
Abstract
Background:
Diabetes clinicians are key facilitators of continuous glucose monitoring (CGM) provision, but data on provider behavior related to CGM use and CGM generated data are limited.
Methods:
We conducted a national survey of providers caring for people with diabetes on CGM-related opinions, facilitators and barriers to prescription, and data review practices.
Results:
Of 182 survey respondents, 73.2% worked at academic centers, 70.6% were endocrinologists, and 70.7% practiced in urban settings. Nearly 70% of providers reported CGM use in the majority of their patients with type 1 diabetes. Half of the providers reported CGM use in 10% to 50% of their patients with type 2 diabetes. All respondents believed CGM improved quality of life and could optimize diabetes control. We found no differences in reported rates of CGM use based on providers’ years of experience, patient volume, practice setting, or clinic type. Most providers reviewed CGM data each visit (97.7%) and actively involved patients in the data interpretation (98.8%). Only 14.1% of clinicians reported reviewing CGM data without any prompting from patients or their family members outside of visits. Most providers (80.7%) reported their CGM data review was valued by patients although only half reported having adequate time (45.1%) or an efficient process (56.1%) to do so.
Conclusions:
Despite uniform support for CGM by providers, ongoing challenges related to cost, insurance coverage, and difficulties with prescription were major barriers to CGM use. Increased use of CGM in appropriate populations will necessitate improvements in data access and integration, clearly defined workflows, and decreased administrative burden to obtain CGM.
Introduction
The accuracy and usability of continuous glucose monitoring (CGM) technology has dramatically improved in the past decade, leading to enhanced quality of life and improved glycemic control.1-5 However, despite guidelines and emerging evidence supporting CGM use for all people with type 1 diabetes (T1D) and many people with type 2 diabetes (T2D),6,7 uptake remains low. 8
Although diabetes clinicians are key facilitators of CGM use, there has been limited investigation into their role in the extent to which their patients use CGM. In addition to being the prescribers of CGM, diabetes clinicians play an important role in promoting adherence to CGM and providing education and support. 9 A prior study examined clinician perspectives on barriers and facilitators of device use and found that younger, academic, urban clinicians treated more patients using CGM and were more likely to have positive attitudes toward technology. 9 Another study of rural providers identified that lack of provider experience and proficiency with diabetes devices was a major factor in limited CGM use in their patient population. 10 A recent investigation has demonstrated disparities in prescribing diabetes technology, 11 further spotlighting the critical role of the provider in CGM use.
While provider opinion has been previously considered with regard to patient CGM use, implementation and uptake of “new” technologies are influenced by myriad factors. The Consolidated Framework for Implementation Research (CFIR) is a widely used implementation science framework that recognizes five specific domains influencing technology adoption. 12 As applied to the diabetes clinician’s role in CGM uptake, the domains include characteristics of CGM itself, the outer setting (external influences, eg, patient preference, national guidelines, insurance coverage, reimbursement), the inner setting (internal influences, eg, clinic infrastructure), the individual (eg, the diabetes clinician), and the implementation process. We used CFIR to comprehensively evaluate the provider’s role in CGM adoption.
Although retrospective review of diabetes data by patients has been associated with improved glycemic control, 13 less is known about how providers use CGM-generated data in patient care. From the provider perspective, diabetes care has historically relied on interpretation of glycemic data to inform treatment recommendations. 14 However, with recent broadened use of CGM, specific provider behaviors related to CGM generated data review and interpretation are not well described. Key steps in the CGM data review process that require further exploration include methods of data access, frequency of data review inside and outside of scheduled encounters, electronic health record integration strategies, and billing and reimbursement practices.
As CGM technology improves and evidence grows supporting the use of CGM to achieve better clinical outcomes, more investigation is needed to understand facilitators and barriers to widespread use of CGM in real-world clinical practice. The primary aims of this study were to (1) examine relationships between provider attributes and rates of CGM use among their patients, (2) characterize provider behavior related to CGM data, and (3) describe the implementation landscape of CGM, including facilitators and barriers to broader use.
Methods
Study Population and Recruitment
We administered a national cross-sectional survey to clinicians who treat people with diabetes, between March 12, 2020, and April 30, 2020. The intended survey population included primary care doctors, endocrinologists, advanced care practitioners, diabetes educators, pharmacists, and endocrinology fellows caring for pediatric and/or adult patients with diabetes using CGM.
