
Abstract

Keywords
Pregnancy-specific intravenous insulin infusion (IVI) algorithms are recommended to improve glycemic control during antenatal corticosteroids, illness, or labor, and may reduce neonatal hypoglycemia.1 -3 Frequent capillary-glucose testing during intensive IVI therapy can be disruptive to women and time-consuming for ward-staff. Although the supplementary use of continuous glucose monitoring (CGM) for pregnant inpatients with type 1 diabetes mellitus (T1DM) has recently been acknowledged, to our knowledge, there are no data on the accuracy of CGM in this setting. 1
We conducted a retrospective observational study to assess accuracy of CGM worn by hospitalized pregnant women with T1DM in the third trimester of pregnancy who required hourly capillary-glucose monitoring due to glucose instability or IVI therapy. Eleven episodes of care were analyzed over an eight-month period (intercurrent illness = 2, betamethasone = 1, intrapartum = 8), using Dexcom G5 Mobile CGM System (n = 9) or Medtronic Guardian Carelink (n = 2). Median gestation at time of evaluation was 37 weeks. The accuracy of CGM glucose was compared with nearest time point capillary glucose (Freestyle Optium Neo H) taken at 30 to 60 minutely intervals (n = 255 non-calibration points) using recognized metrics. 4 The study received prospective ethical approval.
Overall mean absolute relative difference (MARD) between CGM and capillary glucose was 11.4% (SD = 11.6; n = 255), with a MARD of <10% deemed suitable for non-adjunctive dosing of insulin. MARD was 9.98 (SD = 9.26) when capillary-glucose levels were 68 to 180 mg/dL (3.8-10.0 mmol/L; n = 236), indicating good accuracy of CGM when glucose is within this range. When capillary-glucose values were <68 mg/dL (<3.8 mmol/L; n = 9), MARD was 35.75 (SD = 21.77) and when glucose values were >180 mg/dL (>10.0 mmol/L; n = 10), MARD was 23.70 (SD = 18.86). Pearson’s correlation coefficient was 0.8 (P < .001; Figure 1a). Bland-Altman analysis demonstrated negative bias of −0.22 mmol/L, indicating slightly lower CGM values compared with capillary glucose (Figure 1b). Clarke Error Grid Analysis (classifying risk based on level and direction of discrepancy between CGM and capillary glucose) identified 97% of values within “safe” areas (Figure 1c). 