
Abstract
Widespread uptake of telehealth in response to the COVID-19 pandemic has highlighted geographic, demographic, and economic disparities in access to virtual care. However, research studies and clinical programs that predate the pandemic demonstrate the potential for telehealth-based interventions to improve access to and outcomes of type 1 diabetes (T1D) care for individuals in geographically or socially marginalized communities. In this expert commentary, we discuss telehealth-based care models that have been successful in improving care for marginalized T1D populations. We also outline the policy changes needed to expand access to such interventions to reduce established disparities in T1D care and promote better health equity among people living with T1D.
Introduction
The dramatic rise in telehealth use during the COVID-19 pandemic has increased both awareness of its potential benefits and critique for its limitations and potential harms. This is particularly true in the arena of health equity. Concerns abound regarding the impact of telehealth on existing race-, income-, language- and geography-related health disparities, and its capacity to introduce new disparities based on age and digital literacy.1 -10 However, broader telehealth use during the pandemic has also fostered an appreciation for its ability to facilitate individualized and person-centered care, and has led to thoughtful consideration for how it can be used to improve health equity moving forward.11 -14
Type 1 diabetes (T1D) is uniquely positioned among chronic conditions to explore questions of technology-based health equity. The importance of the digital divide has been increasingly apparent in T1D care during recent decades due to the expanding role of therapeutic technology such as continuous glucose monitoring, insulin pumps, and automated insulin delivery. 15 Disparities in access to therapeutic technology and health outcomes based on income and race/ethnicity are well-documented for people with T1D.16 -26 In addition, T1D care is well-suited to telehealth due to its reliance on patient-generated health data and behavioral health coaching; for this reason, telehealth was employed for T1D management even prior to the COVID-19 pandemic.
