
Abstract
Background:
Elective surgery in patients with insulin-treated type 2 diabetes mellitus (T2D) and the admission period in the hospital, comprise a distinctive and challenging situation for physicians, nurses, as well as for the patients themselves. There is a lack of widely accepted evidence-based and standardized approach of care in regard to perioperative management of patients with insulin-treated T2D.
Methods:
The main purpose of this proof-of-concept study was to investigate whether a standardized insulin and meal regimen on the day of surgery leads to a better management of diabetes in terms of blood glucose (BG) levels. Two different insulin and meal regimens—group A with half of insulin dose given with a standardized postoperative meal and group B with a custom preoperative breakfast and full insulin dose—were compared with Group C with routine care (no meal and no insulin injection on the day of surgery). Each group consisted of 12 to 15 patients. BG measurements were performed pre- and immediately postoperatively, before meals and at bedtime.
Results:
Both standardized and well-defined insulin and meal regimens resulted in better average BG levels in the perioperative period, especially in the morning after the surgery.
Conclusions:
In this study, we observed that a standardized perioperative insulin regimen efficiently lowered postoperative BG levels. Providing a custom breakfast and a full insulin dose resulted in lower postoperative BG levels. These approaches were not associated with an increase in hypoglycemic events. Physicians and nursing staff gave positive feedback to the structured and well-defined approaches.
Keywords
Introduction
Elective surgery in patients with T2D and the inpatient stay in general, present a distinctive and challenging situation for physicians, nurses and patients. In addition to diabetes management, comorbidities, general health, food intake, and interaction of medications (antihyperglycemic and regular) type and duration of surgery are some of the factors that influence the outcome of the surgery.1,2
Patients with T2D who are hospitalized in surgical wards often require extra effort by physicians and nursing staff, who may not be familiar with diabetes management, as diabetes is a comorbidity and not the primary disease for which patients are hospitalized. This can result in acceptance of higher blood glucose (BG) values, mostly due to fear of hypoglycemia.3,4
In some cases, patients with insulin-treated T2D are advised not to take their insulin in the morning on the day of surgery, fearing perioperative hypoglycemia. Subsequently, postoperative meals are taken without insulin administration or with an inadequate insulin dose. This may result in complications such as postoperative hyper- and hypoglycemia that occur frequently at night or in the morning after surgery. Studies have demonstrated an association between perioperative hyperglycemia and adverse clinical outcomes. 2 A meta-analysis including surgical patients with diabetes showed that perioperative BG control of between 150 and 200 mg/dL was associated with reduced perioperative mortality and stroke compared with more liberal control (BG > 200 mg/dL).5 -7
Most of the studies investigating perioperative management of patients with insulin-treated diabetes were performed in patients undergoing major surgery that usually require perioperative intensive care settings.8 -10 Perioperative management of BG levels in minor surgical interventions in inpatient settings, such as in ophthalmology, encompass much uncertainty and still lack a widely accepted evidence-based and standardized approach of care. Until now, research on this topic has only resulted in recommendations from various diabetes societies and clinics, mostly lacking evidence-based data.
The main purpose of this prospective proof-of-concept study was to investigate a standardized insulin regimen on the day of surgery, aiming for a better management of diabetes in regard to BG levels. Furthermore, the study aimed to provide physicians and nursing staff with a structured and well-defined approach for better quality of care.
Methodology
The Department of Ophthalmology at the Medical University of Graz, in collaboration with the Department for Internal Medicine, Division of Endocrinology and Diabetology, carried out a proof-of-concept study in patients with T2D who had to undergo minor eye surgery under local anesthesia. The study involved a two-part investigation, an observational part and an interventional one, the latter consisting of two groups of patients, each with a different interventional approach. The study was registered and approved by the ethics board of the Medical University of Graz (EK-Nr. 32-028 ex 19/20) and was performed according to the principles of good clinical practice and the Declaration of Helsinki. All participants gave written informed consent prior to any study-related procedures.
The study investigated three approaches of diabetes management (groups A, B, and C). The study was carried out on the general wards of the ophthalmology department as part of a quality assurance procedure. Patients’ selection criteria were as follows:
Insulin-treated T2D.
Age > 18 year old (no pregnant women).
Existing insulin therapy, either basal insulin or conventional insulin therapy.
Planned eye surgery under local anesthesia in the following day (duration <90 minutes).
No insulin pump therapy (continuous subcutaneous insulin infusion [CSII]).
Patients were allocated in two interventional groups (A, B) and one control group (C). In the control group (group C, n = 15), routine care, that is, diabetes management at the treating ophthalmologists’ discretion was carried out on the day of surgery. In most cases during routine care, both meals and insulin are withheld in the perioperative phase. The perioperative phase is defined as morning of surgery until 6 hours postoperatively. In all groups, oral hypoglycemic agents were paused 48 hours perioperatively according to local standard procedures. In intervention group A (n = 15), patients received a standardized postoperative meal and half of their regular morning insulin dose with/before the meal, based on pre-existing insulin therapy and correction dose where applicable. This standardized approach was applied based on the recommendation of the British Diabetes Society. 11
In intervention group B (n = 12), patients received a customized preoperative breakfast and the full morning insulin dose on the day of the surgery. The custom breakfast consisted of a bread roll (or two slices of white bread), jam, and tea. Baseline characteristics of the three groups are indicated in Table 1.