5 Of concern, during nine episodes of capillary-glucose hypoglycemia (<3.8 mmol/L), CGM detected hypoglycemia correctly only four times and incorrectly identified hypoglycemia on six occasions. On a per-episode basis, MARD varied considerably (1.1%-38.2%; median = 12.2, interquartile range [IQR] = 7.2-13.0; Figure 1d) with increasing variability of capillary glucose correlating with larger discrepancy between CGM and capillary glucose (Spearman rank correlation 0.7, P = .019). Glucose variability was lower in the eight birth episodes.
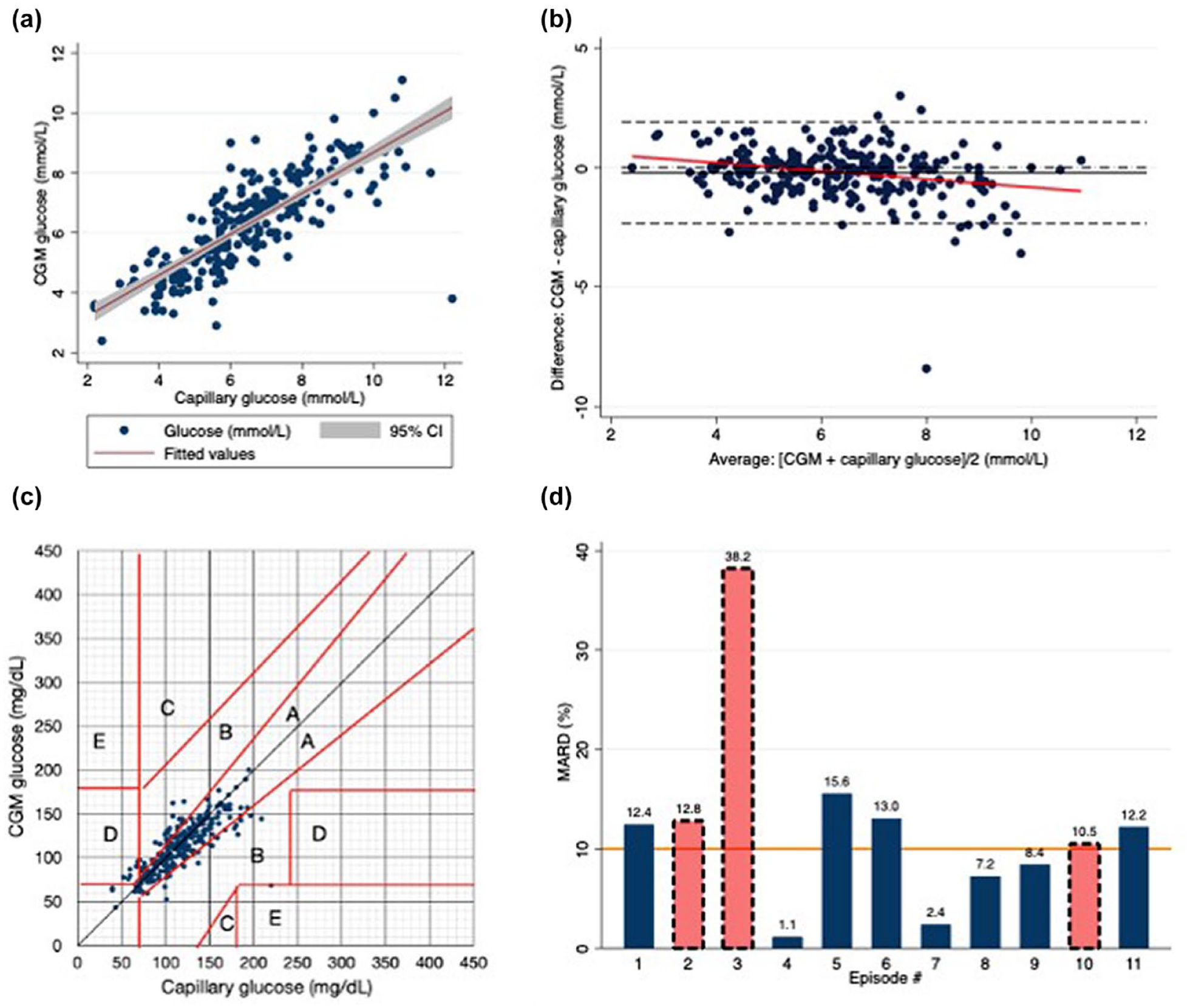
(a) Scatter plot CGM versus capillary glucose (mmol/L). Pearson’s coefficient 0.8 (P = .001; n = 255). (b) Bland Altman Plot (mmol/L). Mean bias −0.22 mmol/L, 95% limits of agreement 2.33 (lower) to 1.89 mmol/L (higher). (c) Clarke Error Grid Analysis CGM versus capillary glucose (mg/dL): A = within 20% of capillary glucose; B = >20% but not lead to inappropriate treatment; C = unnecessary treatment; D = failure to detect hypo/hyperglycaemia; E = erroneous treatment for non-pregnancy target glucose. (d) MARD (%) of each episode. Solid bars represent birth episode. Dashed-outline bars represent reason other than birth. MARD 10% marked by line, below which insulin can feasibly be dosed based on CGM glucose. Abbreviations: CGM, continuous glucose monitoring; MARD, mean absolute relative difference; CI, confidence interval.
This pilot study demonstrates potentially clinically useful correlation between capillary glucose and CGM in pregnant women with T1DM in late pregnancy in the inpatient setting. As expected, CGM is more accurate during periods of low glycemic variability and when glucose is within a range of 68 to 180 mg/dL. CGM could be explored as a non-supplementary measure of glucose during these periods to reduce the burden of capillary-glucose testing. However, capillary blood glucose level should remain standard of care in settings of high glycemic variability. The directional trend of the CGM trace may be useful in detecting impending hyperglycemia or hypoglycemia. Further prospective trials to assess CGM accuracy in pregnant inpatients are recommended.
Footnotes
Abbreviations
CGM, continuous glucose monitoring; IVI, intravenous insulin infusion; MARD, mean absolute relative difference; T1DM, type 1 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.