
Abstract
Background:
Despite the clear benefits of increased physical activity (PA) on glycemic control, little is known about the importance of the timing of exercise among people with diabetes. Our objective was to compare the time of day of PA with concurrent HbA1c levels and body mass index (BMI) among Hispanic/Latino adults with or at risk of type 2 diabetes (T2D).
Methods:
Monitored activity data obtained from Hispanic/Latino adults were summarized as number of steps per day, moderate-to vigorous-intensity physical activity (MVPA), and energy expenditure (kcals/day). We next examined the association between PA measures and participants’ HbA1c. K-means clustering analysis was applied to identify daily PA patterns by time of day and intensity.
Results:
Three dominant clusters were identified: low-intensity PA, and early and late PA by time of day. The step counts were correlated with HbA1c in the late-active group (P = .01). Furthermore, independently in younger adults (age ≤ 50 years) and in overweight adults 25 ≤ BMI < 30 kg/m2), there was an association between HbA1c and step counts (P < .01 and P < .005, respectively) as well as HbA1c and MVPA (P < .05 and P < .035, respectively).
Conclusions:
For Hispanic/Latino adults with or at risk of T2D, there appears to be clustering of PA by intensity and time of day which, in turn, may influence achieved HbA1c and BMI. Our findings demonstrate that the amount of activity is more efficacious on HbA1c in participants who are more active later during the day and separately in overweight and younger individuals. This finding may help design more personalized PA recommendations in this population.
ClinicalTrials.gov Identifiers:
NCT03830840 and NCT03736468.
Keywords
Background
For people living with type 2 diabetes (T2D), it is recommended that physical activity (PA), a term that describes movement associated with increased energy use, be prescribed as part of the management of glycemia and overall health. 1 This is based on evidence that PA can help to improve glycemic control as measured by changes in HbA1c levels 2 and 24-hour ambulatory glucose profiles. 3 In addition, reducing the amount of sedentary time may also help prevent T2D for those at risk. 4
The American Diabetes Association recommends that most adults with T2D should engage in 150 or more minutes of moderate-to-vigorous-intensity aerobic activity each week, with no more than two consecutive days without PA. 5 At present, it is unclear whether the time of day to be more physically active influences health outcomes for people with or at risk of diabetes. The proportion of people with or at risk of T2D who achieve this recommended level currently is below ideal and varies by race and ethnicity. 6 In 2020, the United States Centers for Disease Control and Prevention reported that Hispanic/Latino adults had the highest prevalence of physical inactivity by race/ethnicity, and Hispanic/Latino and non-Hispanic black adults had a significantly higher prevalence of inactivity than non-Hispanic White adults in the majority of states. 7 The report defined PA as a self-report of engaging in any leisure-time PA during the past month. The report did not appear to take into consideration PA as part of work/occupation.
Wearable activity trackers can empower people with obesity, prediabetes, and T2D to improve their activity levels, especially in men. 8 In a previous study among Hispanic/Latino adults with T2D, we compared objective measurements of PA using a research-grade waist-worn accelerometer (ActiGraph) with a ubiquitous wrist-worn consumer device (Fitbit) and with participants’ self-reported levels of PA. Overall, both objectively measured and self-reported levels of PA were moderate, with daily step counts averaging almost 7000 to 9000 steps/day. These findings challenge the assumption that inactivity is commonplace for this population with T2D. 9 In addition, the approach used to promote and assess PA in different racial and ethnic groups is important, given that these communities face a disproportionate burden of T2D compared to the background White population. 10
While the total amount of PA performed is a significant determinant of cardiovascular health and improved glycemic control, few studies have examined the effect of the timing of PA on these outcomes for racial/ethnic minorities. Therefore, this study aimed to investigate the relationship between HbA1c levels and objective measurements of PA, including the effect of timing of PA, in Hispanic/Latino adults with or at risk of T2D.