The anonymous survey was delivered electronically using Qualtrics, a secure web-based application widely used for data capture in research studies. 15 The survey was disseminated using a broad recruitment strategy of email and social media directed toward diabetes-focused clinicians, including listservs through the T1D Exchange Clinic Network, ADA Diabetes Technology Interest Group, Association of Program Directors in Endocrinology, Diabetes and Metabolism, and social media groups for diabetes providers. Recruitment emails linked directly to the online Qualtrics survey. There were no financial incentives related to completion of the survey. The University of California, San Francisco Institutional Review Board approved the research protocol.
Measures
We developed a 55-question survey evaluating provider characteristics, patient demographics, and estimated patient use of CGM. We additionally evaluated providers’ perspectives on CGM, facilitators and barriers to CGM prescription, data review practices, description of clinical infrastructure for CGM, and reimbursement practices. Two open-ended free response questions queried participants’ opinions on CGM-related benefits and challenges. Survey questions were adapted from key references9,10 and the National Institutes of Health (NIH) proficiency scale. 16 We conducted iterative pilot testing with key stakeholders, including endocrinologists, diabetes educators, and a diabetes patient advocate, to adapt and finalize survey language.
Analysis
Descriptive statistics were used to report provider and practice demographic information, and prevalence of Likert scale answers to questions evaluating practice patterns or CGM-related opinions. Chi-square testing was used for the comparative aims to explore relationships between clinician, practice, and patient variables. Using thematic analysis, we mapped survey responses to open-ended questions onto the CFIR. 17 Content was categorized according to CFIR domain, and emerging themes with highest frequency were analyzed.17,18 Data were collected directly via Qualtrics. Quantitative data analyses were conducted using Stata version 16 (StataCorp, College Station, TX). For all statistical tests, significance was set to alpha = .05.
Results
In total, 195 providers completed the survey. After excluding those who did not take care of patients with diabetes (n = 3) or did not take care of patients using CGM (n = 10), 182 responses were used in the subsequent analysis.
