
Abstract
Background:
The majority of youth with type 1 diabetes (T1D) fail to meet glycemic targets despite increasing continuous glucose monitoring (CGM) use. We therefore aimed to determine the proportion of caregivers who review recent glycemic trends (“retrospective review”) and make ensuant insulin adjustments based on this data (“retroactive insulin adjustments”). We additionally considered that fear of hypoglycemia and frequency of severe hypoglycemia would be associated with performing retrospective review.
Methods:
We conducted a cross-sectional survey of caregivers of youth with T1D, collecting demographics, diabetes technology usage, patterns of glucose data review/insulin dose self-adjustment, and Hypoglycemia Fear Survey (HFS).
Results:
Nineteen percent of eligible caregivers (191/1003) responded. Performing retrospective review was associated with younger child age (12.2 versus 15.4, P = .0001) and CGM use (92% versus 73%, P = .004), but was not associated with a significant improvement in child’s HbA1c (7.89 versus 8.04, P = .65). Retrospective reviewers had significantly higher HFS-behavior scores (31.9 versus 27.7, P = .0002), which remained significantly higher when adjusted for child’s age and CGM use (P = .005). Linear regression identified a significant negative association between HbA1c (%) and number of retroactive insulin adjustments (0.24 percent lower mean HbA1c per additional adjustment made, P = .02).
Conclusions:
Retrospective glucose data review is associated with improved HbA1c when coupled with data-driven retroactive insulin adjustments. Barriers to data downloading existed even in this cohort of predominantly CGM-using T1D families.
Keywords
Introduction
The Diabetes Control and Complications Trial (DCCT) demonstrated that intensive insulin therapy alongside frequent insulin dose titration in type 1 diabetes (T1D) was effective at reducing hemoglobin A1c (HbA1c) and long-term diabetes complications. 1 Significant advancements in diabetes technology, including continuous glucose monitors (CGM), have been integrated into routine clinical practice since those results were published in efforts to improve glycemic control.2-6 Consistent technology use has been shown to lower HbA1c and reduce episodes of severe hypoglycemia.7-9 However, data from the T1D Exchange illustrate that despite a significant uptake in pediatric CGM use, glycemic control in youth remains woefully suboptimal. 8 Current pediatric care standards recommend clinical diabetes visits occur quarterly, 10 necessitating regular data-driven insulin dose adjustment occur between visits in order to achieve optimal glycemic control. Worsening glycemic control in the face of improved utilization of technology may in part be due to lack of caregiver-initiated retrospective data review and subsequent data-driven retroactive insulin adjustments.11,12
In this cross-sectional study, we conducted an electronic-based survey examining patient and caregiver demographics, diabetes technology use, patterns of diabetes management (i.e. self-reported CGM and insulin pump use, self-reported data review/changes to insulin regimen), and the Hypoglycemia Fear Survey (HFS).13,14 The primary aim of this study was to further describe the relationship between caregiver-initiated retrospective data review, caregiver-initiated retroactive insulin adjustment, fear of hypoglycemia, and glycemic control. Retrospective data reviewers encapsulates caregivers who review recent glycemic trends (“retrospective review”) with the intent to make insulin adjustments (“retroactive insulin adjustments”). A secondary aim was to evaluate barriers to downloading diabetes data for retrospective review. We hypothesized that better glycemic control as measured by HbA1c would be associated with retrospective data review and subsequent retroactive insulin adjustments based on review of the historical data. We hypothesized that the frequency of retrospective data review would also be associated with fear of hypoglycemia.
Methods
Participant Characteristics
The protocol was approved by the Institutional Review Board. Inclusion criteria included having a pediatric patient (defined as patients ≤ 22 years of age) with T1D who received care in the University of Iowa Stead Family Children’s Hospital within the preceding 2 years. All caregivers were required to have an understanding of written English. We identified 1003 eligible patients. A list of pediatric patients meeting those criteria was ascertained utilizing TriNetX (https://www.trinetx.com), a global health research network. The University of Iowa Healthcare informatics team further filtered the data by date of last pediatric diabetes clinic visit. The data were ultimately coded and de-identified based on standards defined in Section 164.14(a) of the HIPAA Privacy Rule. The coding system enabled linkage of de-identified individuals back to a previously coded but otherwise de-identified data set that allowed for confirmation of responder status and validation of reported demographic information and clinic point-of-care HbA1c.
Study data were collected and managed using REDCap (Research Electronic Data Capture).15,16 REDCap is a secure, web-based software platform designed to support data capture for research by providing an interface for validated data capture, audit trails for tracking data manipulation and export procedures, and automated export to statistical packages. Automated reminders were sent weekly for 3 weeks. Caregivers without a valid email address were contacted in person at their child’s next clinic appointment and had the opportunity to complete the survey on a tablet, which was subsequently coded and de-identified.
Measurements
The survey collected information from caregivers regarding patient demographics and included the Institute of Medicine’s Social and Behavioral Determinants of Health, HFS, diabetes management behaviors, and information about participants’ ability to review blood glucose and/or insulin pump data.13,17,18 The HFS is a validated instrument for quantifying fear of hypoglycemia in diabetes and was modified for parents of children with diabetes.19,20 It contains two subscales, the 10-item HFS-behavior subscale and the 15-item HFS-Worry subscale. Higher scores suggest greater fear of hypoglycemia.
