
Abstract
Background:
Between-system differences for continuous glucose monitoring (CGM) devices have important clinical consequences.
Purpose:
Here we review attributes of Dexcom’s fifth-, sixth-, and seventh-generation (G5, G6, and G7) CGM systems.
Methods:
Accuracy metrics were derived from preapproval trials of the three systems and compared after propensity score adjustments were used to balance baseline demographic characteristics. Metrics included mean absolute relative differences (MARD) between CGM and YSI values and the proportion of CGM values within 20% or 20 mg/dL of the YSI values (“%20/20”). Ease-of-use was evaluated by formal task analysis.
Conclusions:
Adjusted MARD and %20/20 agreement rates were 9.0%/93.1% (abdomen-placed G5), 9.9%/92.3% (abdomen-placed G6), 9.1%/93.2% (abdomen-placed G7), and 8.2%/95.3% (arm-placed G7). Task analysis favored G7 over earlier systems. Favorable clinical outcomes such as hemoglobin A1c reduction and hypoglycemia avoidance seen with G5 and G6 are anticipated with G7 use.
Introduction
The accuracy, usability, and adoption rates of real-time continuous glucose monitoring (CGM) systems continue to improve. The accuracy of some CGM systems is now approaching that of some blood glucose meters, and in the case of the G5 system (Dexcom, Inc, San Diego, California), accuracy is sufficient as the basis for insulin dosing decisions. 1 The company’s current flagship product, the G6 system, also allows for nonadjunctive insulin dosing decisions and includes features such as voice activation and predictive alerts that have been associated with improved glycemic control, 2 and an easier-to-use 3 automated sensor applicator.
Several large trials have established the clinical benefits of the G5 system with respect to hemoglobin A1c (HbA1c) reduction, hypoglycemia avoidance, and improved time in range (TIR).4-11 More recent studies of the G6 system have demonstrated glycemic improvements when G6 was used by adolescents and young adults with T1D 12 and by adults with T2D managed with nonintensive insulin regimens.13,14 However, benefits obtained with different CGM systems may differ in both scope and extent. For example, Visser and colleagues 15 documented improved TIR for participants transitioning from a CGM system without alarms to one with alarms, and our group 16 demonstrated improved utilization rates and TIR for customers who transitioned from the G5 to the G6 system.
The accuracy of arm- and abdomen-placed seventh-generation “G7” CGM sensors (Dexcom) was recently established in adults 17 and in children and adolescents. 18 We compared attributes of G7 sensors with those of abdomen-placed G5 and G6 sensors to inform expectations regarding G7 clinical outcomes.
Methods
Separate pivotal studies established the accuracy of the abdomen-placed G5 (NCT02087995), 19 abdomen-placed G6 (NCT02880267), 20 and arm- and abdomen-placed G7 (NCT04794478) 17 systems. In each, CGM and blood glucose data (obtained with the YSI 2300 Stat Plus system; YSI, Inc, Yellow Springs, Ohio) were obtained from adults participating in clinic sessions that involved intentional glucose manipulations. Accuracy metrics included the mean absolute relative difference (MARD) between contemporaneous CGM and YSI values 21 as well as agreement rates for the proportion of CGM values within 15 mg/dL of comparator values ≤100 mg/dL or within 15% of comparator values >100 mg/dL (“%15/15”) and the analogous %20/20 and %30/30 agreement rates. The glucose concentration limit of 100 mg/dL used in agreement rate calculations was chosen for consistency with the ISO 15197:2013 standard for in vitro blood glucose monitors. 22 MARD and agreement rates are presented as unadjusted point estimates as well as estimates that were adjusted by propensity score methods 23 to reduce the effect of confounding variables in the three studies. As described previously, 16 adjustments were made for potentially confounding baseline attributes, including age, sex, type of diabetes, log-transformed HbA1c, and body mass index. Lag times, which represent intervals between changes in blood glucose concentrations and corresponding changes in CGM readings, 24 were calculated as previously described.25,26
Using existing design principles and in compliance with recognized usability guidelines, 3 a task analysis identified the individual perceptual inputs, cognitive processes, and actions required for a user to complete the overall task of sensor insertion. Tasks required for successful insertion of the G5, G6, and G7 sensors were enumerated. Participants in the G7 accuracy study were surveyed with respect to ease of insertion and comfort during insertion and wear.