Participating clinicians were predominantly female (73.2%) and endocrinologists (70.6%) with varying years of experience (Table 1). Practice setting varied although most providers practiced in academic health systems (77.4%) and urban settings (70.7%). The majority of respondents (69.4%) reported CGM use in >51% of their T1D patients. Reported CGM use in type 2 diabetes patients was lower, with half of the respondents noting less than 10% usage and another half reporting between 10% and 50% usage (Figure 1).
Clinician and Practice Characteristics (n = 182 a ).
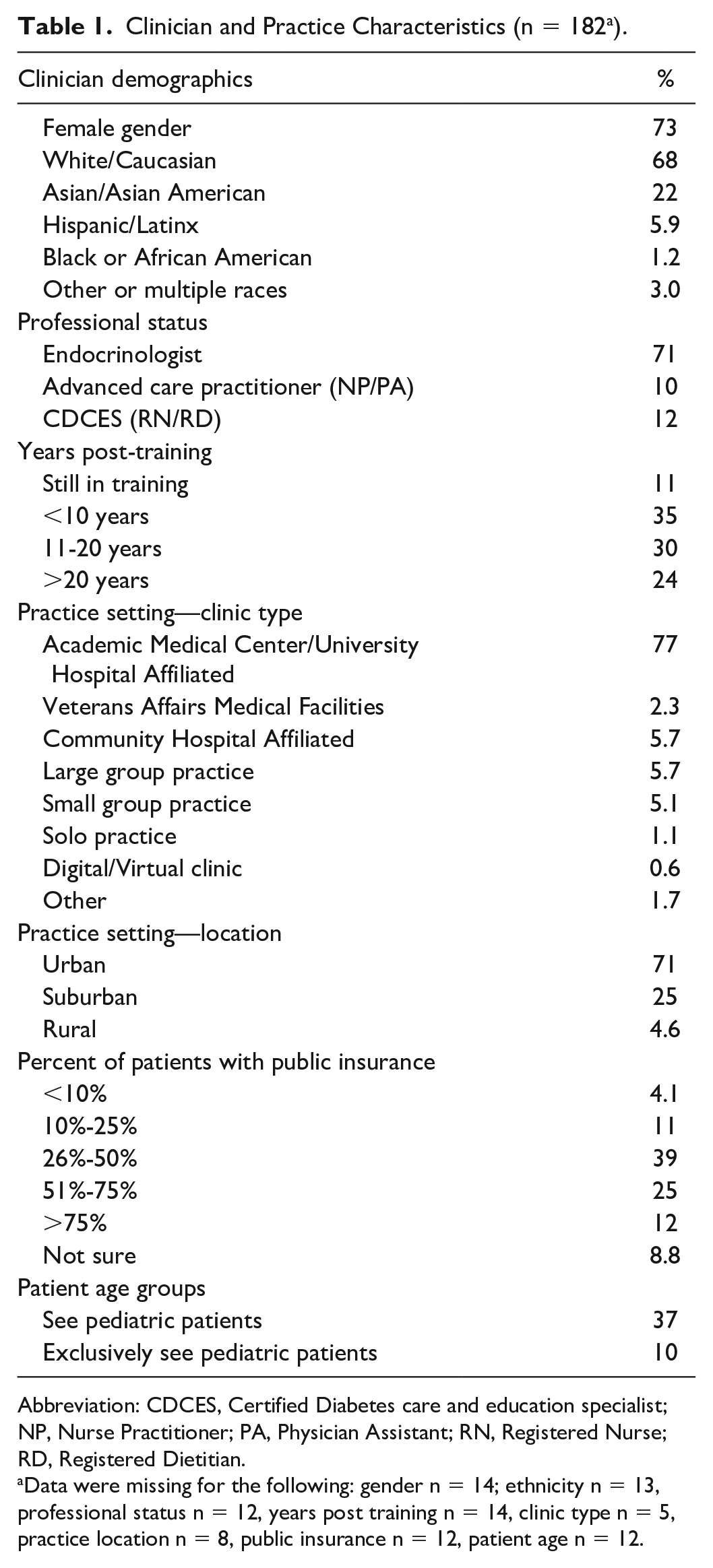
Abbreviation: CDCES, Certified Diabetes care and education specialist; NP, Nurse Practitioner; PA, Physician Assistant; RN, Registered Nurse; RD, Registered Dietitian.
Data were missing for the following: gender n = 14; ethnicity n = 13, professional status n = 12, years post training n = 14, clinic type n = 5, practice location n = 8, public insurance n = 12, patient age n = 12.
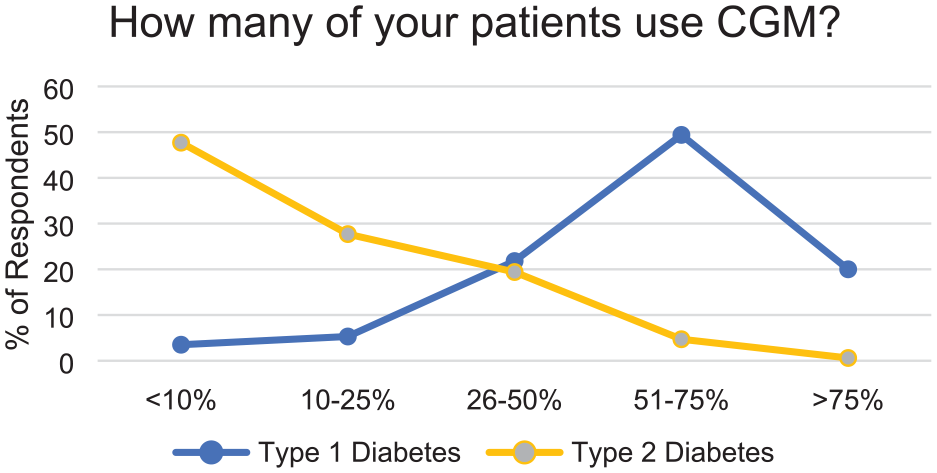
Percent of patients who use CGM as reported by survey respondents. Abbreviation: CGM, continuous glucose monitoring.
CGM Data Review Frequency and Efficiency
Regarding CGM data review frequency, nearly all providers reviewed CGM data during each scheduled visit (97.7%) and actively involved patients in the data review and interpretation (98.8%). If contacted by patients or patients’ family members outside of the visits, 71.7% reported reviewing CGM data “often” or “always.” However, only 14.1% of clinicians reported reviewing CGM data outside of a scheduled visit without any prompting from the patient or family, consistent with a definition of remote patient monitoring. 19
We asked about the process to obtain and view CGM data during a typical scheduled in-clinic visit and found that 56.1% of clinicians agreed they had an efficient process. About two-thirds (68.9%) of respondents endorsed having adequate software and computer resources to visualize the CGM data, but fewer (45.1%) endorsed adequate time to obtain and interpret the CGM data. Participants were asked how they accessed CGM data; multiple responses were permitted. Of all responses, the two most common methods for accessing CGM data during a scheduled visit were physically downloading data from a device (84.7%) or accessing data online from a continuously connected device (62.9%) (Table 2). Despite limitations in the efficiency of the review process, nearly all (98.7%) agreed it was worth the effort to have CGM data to discuss with the patient.