In this commentary, we outline ways in which telehealth can be harnessed to improve care delivery and outcomes for people with T1D from communities experiencing geographic or social marginalization. We provide examples of successful telehealth interventions for marginalized T1D populations (summarized in Table 1) and conclude by discussing the policy context that will enable telehealth-based strategies to reduce health disparities in T1D care moving forward. While the term telehealth can refer broadly to any medical care delivered via telecommunications technology, this article focuses on synchronous telehealth interactions between patients and health care team members and does not discuss the parallel sphere of mobile and digital health applications within diabetes care. 49
Telehealth-Based Interventions to Improve T1D Care for Marginalized Communities.
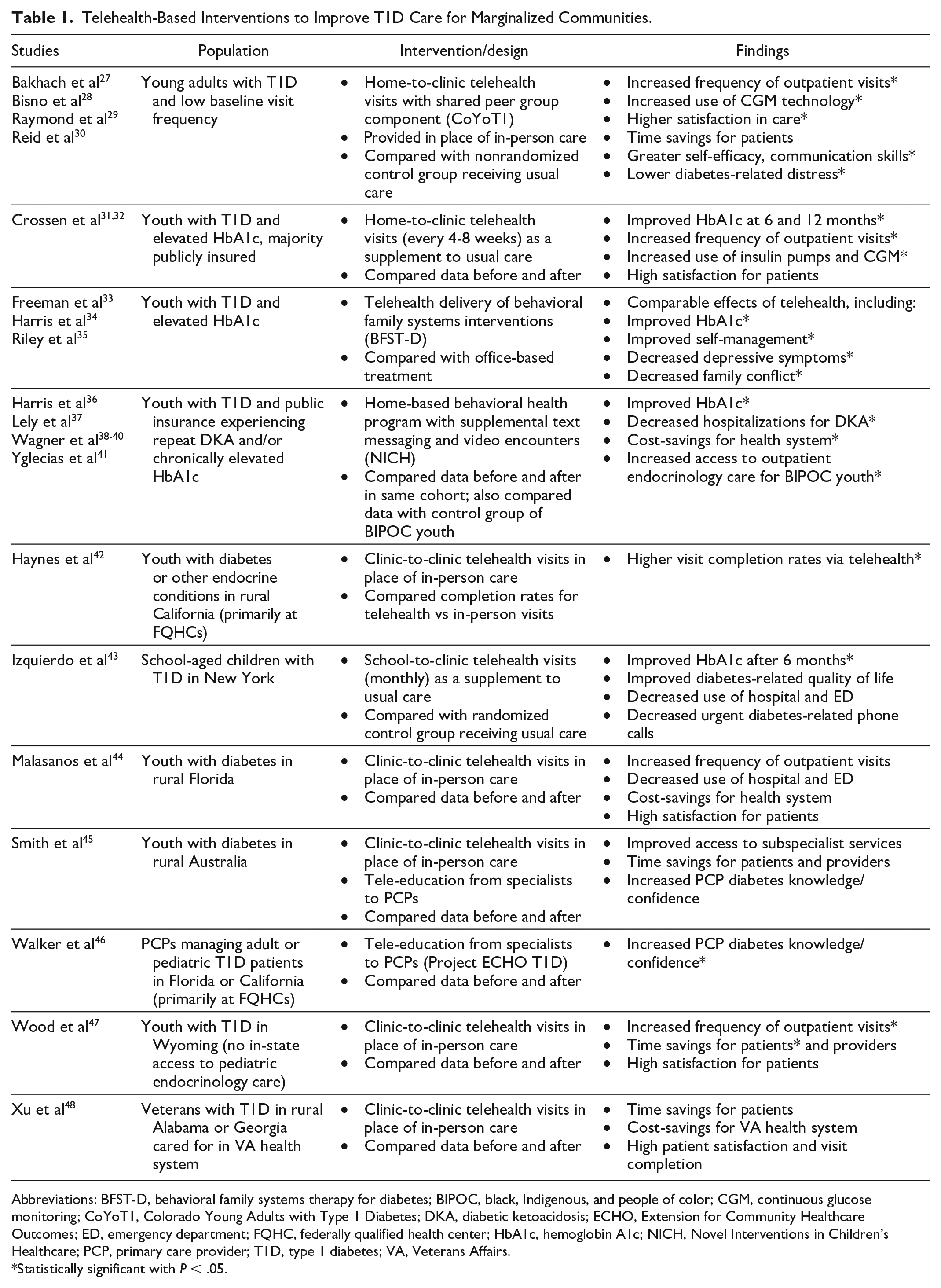
Abbreviations: BFST-D, behavioral family systems therapy for diabetes; BIPOC, black, Indigenous, and people of color; CGM, continuous glucose monitoring; CoYoT1, Colorado Young Adults with Type 1 Diabetes; DKA, diabetic ketoacidosis; ECHO, Extension for Community Healthcare Outcomes; ED, emergency department; FQHC, federally qualified health center; HbA1c, hemoglobin A1c; NICH, Novel Interventions in Children’s Healthcare; PCP, primary care provider; T1D, type 1 diabetes; VA, Veterans Affairs.
Statistically significant with P < .05.
Geographically Marginalized Communities
Many of the pre-pandemic applications of telehealth within T1D care were designed to address geographic access barriers. These barriers apply not only to persons with diabetes (PWD) living in rural areas but also to those who are mobile due to career (eg, military) or life stage (eg, young adults [YAs]). The shortage and uneven geographic distribution of adult and pediatric endocrinologists in the United States,50 -54 combined with rising incidence of T1D 55 has necessitated telehealth solutions to provide subspecialty care for PWD living at a significant distance from their T1D care providers.
Pilot programs in both the United States and Australia have demonstrated success in using telehealth to connect endocrinologists to PWD living in rural areas without local access to subspecialty care.42,44,45,47 These programs—enacted prior to the COVID-19 pandemic and its attendant health care policy changes related to place of service 56 —used clinic-to-clinic rather than home-to-clinic telehealth connections. They therefore relied on partnerships between urban and rural health care centers, located anywhere from 40 45 to >200 miles 47 apart. Findings from these studies included high levels of satisfaction as well as cost-savings and time-savings for participants. Some also documented an increased frequency of subspecialty visits with the addition of telehealth,42,44,47 illustrating that patient-centered outcomes like time-savings can be achieved alongside labor-intensive care processes like quarterly visits.