The systems were also compared with respect to their ability to detect hypoglycemia by retrospectively examining CGM data during intervals in which the YSI value was either ≤55 mg/dL or ≤70 mg/dL (a “hypoglycemic event”). In this analysis, CGM values within 15 minutes of a hypoglycemic event were considered and the missed detection rate was defined as the fraction of events that were not accompanied by CGM values (either ≤55 mg/dL or ≤70 mg/dL) that would have triggered an alert. Results are presented separately for CGM alert thresholds of 55 mg/dL and 70 mg/dL. Consistent with earlier studies,17,27 the false hypoglycemia alert rate was defined as the proportion of CGM excursions ≤55 mg/dL that were not accompanied by YSI value(s) <70 mg/dL within 15 minutes.
Results
As shown in Table 1, arm-placed G7 sensors provided higher agreement rates with the %15/15 and %20/20 criteria, and lower MARD values, than abdomen-placed G5, G6, or G7 sensors, with or without propensity adjustments. Missed hypoglycemia detection rates shown in Table 2 show that this parameter depends on the threshold value chosen for the CGM system—all three systems were much less likely to miss a true hypoglycemic event if the CGM threshold was set to 70 mg/dL rather than 55 mg/dL. With the CGM hypoglycemia alert setting of 55 mg/dL, the G7 system had a lower rate of missed hypoglycemia detections than either of the earlier systems, suggesting that it can more reliably detect and alert users to dangerously low blood glucose values. The rates for falsely alerting users to hypoglycemia—occasions where a CGM value ≤55 mg/dL was not accompanied by a YSI value <70 mg/dL within 15 minutes—were low for all three systems.
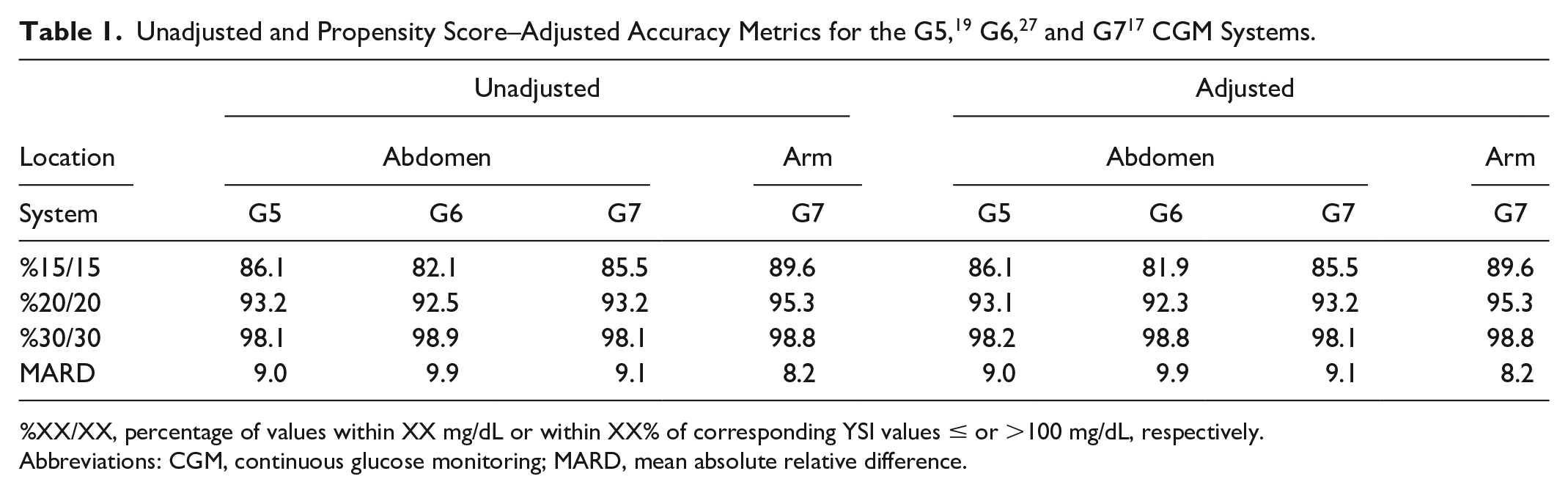
%XX/XX, percentage of values within XX mg/dL or within XX% of corresponding YSI values ≤ or >100 mg/dL, respectively.
Abbreviations: CGM, continuous glucose monitoring; MARD, mean absolute relative difference.
Alert Performance of the G5, G6, and G7 CGM Systems.