Methods of CGM Data Access.
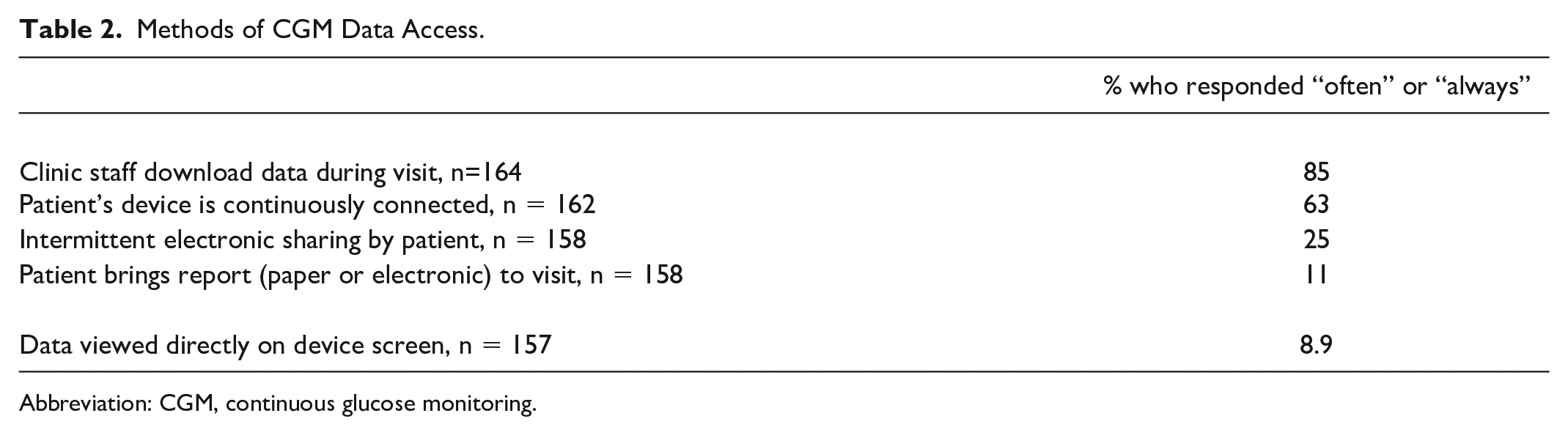
Abbreviation: CGM, continuous glucose monitoring.
Electronic Health Record Practices
Respondents equally agreed (40.9%) and disagreed (41.5%) about having an efficient process to include CGM data in the electronic health record (EHR). Clinicians reported manual entry of CGM data into the visit note (35.0%) or attachment into EHR as a scanned document or image (47.5%). A minority of respondents (15.4%) reported CGM data being directly integrated into the EHR. Of those who reported direct EHR integration, there were no significant differences in their provider characteristics; the majority (74.1%) practiced at academic health centers.
Reimbursement Practices
Regarding reimbursement, 78.8% of providers reported billing for CGM data interpretation during a visit, while a much lower number (40.1%) sought reimbursement for CGM interpretation outside of a scheduled visit. We excluded providers in integrated health systems in which no fee for service billing is possible.
Provider Opinion
We surveyed providers about CGM technology itself, provider perception, patient perception, and clinical infrastructure (Table 3). Nearly uniformly, clinicians agreed that CGM is an important diabetes technology that can increase quality of life, optimize diabetes control, and provide more data. The majority of respondents reported that their patients are interested in CGM. Despite strong patient and provider interest in CGM, respondents also endorsed prohibitive cost of CGM and associated supplies, and inadequate time and training resources (eg, clinical staff time, educational materials) to support patients’ CGM use.
Provider Opinions on CGM, n = 166 a .