Telehealth can also be used to improve T1D care for PWD in rural and underserved areas by facilitating education and support of local primary care providers (PCPs) by regional subspecialists. Project ECHO (Extension for Community Healthcare Outcomes) T1D connects PCPs at community health centers with endocrinologists at regional “hub” locations. The endocrinologists provide PCPs with regular education about T1D care via group videoconferencing sessions, and also support them as needed with real-time advice about diabetes-related care decisions for their patients. 46 Initial pilots of Project ECHO T1D have demonstrated improved diabetes-specific knowledge among participating PCPs, 46 with large-scale implementation and evaluation ongoing.
Geographically marginalized communities include demographic groups who are mobile due to profession or life stage and therefore unable to sustain physical proximity to their T1D care providers. For example, US military veterans rely on the Veterans Affairs (VA) health care system for medical care but may reside at a distance from a VA health care facility with T1D specialists. An innovative solution to this problem was piloted in the Southeast in 2014-2016, connecting veterans living with T1D in rural Alabama and Georgia to Atlanta endocrinologists via telehealth. 48 The intervention resulted in time-savings for patients, cost-savings for the VA, and high rates of patient satisfaction and appointment completion. 48
Another mobile demographic group is YAs, who often leave home between the ages of 18 and 25 years but do not yet have independent access to health insurance or health care services, and therefore remain reliant on T1D providers in their previous home communities. Maintaining regular in-person appointments at a distant location presents significant challenges, contributing to the detrimental gaps in outpatient care observed among this age group.21,57 However, YAs tend to have high levels of access to both smartphones and Internet coverage, 58 making home-to-clinic telehealth a viable option. Recent studies have demonstrated success at improving T1D care frequency as well as satisfaction and engagement with T1D care among YA using telehealth visits as compared with in-person care.29,30
Use of telehealth can thus improve care delivery for demographic groups which are geographically distant from their designated T1D providers, as well as those located in rural areas without subspecialist access. It is important to note that the ability to participate in home-to-clinic telehealth relies heavily on home Internet and smartphone access, 59 for which significant disparities exist based on rurality, age, income, education, and race/ethnicity.58,59 Therefore, clinic-to-clinic telehealth programs remain an important conduit for delivering care to geographically marginalized communities, and partnerships between urban specialists and rural health centers for the purposes of provider education and/or direct care delivery hold the potential to significantly improve care for PWD living in historically underserved regions.
Socially Marginalized Communities
The effects of social determinants of health (SDOH) on T1D care and outcomes are well-established. PWD who live with stressors like financial insecurity, mental illness, and limited family or peer support are less likely to receive the care they need or to achieve optimal health outcomes.60 -66 While telehealth cannot solve many of these root issues, it can reduce the barriers they pose to receiving T1D care and can facilitate additional interventions—such as access to supplemental visits, peer support, and behavioral family therapy—that may benefit these communities. In contrast to interventions for geographically marginalized communities—which tend to replicate typical T1D care at a distance—successful interventions for socially marginalized communities often leverage telehealth to implement new care delivery models that would not be feasible in-person.
National data demonstrate that PWD from low-income households and historically marginalized racial/ethnic groups in the United States experience higher hemoglobin A1c (HbA1c) levels, 19 which puts them at heightened risk for short-term and long-term complications of T1D. The Diabetes Complications and Control Trial demonstrated that delivery of more frequent outpatient care (monthly clinic visits with additional telephone contact) could improve glycemic control and long-term outcomes for individuals with T1D. 67 However, this frequency of in-person care has proved difficult to replicate in practice, even with dedicated care coordinators.68,69 Telehealth presents an opportunity to deliver supplemental care to individuals with T1D experiencing high glycemic levels and SDOH like financial and transportation insecurity which make in-person visits infeasible.