Methods
Study Design and Participants
Institutional Review Board approval was obtained for both a pilot (Quorum Independent Review Board, QR# 32669/1) and an observational cohort study (Advarra Independent Review Board—Sansum Diabetes Research Institute (SDRI) #2017-6004). We have included participants from both the pilot and observational studies. Participants provided written informed consent in their preferred language (English or Spanish).
For the pilot and longitudinal observational cohort studies, Hispanic/Latino adults with or at risk for T2D were recruited from the local community using bilingual (Spanish and English) outreach materials and with help from bilingual community health workers through community outreach, from existing programs, Hispanic/Latino-focused community organizations, and local health and social services. Inclusion criteria included adults ≥18 years of age with T2D for at least 6 months or self-reported as at risk for developing T2D using the American Diabetes Association diabetes risk assessment tool. 11 Exclusion criteria included pregnancy or any active clinically significant disease or disorder which in the investigator's opinion could interfere with participation in the study.
Sansum Diabetes Research Institute has developed an “Especialista” model, in which bilingual Latino/a community’s health workers are trained by SDRI in diabetes identification, research methodology, and referrals to health care and other social needs resources. 12 After enrollment, each participant was paired with an especialista who spoke their preferred language/s (Spanish and/or English). Especialistas facilitate research activities, which include administering the informed consent and conducting study encounters, such as training and placement of activity monitors. Participants could meet with their especialista physically, or reach them via email or phone while enrolled in the study.
Data Collection and Measurements
Following informed consent, demographic data, including date of birth, and anthropometric data were recorded at the screening/enrollment visit. Height was measured in centimeters and weight in kilograms using a mechanical column scale with an eye-level beam (Seca 700, Seca GmbH & Co, KG, Hamburg, Germany), or a wall-mounted stadiometer (Ayrton, Ayrton Measuring Devices) and a Tanita digital scale (TBF-300A, Tanita Corporation of America, Inc, Arlington Heights, Illinois, USA). Waist circumference was measured using a flexible tape at the umbilicus. Measurements were made following the National Health and Nutrition Examination Survey (NHANES) Anthropometry Procedures Manual. 13
The screening/enrollment, physical exam, and laboratory visits were completed before a visit for instruction and placement of the activity monitors. Instruction was undertaken in the participant’s preferred language (Spanish or English), and written reminders were also provided in the participant’s preferred language.
PA Measures
Physical activity was measured using the ActiGraph wGT3X-BT (ActiGraph, LLC, Pensacola, FL, USA). The ActiGraph is a small (length 4.6 cm × width 3.3 cm × height 1.5 cm) and lightweight (19 g) triaxial accelerometer. It is a commonly used research device for monitoring PA in free-living conditions. 14 The ActiGraph was worn on the dominant hip with an elastic belt. Participants were asked to wear the device 24 hours per day, except when bathing or swimming, for 7 days.
The device was initialized using software for the device and with the participant’s sex, height, weight, age, and ethnicity. ActiGraph measured activity is blinded to the participant and was recorded at a frequency of 30 Hz and analyzed in 60-second epochs using the manufacturer’s software (ActiLife 6.13.4). The downloaded data were screened for wear time using the Troiano algorithm, 15 and the Freedson VM3 Combination was used to calculate PA energy expenditure (EE, kcals/day). 14
The ActiGraph accelerometer assessed acceleration using counts as the output metric. To interpret counts, there are several approaches to defining cut points or thresholds to distinguish activities by intensity, 16 which includes sedentary, light, moderate, or vigorous activity. In line with previous studies that incorporated lifestyle activities, vigorous PA was defined as >2020 counts/minute, the moderate to vigorous PA or lifestyle range was between 760 and 2019 counts/minute, light-intensity PA was between 101 and 759 counts/minutes, and sedentary behavior was defined as less than or equal to 100 counts/minute. 17
Statistical Analyses
Physical activity measures utilized in the analysis were assessed by hip-worn accelerometers, with indices including the overall number of steps, moderate-to-vigorous-intensity PA (MVPA), and energy expenditure (kcal). In a first analysis, PA and energy expenditure measurements were averaged over 24-hour periods and the total number of days to obtain a single data point for each participant in the study. Next, univariate analyses were used to compare PA characteristics in different gender, age, and body mass index (BMI) categories.