Diabetes management behaviors encompassed questions related to device use, data downloading platforms, downloading frequency, and types of insulin adjustments made. Retroactive insulin adjustments were considered any dose adjustment made in response to a recent historical pattern of data (including increasing or decreasing long-acting or basal insulin, increasing or decreasing meal doses). One-time insulin adjustments included any dose adjustment made by the caregiver in response to current or expected blood glucose data (including the use of temporary basal rates, manual pump suspensions, or decreasing insulin doses due to anticipated activity). See Supplement 1 for the complete diabetes data review survey questions.
Clinic point-of-care HbA1c values were available for 100% of responders and 99.8% of non-responders and were measured via the Afinion AS100 (Abbott Diabetes Care, Alameda, California).
Statistical Analysis
Statistical analyses were performed using SAS V9 and SAS/STAT 15.2, and graphs were created with GraphPrism version 9.0.1 (GraphPad Software, San Diego, California, www.graphpad.com). Student’s t-test was used to assess for significant differences between means of normally distributed data. Wilcoxon rank-sum test was used to assess for significant differences between non-normally distributed data. Pearson chi-square test was used to compare categorical data. Multivariable linear regression models were used to examine the association between HbA1c and the number of retroactive insulin adjustments and one-time insulin adjustments made, adjusted for the child’s age and CGM use. P-values presented in the text are unadjusted; however, p-values were adjusted using the Benjamini-Hochberg algorithm for multiple comparisons to control the false discovery rate at 0.05 and did not impact the significance of any analyses. These are reported in the subsequent tables for clarity. All P-values are 2-tailed.
Results
Participant Characteristics
Nineteen percent (191/1003) of eligible caregivers responded to the survey. Median self-reported HbA1c for patients whose caregiver responded to the survey (responders) was 7.5% and did not differ significantly from the last documented clinic point-of-care HbA1c for that group (7.4%), P = .32. Median last clinic point-of-care HbA1c was significantly lower in the responders group (7.4%) compared to those whose caregiver did not respond to the survey (non-responders) (8.0%), P < .0001. Median child age of responders was 14 years, which was significantly younger than non-responders (16 years), P < .0001. A significantly higher percentage of responders had commercial insurance (78.5%) as compared to non-responders (63.5%), P < .0001. There was no significant difference in gender between groups, P = .97. Table 1 contains demographic data of responders compared to non-responders.
Demographic Information Comparing Survey Responders to Non-Responders.
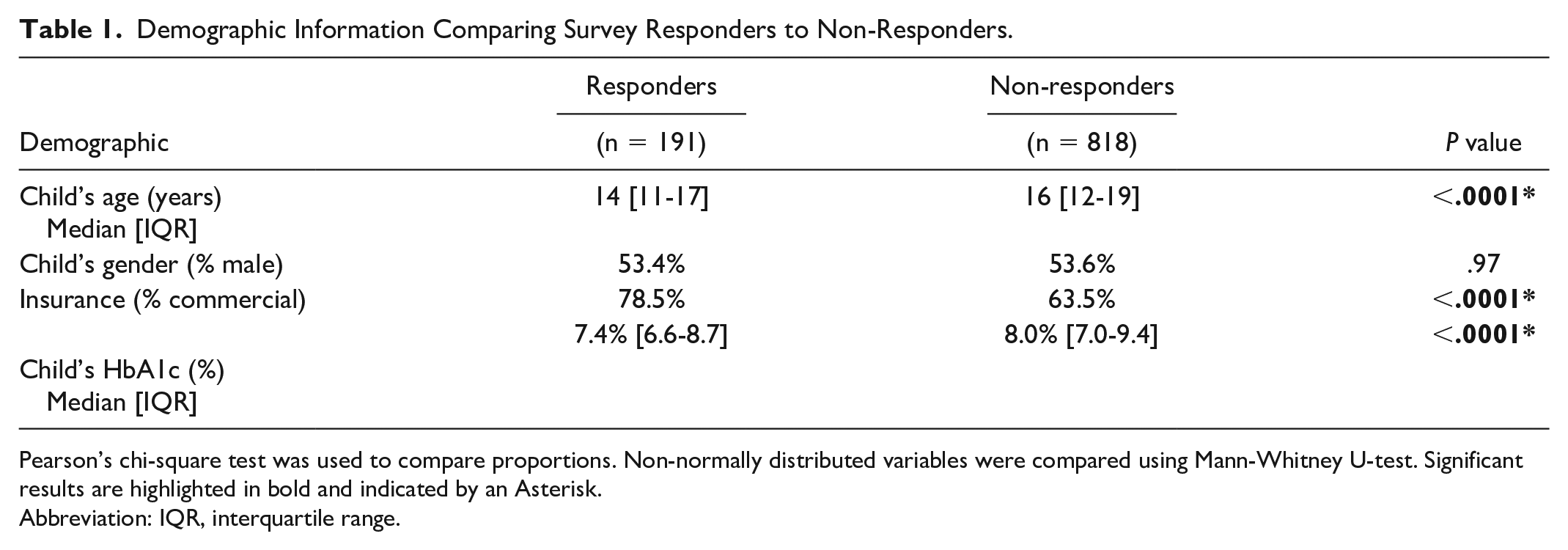
Pearson’s chi-square test was used to compare proportions. Non-normally distributed variables were compared using Mann-Whitney U-test. Significant results are highlighted in bold and indicated by an Asterisk.
