
Abstract
Background:
Burnout in people with diabetes and healthcare professionals (HCPs) is at an all-time high. Spotlight AQ, a novel “smart” adaptive patient questionnaire, is designed to improve consultations by rapidly identifying patient priorities and presenting these in the context of best-practice care pathways to aid consultations. We aimed to determine Spotlight AQ’s feasibility in routine care.
Materials and Methods:
The Spotlight prototype tool was trialed at three centers: two UK primary care centers and one US specialist center (June-September 2020). Participants with type 1 (T1D) or type 2 diabetes (T2D) completed the questionnaire prior to their routine consultations. Results were immediately available and formed the basis of the clinical discussion and decision-making within the clinic visit.
Results:
A convenience sample of 49 adults took part, n=31 T1D, (n=18 female); and n=18 T2D (n=10 male, n=4 female, n=4 gender unreported). Each identified two priority concerns. “Psychological burden of diabetes” was the most common priority concern (T1D n = 27, 87.1%) followed by “gaining more skills about particular aspects of diabetes” (T1D n=19, 61.3%), “improving support around me” (n=8, 25.8%) and “diabetes-related treatment issues” (n=8, 25.8%). Burden of diabetes was widespread as was lack of confidence around self-management. Similarly, psychological burden of diabetes was the primary concern for participants with T2D (n=18,100%) followed by “gaining more skills about aspects of diabetes” (n=7, 38.9%), “improving support around me” (n=7, 38.9%) and “diabetes-related treatment issues” (n=4; 22.2%).
Conclusions:
Spotlight AQ is acceptable and feasible for use in routine care. Gaining more skills and addressing the psychological burden of diabetes are high-priority areas that must be addressed to reduce high levels of distress.
Background
There is an urgent need to develop interventions that lead to long-term improvements in glycemic and quality of life outcomes for people with diabetes. Therapeutic interventions to treat diabetes are well known, yet >75% of people with diabetes consistently do not achieve blood glucose targets (even individual therapy targets) for optimal health, despite the large variety of drugs, including insulin, and medical devices available. 1 Such glycemic outcomes have remained stubbornly poor for decades. A greater understanding of the facilitators and barriers to patient behavior, individually supported in routine clinical care, is an important missing component to improved outcomes, in a medical healthcare model poorly suited to supporting successful diabetes management.
Routine patient care visits currently leave both people with diabetes and healthcare professionals (HCPs) feeling frustrated both in primary and specialist care settings. The lack of understanding of the psychosocial burden of diabetes and the evolving consequences results in a negative impact on clinical practice with consequential negative outcomes for patients and increasing frustration for HCPs. At present, healthcare visits are designed to focus on biomedical outcomes of diabetes by using a didactic medical model. Complex and detailed algorithms are supplied by various guidelines for the management of blood glucose, lipids, blood pressure, and long-term complications, but these relate only to medical management. Even mutually agreed on goals are often not followed up, leaving people with diabetes frustrated and HCPs struggling to provide tailored support. Typically, physicians interrupt their patients 11 seconds after they start describing their problems; approximately half of patients’ concerns are not discussed, and in 50% of healthcare visits, patients and physicians disagree on the central problem presented.2,3 Disagreement about treatment goals, inconsistency among healthcare teams, and confusion about treatment priorities are associated with poorer outcomes. 4
HCP burnout is at an all-time high with over half of physicians and a third of nurses experiencing symptoms. 5 This burnout epidemic is both detrimental to HCP well-being, to patient care and to impending physician shortage. There is a pressing need to develop interventions that lead to long-term improvements in the patient–professional interface in routine clinical outpatient appointments. This will improve HCP experience and patient care, and lead to improved outcomes for people with diabetes.
Spotlight AQ, based on the Kaleidoscope Model of Care, 6 identifies the main personal barriers to effective self-management, providing personalized healthcare for each individual person with diabetes according to their current situation, delivered with HCP support. Pilot data show that the tools are acceptable, relevant, and tailored to individual needs when implemented in clinical practice. 7 The tools are designed specifically for routine clinical practice to reduce the burden on HCPs, directly facilitating national roll-out at low cost, with no increase in outpatient visit time. It has the potential to reduce the public health burden of diabetes and associated long-term complications significantly. In essence, the tool is a brief, algorithmic smart questionnaire comprising less than 40 questions (it is not possible to state the exact number of questions as questions change depending on the responses provided by each individual).
