
Abstract
Background:
The magnitude of the response of the diabetes professional community to the COVID-19 pandemic is not known. We aimed to examine diabetes technology research trends and resources offered by professional organizations during this period.
Methods:
We explored patterns of the response from the professional diabetes community to the pandemic by (1) systematically searching for articles related to diabetes, COVID-19, and diabetes technologies; (2) examining publication trends of research protocols (clinicaltrials.gov) and preprints (medRxiv); and (3) reviewing online resources from professional organizations including our website (COVIDinDiabetes.org; an Emory University—Diabetes Technology Society collaboration).
Results:
We identified 492 articles published between December 2019 and December 2022 meeting our inclusion criteria. Telemedicine and continuous glucose monitoring were the most common reported technologies from most parts of the world. The largest number of preprint articles was published in 2020, with a decline in 2021 and 2022. The number of research protocols related to COVID-19 was the highest in 2020 and declined in 2021 and 2022. Resources from organizations included protocols adapted to treat patients with diabetes and COVID-19, training programs, emergency preparedness, and literature on diabetes and COVID-19. On our website (COVIDinDiabetes.org), there were 12 236 visits and 18 149 pageviews, with 1.6 actions per visits, with most visits coming from North America (N = 7233, 54.2%), South America (N = 2663, 21.8%), and Europe (N = 1219).
Conclusions:
We conclude that the COVID-19 pandemic promoted unprecedented global research productivity related to diabetes and COVID-19 and that the transition to the use of technology resources has been evident during this period.
Keywords
Introduction
In March 2020, the COVID-19 pandemic led to lockdown for most of the world. Since that time, countries around the world have been adjusting their policies and guidelines for the public to avoid the spread and potential infection of COVID-19. Evidence suggests a bidirectional interaction between type 2 diabetes and COVID-19. 1 At the end of 2019 and beginning of 2020, many scientists and clinicians who were working in diabetes research pivoted their research activities to focus on COVID-19 projects to better understand the pathophysiology of COVID-19, risk factors for people contracting the disease, and the best treatments for people with diabetes (PWD) coping with the effects of COVID-19 and pandemic-related precautions. Many turned to using novel monitoring and communication technologies for these purposes. The use of telehealth escalated as PWD and health care professionals both found it safer and, in many cases, more efficient to communicate remotely via telehealth portals. 2
During the pandemic, health care professionals and PWD have sought accurate information about the effects of COVID-19 on PWD as well as the risk of contracting diabetes following an infection with COVID-19. Many protocols to care for patients with COVID-19 were modified to reduce the risk of exposure to health care professionals while attempting to achieve goals of care.3-5 In addition, new resources emerged during the pandemic to facilitate access to literature, protocols, news, and education on diabetes and COVID-19. 6 However, it is important to note that the mass generation of COVID-19-related data also spurred an era of misinformation, with the dangerous potential of harming PWD. 7
First, we present a systematic analysis of the literature published on the use of technologies for PWD since the beginning of the pandemic, including an overview of trends in publications by year, region, and types of technologies. The purpose of the article was to analyze publication trends during the pandemic and the content and utilization of an academic/nonprofit resource website that we developed. Second, we discuss the widespread concern among journal editors about the integrity of the scientific evidence base for information about COVID-19 and diabetes. Finally, we present an overview of selected resources that emerged during the pandemic to facilitate access to relevant information about diabetes and COVID-19, including our experience with a model that aimed to foster collaboration, resource sharing, and service to the community. In our article, we combined a literature review with an analysis of our own resources data because we felt that information from the literature provided a useful perspective for our own findings.
Methods
We systematically searched the PubMed database for articles published between December 2019 and December 2022. We used a combination of terms including ([COVID-19] OR (coronavirus)) AND ([OR (hyperglycemia]) OR (hyperglycaemia)) AND ([CGM] OR (continuous glucose monitoring)) OR (telehealth)) OR (“remote monitoring”)) OR (“virtual care”)). We constructed our search terms based on the fact that our authors felt that the four most important technologies for diabetes at this time were continuous glucose monitoring (CGM), telehealth, remote monitoring, and virtual care. Research articles were selected based on the content of the title and abstract. Full content was then reviewed to determine final inclusion. The search strategy was conducted by AMY, JH, AA, and GMB. Studies were categorized as original, review, commentary, guideline, protocol, meeting summary, or case reports. We also determined the origin of publication and stratified the data according to quarters from the year 2020 to 2022. A total of 790 studies were assessed for inclusion. Following inclusion criteria, a total of 492 studies remained from those initially identified.
To provide an overview of research productivity and efforts to share information as soon as they were emerging, we also examined trends in preprints (not yet peer reviewed) of preliminary reports by examining preprints posted on medRxiv, a free online archive founded by Cold Spring Harbor Laboratory, Yale University, and British Medical Journal. In addition, we examined trends in research studies posted in ClinicalTrials.gov, a database provided by the United States National Library of Medicine to track privately and publicly funded clinical studies conducted around the world. Finally, we discussed the issue of misinformation in scientific journals.
Databases for Resource Sharing
The website COVIDinDiabetes.org was formed by the Emory University School of Medicine in collaboration with the Diabetes Technology Society to focus on relevant literature and resource-sharing initiatives (diabetes protocols, news, meetings) related to diabetes care and COVID-19 with the diabetes community. Four areas of particular interest included (1) inpatient management of patients with both diabetes and COVID-19, (2) applications of technology for diagnosing and treating COVID-19 in PWD, (3) sequelae of COVID-19 in PWD, and (4) pharmacotherapy in people with COVID-19 and diabetes. The website contains an online database of articles from PubMed-referenced journals and the popular press about these four topics, as well as treatment protocols. The database (www.covidindiabetes.org) brought clinicians and scientists from various countries (Brazil, Ecuador, Peru, Spain, United Kingdom, and United States of America) to share ideas and treatment protocols. The two developer teams met every one to two weeks until December 2022, and together, they selected articles for inclusion on the website that were clearly written, based on a consensus that they represented sound science and contained important information. Clinicians and scientists from other institutions also contributed treatment protocols to the database. We present an overview of visits to the website based on data-derived web analytics. In addition, to provide an overview of other platforms that focused on diabetes and COVID-19 resources shared during the pandemic, we examined overall resources shared including literature, protocols, education/training material, preparedness resources, and social media information by the American Diabetes Association (ADA), the Centers for Disease Control and Prevention (CDC), the Association of British Clinical Diabetologists, and MyWay Digital Health.