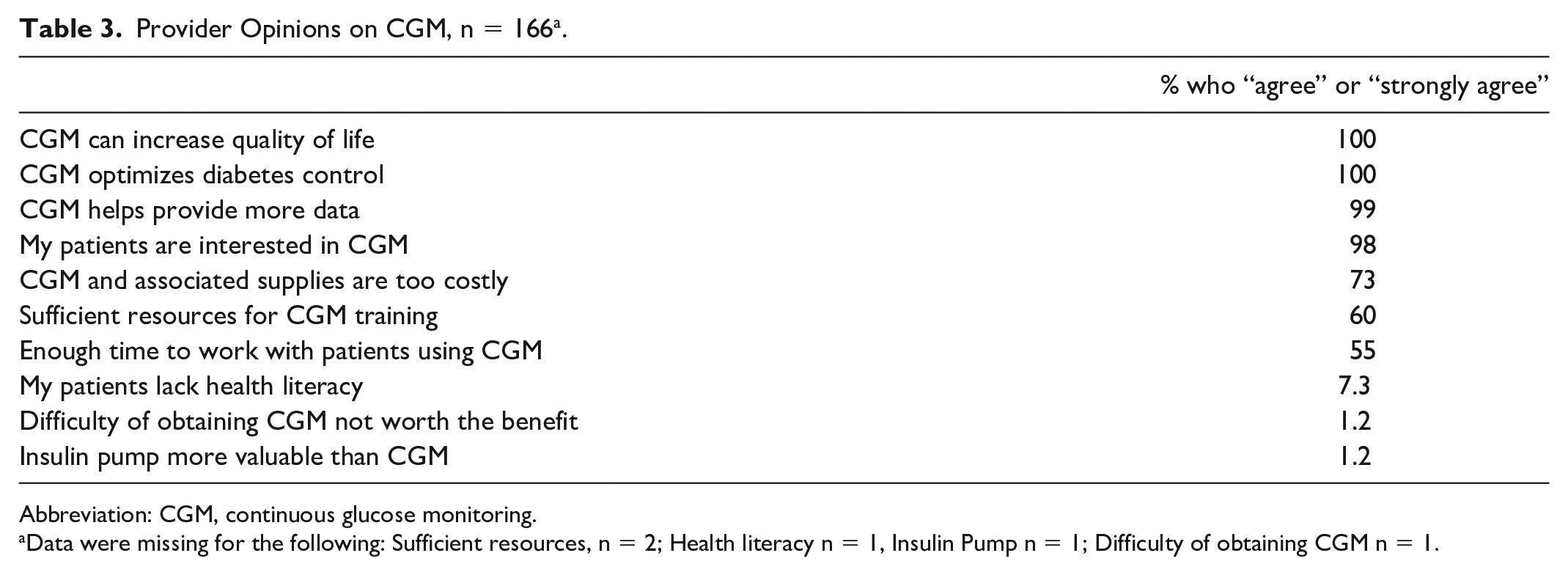
Abbreviation: CGM, continuous glucose monitoring.
Data were missing for the following: Sufficient resources, n = 2; Health literacy n = 1, Insulin Pump n = 1; Difficulty of obtaining CGM n = 1.
Practice Volume
Regarding practice volume, we compared providers who saw 50 or fewer patients with T1D per month (“low-volume” providers, n = 124) with providers who saw 51 or more patients with T1D per month (“high-volume” providers, n = 40). Low-volume providers and high-volume providers both reported CGM use in the majority of their patients with T1D (69.5% vs 69.1%, P = .95). Low-volume providers and high-volume providers had no significant differences in terms of years of practice, proportion of patients with public insurance, remote monitoring practices, or reimbursement practices. High-volume providers, as compared to low-volume providers, were more likely to report efficient data review processes (75.0% vs 50.0%, P = .01). Regarding self-described proficiency with CGM, we used the NIH scale to categorize providers as “Novice,” “Intermediate,” “Advanced,” and “Expert.” 16 High-volume providers were more likely to describe themselves as “Expert” than low-volume providers (60.0% vs 33.1%, P = .02).
Provider Experience
Survey respondents had a wide range in years in practice (Table 1). Providers with 10 or fewer years of clinical practice were similar to those with 11 or greater years of practice: there were no significant differences in terms of reported CGM use, remote monitoring practices, reimbursement practices, perceived efficiency with CGM data review, or self-described proficiency with CGM.