In a secondary analysis, an aggregation process to summarize the 24-hour temporal data into three-dimensional data was created with each dimension representing PA performed in 6-hour blocks of each day. Owing to sporadic behavior observed in PA data, each participant's number of steps through the morning, afternoon, and evening for each day were aggregated. After excluding data recorded from 00:00 to 06:00 hours (as there was rarely any activity occurring in this time due to sleep), steps taken during 06:00 to 12:00 were categorized as a morning activity, 12:00 to 18:00 as an afternoon activity, and 18:00 to 00:00 as an evening activity, with each day stratified into three segments with PA data (yielding each day PA represented by a point in 3D space). Thus, excluding the monitor placement and removal days, 715 days of complete data were aggregated into 715 3D points. To identify repetitive daily patterns of PA, the k-means clustering method was used. For this, the within-group sum of squared error of clustering solutions from k = 1 to 10 was calculated, and the optimum number of clusters was identified by the elbow curve method using a Python algorithm.18,19
Non-parametric (Kruskal–Wallis) tests were used to compare characteristics in PA groups and groups with different age, sex, BMI, and waist circumference ranges, with further analysis for different risk categories involving HbA1c ranges and lipid profile (P <.001 for Kolmogorov–Smirnov normality tests). Bivariate correlation analyses were also performed using the Spearman correlation. Linear regression was used to examine any monotonic relationship between PA and blood glucose measures. All statistical analyses were performed in Python. A P value of .05 or less was considered statistically significant.
Results
A total of 121 participants (aged 27-83 years, 80 women) were included in the study (Table 1). The majority (85%) had a self-reported diagnosis of T2D. Overall, 61 participants (50.4%) had a BMI of 30 kg/m2 or more, with 41 (33.9%) having a BMI between 25.0 and 29.9 kg/m2. Insulin use was reported by 21 (17.4%) participants. Women were more obese than men (with BMI of 31.5 ± 5.5 kg/m2 vs. 29.12 ± 4.86 kg/m2 for men, P < .01). Women in this group had higher low-density lipoprotein (LDL) levels (99.4 ± 33.4 mg/dL) as compared to 83.7 ± 33.3 mg/dL for men (P < .05), and total cholesterol (181.5 ± 36.5 mg/dL) as compared to 166.1 ± 46.6 mg/dL for men (P < .05).