Results
Research Availability: COVID-19, Diabetes, and Technology Articles
On November 28, 2022, we conducted a literature search in PubMed to identify all articles published since 2019 that were related to COVID-19, diabetes, and technology (Figure 1). Out of 790 articles that resulted from our search strategy, 492 met our inclusion criteria after reviewing the title and abstract. Some articles (N = 298) were excluded because they were not framed within the context of COVID-19, were not focused on diabetes, or did not discuss any technology.
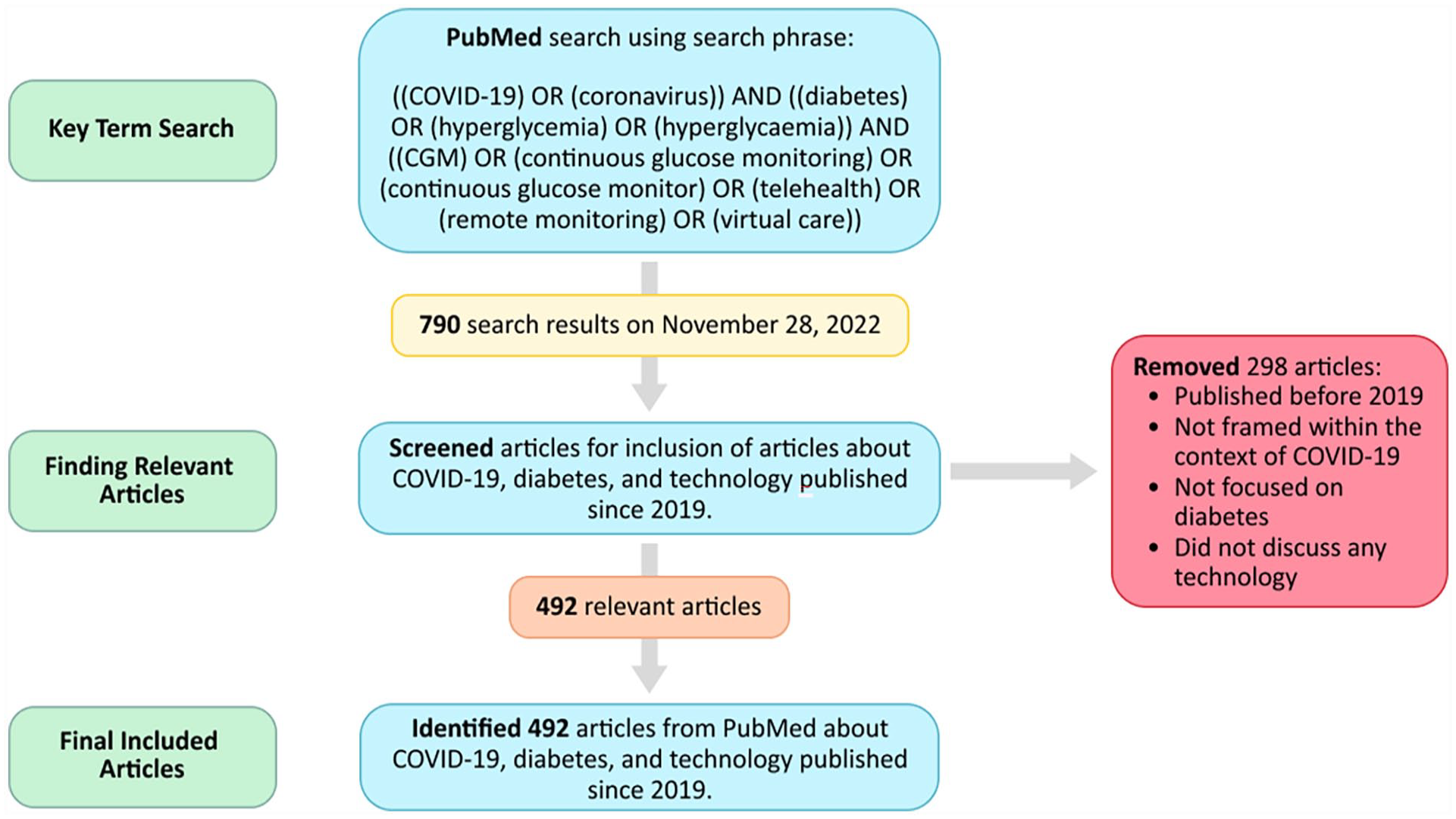
PRISMA diagram to identify articles from PubMed about COVID-19, diabetes, and technology published between December 2019 and December 2022.
There was a steady linear trend of the number of articles published in 2020, 2021, and 2022 (Figure 2). The greatest number of articles published from 2020 to 2022 was in July, August, and September of 2020, with a total of 90 articles. The greatest number of articles was published in 2021, followed by 2020, and 2022.