Provider Perspectives on CGM Use
Related to their roles as providers, respondents were asked two open-ended questions about benefits and challenges of working with patients using CGM. Responses were categorized as facilitators or barriers according to the CFIR domains and themes that emerged most frequently are presented (Table 4). Top reported facilitators of CGM use were the providers’ view of CGM as a beneficial tool for diabetes care and patients’ desire to use CGM. Frequently reported barriers related to challenges in insurance coverage, burdensome prescription process, and prohibitive cost. Respondents also described the challenges in accessing CGM data and limited time and support for training patients and CGM review.
Facilitators of and Barriers to CGM Provision and Data Use by Providers (CFIR) (n = 87).
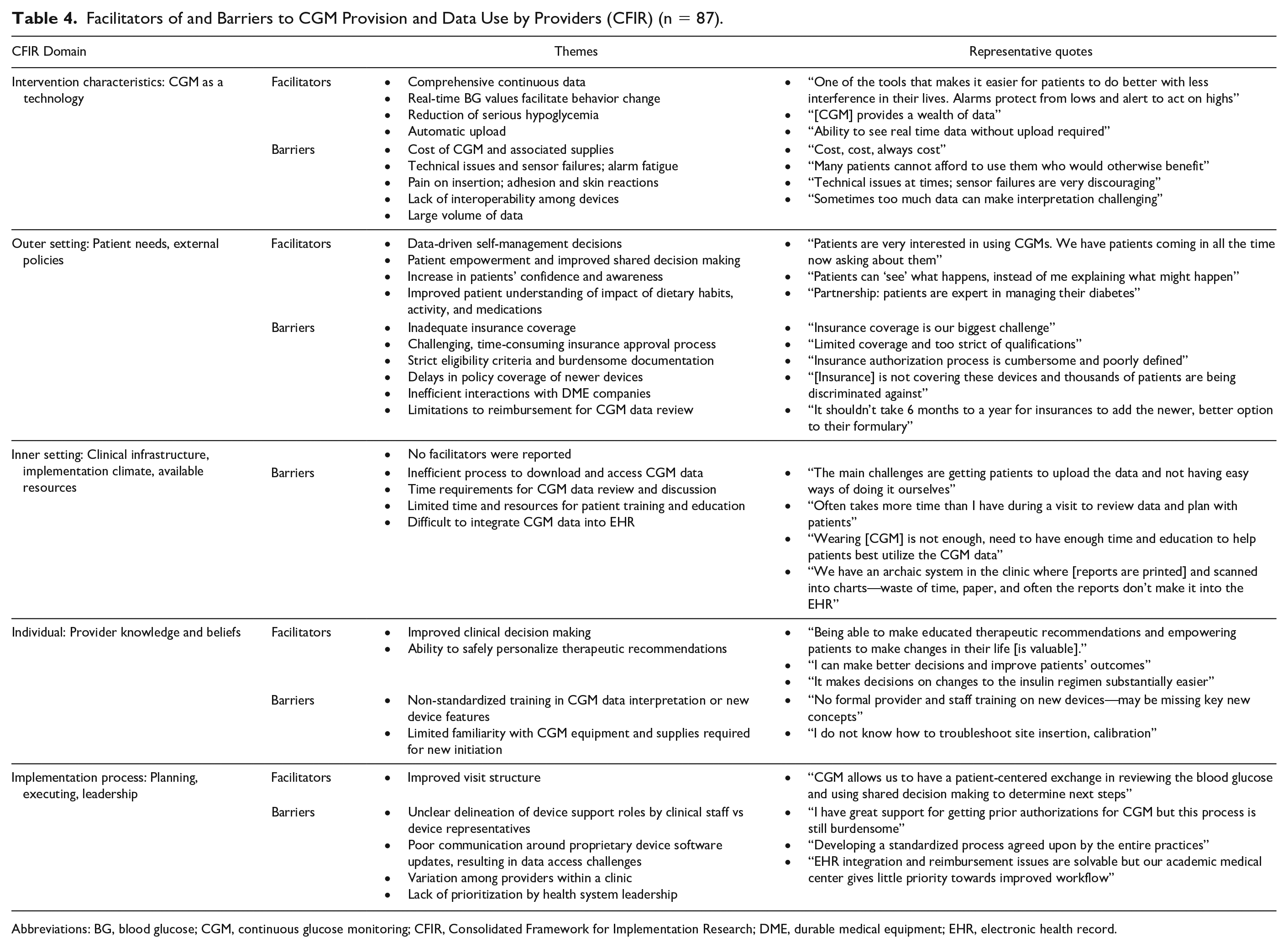
Abbreviations: BG, blood glucose; CGM, continuous glucose monitoring; CFIR, Consolidated Framework for Implementation Research; DME, durable medical equipment; EHR, electronic health record.