Demographic, biological, and physical activity data for study participants. Data are shown as mean ± standard deviation for normally distributed variables and median (interquartile range) for non-normally distributed variables.
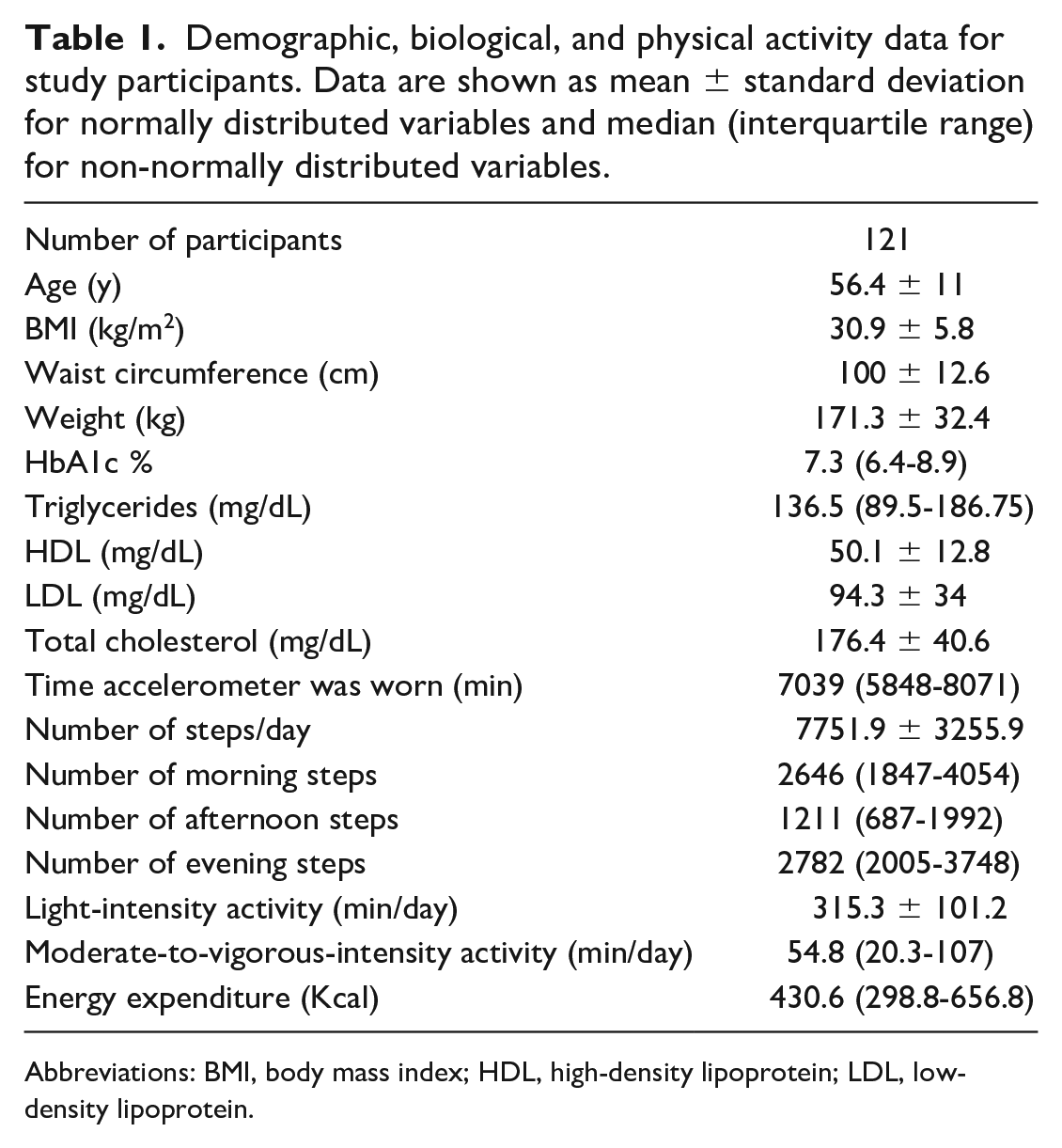
Abbreviations: BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Women were more adherent in wearing the accelerometer than men with an average wear time (±SD) of 4.9 ± 1.1 versus 4.3 ± 1.2 days, respectively, P < .05. Physical activity time was disproportionately distributed between light-intensity activities (27%), moderate-to-vigorous-intensity physical activity (MVPA) (6.3%), and vigorous-intensity activities (1.5%). On average, 68 participants (56%) spent less than 10 minutes of vigorous-intensity activity per day. In addition, for men, there was a significant inverse linear relationship between HbA1c and steps per day (b = −0.32, R = −0.35, P = .03), MVPA (b = −0.42, R = −0.43, P < .01), and energy expenditure (b = −0.47, R = −0.38, P = .01).
Clustering Analysis and Characteristics of the Habitual Routine Labeled Groups
Each monitored day was converted into three aggregated segments, so there were 715 data points collected in general. k-means clustering was applied to identify the repetitive patterns and allocate every data point to the nearest one. While k-means clustering does not yield clear-cut boundaries and cutoffs, almost 98% of the low-active days had less than 2500 step counts in the evening or 3500 step counts in the morning or afternoon.
The days with more than 4500 morning steps were mostly clustered in the early-active group. The late-active cluster consisted mostly of days with more than 5000 steps in the afternoon and evening. Thus, three dominant clusters were identified: (1) 352 low-active days (49.2%), (2) 150 early-active days (21.0%), and (3) 213 late-active days (29.8%) (Figure 1).