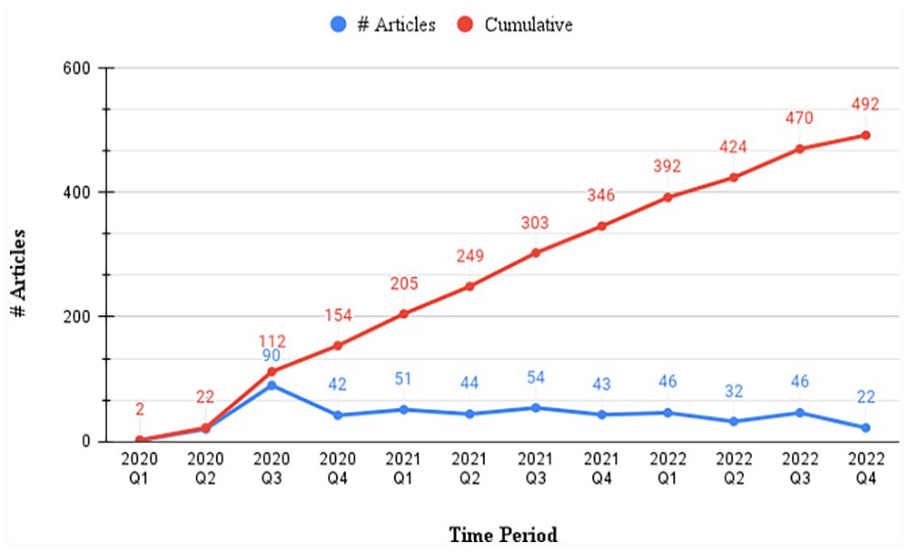
Number of articles per time period.
We grouped the 492 articles by region of publication (Figure 3). The greatest number of articles originated from North America, Europe, and Asia. North America produced the greatest number of articles, and Africa produced the least number of articles about COVID-19, diabetes, and technology over the years 2020, 2021, and 2022.
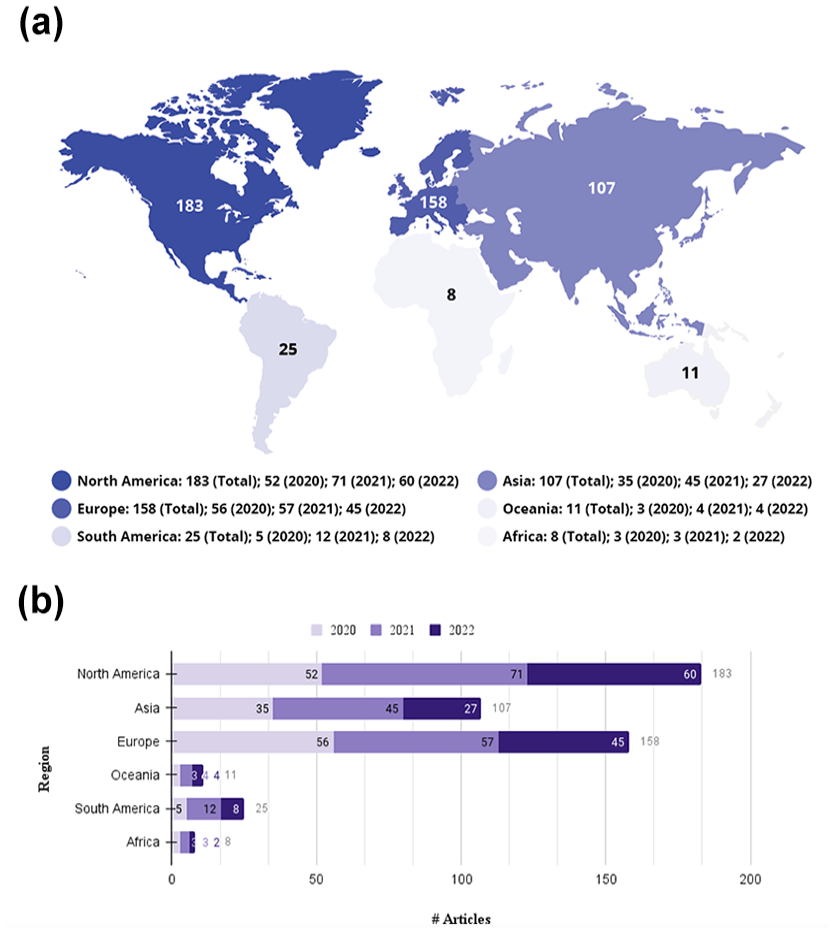
Number of articles per region in (a) global map illustration and (b) articles per region and per year.
Figure 4 shows the distribution of articles focused on COVID-19, diabetes, and technology categorized into the following groups: original, review, commentary, guideline, protocol, meeting summary, and case reports. The greatest number of original articles was published in July, August, and September of 2021. Europe, North America, and Asia published the highest number of original articles about this intersection of topics. The greatest number of commentary articles was published in July, August, and September of 2020. Except for the large number of commentaries published in the third quarter of 2020, the most common types of articles published about COVID-19, diabetes, and technology were original contributions. The number of original articles about COVID-19 and diabetes increased from 2020 to 2021 and slightly decreased in 2022. In each year, the majority of original articles were retrospective, followed by cross-sectional and prospective.