Baseline Characteristics of the Three Groups.
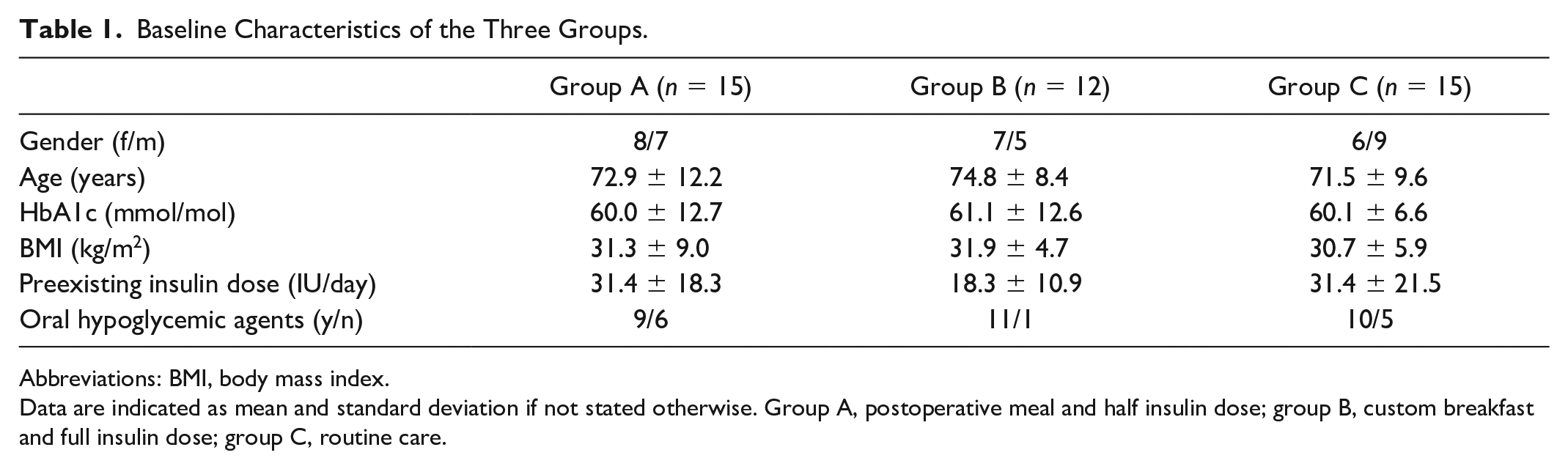
Abbreviations: BMI, body mass index.
Data are indicated as mean and standard deviation if not stated otherwise. Group A, postoperative meal and half insulin dose; group B, custom breakfast and full insulin dose; group C, routine care.
BG was measured preoperatively, immediately postoperatively, before each meal and at bedtime by AccuChek Inform II (Roche Diagnostics, Mannheim, Germany) in each group. Perioperative care was provided by experienced nursing staff.
Results
Baseline characteristics of the three groups were comparable except for antihyperglycemic medication. Insulin dose was lowest in group B who also had the highest rate on adjunct oral hypoglycemic agents.
Preoperative fasting glucose levels were comparable for the three groups (group A: 162.1 ± 52.9 mg/dL, group B: 161.8 ± 34.2 mg/dL and group C: 175.8 ± 43.3 mg/dL). All data are indicated as mean and standard deviation if not stated otherwise.
Patients in the intervention group A who received the administration of a defined postoperative insulin dose (half of their regular morning dose after the postoperative meal) had lower BG values compared with group C except for the bedtime BG value. However, when compared with group A, BG values in group A were higher at all timepoints (Figure 1).