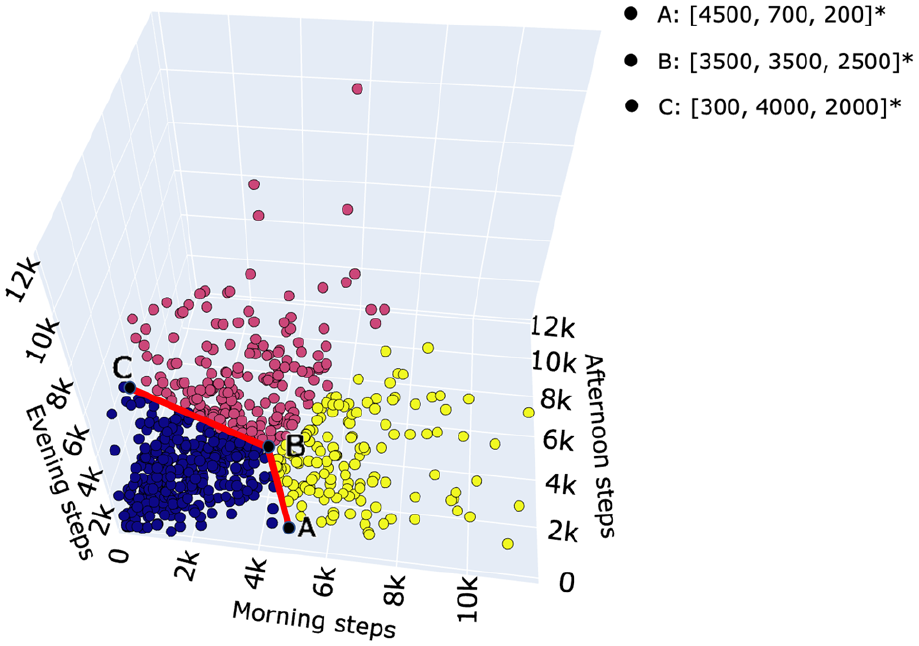
A three-dimensional plot of 715 days by clusters with axes labeled as morning, afternoon, and evening number of steps. Three categories of cluster were low-active, early-active, and late-active days by time of higher physical activity (PA). The red cluster has the days with the lowest activity in all the dimensions (low active days). The blue cluster consists of points with the highest number of steps in the morning (x-axis) and fewer steps taken in the evening (z-axis); hence labeled as early active days. The yellow cluster consisting of the highest values of evening and afternoon steps (y-axis) is labeled as late active days.
Eventually, the participants were labeled based on the majority of their monitored days falling into one of these clusters. We called the participants in each of these clusters “habitual routine groups,” with descriptors “low active,” “early active,” and “late active.” If there was no clear majority placement, for instance, if a participant spent 3 days as low active and 3 days as early active, they were not labeled in any of the groups. Table 2 shows the characteristics of the three groups.
Characteristics of the three habitual routine groups. Data are shown as mean ± standard deviation for normally distributed variables and median (interquartile range) for non-normally distributed variables.