At a time where COVID has forced the majority of consultations online and away from traditional face-to-face consultations, novel and effective ways to improve those encounters are required. The aims of the current study were to evaluate the feasibility of delivering the Spotlight AQ e-tools in routine primary and secondary care settings for individuals with type 1 or type 2 diabetes (T1D and T2D). This study design was adopted as a progressive step from previously published pilot data and prior to multi-center randomized controlled trial planned for early 2021.
Materials and Methods
Participants
Adults aged 18 years or above with T1D or T2D attending routine clinical appointments were invited to participate. A convenience sampling strategy was adopted based on outpatient patient lists held at each participating center. HCPs approached the principal investigator requesting participation, thus representing a convenience sample.
Methods
Following institutional ethics approval, participants were recruited via two primary care centers in the United Kingdom and one specialist care Centre in the United States. Participants were asked to complete the Spotlight AQ e-tools prior to their routine out-patient visit. Completion of the e-tool takes three to five minutes on a smartphone, tablet, or computer. The e-tools each comprise a novel “smart” adaptive patient questionnaire designed to improve routine outpatient consultations by rapidly identifying patient priorities and presenting these in the context of personalized areas for concern and best-practice care pathways to illuminate consultations. The number of questions presented to participants varies based on their responses to previous questions and priority concerns identified throughout the process. HCPs received a brief instruction manual but no other training was needed or provided. Links to the questionnaire were sent by HCPs to participants within the seven days prior to the scheduled outpatient appointment. They were able to use the tools in the best way that suited their clinical practice in terms of precise timing of when participants completed the tool. HCPs were provided with lists of support resources for psychological aspects and social aspects of diabetes to signpost to their participants should these be highlighted as a priority concern. Therapy and knowledge priority concerns were addressed using usual care pathways at each participating site.
Data collection occurred during the COVID pandemic with all consultations being held remotely via telehealth. Secure individual links to the questionnaire were sent to participants by their HCP within the week prior to their scheduled appointment. The questionnaires were completed online and results immediately presented to both the participant and the HCP. These results guided the discussion and goal-focused decisions made within the routine clinic appointment.
Results
Forty-nine participants took part in the study, of whom 31 had T1D. Three HCPs participated: two general practitioners (GPs) in primary care in the United Kingdom and one endocrinologist in specialist secondary care in the United States. Participant demographics are presented in Table 1.
Demographic Characteristics of Participants.

Type 1 Diabetes
Thirty-one adults with T1D (n = 13 male; n = 18 female) participated in this real-world evidence collection (see Table 1 for demographic data), each identifying two priority concerns (Figure 1). “Psychological burden of diabetes” was the most common primary concern (n=27, 87.1%) followed by “gaining more skills about particular aspects of diabetes” (n=19, 61.3%), “improving support around me” (n=8, 25.8%) and “diabetes-related treatment issues” (n=8, 25.8%). Burden of diabetes was widespread as was lack of confidence around self-management. Participants with diabetes-related complications more often prioritized “diabetes related treatment issues” than those without complications. For most cited concerns, see Table 2.