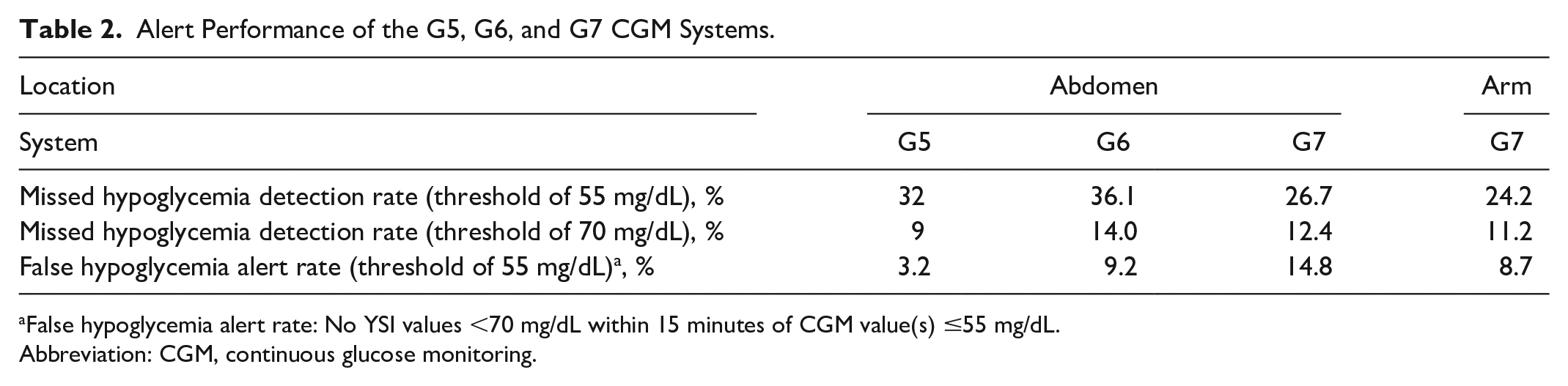
False hypoglycemia alert rate: No YSI values <70 mg/dL within 15 minutes of CGM value(s) ≤55 mg/dL.
Abbreviation: CGM, continuous glucose monitoring.
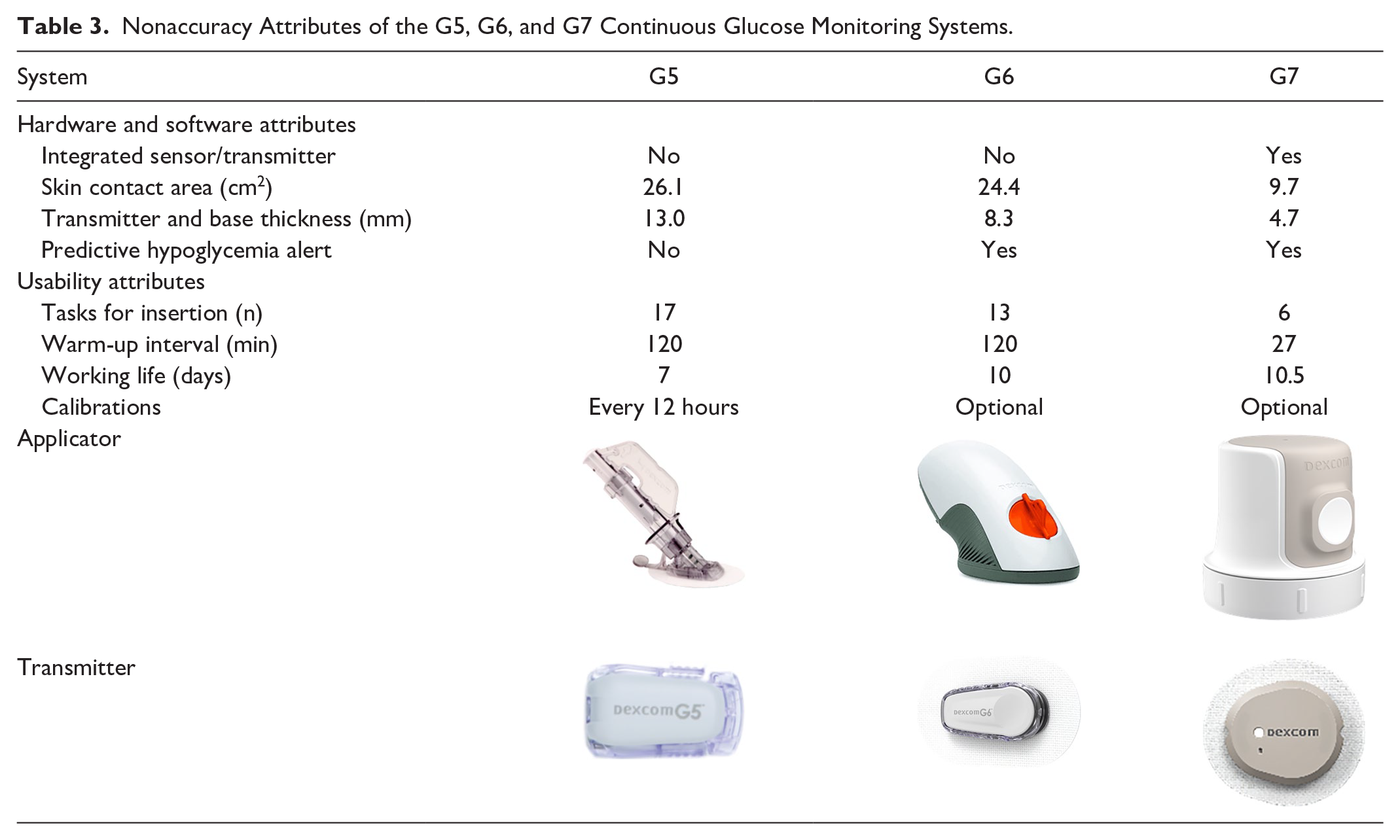
Task analysis results (Table 3) revealed that successive generations of the CGM systems required fewer decisions and actions from the user for successful insertion. Among participants in the G7 accuracy study, 96% reported that sensor insertion was “somewhat” or “very” easy, 94% reported that there was “no pain” or “mild pain” during insertion, and 95% reported that there was “no discomfort” or “mild discomfort” during wear. The lag time of G7 sensors (arm, 3.6 ± 3.2 minutes and abdomen, 3.4 ± 3.5 minutes) 17 was shorter than previously reported lag times of five to six minutes for G5 19 and 3.7 ± 3.1 minutes for G6 26 systems. Other nonaccuracy attributes of the systems, along with images of the different sensor applicators and transmitters, are shown in Table 3. The G7 system is notable for having a smaller skin contact area, a thinner transmitter, a shorter warm-up time, and a longer working life than earlier systems.
Nonaccuracy Attributes of the G5, G6, and G7 Continuous Glucose Monitoring Systems.
Discussion
As described here, accuracy performance of G7 sensors, whether placed on the arm or abdomen, is similar to that of abdomen-placed G5 and G6 sensors. Egregious errors were rare with all three systems.
Simplification of the sensor insertion process should result in G7 being even easier to learn and several software improvements may contribute to better glycemic outcomes. For example, the new G7 app offers retrospective analysis of glucose patterns and trends on either the dedicated receiver or a compatible device; a list of compatible devices is maintained at dexcom.com/compatibility. The G7 transmitter stores 24 hours of historical data (compared with three hours for the G6 transmitter), which should reduce the length of data gaps attributable to periods of nonconnectivity. The warm-up time between sensor insertion and