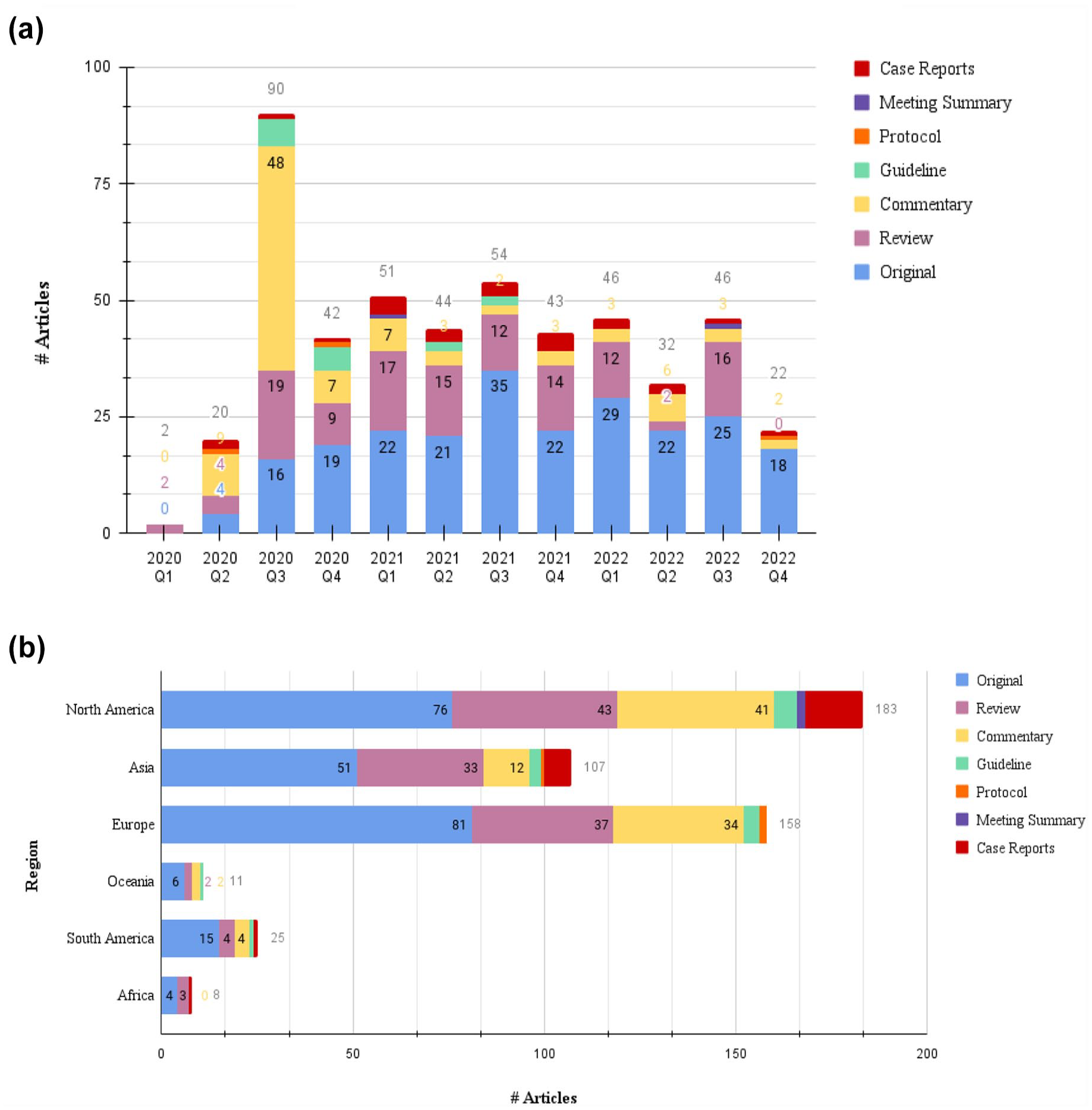
Types of articles per (a) types of articles over time and (b) types of articles per region.
Figure 5 shows the distribution of different types of technologies included in articles focused on diabetes and COVID-19. Several technologies were used by PWD during the COVID-19 pandemic as described in these articles (Figure 5), including electronic health records (1.4%), blood glucose monitors (3.5%), remote monitoring (1.7%), mobile apps and smartphones (3.6%), artificial pancreas/insulin infusion systems (3.8%), CGM (24.0%), and telemedicine (60.7%). Telemedicine was the most common technology discussed in these articles, which aligns with the trend of increasing telemedicine use by PWD during the COVID-19 pandemic. In a population of 8 339 633 PWD over a 3-month period, <1% of them received a telemedicine visit in 2019, whereas 27% of them received a telemedicine visit in 2020. 8 Both telemedicine and CGM were the most common reported technologies from articles around the world, except for Africa, with reports on telemedicine and mobile apps only.
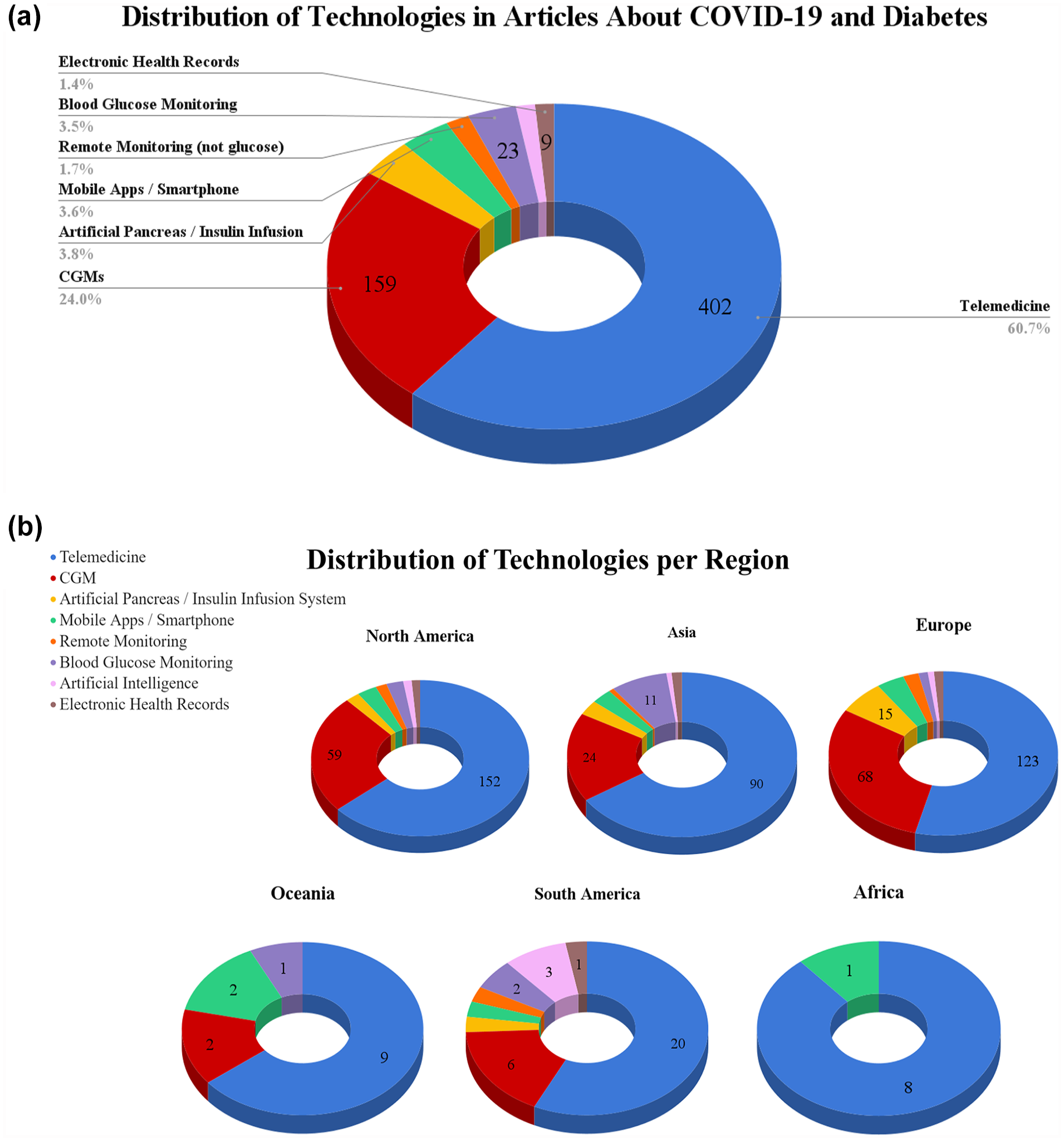
Distribution of articles about technologies: (a) overall and (b) per region.