This was illustrated by a recent study which delivered telehealth visits every 4 to 8 weeks as a supplement to usual in-person visits to a cohort of primarily publicly insured youth with elevated HbA1c levels. The cohort demonstrated significant improvement in glycemic control (0.8%-1.2% decrease in mean HbA1c) at 6 months and 1 year, as well as dramatic increases in visit frequency and high levels of satisfaction with the intervention.31,32 Participants in this study faced a variety of environmental stressors—including home loss due to wildfire, domestic violence requiring evacuation to a shelter, and lack of permanent housing—but maintained high access to T1D care via telehealth. Another study which delivered monthly school-based diabetes visits via telehealth in addition to usual quarterly T1D care also demonstrated significant improvement in glycemic control compared with a control group. 43 These projects illustrate the potential for telehealth to enable the higher frequency of care that may be needed to improve glycemic outcomes for PWD struggling with negative SDOH.
Telehealth modalities can also be used to provide support that falls outside the scope of traditional medical care. Novel Interventions in Children’s Healthcare (NICH) 36 is a program that serves youth with chronic medical conditions who are experiencing avoidable health complications due to social risk. Approximately one third of families in this program experience houselessness, and over half experience child protective services involvement, unreliable transportation, and mental health diagnoses—all of which affect their ability to attend appointments and engage in daily T1D management. NICH providers use telehealth communication modalities (eg, synchronous video encounters, text messaging) to identify and address SDOH such as limited transportation and jobs that discourage time off for medical appointments. Among youth with T1D, NICH has led to reduced hospitalizations and emergency department visits, improved glycemic control, and increased care access for PWD from historically marginalized racial and ethnic groups.37 -41 Programs like NICH that use telehealth technology to better understand and meet the needs of youth and families experiencing disparities represent innovative solutions to the access barriers associated with traditional models of health care delivery.
In addition to facilitating added support from health care teams, telehealth can also be used to augment peer support for PWD. This is particularly important for YAs, who tend to experience worse glycemic control and higher rates of psychosocial challenges compared with other ages.19,21,70 -73 The CoYoT1 Clinic model—which uses telehealth to enable virtual peer group interaction as part of shared medical appointments 30 —has been highly successful at meeting the needs of this age group. CoYoT1 Clinic visits have been shown to reduce psychosocial distress and to improve self-efficacy, problem-solving, and communication skills among YAs with T1D when compared with usual care 27 or with telehealth-only appointments without peer support. 28
For adolescents and children with T1D, family dynamics are also a strong determinant of glycemic control.74 -78 Behavioral Family Systems Therapy (BFST), 79 a family-targeted skills building intervention designed to address barriers to diabetes management, has been successfully modified to be delivered via telehealth. When compared with office-based delivery of BFST, BFST delivered via telehealth was equivalent and demonstrated success in improving HbA1c, improving diabetes self-management, and reducing depressive symptoms in youth as well as parent-child conflict.33 -35 Targeted telehealth interventions have also demonstrated success in reducing parenting stress and hypoglycemia fear in parents of youth with T1D 80 as well as improving problem-solving skills. 81 While these studies did not specifically enroll families from marginalized communities, such interventions show promise in increasing access to evidence-based behavioral health treatments via telehealth, and should be evaluated at a larger scale among those experiencing negative SDOH.
Discussion
The explosion in telehealth use since onset of the COVID-19 pandemic has focused attention on the “digital divide,” and resulting disparities in virtual care access—particularly for individuals with public insurance, minority race or ethnicity, older age, and non-English language preferences—have been well-documented.1 -10 However, many innovative care programs outlined in this article demonstrate how telehealth can be used to reduce longstanding disparities in T1D care access and outcomes. For geographically marginalized communities, telehealth interventions have been shown to improve access to and frequency of T1D care. For socially marginalized communities, telehealth can enable supplemental care that improves glycemic control, mental health, and self-efficacy.