Abbreviation: IQR, interquartile range.
There were 116 caregivers (76%) who indicated that they review their child’s historical blood glucose data with the intent of considering insulin dose changes; these caregivers will subsequently be referred to as retrospective reviewers. CGM use was significantly associated with retrospective review (92% of retrospective reviewers used CGM versus 73% of non-reviewers, P = .004). Younger median age of child was also associated with retrospective review (12.2 versus 15.4, P = .0001). Retrospective review groups did not differ in the percentage of participants whose providers discussed the importance of regular data download or retrospective review (55% versus 56% strongly agreed or agreed, P = .68). The remainder of demographic and clinical characteristics were not statistically different between retrospective reviewers and non-reviewers and are summarized in Table 2.
Demographic and Clinical Characteristics by Whether Child’s Diabetes Data was Reviewed in Between Clinic Visits with the Intent to Make Insulin Dose Adjustments.
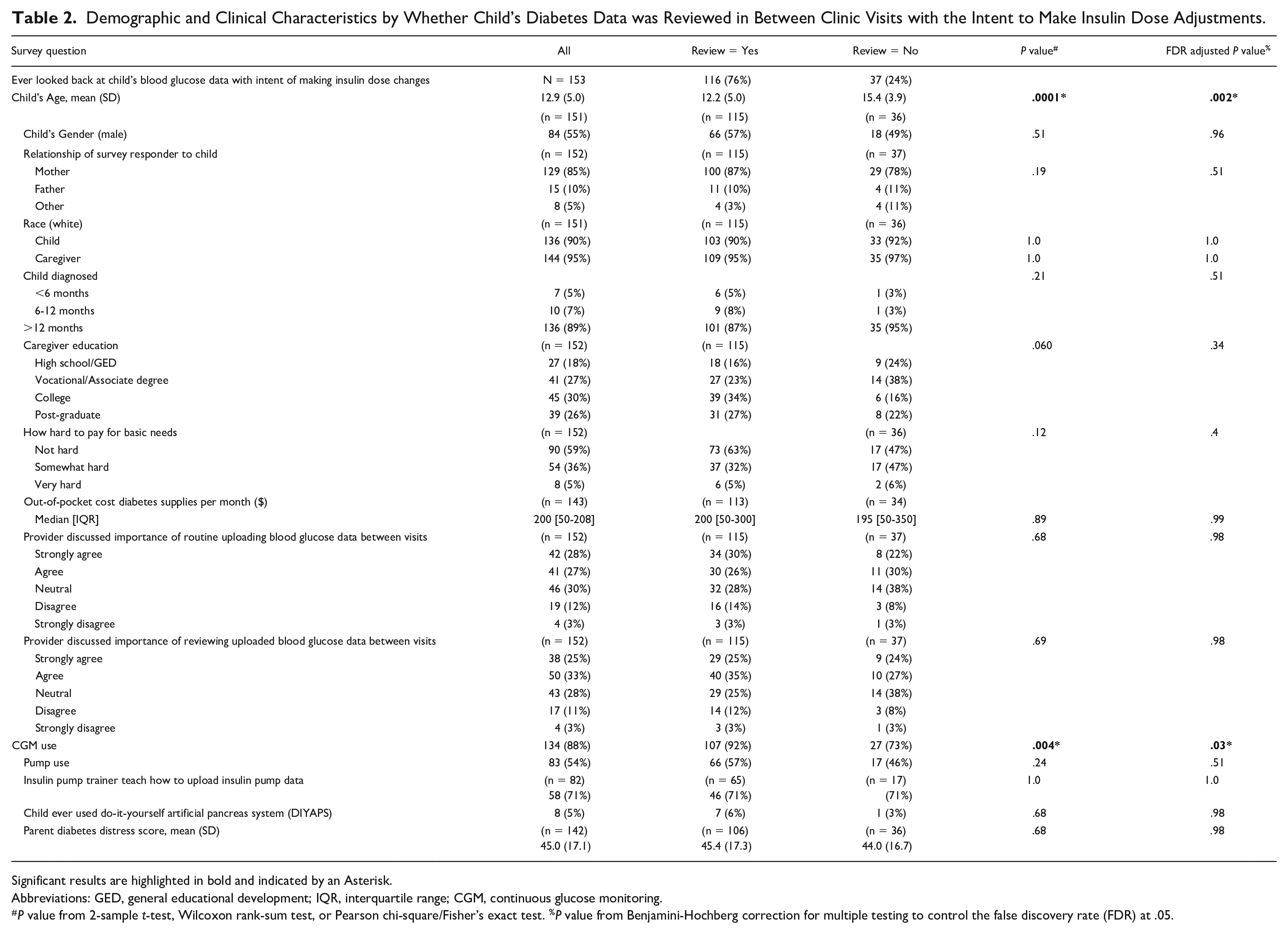
Significant results are highlighted in bold and indicated by an Asterisk.
Abbreviations: GED, general educational development; IQR, interquartile range; CGM, continuous glucose monitoring.
P value from 2-sample t-test, Wilcoxon rank-sum test, or Pearson chi-square/Fisher’s exact test. %P value from Benjamini-Hochberg correction for multiple testing to control the false discovery rate (FDR) at .05.