Figure 6 provides an overall overview of articles published in PubMed, preprint publications (MedRxiv), and protocols published in clinicaltrials.org. The highest number of preprint articles was published in 2020, with a steady decline in 2021 and 2022 (Figure 6a). This indicates that preprint articles, without having gone through the peer review process, were made widely available at the start of the pandemic. While slowly declining, the number of preprint articles renamed was extremely high during the pandemic (1485 preprint articles about COVID-19 and diabetes in 2022) as compared to that before the pandemic (four preprint articles about COVID-19 and diabetes in 2019). The number of overall research publications (all articles including COVID-19 papers) in PubMed was the highest in 2021 (Figure 6b). The aforementioned PubMed search included articles about COVID-19, diabetes, and technology, whereas this PubMed search only included articles about COVID-19 or about both COVID-19 and diabetes. The number of research protocols related to COVID-19 was the highest in 2020 and declined in 2021 and 2022 (Figure 6c).
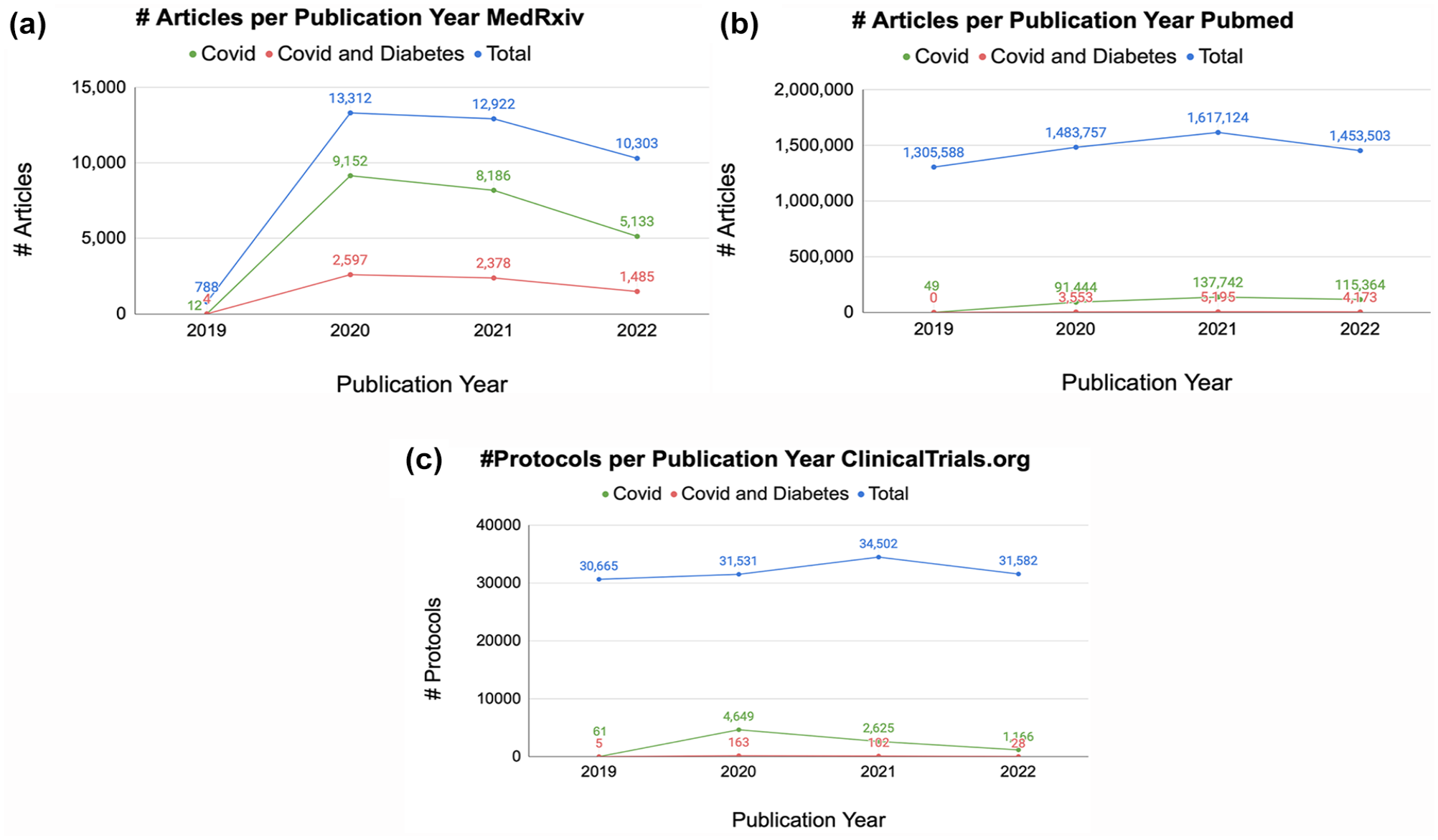
(a) Number of articles published on MedRxiv per publication year on COVID, COVID and diabetes, and the total number of articles. There was a significant increase in the number of articles published from 2019 to 2020. From 2020 to 2022, there is a downward trend in the three categories mentioned. (b) Number of articles published on PubMed per publication year on COVID, COVID and diabetes, and the total number of articles. In 2019, there were 0 articles published on COVID and diabetes. There was a significant increase in the number of articles published from 2019 to 2020. From 2020 to 2021, the number of articles held an upward trend in the three categories. From 2021 to 2022, the number of articles published decreased. (c) Number of protocols published on ClinicalTrials.org per publication year on COVID, COVID and Diabetes, and the total number of articles. There was a significant increase in the number of protocols published from 2019 to 2020 on COVID and COVID and Diabetes. From 2020 to 2021, the total number of protocols held an upward trend while the number of protocols on COVID and COVID and Diabetes decreased. From 2021 to 2022, the number of protocols published decreased for the three categories.