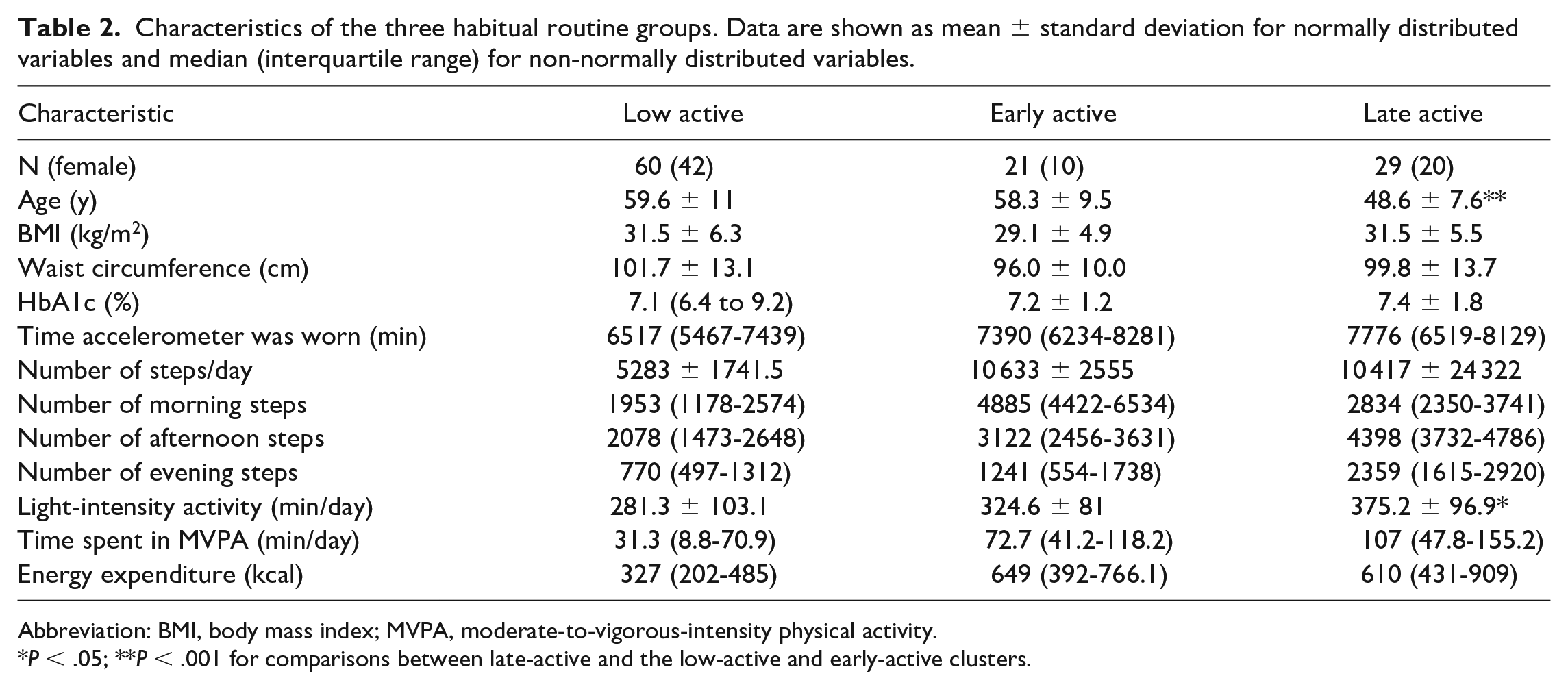
Abbreviation: BMI, body mass index; MVPA, moderate-to-vigorous-intensity physical activity.
P < .05; **P < .001 for comparisons between late-active and the low-active and early-active clusters.
Linear regressions between the activity measures and HbA1c in each group were calculated. There was an inverse linear relationship between the average number of steps per day with HbA1c levels in the late-active participants (b = −0.49, R = −0.45, P = .01).
Participants were also categorized into three groups of age: less than 50 years, between 50 and 65, and more than 65 years of age. Moderate-to-vigorous-intensity physical activity and energy expenditure (kcal) were significantly higher in the age group less than 50 years (P < .005). Table 3 shows the results from the Spearman test between PA measures and HbA1c within each of the three age and BMI categories. For younger adults (age ≤ 50 years), there was an inverse correlation between HbA1c and the number of steps per day (P < .01). Furthermore, the association between the MVPA and HbA1c was significant (P < .05). Linear regression also showed an inverse association of PA measures with the HbA1c level in the overweight group for number of steps per day (b = −0.486, R = −0.429, P = .005), MVPA (b = −0.343, R = −0.329, P =.035), and energy expenditure (b = −0.623, R = −0.397, P = .010).
Spearman rank correlation coefficients of physical activity measures with HbA1c in different age and BMI groups.