Discussion
Recognizing their key role as facilitator for widespread CGM use, we studied providers involved in diabetes care and their role in CGM provision and data use. We used a comprehensive implementation framework to explore facilitators and barriers. To our knowledge, this study included the largest number of US endocrinologists to date on this topic and is the first to focus on factors such as EHR integration or reimbursement patterns.
Recent investigation has highlighted the role of endocrinologist as “gatekeeper” to people with diabetes accessing diabetes technology.20-22 Previous studies evaluating the role of diabetes care provider have largely focused on primary care providers and diabetes educators.9,10,23 Therefore, we felt it important to understand the role of the endocrinologist. Our collective findings contrast with prior published data which have focused primarily on diabetes educators in urban, academic settings. 9 First, we found no differences in positive beliefs toward CGM or reported rates of CGM use across provider experience level or practice setting. Second, the majority of clinicians in our survey endorsed strong patient interest in CGM. Broadly positive views on CGM, and higher reported rates of use compared to prior studies, may be explained by technology improvements and national trends toward increased CGM use. Finally, in contrast to prior study where only a minority of providers reported a need for more staff and time to support CGM use, this limitation was commonly endorsed in our study. 9 This may be related to a higher proportion of endocrinologists in our sample, for whom a large proportion of data review and documentation responsibilities fall.
Although regular CGM data review by providers is broadly encouraged, the nature of data review practices has not previously been characterized. Our evaluation identified that a majority of diabetes care providers review CGM data at every scheduled visit and actively involve patients in visit-based CGM data review, something patients and providers believed to be of value, despite the efficiency challenges. In diabetes care, a higher frequency of clinical interactions between the patient and care team is associated with improved control and increased treatment satisfaction.24,25 However, despite most providers having continuous cloud-based access to CGM data, we found that most providers continued to practice a traditional approach to chronic condition care with episodic visits every few months. A population health approach, leveraging unprompted, non-visit-based CGM review and asynchronous messaging, was rare. Although reimbursement structures for CGM interpretation exist, concerns about inadequate allowable billing frequency and lack of protected provider time for asynchronous review are likely to limit remote patient monitoring practices. In addition, providers who performed asynchronous CGM review were unlikely to seek reimbursement for their time or reported being unaware they were able to do so.
These data from a group largely comprised of diabetes specialists were collected at a unique moment in American health care, just as the COVID-19 pandemic was beginning to unfold at the start of 2020. The pandemic, and a shift toward telehealth, has since accelerated rapid restructuring of data access practices, including incorporation of fully web-based workflows.26-28 Endocrinology practices, compared to other specialties, conducted visits largely through telemedicine throughout the pandemic. 29 By the start of 2021, Endocrinology was second only to Behavioral Health in continued telemedicine usage, 30 and many have described the data-driven coaching approach in diabetes care as particularly amenable to virtual care. 31 As we move into an ongoing hybrid of telemedicine and in person care,26,28,32 these new data sharing processes will likely facilitate restructuring of traditional diabetes care models. Much more frequently, connected device data from smart pens, insulin pumps, and CGM are likely to be passively shared and continuously available, not just as a periodic data upload during a scheduled visit. Health systems with nontraditional care structures and newer digital coaching programs are able to more frequently review CGM data, as well as separately from synchronous one-on-one visits.33-35 In addition, people with diabetes are increasingly open to remote monitoring, with the promise of receiving additional support from health care teams. 36 Although our survey found infrequent remote monitoring of CGM data, these data were collected at the onset of the COVID-19 pandemic, and we expect to see more frequent and consistent use of remote monitoring going forward. As the national health care landscape increasingly shifts toward value-based and risk-based reimbursement models, passively shared, connected device data may be key to proactive, population-based diabetes management.