A total of 35 protocols adapting treatment protocols for patients with diabetes and COVID-19 were reviewed by the editorial team and posted on our website (COVIDinDiabetes.org). Protocols included adaptations focused on hyperglycemic crises (N = 7), steroid-induced hyperglycemia (N = 7), non-ICU diabetes care (N = 6), ICU diabetes care (N = 6), medical nutrition-induced hyperglycemia (N = 4), and inpatient CGM implementation (N = 5). There were 12 236 visits and 18 149 pageviews, with 1.6 actions (page views, downloads, outlinks, and internal site searches) per visit, with a maximum of 71 actions in one visit on our website. By continent, most visits came from North America (N = 7233, 54.2%), South America (N = 2663, 21.8%), and Europe (N = 1219, 10%). The least number of visits was from Africa (N = 198, 1.6%).
The highest number of visits occurred during the third quarter of 2020, remained stable during 2021, and steadily declined since March 2022, two years after the lockdown.
Resource Sharing: COVID-19 and Diabetes Information
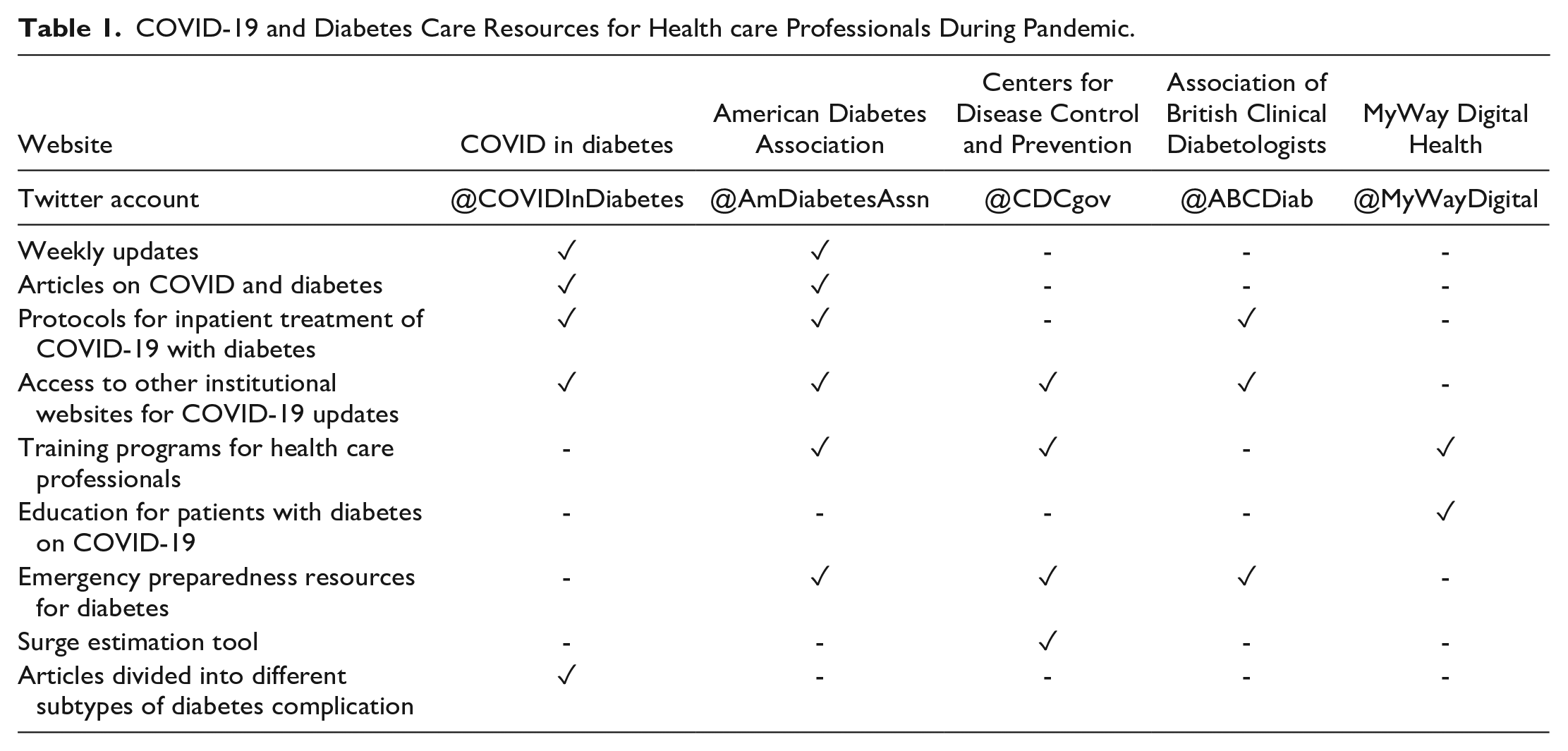
Table 1 provides an overview of resources offered by different platforms on information related to COVID-19 and diabetes, including resources from COVIDinDiabetes, the ADA Website, CDC, Association of British Clinical Diabetologists, and MyWay Digital Health. These websites were selected by two endocrinologist investigators for representing the four organizations with the best combination of professional reputation and popularity among the diabetes patient population. Common resources offered by these platforms included articles on COVID-19 and diabetes, protocols for diabetes management in patients with COVID-19, training programs for health care professionals, education resources for patients with diabetes and COVID-19, and emergency preparedness resources for diabetes.