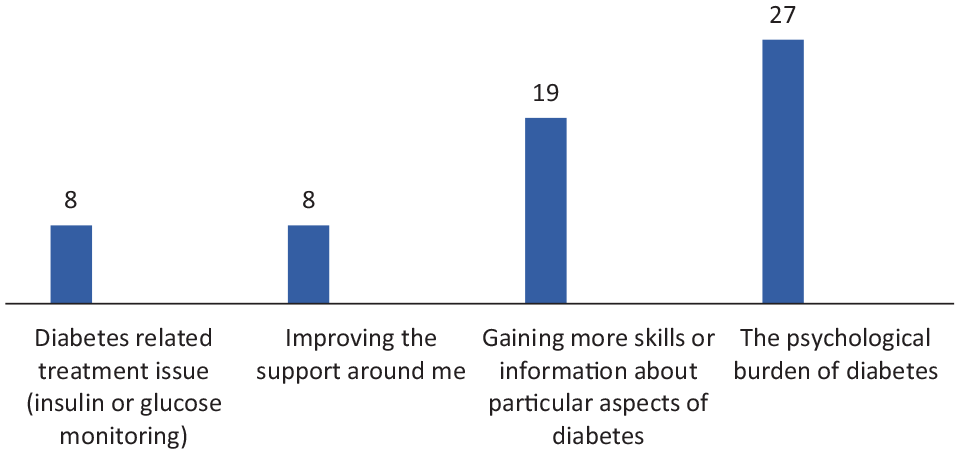
Main areas of priority concern for participants with type 1 diabetes (T1D).
Priority Concerns by Duration of Diabetes (T1D and T2D).
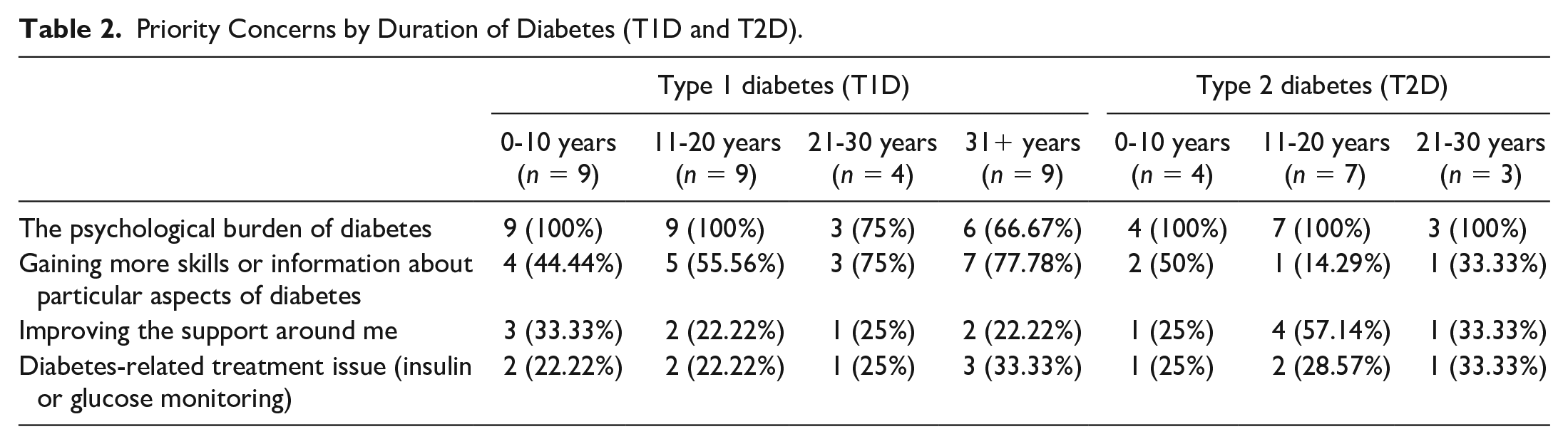
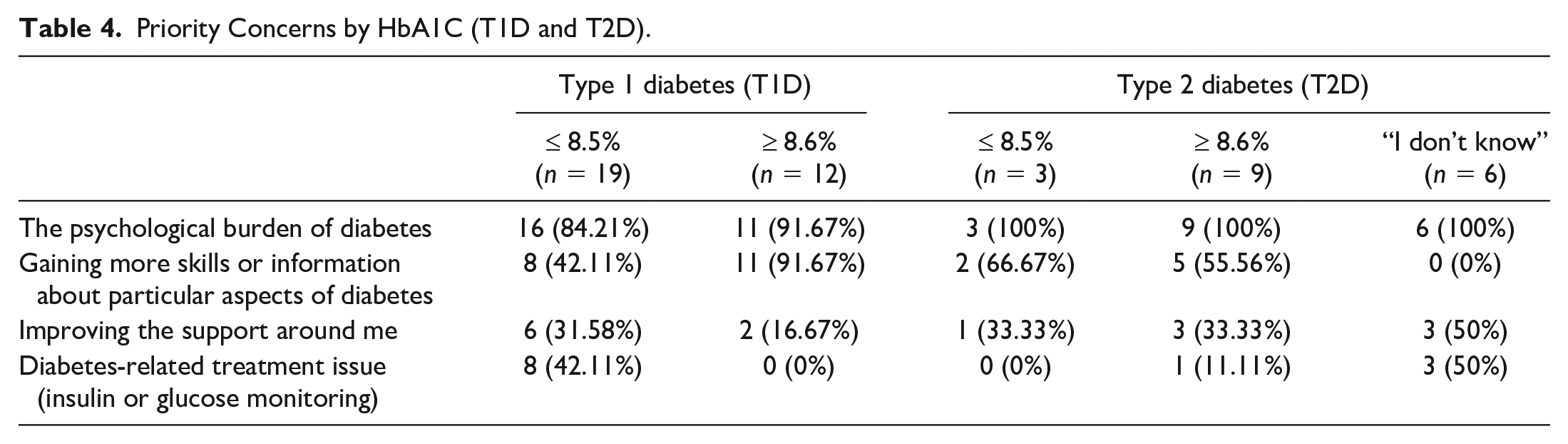
People whose latest haemoglobin A1c (HbA1c) was ≥8.6% were more likely to prioritize “gaining more skills” than those whose A1c was ≤8.5. Men reported greater psychological burden (92.3% vs 83.3%), while women prioritized gaining more skills (66.7% vs 53.9%). Those aged <35 years more often prioritized psychological burden than those ≥35 years (100% vs 82.6%). Gaining more skills was more frequently a priority concern among those with higher duration of diabetes (44% among <10 years vs 68% among >10 years).
Type 2 Diabetes