The successful telehealth interventions discussed in this commentary provided increased assistance from medical and support staff as compared with usual clinical care, increased technical infrastructure in some cases (eg, internet-enabled mobile devices), and often provided care outside of payer-imposed restrictions due to separate funding sources. Therefore, it is not surprising that the rapid, broad-scale expansion of telehealth at the start of the COVID-19 pandemic—which made virtual care “available” without added staff assistance or infrastructure for patients in most locations—did not succeed in narrowing care disparities for marginalized groups. The missing link between research and practice consists of the policy environment needed to support broad-scale implementation of telehealth-based interventions that have proven to be effective.
To “narrow the divide” and improve health equity among people living with T1D, policy changes are needed in the arenas of health insurance coverage, digital infrastructure, and the health care workforce. Remote care for T1D hinges on the ability to access patient-generated health data from continuous glucose monitoring (CGM) devices and insulin pumps, but disparities in use of such therapeutic technology persist.16 -20,24 -26 Health insurance plans must universally cover CGM and insulin pump devices—now recommended as treatment options for people of all ages82,83—as a first step. Government policies are needed in parallel to expand broadband Internet access—no longer a luxury but now a strong determinant of outcomes in both health 84 and education 85 —which would enable remote data-sharing as well as synchronous telehealth interactions. In addition, government programs to make audio-video devices available at no cost and to provide personalized training in their use at community centers or libraries would help address technological barriers to telehealth engagement.
At a fundamental level, the innovations needed to optimize outcomes for marginalized T1D communities would be best supported through value-based or capitated reimbursement structures. However, revisions to current fee-for-service systems can also facilitate the broader adoption and maintenance of beneficial telehealth-based care. Reimbursement for telehealth visits must remain comparable with in-person visits in the post-pandemic era, or health care systems will not continue to make resources and staff available to support virtual care. In addition, a variety of telehealth modalities—including video, audio-only, and electronic messaging—should be covered by medical insurance to support flexible, personalized care plans that can be adapted to patients’ individual needs and circumstances. Finally, behavioral and psychosocial interventions—such as NICH, BFST, and virtual peer group support—that are demonstrated to improve health outcomes for PWD from marginalized communities need to be covered by medical insurance plans. This coverage would allow them to be broadly accessible, rather than restricted to populations where funding is available from external contracts or research grants. It would also enable them to be delivered in close coordination with medical T1D care, instead of requiring external providers—who may have no T1D expertise—to deliver all behavioral health care under “carve out” mental health benefit plans.
Several policy changes related to the medical workforce are needed to better promote T1D health equity via telehealth. First, expanding interstate licensing agreements 86 and/or redefining site of care as the provider’s location would facilitate access to and continuity of subspecialty care for people with T1D living across state lines from their T1D providers. This is of particular concern for marginalized communities, including those in rural areas without access to endocrinologists, YAs who move away from home for educational or work opportunities, and individuals with employment or housing insecurity who move frequently. Second, incentives to expand the T1D health care workforce—not just endocrinologists 87 but also certified diabetes care and education specialists, psychologists, and social workers—are needed to ensure there are enough providers to deliver the frequent T1D care and behavioral health care that we know can improve outcomes for PWD in marginalized communities. During this process of workforce expansion, health care systems must also prioritize hiring practices and training efforts that intentionally recruit and retain individuals from historically marginalized populations, as patient-provider cultural concordance has been shown to influence trust, 88 which in turn affects the likelihood of telehealth adoption. 89
In summary, significant policy changes across multiple systems are required to increase access to effective telehealth interventions for populations frequently marginalized. Innovative clinical and research programs have demonstrated the potential for telehealth to reduce inequities in T1D care delivery and outcomes. However, this potential will not be fully realized unless health care and government leaders alter existing regulations and reimbursement systems to ensure such services can reach those most in need.
Footnotes
Abbreviations
CGM, continuous glucose monitoring; HbA1c, hemoglobin A1c; NICH, Novel Interventions in Children’s Healthcare; PCP, primary care provider; PWD, persons with diabetes; SDOH, social determinants of health; T1D, type 1 diabetes; YA, young adult.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Crossen receives research funding from the National Institute of Diabetes and Digestive and Kidney Diseases (grant number K23DK125671). The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.