Retrospective reviewers were further divided for sub-group analysis. Regular retrospective reviewers (43 individuals) were defined by caregivers who indicated they review the data daily, weekly, or monthly. In all, 70 individuals were classified as “as needed” retrospective reviewers. Three individuals did not answer this question and could not be classified. No further clarification was provided by any responders into how they determined when data review was needed.
Diabetes Outcomes and Data Review
There was no difference in child’s mean HbA1c when comparing retrospective reviewers versus non-reviewers (7.89% versus 8.04%, P = .65) (Tables 3 and 4). There was also no difference in child’s HbA1c when adjusting for child’s age and CGM use (P = .98).
Association of Diabetes Outcomes with Whether Child’s Diabetes Data was Reviewed in Between Clinic Visits with Intent of Making Insulin Dose Changes.
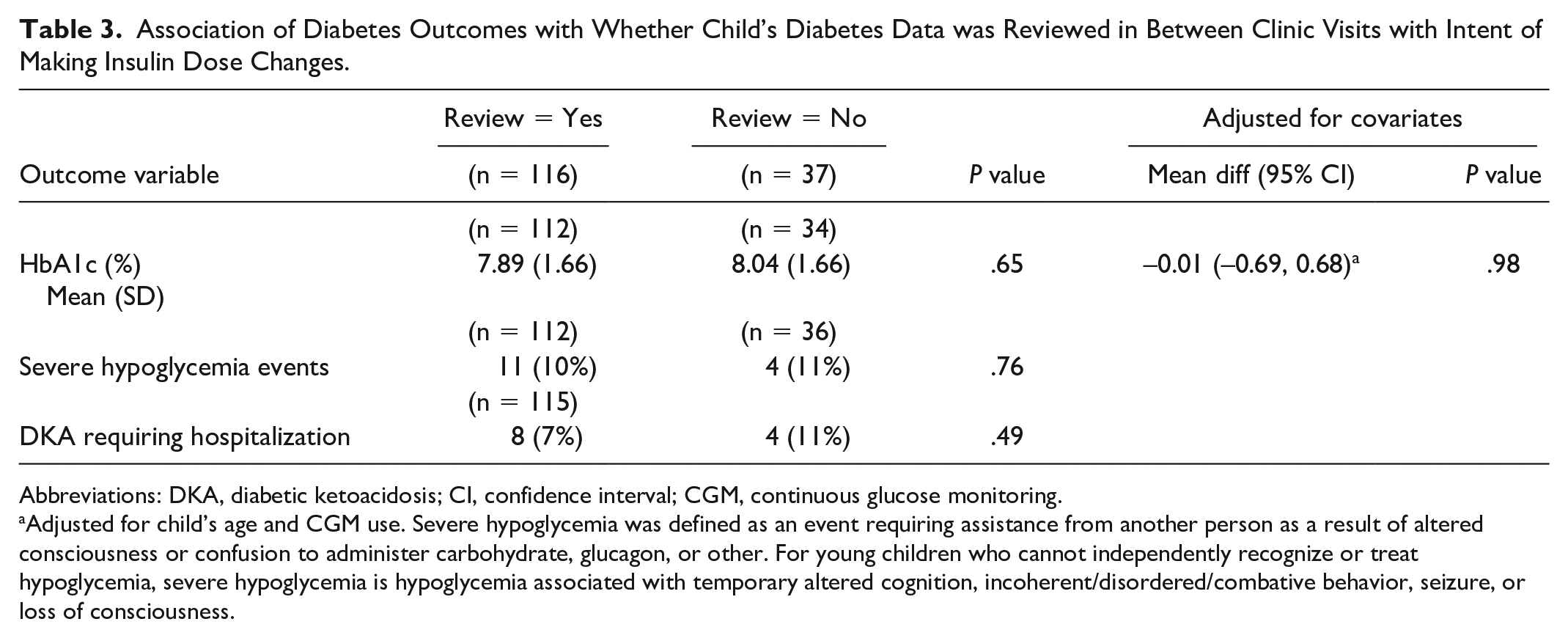
Abbreviations: DKA, diabetic ketoacidosis; CI, confidence interval; CGM, continuous glucose monitoring.
Adjusted for child’s age and CGM use. Severe hypoglycemia was defined as an event requiring assistance from another person as a result of altered consciousness or confusion to administer carbohydrate, glucagon, or other. For young children who cannot independently recognize or treat hypoglycemia, severe hypoglycemia is hypoglycemia associated with temporary altered cognition, incoherent/disordered/combative behavior, seizure, or loss of consciousness.
Association of Diabetes Outcomes with Frequency of Review of Child’s Diabetes Data in Between Clinic Visits with Intent of Making Insulin Doses Changes.
