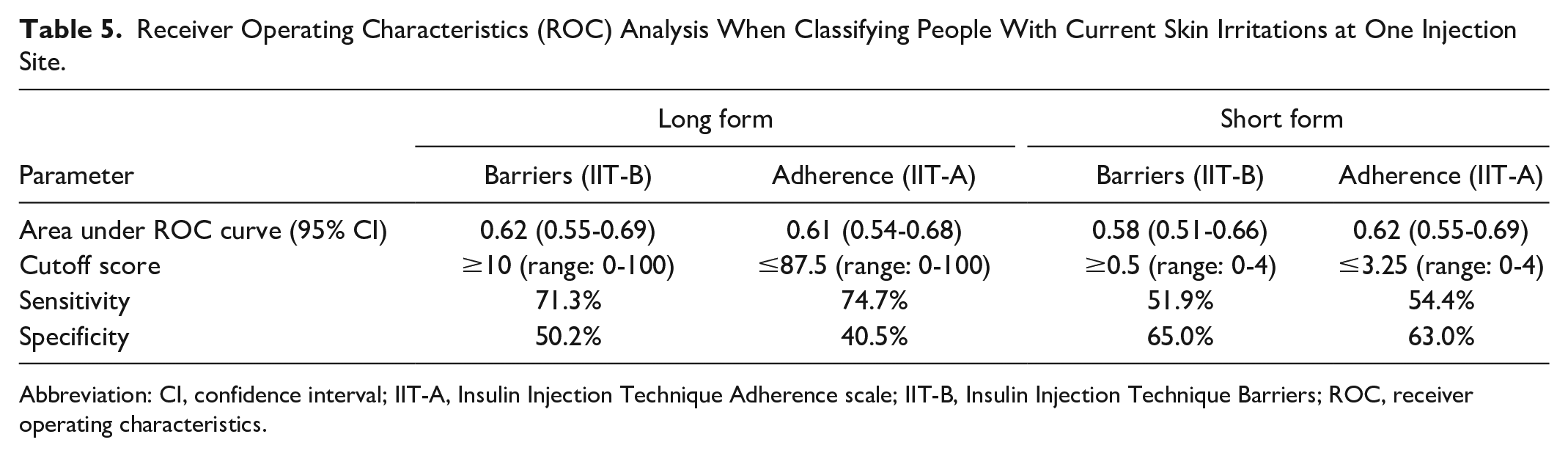
Abbreviation: CI, confidence interval; IIT-A, Insulin Injection Technique Adherence scale; IIT-B, Insulin Injection Technique Barriers; ROC, receiver operating characteristics.
Possible Short Versions
For the barriers scale, items 2, 9, and 11 had the strongest psychometric properties within each factor. A sum score of these three items was calculated that showed a correlation with the 12-item total scale of r = 0.86 (P < .001). The barriers short form achieved an AUC of 0.90 (P < .001) for classifying increased barriers in the 12-item total scale. For the adherence scale, items 2 and 6 had the strongest psychometric properties. A sum score of these two items was calculated that showed a correlation with the nine-item total scale of r = 0.76 (P < .001). The adherence short form achieved an AUC of 0.86 (P < .001) for classifying problematic adherence in the nine-item total scale. Using further ROC curves, both scales achieved a significant AUC when classifying people with current skin irritations (barriers AUC = 0.58; P = .027; adherence AUC = 0.62; P = .002).
Discussion
Two new assessment tools were developed that reliably and validly assess potential barriers (IIT-B) toward insulin injections and the adherence (IIT-A) to the correct injection technique. The exploratory factor analysis showed that three types of barriers could be assessed namely emotional barriers, behavioral barriers, and knowledge barriers. Emotional barriers comprise mental occupation with insulin injections regarding insulin action, correct injections, and worries around injections and feeling tense when injecting insulin. Avoidance behavior, behavior to minimize injection pain, and forgetfulness constitute the behavioral barriers that are assessed. Knowledge barriers comprise the awareness that rotating injection sites and changing needles are beneficial to avoid problems. In addition to these barriers, nine items assessed the adherence to the correct insulin injection technique as defined in the international recommendations.6,7,22 Correlations to other questionnaires demonstrated the criterion validity of both scales as significant associations in the expected direction were found. Of particular interest, greater barriers were associated with greater diabetes distress and lower diabetes acceptance, indicating that the questionnaire indeed covered important barriers. Significant associations of both scales with general diabetes self-management behavior showed that the assessed barriers and injection behaviors are clinically important. The ROC analysis also demonstrated that both scales allow a classification of people with skin irritations at an injection site, which is better than a classification by chance. This indicates the utility of both scales for clinical practice.