Diabetes clinics largely lacked a sufficient and prepared remote data monitoring infrastructure for the pandemic. Knowing that our survey was distributed just as the pandemic was beginning across the United States, it was notable that the majority of clinicians depended on clinic staff to physically download device data in person. Only 56.1% of respondents felt that they had an efficient method for data access and only 45.1% had sufficient time for meaningful data review, despite the group being mostly diabetes specialists in academic centers. To facilitate appropriate clinical use of CGM data, and amid increasingly telehealth-driven care settings, improvements in data access are needed. Clearly defined workflows within a clinical practice setting, including designating a “diabetes technology champion,” and close collaboration with information technology support were identified as strategies to improve and maintain data access. 37 Recently, some diabetes practices have successfully collaborated with device manufacturers to directly integrate CGM data into the electronic health record,38-40 a feature reported by only 14% of our respondents at the time of our survey.
Effective interpretation of CGM data requires time and improves with experience. We found that clinicians who saw a higher volume of patients using CGM reported higher perceived proficiency related to CGM. As CGM prescribing extends beyond diabetes specialists and into primary care settings, standardized training on CGM interpretation may support primary care providers for whom CGM-related education has been limited. 41 Existing education on standardized CGM data interpretation developed by national organizations including the American Diabetes Association and the American Association of Clinical Endocrinology could be leveraged. CGM data interpretation is time-intensive, and the majority of respondents reported inadequate time for data review, which is likely to be another barrier to widespread prescribing by primary care providers. Although reimbursement for CGM data interpretation was widely reported, reimbursement alone has not allowed diabetes clinicians to spend sufficient time on CGM-related activities. In the future, advanced decision support driven by machine learning may increasingly empower endocrinologists and primary care providers to efficiently interpret CGM data into actionable insights for patients.42,43
The greater clinical uptake of CGM has been accompanied by an increased recognition of disparities in use of diabetes technology. Recent studies have queried the combined role of provider implicit bias and systemic barriers in contributing to inequities in diabetes care and device use among patients with T1D.11,44-47 In our study, while clinicians reported higher rates of CGM use in their patients than prior studies, they also highlighted factors beyond provider opinion that negatively influence CGM prescription, including high cost, insurance coverage, and burdensome documentation requirements. Addressing these external factors will require a multifaceted approach by policy makers, health systems, and manufacturers to ensure an equitable prescribing environment to increase CGM uptake in all eligible people with diabetes.48-50
We recognize several limitations of our study, including the cross-sectional nature and the dependence on self-reported data. Our study population was heavily skewed toward diabetes specialists at urban academic centers, so may not reflect practices of diabetes specialists and non-specialists in other settings. Perhaps most importantly, we focused only on those providers who do care for patients using CGM. We intentionally chose to focus on providers who use CGM to characterize current practices and challenges that will influence wider CGM uptake. However, the perspectives of diabetes providers who do not care for patients using CGM, including primary care providers, are critical to understand as they provide care to a substantial portion of people with diabetes. 51 We found higher CGM use reported than prior T1D Exchange data, 8 which may reflect overestimation in self-report, but also likely reflects trends over time toward increasing CGM use. Future studies should further investigate CGM use in varying care delivery modalities, and deeper evaluation of these practices in non-academic and non-urban settings, as well as a focus on providers who do not regularly use CGM.
Conclusions
Clinicians involved in diabetes care play an important role in promoting and supporting CGM use in their patients. Our results show that diabetes specialists strongly support CGM use and value CGM-generated data in routine diabetes care. Major barriers to CGM use include cost and challenges with insurance coverage. Related to CGM data review, improvements in clinical infrastructure, data access, EHR integration, and sufficient clinician time are required to support providers in caring for a growing population of people with diabetes using CGM. These implications are increasingly relevant as CGM use increases, including in nonacademic centers and in people with T2D.
Footnotes
Abbreviations
CFIR, Consolidated Framework for Implementation Research; CGM, continuous glucose monitoring; DME, durable medical equipment; EHR, electronic health record; NIH, National Institutes of Health; PWD, people with diabetes; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.K. has received consulting fees from Lilly. J.W. has received research support from Dexcom, Inc. and Tandem Diabetes; is a medical advisor; and co-founder of Tidepool (for which she receives no compensation). A.N. has received research support from Cisco Systems, Inc.; has received consulting fees from Lilly, Nokia Growth Partners, and Grand Rounds; serves as advisor to Steady Health (received stock options); has received speaking honoraria from Academy Health and Symposia Medicus; has written for WebMD (receives compensation); and is a medical advisor and co-founder of Tidepool (for which he receives no compensation).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.