availability of glucose concentration estimates is 27 minutes for G7, compared with 120 minutes for the G6 and G5 systems. G7 also offers a 12-hour “grace period” of normal functionality at the end of each ten-day sensor session that gives users more time to replace an expired sensor. These features should reduce intersession intervals in which no CGM data are available. The hyperglycemia threshold alert function can now be set with a delay, such that transient postprandial excursions remain unannounced until they become persistent. Rate-of-change alerts have also been redesigned so as to make them more actionable—for example, hypoglycemia treatment is expected to result in rapidly increasing glucose levels and the rate-of-rise alert in this circumstance can be disabled. G7 alert performance, evidenced here as low rates of missed hypoglycemia detection and a low rate of false alerts for hypoglycemia, is also likely to contribute to improved clinical outcomes. Taken together, these attributes may incentivize even higher ongoing use of the devices for diabetes management.
Favorable clinical outcomes established in earlier clinical trials of the G5 and G6 systems such as HbA1c reduction and hypoglycemia avoidance are anticipated for patients who choose G7 as their first CGM system. Patients who transition from earlier systems to G7 will likely enjoy sustained glycemic benefits from the new system’s improved accuracy and usability.
Footnotes
Acknowledgements
The authors thank Drs David Price, Tomas Walker, Courtney Green, Christy Chao, Jennifer Reid, and Stayce Beck (employees of Dexcom, Inc) for helpful advice. Dexcom is a registered trademark of Dexcom, Inc, in the United States and may be in other countries.
Abbreviations
CGM, continuous glucose monitoring; HbA1c, hemoglobin A1c; MAD, mean absolute difference; MARD, mean absolute relative difference; T1D, type 1 diabetes; T2D, type 2 diabetes; TIR, time in range.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employees and stockholders of Dexcom, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dexcom, Inc.