COVID-19 and Diabetes Care Resources for Health care Professionals During Pandemic.
Discussion
The onset of the COVID-19 pandemic left several people with chronic and pre-existing conditions vulnerable, including PWD. 9 Clinicians, researchers, and PWD sought technologies that could reduce the burden of diabetes care during the pandemic, such as telehealth10-12 and CGM.13,14 Our systematic literature review in PubMed reveals that since 2019, 492 articles were published about COVID-19, diabetes, and technology. These articles were published steadily throughout 2020, 2021, and 2022 and in all regions of the world. North America, Europe, and Asia were the greatest producers of articles about diabetes technology and COVID-19. Many types of articles were written about this topic, including guidelines, protocols, and case reports, but original articles were the most common type of article. Within original articles, retrospective articles were the most common ones, and authors frequently compared an outcome of interest before and after the start of the pandemic. The rapid rise in telehealth use 15 during the pandemic was paralleled by the prominence of telehealth as a topic in the diabetes technology and COVID-19 literature. This PubMed literature search confirms that diabetes technologies were of great interest and utility for PWD all over the world during the COVID-19 pandemic.
The COVID-19 Infodemic and Misinformation
Much of the literature about COVID-19 and diabetes technology was produced at a time when there was rapid dissemination of information at the start of the pandemic. The COVID-19 pandemic has been called an infodemic by the World Health Organization, defined as a period of time when there is excessive availability of both information and misinformation during a disease outbreak. 16 The pandemic was similarly described by authors in several other countries, including China, 17 Africa, 18 South Korea, 19 and Ireland. 20 The high media-dependency for rapid dissemination of current data and research on COVID-19 information that emerged during the pandemic only exacerbated the infodemic, 21 as people were hoping to learn from quick information sources in a rush to obtain substantive data and research about COVID-19. Traditional mass media, such as television, newspapers, and websites, provided an abundance of pandemic-related information, and many people relied on the news for reliable information, especially if they were of the low-income category. 21 Online platforms, such as social media and online forums, provided a new and important information source for many laypeople. 21 However, without accuracy checks against current journalistic standards or medical evidence, social media became a hotspot for misinformation. Much of the information and misinformation disseminated on social media platforms came from laypeople and not medical and scientific experts. 21 Social bots, automated social media accounts, also diluted the amount of accurate medical information online by purposely spreading misinformation. 22 Such examples of pervasive false claims included the recommendation of bleach, cocaine, and hydroxychloroquine as COVID-19 treatments, as well as the idea that 5G wireless technology initiated the COVID-19 pandemic, both of which have serious dangerous consequences. 22 The use of social media platforms, including Facebook and Instagram, thus led to widespread beliefs in various conspiracy theories and a decrease in compliance behavior. 21 Distrust in public health officials and noncompliant behaviors due to misinformation serve as major barriers to a successful and timely public health response, at the potential expense of thousands.
Rapid Publication Adding to Misinformation Online
There was a large effort from the research community to disseminate accurate information about COVID-19 to the global community quickly. From February 2020 to January 2022, an average of 137 scientific articles about COVID-19 were published per day in PubMed. 23 Top journals received a record number of articles; for example, the New England Journal of Medicine reported receiving up to 40 COVID-19-related publications per day, and the editor of the Journal of American Medical Association reported receiving up to 235 COVID-19-related articles or submissions per day. 24 The thoroughness of the peer review process put an immense strain on reviewers for a quick turnaround. In addition, many journal reviewers noted the drop-off in quality of the submitted articles. For example, the editorial team at Science said that many submissions were clearly rushed and did not meet their standards for publication and dissemination. 24 As a result of the decreased quality, the ratio of retracted articles to accepted articles was much greater for COVID-19-related articles than for any other research topic. This is a problem because many of these articles continue to be shared after retraction. 23 For example, platforms such as Twitter and news outlets may continue to share retracted articles, which have tangible impacts on clinical decision-making and public health guidelines. 25
To publish their information quickly, many researchers turned to preprint servers, websites that allow readers to access articles that are not yet peer-reviewed, such as SSRN and MedRxiv.24,26 Researchers used preprint servers to circumvent the lengthy review process and meet the need for knowledge about COVID-19, and this resulted in unreviewed articles initially outnumbering those published in conventional biomedical journals. 26 One study found that, in the first four months of 2020, the average time for a preprint to become a published article was just 63 days. 27 Looking at one preprint server, 1784 manuscripts about COVID-19 were posted to MedRxiv from the beginning of the pandemic to April 27, 2020. 24 MedRxiv posts a notice on the top page of all preprints: “Caution: Preprints are preliminary reports of work that have not been certified by peer review. They should not be relied on to guide clinical practice or health-related behavior and should not be reported in news media as established information.” 27 Thus, creators of MedRxiv themselves understand the risks in relying on preprints for decision-making. While the articles posted to MedRxiv are distinctly noted to have not yet been reviewed, it is important to recognize that manuscripts on MedRxiv, and mistakes made in these articles before going through the revision process, remain a part of the COVID-19 literature and narrative during future searches. 24 It is especially concerning because retraction of preprints from the published public record is often silent, without the provision of any transparent explanation. 27 Confusion can arise, especially in laypeople who may not understand the difference between a preprint and peer-reviewed manuscript. While useful, preprint servers should also make clear their limitations, taking care to not promulgate unreviewed conclusions. 26 Overall, it is important that, while researchers aim to disseminate information quickly during an international emergency, the scientific community does not contribute to this misinformation.