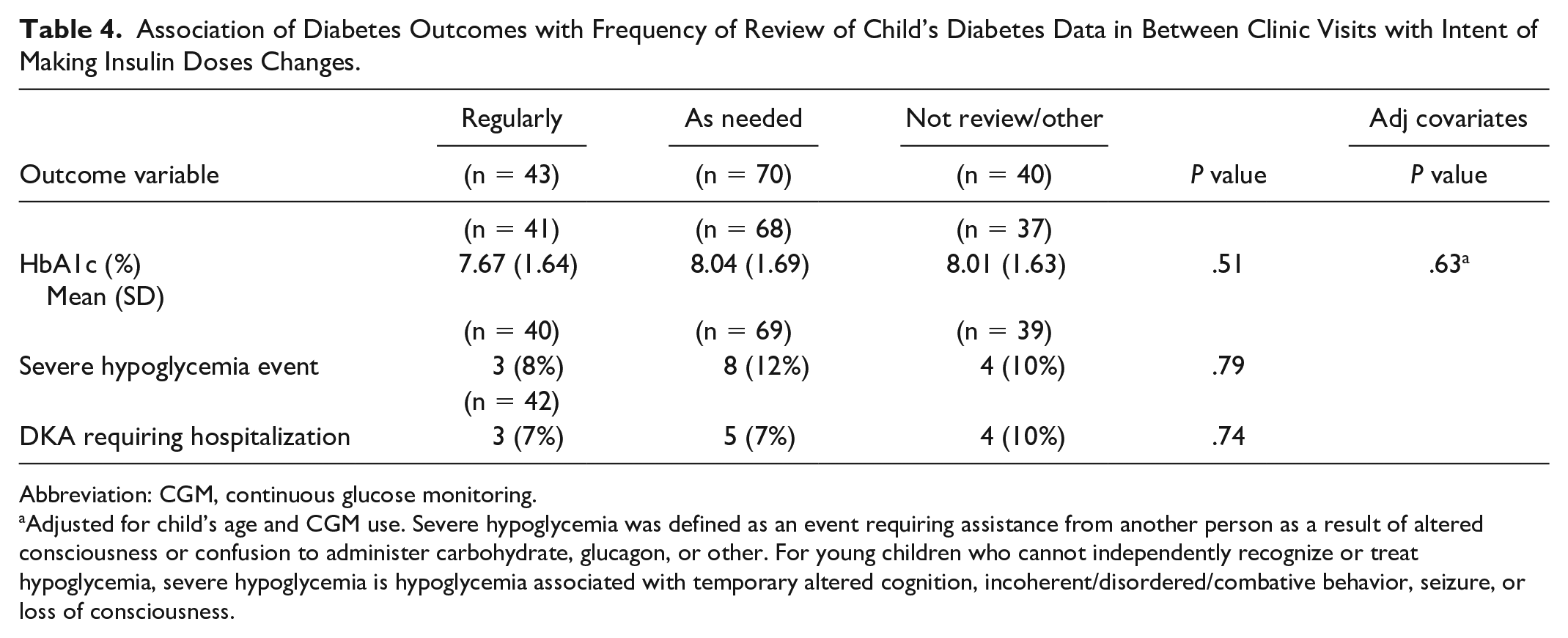
Abbreviation: CGM, continuous glucose monitoring.
Adjusted for child’s age and CGM use. Severe hypoglycemia was defined as an event requiring assistance from another person as a result of altered consciousness or confusion to administer carbohydrate, glucagon, or other. For young children who cannot independently recognize or treat hypoglycemia, severe hypoglycemia is hypoglycemia associated with temporary altered cognition, incoherent/disordered/combative behavior, seizure, or loss of consciousness.
There were no differences in child’s HbA1c among regular retrospective reviewers, as needed retrospective reviewers, and non-reviewers (7.67% versus 8.04% versus 8.01%, P = .51), with again no statistically significant differences noted when HbA1c was adjusted for child’s age and CGM use (P = .63). Additionally, there were no differences in the number of episodes of self-reported severe hypoglycemia events or episodes of DKA requiring hospitalization between groups.
Retrospective Data Review and Fear of Hypoglycemia
Retrospective reviewers had significantly higher HFS-behavior (31.9 versus 27.7, P = .0002) and HFS-total scores (66.3 versus 58.4, P = .015) (Table 5). Higher HFS-behaviors scores in retrospective data reviewers persisted when adjusted for child’s age and CGM use (P = .005). There was no significant association of HFS behavior, worry, or total scores with CGM use. HFS-behavior scores showed weak but significant negative associations with child’s age (Pearson’s R =-0.28, P = .0006).
Association of Caregiver’s Fear of Hypoglycemia with Whether Child’s Diabetes Data was Reviewed in Between Clinic Visits with Intent of Making Insulin Dose Changes.