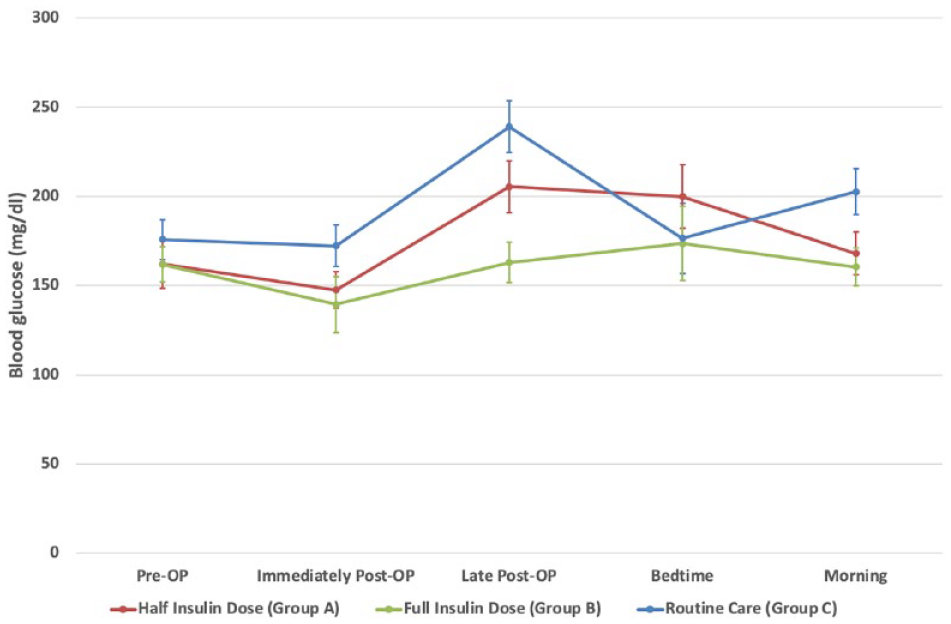
Glucose levels of the three groups (BG, blood glucose levels; Group A, postoperative meal and half insulin dose; Group B, custom breakfast and full insulin dose; Group C, routine care) throughout hospitalization. Data are indicated as mean ± standard error of the mean.
Patients in the intervention group B who received a custom breakfast and full insulin morning dose on the day of surgery showed lower average BG throughout the day of surgery and the subsequent morning when compared with the observational group C, who received routine care.
No hypoglycemic event was observed in any patient.
Insulin doses were lower in group A compared with group B (6.7 ± 6.6 vs 13.9 ± 7.6 IU) as they only received half of their regular insulin dose in the perioperative phase. In group C, only five patients received an insulin injection in the perioperative phase (range of the individual insulin doses: 2-28 IU).
Duration of surgery and types of surgery were comparable between groups (group A: 25 (15-70) minutes, group B: 40 (20-60) minutes and group C: 50 (25-90) minutes; data are indicated as median and range). In the majority of cases, patients underwent vitrectomy.
Because of the proof-of-concept methods of the study and its small sample size, the study possesses no statistical power, and the results are not statistically significant.
Discussion and Conclusions
Inpatient stays of patients with insulin-treated T2D present a challenging situation for physicians and nursing staff, especially on the day of surgery when managing meals and insulin therapy. The increasing demand for shorter inpatient stays and same-day surgery leads to additional stress, requiring special attention to patients’ metabolic control. The lack of standardized evidence-based guidelines in perioperative settings means that BG fluctuations may be observed on the day of surgery and the day after.
This proof-of-concept study aimed to address these challenges by investigating whether a standardized perioperative administration of insulin according to a well-defined scheme could efficiently lower postoperative BG levels, which are associated with better outcomes.5 -7
The study’s findings suggest that customized diabetes management interventions can show promising results in managing perioperative BG levels in patients with insulin-treated T2D undergoing minor eye surgery under local anesthesia.
Providing a custom breakfast and patients’ regular insulin dose resulted in a further lowering of postoperative BG levels without increasing the risk of hypoglycemia. The interventions were safe and feasible and could potentially lead to better surgical outcomes and less postoperative complications in this patient population.
It is worth mentioning that physicians and nursing staff gave positive feedback on the structured and well-defined perioperative approach. This offers the possibility of providing better care to patients, which can have significant implications for managing perioperative BG levels and preventing complications in patients with insulin-treated T2D.
This study had some limitations. The small sample size and lack of statistical power mean that the results are not statistically significant. Furthermore, the study only investigated minor ophthalmological surgeries, limiting the generalizability of the findings to other types of surgeries. Therefore, larger studies with a more diverse patient population are necessary to validate the effectiveness of these interventions.
As a next step, this proof-of-concept approach will be tested in other departments, including Dermatology, General Surgery, Gynecology and Obstetrics, and Otolaryngology, for minor surgeries through studies with higher statistical power. If this approach proves successful, it will be incorporated into the clinical decision support system for diabetes management (GlucoTab, decide Clinical software GmbH, Graz, Austria) routinely used at the University Hospital Graz.
Footnotes
Abbreviations
BG, blood glucose; T2D,type 2 diabetes mellitus; CSII, continuous subcutaneous insulin infusion.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JKM is a member on the advisory board of Becton-Dickinson, Eli Lilly, embecta, Medtronic, NovoNordisk, Pharmasens AG, Roche Diabetes Care, and Sanofi-Aventis and received speaker honoraria from Abbott Diabetes Care, A. Menarini Diagnostics, Becton-Dickinson, Dexcom, Eli Lilly, Medtrust AG, NovoNordisk, Roche Diabetes Care, Sanofi-Aventis, Servier, and Ypsomed. BS received speaker honoraria from NovoNordisk. The other authors do not have a conflict of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.