Eighteen adults with T2D (n=10 male, n=4 female, n=4 did not state) took part in this real-world evidence collection, each identifying two priority concerns (Figure 2). For most cited concerns, see Table 3. The psychological burden of diabetes was the primary area of concern (n=18, 100%) followed by gaining more skills about aspects of diabetes (n=7, 38.9%), improving support around me (n=7, 38.9%) and diabetes-related treatment issues (n=4, 22.2%). Feeling sad about living with diabetes and frustrated that efforts are never enough (each n = 15, 83.3%), feeling scared (n=11, 61.1%) and lacking confidence (n=9, 50%) were all commonly reported. Participants who had diabetes for >10 years were more likely to report lack of social support as a priority concern (50% vs 25%); those with diabetes duration <10 years were more likely to report gaining more skills as a priority concern (50% vs 20%).
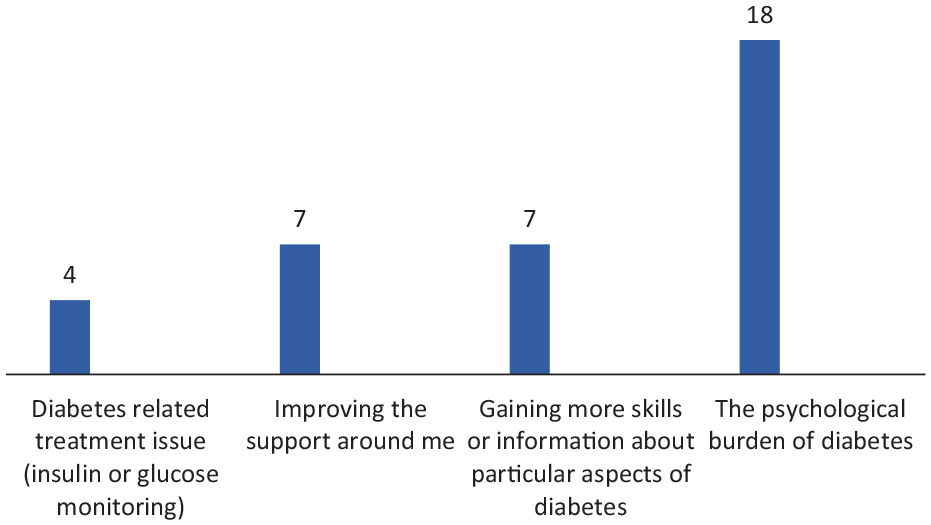
Main areas of priority concern for participants with type 2 diabetes (T2D).