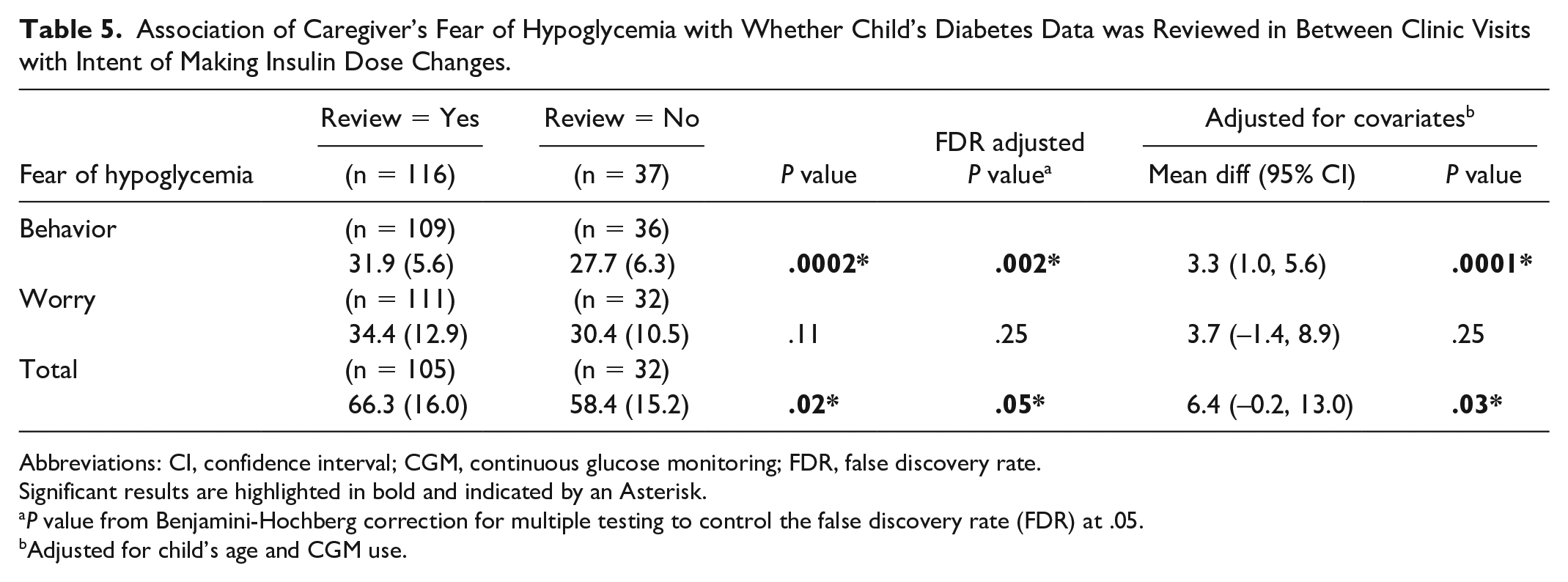
Abbreviations: CI, confidence interval; CGM, continuous glucose monitoring; FDR, false discovery rate.
Significant results are highlighted in bold and indicated by an Asterisk.
P value from Benjamini-Hochberg correction for multiple testing to control the false discovery rate (FDR) at .05.
Adjusted for child’s age and CGM use.
Retrospective Insulin Adjustment
Among retrospective reviewers, there was a significant association between the child’s HbA1c (%) and number of retroactive insulin adjustments made, with a 0.24% lower mean HbA1c per additional adjustment made (95% CI: -0.035, -0.439; P = .02). Including child’s age and CGM use as covariates in the regression model showed very similar results, with adjusted slope corresponding to a 0.231% lower mean HbA1c per adjustment made (95% CI: -0.025, -0.436; P = .03). Among retrospective data reviewers, the data suggested a possible association between number of one-time adjustments and HbA1c but was not significant at the 0.05 significance level (95% CI: -0.019, 0.318; P = .08).
Barriers to data download
Barriers to home download of diabetes data were assessed in the context of telehealth transition. Seventy-two caregivers (38% of responders) indicated that their child had a diabetes telehealth visit between March 18, 2020 and June 24, 2020. Twelve percent did not download data for the visit. The majority of individuals who downloaded data utilized the Dexcom Clarity platform (42, 59%). Only 5 (11%) of those using Dexcom Clarity were not already remotely sharing data with our clinic prior to the telehealth visit. The majority (78%) of those who did not download data indicated that they were unable. One individual had no computer and no internet. Three individuals were missing the cable required to download. One indicated the directions were too complicated. Three selected “other reasons” but did not elaborate. Nine successful data downloaders indicated via free-text that they had difficulties downloading due to operating system incompatibilities (Figure 1a and b).
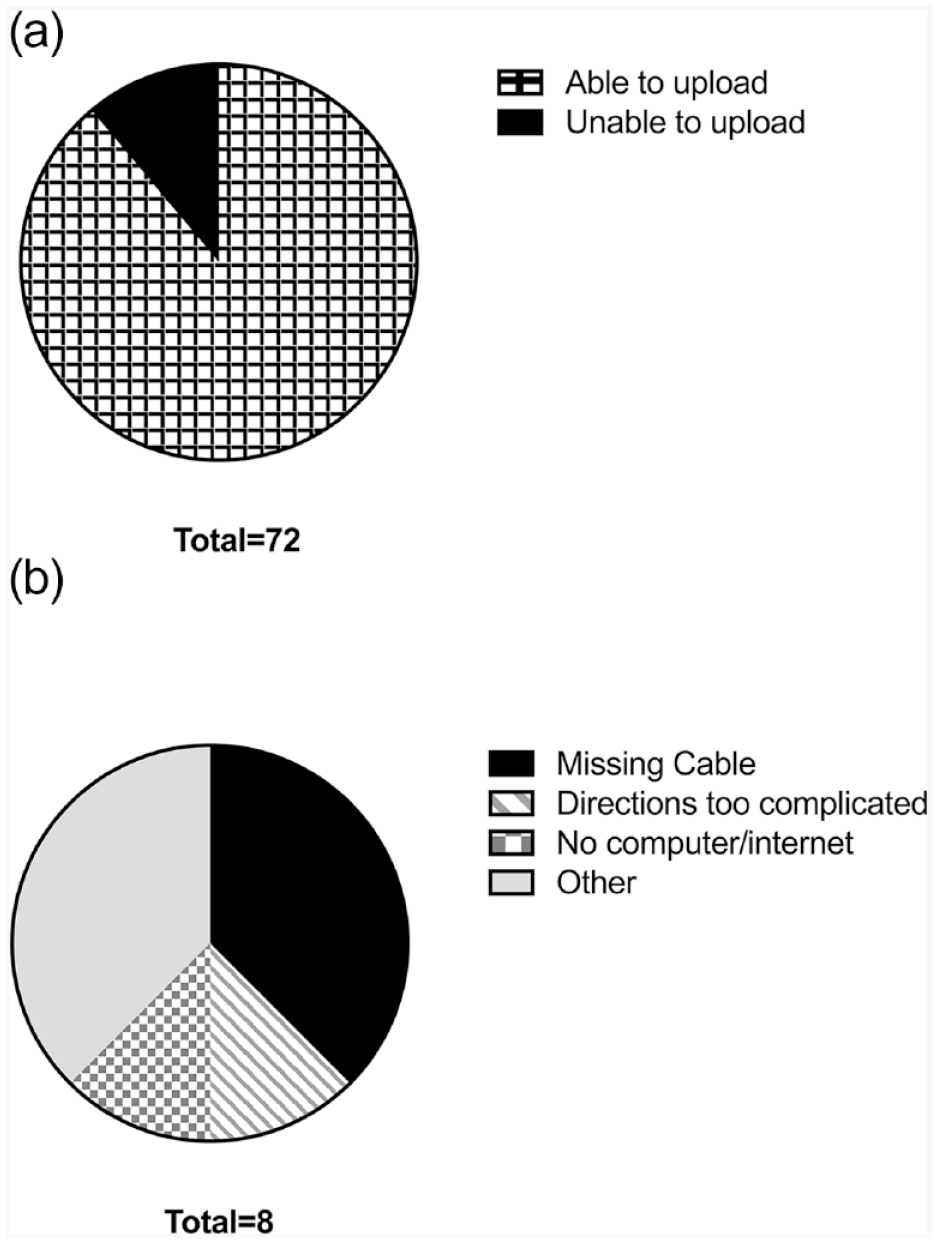
(a) Ability to upload data for telehealth visit. (b) Barriers to upload. Figure 1a and b. Of the 72 patients who reported having telehealth visits, 12% did not upload data. Reasons for not uploading are detailed on the right. Nine successful data uploaders indicated via free-text that they had difficulties uploading due to operating system incompatibilities.
Discussion
This study aimed to evaluate effectiveness of retrospective data review in the context of insulin adjustments made by a caregiver. There are no published studies to our knowledge evaluating real-world effectiveness of caregiver-driven retrospective data review in the context of retroactive insulin adjustment. We demonstrated high rates of retrospective data review but no associated overall HbA1c benefit. However, we did demonstrate a significant association between increasing numbers of retroactive insulin adjustments and improvement in HbA1c. Similar improvements in HbA1c were not demonstrated when analyzing the number of one-time insulin adjustments made. This suggests that retrospective data review with ensuant retroactive insulin adjustment is an important contributor to glycemic control in this group of predominantly CGM users. Frequent insulin dose adjustment has been demonstrated in clinical studies with younger children to be important given their evolving insulin needs. 