Thus, both scales allow an identification of persons in need of both education and re-education either due to substantial barriers toward insulin injections or due to problems with the correct injection technique. Substantial barriers may indicate psychosocial issues with the injection process that should be carefully addressed in a one-to-one education session or in a group education where different experiences and attitudes toward injection can be discussed with other people with diabetes. Problems with the correct injection technique requires training of the technique and raising awareness that the correct injection process is important for achieving optimal insulin action. There is some evidence that such an education about the injection technique is beneficial with some effects on glycemic control18,21 and even cost-effectiveness. 28 However, randomized controlled trials by Campinos et al 29 and Chen et al 30 did not find similar effects. A recent meta-analysis therefore concludes that education on injection technique may have beneficial effects on total daily dose of insulin, but evidence on HbA1c and hypoglycemia is uncertain. 31
Based on psychometric characteristics, we propose a short form for assessing barriers consisting of three items and a short form for assessing adherence consisting of two items. The correlational analysis showed that these short forms represent the respective total scale quite well. Thus, these short forms may be used in clinical practice as screening tools to quickly identify potential problems with insulin injections. However, further validation of these short forms is needed.
When interpreting the findings, the following limitations should be considered: The barriers scale showed a floor effect with a mean score of only about 13% of the scale range. Simultaneously, the adherence scale showed a ceiling effect with a mean score of 78% of the scale range. As a result, the ROC analysis yielded significant results, but its sensitivity and specificity to identify people with skin irritations certainly have room for improvement. Further evaluation of the two newly developed scales in clinical practice and intervention studies is needed, particularly with respect to cutoff scores. In addition, the adherence scale contains items specific to injection therapy with pens. Applicability and generalizability to people using syringes may be limited.
Conclusions
Proper insulin injections are an important foundation for correct insulin therapy.6,7 Thus, it is of high clinical value to assess any barriers toward correct insulin injection technique. Although the existing ITQ assesses correct injection technique, 22 it rather allows a more qualitative assessment of injection technique without calculation of a quantitative sum score. Furthermore, the ITQ does not address potential psychosocial barriers to insulin injections. Therefore, we developed two scales (IIT-B and IIT-A) that assess (psychosocial) barriers to insulin injections and adherence to the correct insulin injection technique. In an evaluation study including inpatients from a specialized diabetes center and outpatients from a diabetes online panel, the reliability and validity of both scales were demonstrated. The two scales can be used in clinical practice to identify persons in need of education regarding insulin injections. The two scales are eligible to be used in clinical practice to find starting points for discussing barriers and behaviors related to correct insulin injections, allowing a personalized approach to improving insulin injections.
Footnotes
Acknowledgements
We thank Gina Lehmann for her help with the data collection.
Abbreviations
AUC, area under curve; CGM, continuous glucose monitoring; DAS, Diabetes Acceptance Scale; DSat, diabetes-related problems and satisfaction with insulin treatment; DSMQ-R, Diabetes Self-Management Questionnaire—Revised; GDES, German Diabetes Empowerment Scale; ITQ, Injection Technique Questionnaire; PAID, Problem Areas in Diabetes questionnaire; ROC, receiver operating characteristics.
Authors’ Contributions
D.E., B.K., and N.H. developed the items for the two scales. D.E. collected data and prepared the manuscript. D.E. and N.H. analyzed the data. All authors contributed to the discussion and revised the manuscript.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The evaluation study was approved by the Ethics Committee of the German Psychological Association.
Informed Consent
All participants provided written informed consent before study participation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.E., B.K., T.H., and N.H. received research support from embecta GmbH formerly known as Becton Dickinson Diabetes Care. I.W., S.W., and J.S. are employees of embecta GmbH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of the scales and the evaluation study were funded by embecta formerly known as Becton Dickinson Diabetes Care.