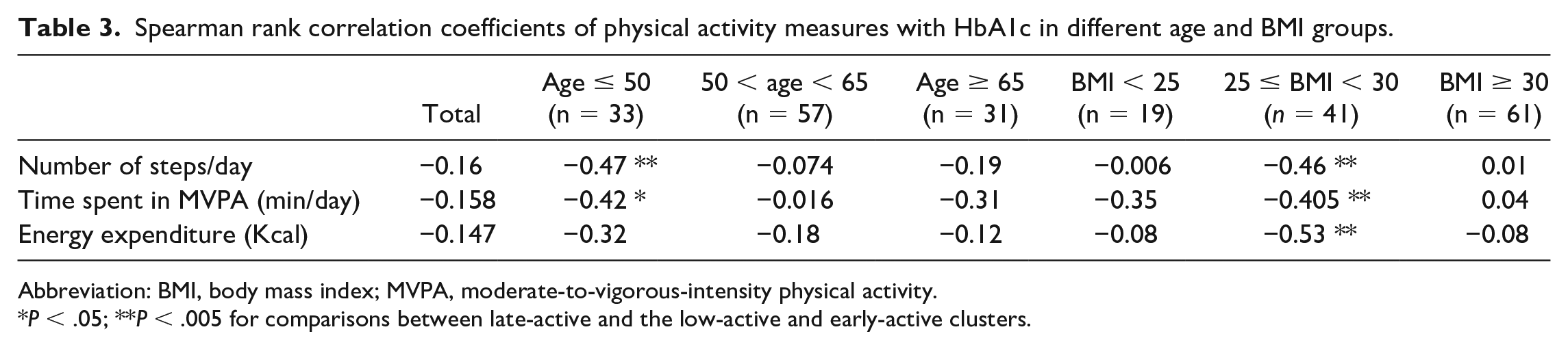
Abbreviation: BMI, body mass index; MVPA, moderate-to-vigorous-intensity physical activity.
P < .05; **P < .005 for comparisons between late-active and the low-active and early-active clusters.
Discussion
Despite the importance of PA in T2D management, current evidence suggests that only a proportion of adults with T2D achieve recommended PA levels with significant variations by race/ethnicity. In a previous study among Hispanic/Latino adults with T2D, we reported moderate levels of PA levels, challenging the assumption that inactivity is commonplace for this population. 9 In this study involving Hispanic/Latino adults at risk and with T2D, there appears to be clustering of PA by intensity and time of day which, in turn, appear to influence achieved HbA1c and BMI levels.
The population under investigation, predominantly Hispanic/Latino women, had a high burden of cardiometabolic risk factors, including obesity, high waist circumference, abnormal lipid profiles, and T2D. Over 7 days, participants averaged approximately 8000 steps/day measured using Actigraphy. Most time was spent in light-intensity PA with less than 10 minutes per day in vigorous-intensity PA. The average step count measured in this study is likely to have important clinical benefits. In a nationally representative cohort of 4840 U.S. adults, a greater number of steps per day was significantly associated with lower all-cause, cardiovascular, and cancer mortality. 20 In that study, compared with individuals who took 4000 steps per day, taking 8000 steps per day at baseline was associated with a 51% lower risk of all-cause mortality including for women and Mexican American participants. In contrast, there was no significant association between higher step intensity and mortality after adjusting for total steps per day.
In this study, using clustering analyses, it was possible to stratify participants into three groups based on step counts and timing of PA. Specifically, participants were classified into “low-active,” “early-active,” and “late-active” groups. Late-active group participants tended to be younger with more time spent in light-intensity PA compared to participants in the early-active and low-active groups. Levels of MVPA were similar across groups. However, there was an inverse relationship between the average number of steps/day and MVPA with HbA1c levels in the late-active group.