21 Both major organizations advocating for pediatric diabetes care recommend quarterly clinic follow up—specifically, the International Society for Pediatric and Adolescent Diabetes (ISPAD) explicitly discusses interval communication and remote data monitoring, citing that families should be encouraged to review and attempt to analyze the data before contacting the diabetes team for advice.10,22 However, no guidance surrounding how to structure education on retrospective data review or best practices for downloading is provided.22-24 Further studies involving practices of successful retrospective data reviewers may provide insight into how to initiate structured education surrounding retrospective data review.
Our study further adds to the literature on retrospective data review by evaluating data review in the context of caregiver fear of hypoglycemia. There is conflicting evidence regarding the impact of fear of hypoglycemia on overall glycemic control.19,25,26 Retrospective data review in our study was associated with increased HFS-behavior scores but not improved HbA1c, suggesting that perhaps avoidance of hypoglycemia rather than mitigation of hyperglycemia prompted the retrospective review. This population of caregivers with higher HFS-behavior scores may benefit from automated pattern recognition software, which has shown non-inferiority to dose adjustments based on physician-driven retrospective data review. 27 Real-world studies exploring feasibility and safety of automated pattern recognition software by caregivers with higher HFS-behaviors scores compared to standard retrospective data review with retroactive insulin adjustment would be informative and may improve glycemic control of children whose caregivers are already reviewing data.
Our study evaluated caregiver retrospective review in the context of child’s HbA1c, but it did not include an assessment of patient-initiated retrospective review. The median age of child of retrospective data reviewers was 12.2 versus 15.4 in non-reviewers and may reflect the developmentally appropriate progression of diabetes management tasks. 10 A follow-up study on retrospective data review/insulin adjustment behaviors of adolescents is a critical next step in understanding their relationship with retrospective review as they begin their transition to independent diabetes care. This is especially important given that the greatest rise in HbA1c in the T1D exchange occurred in the 13- to 25-year-old cohort. 1
Barriers to downloading data that prevented caregiver-driven retrospective data review were also identified as part of this study. There were no published studies on barriers to device download as of the publication of the 2018 ISPAD Clinical Practice Consensus Guidelines for Diabetes Technology. 28 We did not identify any interval publications related to such barriers, making this the first study to directly address this issue. In our study, 12% of caregivers did not download data for their telehealth visit, the majority of them indicating that this is because they were unable. This is likely a significant underestimate, but is still an important finding given that survey responders represent a portion of our clinic population who were able to complete an electronic-based survey. Presumably, these responders have high technology literacy. It is also important to note that most individuals in this sample who downloaded data were CGM users with prior remote data sharing capability. This highlights the utility of helping patients enable automatic data sharing at the time of CGM initiation and should become part of CGM start protocols.