Priority Concerns by Age and Gender (T1D and T2D).
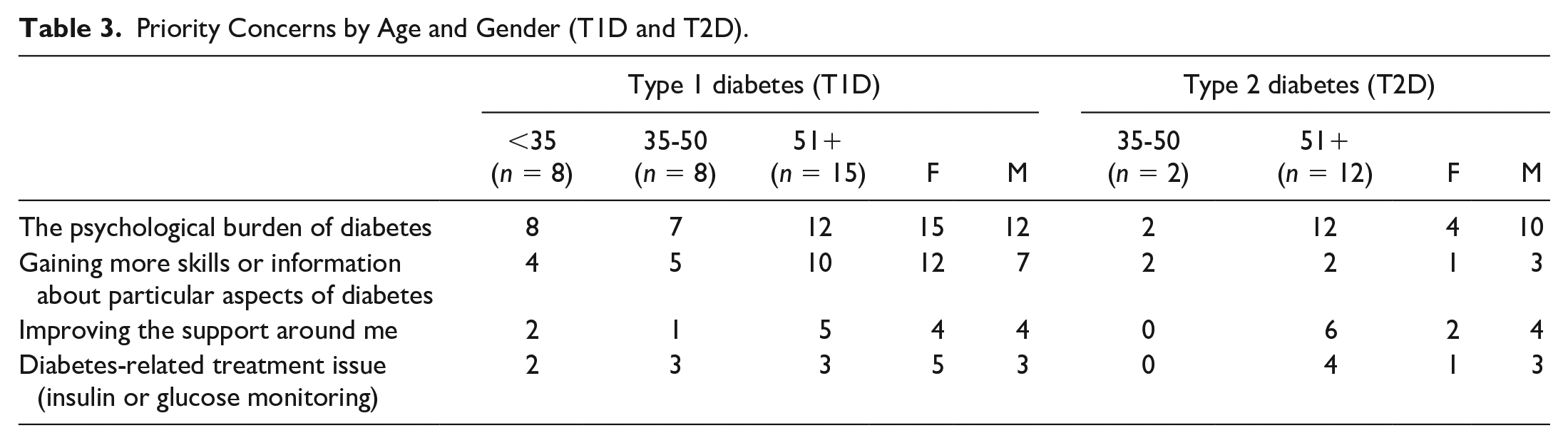
Table 2 presents data broken down by duration of diabetes.
Table 3 presents data broken down by age and gender.
Tables 4 and 5 presents data broken down by HbA1c.
Priority Concerns by HbA1C (T1D and T2D).
Self-Reported Versus Objective Measure of HbA1c (T1D and T2D).

As part of the study, participants were asked to provide their latest HbA1c result. During the study, it was noticed that this subjective recall differed somewhat from the latest recorded HbA1c on the participants’ medical records. As such, both subjective and objective HbA1c data, which were available for 45 participants (n=31 with T1D; n=14 with T2D), underwent comparative analysis. Whilst P values are not provided due to small participant numbers, results enable us to gain an understanding of the level of accuracy surrounding subjective recall of individual HbA1c results. Overall, accurate recollection of HbA1c was poor with only 22 participants (48.9%) having correct recall (Table 6). Six participants (13.3%) did not know their A1c, eight (17.8%) reported it as lower than it actually was, and nine (20.0%) reported it as higher than it actually was. Individuals with T1D were more likely to correctly report their A1c (n=18, 58.1%) than those with T2D (n=4, 28.6%); overestimation was reported by n=7 with T1D (22.6%) versus n=2 with T2D (14.3%); underestimation was reported by n=6 with T1D (19.4%) and n=2 with T2D (14.3%). People with T1D who overestimated their A1c were more likely to have “gaining more skills” (n=6; 85.7%) as a priority concern. People with T1D correctly recalling their A1c were more likely to have “psychological burden” as a priority concern (n=17; 94.4%). Those who did not know their A1c (all with T2D) reported “psychological burden” as a priority concern.