Regular MVPA improves cardiorespiratory fitness and is associated with a lower risk of cardiovascular complications and premature mortality in adults with T2D. 21 Recently, in a cross-sectional study of adults with T2D and obesity, the timing of MVPA appeared to be associated with cardiorespiratory fitness independent of volume or intensity of MVPA. Among women, those most active in the evening had higher cardiorespiratory fitness than those who were active at other times. In contrast, the timing of MVPA among men was more impactful for those undertaking MVPA in the morning. 22 The positive impacts of the timing of PA on glucose control in T2D and lipid and amino acid metabolism in obese men have also been shown in small group studies using structured exercise interventions. 23 These studies suggest that the application of PA may be optimized by also considering the time of day. 24 In the United States, adults accumulate almost 80% of their current overall PA at work and in household-related activities, with leisure-time PA comprising the bulk of the remaining contribution with walking being the most common leisure-time PA. 25 Similarly, in insulin-resistant adults, encouraging more time spent standing improves insulin sensitivity. 26 Another approach is to promote PA after meals. In adults with T2D, the interruption of prolonged sitting with light-intensity walking or simple resistance activities decreases postprandial glucose, insulin, and triglyceride levels. 27
Here, we found that Hispanic/Latina women had higher cardiometabolic risk than men. Low-income Hispanic/Latina women, particularly those of Mexican descent, are known to be at greater risk of metabolic syndrome. 28 Despite a burden of cardiovascular disease (CVD) risk and a higher prevalence of certain risk factors, such as T2D, Hispanics/Latinos have a lower-than-expected rate of premature death from CVD. 29 Hispanics/Latinos are not sedentary, 9 and Latina women often engage in short stints of moderate PA rather than a long-sustained moderate-to-vigorous activity, which has been reported to be associated with higher high-density lipoprotein cholesterol (HDL-C) levels. 30 In this study, HbA1c was also significantly lower in younger adults (<50 years) who had more steps per day and moderate-to-vigorous levels of PA. Furthermore, categorizing the participants based on their BMI also suggested that higher PA measures were associated with lower HbA1c values in the overweight group. These significant associations persisted for the number of steps per day and time spent in MVPA during the day. A previous study on adults with T2D demonstrated that the timing of PA impacts glycemic profiles in men. 31 Our findings further supported the associations between the step counts in the late active group of participants with HbA1c in this group (P = .01). The mechanism for the effect of timing of PA on glycemic control is unclear but may relate to changes in insulin sensitivity due to effects on sympathetic and parasympathetic activity and fuel utilization, on gastric emptying or perhaps food choices.23,31
Strengths of the study include the focus on an underserved and clinically important population (i.e., predominantly Hispanic/Latina women) who are underrepresented in clinical research. 32 The study has a few critical limitations. As an exploratory-feasibility study, the sample size is relatively small and unbalanced between the sexes, and this is likely to limit the interpretability of our findings especially related to stratifying groups. The participants did not keep daily PA logs, so we cannot precisely describe what activities these participants were doing each day. This cohort overwhelmingly consisted of participants of Mexican descent, and therefore, the findings cannot be generalized to other groups identifying as Hispanic/Latino. Also, this is a cross-sectional study, and the participant’s usual behavior may have been influenced by wearing the activity monitor. Simply wearing an activity monitor, even when participants are blinded to the data, as in this study, may have increased awareness of how much activity they were doing and could reflect an increase in PA that occurs with self-monitoring. Another limitation is the length of wear time, 7 days, to describe the mean activity level.
Conclusion
Our results lend support to the link between the timing of PA and cardiometabolic risk which is likely to be mediated through circadian rhythms. 22 Our findings suggest that participating in PA later in the day may be more impactful than at an earlier time, but this needs to be determined in larger trials adequately powered for stratification into subgroups based on age, BMI, sex, and other variables.
Wearable activity monitors that count steps are widely available and provide immediate feedback to the user. When combined with individual’s characteristics and behavioral strategies, they may be an effective way to help design more personalized PA recommendations especially for underserved populations facing a disproportionate burden of T2D.
In addition to encouraging or prescribing steps (i.e., dosing) to at risk individuals, there may also be a need to consider the timing of PA to achieve the maximum return on investment for individuals with or at risk of diabetes.
Footnotes
Acknowledgements
The authors would like to thank the SDRI Especialistas for their help with this study.
Abbreviations
PA, physical activity; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an unrestricted grant from Eli Lilly and Company, the Elsevier Foundation, and NSF ERC PATHS-UP (grant no. 1648451).