Comparing our findings to prior work demonstrates a higher overall percentage of retrospective data review than previously published.11,12,28 Unlike Wong et al, we did not demonstrate improvements in HbA1c with retrospective review.12,24 Mean age (11.9 versus 12.9) and private insurance status (80% versus 78.5%) are similar in our study and Wong et al; however, our study population has a higher percentage of CGM usage (88% versus 36%). This is anticipated given the significant longitudinal increases in youth CGM use since that study was completed in 2015. 29 An earlier study found that CGM users are most likely to be data downloaders and may explain the comparatively higher proportion of overall data review in our study. 28 However, even with such a high percentage of CGM use in our study, a significant portion of our population still did not review the data with the intent to make insulin dose changes.
This study also differed with respect to prior work regarding effectiveness of types of insulin dose adjustments made, namely that our study showed HbA1c improvements related to retroactive insulin adjustments but not one-time insulin adjustments. The SWITCH study, in which children and adults used insulin pumps and crossed over from a CGM sensor-on to a sensor-off arm noted improvements in HbA1c favoring the CGM sensor-on arm. HbA1c improvements in this group were attributed to one-time insulin adjustments (increased number of boluses/day, more temporary basal rates, more manual pump suspensions, and increased use of the pump bolus wizard) as they noted an increased number of such adjustments when participants had real-time access to the CGM data. 30 A 2015 study of adult CGM users indicated that 80% believed real-time analysis was more useful than retrospective analysis and almost 20% never or rarely downloaded their data. 31 However, our study demonstrates that retrospective review with retroactive insulin adjustment may actually be superior to one-time insulin adjustments in youth patients using CGM and should be equally emphasized and encouraged. The discrepancy in perceived versus actual benefit of real-time and retrospective analysis strongly suggests this as an area for improvement in patient and clinician education.
Strengths of this study include detailed assessment of retroactive insulin adjustments and one-time insulin adjustments in the context of CGM use and retrospective data review in a real-world population of diabetes caregivers. Additional strengths include evaluating retrospective review in the context of fear of hypoglycemia and assessing for barriers to data download, neither of which have been previously published. It is notable that the population that responded to the survey is significantly different than those who did not with regards to age, insurance payor, and HbA1c. This is further confounded by the fact that an electronic-based survey is more likely to garner response from those participants who are more familiar or comfortable with the technologies that are required for data review and download. We attempted to mitigate this by offering an option to complete the survey during a clinic appointment; however, almost 40% of those without email addresses did not have a clinic visit scheduled within study enrollment period and in-person clinic visits were reduced due to the COVID-19 pandemic. As such, utilization of the in-person option was too limited to perform additional statistical analysis on this sub-population. An additional weakness of the study is utilization of self-reported data—however, by including a linker back to a pre-existing database, we were able to validate some of the self-reported information including our primary outcome variable. Median HbA1c of children in our responders sample is low relative to population data reported from the United States and may suggest responder bias. The results are still important and demonstrate room for improvement in retrospective review, retroactive insulin adjustment practices, and addressing barriers to download in a technology literate subset of caregivers.
Conclusions
Caregiver-initiated retrospective data review is common among caregivers of primarily younger CGM users. HbA1c improvements corresponded to increasing number of retroactive insulin adjustments but were not noted among the retrospective review group independent of retroactive insulin adjustment. Additionally, it is important to note that barriers to data downloading exist even among highly technology-literate caregivers.
A moveable target to encourage more frequent data downloading includes simplification of data access—namely facilitating automated data sharing at the time of diabetes device start and incorporating data downloading into diabetes device education. Diabetes technology companies should prioritize wireless data sharing and aim to use universal cords. Future studies are needed to determine the most effective retrospective data review strategies (i.e. clinical training, patient education, automated pattern recognition).
Supplemental Material
sj-pdf-1-dst-10.1177_19322968211059537 – Supplemental material for Diabetes Device Downloading: Benefits and Barriers Among Youth With Type 1 Diabetes
Supplemental material, sj-pdf-1-dst-10.1177_19322968211059537 for Diabetes Device Downloading: Benefits and Barriers Among Youth With Type 1 Diabetes by Benjamin A. Palmer, Karissa Soltys, M. Bridget Zimmerman, Andrew W. Norris, Eva Tsalikian, Michael J. Tansey and Catherina T. Pinnaro in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
We thank the patients and staff at the University of Iowa Stead Family Children’s Hospital for participation in this study. We would also like to thank the pediatric diabetes research team, particularly Marissa Goetz.
Abbreviations
T1D, type 1 diabetes; CGM, continuous glucose monitor; HFS, hypoglycemia fear survey; HbA1c, glycated hemoglobin A; DCCT, The Diabetes Control and Complications Trial; REDCap, Research Electronic Data Capture; ISPAD, International Society for Pediatric and Adolescent Diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from NIH T32DK112751, K12 HD27748, R01DK115791, and UL1TR002537.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.