Discussion
Thirty-one adults with T1D and 18 with T2D participated, along with three HCPs from primary and specialist care services. The Spotlight AQ e-tools were acceptable to all participants based on participant and HCP feedback, and are feasible for delivery in routine care. Not unsurprisingly, high levels of diabetes psychological burden were identified amongst participants. In addition, a need to gain more skills about particular aspects of diabetes management was prioritized by the majority of participants.
Addressing the psychosocial challenges of T1D and T2D has been shown to be effective. The barriers to optimal self-management of diabetes lie beyond HbA1c-defined glycemic outcomes. It is well known that factors including (but not limited to) affordability, treatment complexity, potential medication side effects, and poor health literacy all play a major role in people’s ability to follow recommended treatment plans. Furthermore, the impact of psychological factors must be considered for optimal biomedical and quality of life outcomes. Diabetes distress affects a fifth of people with diabetes and rates of depression remain high—20% to up to 46%. Novel, holistic, patient-centered care that is deliverable within the constraints of routine clinic settings is necessary to help people with diabetes explore their barriers and facilitators to diabetes self-management in the context of their lived experience. Such care, harbouring the power of intrinsic motivation, will achieve better personal outcomes in comparison to externally imposed targets by HCPs which are often felt judgemental and unattainable.
Routine patient care visits often leave both people with diabetes and HCPs feeling frustrated both in primary and specialist care settings. The lack of understanding of the psychosocial burden of diabetes and the evolving consequences results in a negative impact on clinical practice with consequential negative outcomes for patients and increasing frustration for HCPs. As highlighted by one participating clinician, the time pressure of approximately 15 minutes per visit in routine consultations is a barrier to addressing psychological aspects in management of individuals with T1D and T2D. Using the intervention tool, with signposting to psychological and/or social support enabled these areas of diabetes self-management to be discussed within the consultation, whereas this would not usually be possible. There may also be a conscious bias to avoidance of such discussions, as HCPs often feel ill-equipped to provide solutions.
At present, healthcare visits are designed to focus on biomedical outcomes of diabetes within a healthcare framework where the didactic medical model prevails. Complex and detailed algorithms are supplied by various guidelines for the management of blood glucose, lipids, blood pressure, and long-term complications, but these relate only to medical management, despite the growing understanding that the psychosocial aspects of diabetes must be addressed for improved outcomes. The current study has demonstrated that using patient-centered e-tools within routine care can improve the healthcare experience for both HCPs and their patients. Spotlight AQ enables ascertaining the patient’s agenda in a time efficient manner, adding value for the individual attending the consultation. As such, all participating HCPs reported that they would recommend the tool to their colleagues.
The strengths of the study include the real-world nature of its design. It was recognized that the tool must work within the constraints of routine care and could not increase consultation times. The limitations of the study include the small sample size and inability to follow up with participants over time to determine any enduring effect of the experience. Furthermore, qualitative aspects were limited so it was not possible to fully understand the experiences of participants. HCPs, however, rated the tool highly saying “ . . . a user friendly, pragmatic tool that helps with patient engagement and sets the scene for the consultation. It is simple to use and implement . . . without an added burden on time.” The current study used a prototype version of the tools, which was functional but rudimentary. Programming is underway to incorporate greater links to electronic medical records and avoid self-report of HbA1c or complications status by participants. Randomized trials are planned to determine the clinical and cost-effectiveness of the commercial platform of the tool and to validate it in a wider population of individuals with T1D and T2D.
Conclusions
Spotlight is acceptable and feasible for use in routine care. Gaining more skills and addressing the psychological burden of diabetes are high priority areas that must be addressed to reduce high levels of distress. Further work to validate the tool is ongoing in English, Mandarin, and Spanish language written and audio/colour versions.
Footnotes
Abbreviations
GP, general practitioner; HCP, healthcare professional; N, number; T1D, type 1 diabetes; T2D, type 2 diabetes, HbA1c, haemoglobin A1c.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KBK is the owner of Spotlight Copyright and IP. All other authors declare that there is no conflict of interest
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.