COVID-19 Information on Websites
Unlike with reputable peer-reviewed journals, there is no system in place to verify the information posted online on websites. 28 Because the general population heavily relies on the Internet to obtain information quickly, it is essential that health-related information found online during a pandemic is accurate and accessible. 29 In a review article, Stern and colleagues 28 reported that the articles found online one year after the confirmed COVID-19 outbreak were riddled with misinformation. Many websites and videos about COVID-19 were of poor quality and needed improvements, and none of the websites or videos met their metric of being good or of excellent quality. 28 Four reports in their review found that ≥28% of websites about COVID-19 contained inaccurate information, including hoaxes. In addition, the readability exceeded recommended levels, 28 making those with lower eHealth literacy more vulnerable to misinformation. Unsurprisingly, sources with a high prevalence of inaccuracies were published by independent users and consumers, whereas sources with a low prevalence of inaccuracies were published by the government, health care organizations, and news sources. 28 This is important to note because laypeople with low self-efficacy in their ability to distinguish between low- and high-quality health information are especially vulnerable to COVID-19 misinformation.
COVIDinDiabetes.org
In response to the misinformation characterizing COVID-19, an international consortium of researchers and clinicians, including authors of this article, created a new, community-centered, and collaborative website containing COVID-19 and diabetes information called COVID In Diabetes. This term stands for the Collaborative Open-Access Virtual Database for COVID-19 In Diabetes and can be accessed at COVIDinDiabetes.org.
Inspired by the early Italian experience of COVID-19 summarized by Nacoti and colleagues, 30 we aimed to respond to the glycemic care needs of PWD with a community-centered perspective focused initially on providing a platform to share protocols to facilitate the care of PWD. In addition to continuing patient-centered care, the pandemic highlighted the importance of other public health practices including mindfulness regarding the use of personal protective equipment, efforts to reduce the risk of infection for health care workers, and minimization of community disease spread.
This website was formed by the Emory University School of Medicine in collaboration with the Diabetes Technology Society along with clinicians, scientists, and researchers from multiple institutions, which fostered collaboration worldwide. This collaborative worked to minimize dissemination of misinformation by assigning team members to carefully select articles to include on the COVIDinDiabetes.org website, on the basis of the information being scientifically sound and accurate. COVIDinDiabetes.org has provided weekly updates, articles on COVID-19 and diabetes, protocols for inpatient treatment of COVID-19 in PWD, and access to other institutional websites for COVID-19 updates. With the creation of this website, our team has taken a step to ensure that the scientific community increases the probability of interfacing with high-quality scientific information online.
In conclusion, the COVID-19 pandemic severely impacted all aspects of life including the way we practice medical care. The transition to the use of technology resources has been evident during this period. There is a clear disparity in research resources and productivity globally, which likely reflects access to these technologies during global disasters. Further efforts are needed to share resources with one another to foster equity in knowledge and quality of care. The COVIDinDiabetes.org website has been one such initiative to promote resource sharing. The COVID-19 pandemic has demonstrated the need for countries around the world to quickly mobilize resources, offer clear directives, and spread accurate information. Learning from the COVID-19 pandemic and building efficient solutions will ensure that we can properly take action and share information during inevitable future international crises.
Footnotes
Acknowledgements
We would like to thank the contributors to our website including: Alyson Myers, MD (USA); Daniel Rubin, MD, MS (USA); Darin Olson, MD, PhD (USA); David Lam, MD (USA); Deborah Wake, MBChB, BSc, PhD, Clin Ed Dip (UK); Emilia Gómez Hoyos, PhD (Spain); Faisal A. Aljehani, MBBS (USA); Fernando Gomez-Peralta, MD, PhD (Spain); Gerry Rayman, MD, FRCP (UK); Guillermo E. Umpierrez, MD, CDE (USA); Javier Carrasco, MD, PhD (Spain); Jose Luis Paz-Ibarra, MD (Peru); Katalina Funke, MD (USA); Kathie L. Hermayer, MD, MS (USA); Kathleen Dungan, MD, MPH (USA); Ketan Dhatariya, MBBS, MSc, PhD (UK); Lillian F. Lien, MD (USA); Marcos Tadashi K. Toyoshima, MD (Brazil); Maya Fayfman, MD (USA); Marie McDonnell, MD (USA); Miguel Pasquel, MD (Ecuador); Mihail Zilbermint, MD, FACE (USA); Mohammed Al-Sofiani, MD, MSc (Saudi Arabia); Nadine E. Palermo, DO (USA); Omar G. Mustafa, MBChB, MRCP (UK); Paul Szumita, PharmD (USA); Priyathama Vellanki, MD (USA); Ricardo Gomez-Huelgas, MD (Spain); Rodolfo J. Galindo, MD, FACE (USA); Shivani Agarwal, MD, MPH (USA); Silvio E. Inzucchi, MD (USA). We also thank our website developer Javier Szyszlican.
Abbreviations
ADA, American Diabetes Association; CDC, Centers for Disease Control and Prevention; CGM, continuous glucose monitoring; PWD, people with diabetes.
Author Contributions
AMY, DCK, and FJP conceptualized the study and wrote the first draft. AMY, JH, AA, and GMB conducted the data extraction for the systematic review. SD carried out the resource search. AMY, JH, AA, GMB, MAU, JDB, KTN, NYX, TS, JYZ, reviewed the literature for the COVIDindiabetes.org webstite. DCK, GD, and FJP supervised the website development and content.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DCK is a consultant to Better Therapeutics, EOFlow, Integrity, Lifecare, Nevro, Novo Nordisk, Sanofi, and Thirdwayv. GMD has received research support from Insulet Corp. and consulting fees from Medscape. FJP has received unrestricted research support (to Emory University) from Insulet, Ideal Medical Technologies, Dexcom, Novo Nordisk, and Tandem Diabetes Care and consulting fees from Dexcom and Medscape. All other authors have nothing relevant to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This effort was partially supported by NIDDK of the NIH under the award number P30DK111024, Georgia Diabetes Translation Research Center (GDTRC) project “The Preparedness Cycle in the Care of People with Diabetes During the COVID-19 Pandemic and Future Outbreaks”.